Abstract
Background
This study describes the experiences and results of a large-scale human immunodeficiency virus (HIV) prevention intervention for long-distance truck drivers operating on the national highways of India.
Methods
The intervention for long-distance truckers started in 2004 across 34 trans-shipment locations. However, due to poor coverage and utilization of services by truckers in the initial 18-month period, the intervention was redesigned to focus on only 17 trans-shipment locations. The redesigned intervention model was based on the McDonald’s business franchise model where the focus is on optimal placement of services, supported with branding and standardization of services offered, and a surround sound communication approach. Program output indicators were assessed using program monitoring data over 7 years (2004–2010) and two rounds of cross-sectional behavioral surveys conducted in January 2008 (n = 1402) and July 2009 (n = 1407).
Results
The number of truckers contacted per month per site increased from 374 in 2004 to 4327 in 2010. Analysis of survey data showed a seven-fold increase in clinic visits in the past 12 months from 2008 to 2009 (21% versus 63%, P < 0.001). A significant increase was also observed in the percentage of truckers who watched street plays (10% to 56%, P < 0.001), and participated in health exhibitions (6% to 35%, P < 0.001). Furthermore, an increase from round 1 to round 2 was observed in the percentage who received condoms (13% to 22%, P < 0.001), and attended one-one counseling (15% to 21%, P < 0.01). Treatment-seeking from program clinics for symptoms related to sexually transmitted infections increased six-fold during this period (16% versus 50%, P < 0.001).
Conclusion
Adoption of a business model for HIV prevention helped to increase program coverage and service utilization among long-distance truckers. Implementing HIV prevention programs in a highly mobile population such as truckers, in a limited number of high-impact locations, supported by branding of services, could help in saturating coverage and optimum utilization of available resources.
Introduction
The role of truckers, particularly long-distance truckers, as an effective bridge in spreading human immunodeficiency virus (HIV) infection from high-risk groups, such as female sex workers, to low-risk women in the general population has been highlighted.Citation1,Citation2 Truckers spend much of their time on the road, where they are likely to engage in risky sexual activities. Their likelihood of exposure to HIV prevention programs is also restricted due to their constant mobility. The situation of truckers in India is no different from that in other countries. There are about 5 million truckers including helpers in India, of whom about 40% operate on long-distance routes covering more than 800 km one way.Citation3 Previous research in India among truckers has revealed a high rate of unprotected sex with female sex workers and sexually transmitted infection (STI).Citation4–Citation7 A large biobehavioral survey indicates that one-fifth of long-distance truckers were using condoms inconsistently with paid female partners and one in five truckers were diagnosed with an STI, including HIV and syphilis.Citation7
HIV prevention interventions targeted at truckers started in India in 1993, when truckers were provided clinical services at major highway stopping points.Citation8 Thereafter, an upscaled intervention, popularly known as “healthy highways,” was introduced in 1996 across 200 sites spread over 19 states. The intervention sites were either trans-shipment locations (places where trucks are unloaded and reloaded, or halt for maintenance and replenishing supplies) or roadside cafes along the highway.Citation9–Citation11 An evaluation of the healthy highways intervention in 2000 revealed that only 43% of truckers and 29% of helpers reported consistent condom use with nonregular female partners.Citation12 An independent survey among health care providers indicated that STI care management in the healthy highways intervention lacked attention, particularly in physical examination, prescription of standard medicines and regimen, counseling on condom use, and partner referral for STI treatment.Citation13 Subsequently, a few small-scale interventions engaged peer educators as part of their behavior change communication strategy.Citation14–Citation17 These programs focused on the distribution of educational materials on safe sex practices, condom promotion, and treatment for STI-related symptoms at STI clinics run by the program. In the late 1990s, the Bhoruka Public Welfare Trust established “free tea parlors” at major truck halt points where truckers were encouraged to utilize STI clinic services.Citation18
However, the healthy highways and other small-scale interventions supported by the government and donor agencies worked independently without any coordinated efforts to scale up the program. Further, most of these programs were mainly driven by the peer education strategy to change the behavior of truckers, which may have resulted in low outreach among these men, given their high degree of mobility. In order to reach the target population at scale, the Bill and Melinda Gates Foundation initiated a comprehensive nationwide intervention for long-distance truckers in 2004 known as Kavach (meaning “shield” in Hindi/Urdu).Citation19 The highlight of the Kavach intervention was to adopt a successful business model to increase the effectiveness of the HIV prevention program. The program was founded on the basic principles of how an intervention can be designed to reach a highly mobile population like truckers, and how innovative communication mechanisms can be designed to sustain behavior change in this group. This paper describes the intervention and discusses how the challenges were addressed through a redesign process with the adoption of a business model. Further, it examines the program outputs in terms of coverage and service utilization by long-distance truckers.
Materials and methods
Intervention
The Kavach intervention was initiated in 2004 by contracting 34 local nongovernmental organizations with prior experience of working with truckers to cover various trans-shipment locations across the country. The program implemented activities similar to those used for healthy highways and other small-scale interventions.
An assessment of the program monitoring data in 2005 revealed that only 4% of those who accessed STI services were indeed long-distance truckers, which was significantly lower than the expected project target. Further, half the individuals who accessed program services were either short-haul truckers or workers in the trans-shipment locations. Qualitative discussions with local nongovernmental organizations and other stakeholders revealed that the main reason for suboptimal performance of the program was inappropriate allocation of services/resources. Several other factors were identified, including lack of standardization of services, continued communication fatigue, limited branding and visibility, the short attention span of truckers, and the need for message reinforcement. The program management decided to redesign its strategy in 2006 in order to improve the utilization of services and coverage of the target population.
Implementation of redesigned program
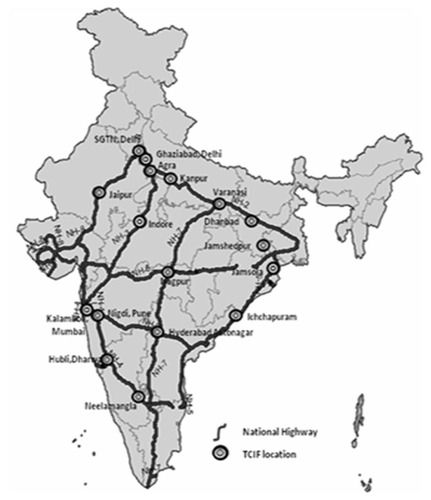
The redesigned intervention strategy was adapted from the well known McDonald’s business franchise model, which is based on the concept of a uniform look and service across all franchise outlets.Citation20,Citation21 Therefore, the redesigning process focused mainly on creating convenience of access through intelligent placement of services, standardization of service delivery, and a uniform look and feel across network clinics. A surround sound communication approach was used, where the number of service touch points was increased within a trans-shipment location to ensure message reinforcement and recall. Further, peer educators from the trucking community were engaged to create awareness about HIV, STIs, and condom use through different innovative interpersonal communication tools. Allocation of service points at optimal locations was done by reducing the number of intervention sites. Trans-shipment locations were selected based on information such as volume of truckers visiting the site (10,000 truckers per month), geographic location, and the average time spent by truckers at the site. In addition, a broker/transporter census was conducted in 2006 which enumerated 766,028 truckers, of whom 451,699 were long-distance truckers. Based on this information, 17 sites (15 trans-shipment locations and two check posts) were identified for intensive intervention in the redesigned phase of the program. These sites were strategically located on the golden quadrilateral highway route connecting the metropolitan cities of Delhi, Kolkata, Chennai, and Mumbai ().
Figure 1 Map of India showing trans-shipment locations and operating routes among long-distance truck drivers.
Provision of STI treatment
In the redesigned intervention approach, efforts were made to achieve high clinic visibility, efficiency, and accessibility. Two types of clinics were set up static clinics (one at each intervention site) and satellite/mobile clinics (six clinics at each intervention site). Static clinics were located at a fixed location in the trans-shipment location, while satellite clinics were organized in natural traffic areas of the trans-shipment location. Around 80 satellite clinics were set up initially, most of which were in the offices of brokers/transporters, with 120 hours of clinical services provided per site per month. Clinics were branded as “Khushi” clinics (Khushi meaning “happiness” in Hindi) with a distinctive logo consisting of two flowers, indicating happiness; these clinics were positioned as general health clinics rather than as exclusive STI clinics to reduce the stigma associated with such clinics. To ensure clinical services had a uniform look and feel, all clinics were painted yellow and blue and a standardized interface of services was developed across the intervention sites. Truckers visiting a Khushi clinic for the first time were issued a diary (called a Khushi passport) in which details of the client’s medical history, diagnosis, and medication provided at each clinic visit were recorded. Truckers were instructed to carry this diary with them during clinic visits. The diary also contained the addresses of all Khushi clinics across the country to encourage truckers to access services while on the move.
Enhanced communications activity
One of the important strategies in the redesigned phase was the adoption of a surround sound communication approach, which is an integrated and multilayered behavior change communication strategy. Outreach workers were replaced with peer educators, who were either active truckers or ex-truckers, to conduct interpersonal communication sessions with fellow truckers. Peer educators were given intensive training on the use of participatory tools and audiovisual aids, including flip books, flash cards, and discussion guides. The training sessions emphasized dialog-based communication designed to generate audience participation and interesting interaction. Trainings were organized at the site level to enable hands-on training. Peer educators facilitated discussions in a group of 10–12 fellow truckers on HIV, STIs, common misconceptions, and the importance of condom use. Typically, group participatory sessions lasted 60–90 minutes. In addition, a multilayered communication strategy was used to ensure message recall and synchronization across locations by street plays, health games, film shows, and distribution of audio cassettes. A series of selected themes related to common misconceptions on STI/HIV transmission among truckers were identified for the communication strategy. Presentation styles of theme messages were standardized to ensure uniform messaging across sites. Theme messages were updated every 6 months to keep them new and contextual. Therefore, while designing communication activities, the views expressed by truckers during focus group discussions were taken into account.
Data
The data used to examine progress in program outputs were drawn from two sources: program monitoring data and two rounds of behavioral tracking survey.
Program monitoring data
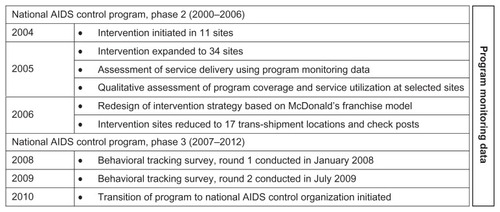
Program monitoring data were collected in paper formats on a monthly basis by program implementing nongovernmental organizations at the site level, which were then aggregated and computerized at the national level. Truckers who accessed services from the Kavach intervention were assigned a unique identification number to track their service utilization in any site across the country. Data on program coverage and service utilization were collected in this system from 2004 to 2010 (). Examples of key indicators for which information was generated include number of truckers contacted, number of truckers visiting Khushi clinics, number of truckers diagnosed with STIs, and number of condoms socially marketed.
Figure 2 Time lines of occurrence of important program activities during Kavach intervention.
Behavioral tracking survey
The behavioral tracking survey is a cross-sectional survey conducted in multiple rounds to assess program exposure, service utilization, effectiveness of communication activities, knowledge and risk perceptions about HIV, condom use, and treatment-seeking behaviors among truckers. We used data from two rounds of the behavioral tracking survey conducted during January–February 2008 and July–August 2009 to examine program coverage and service utilization among truckers. Six intervention sites were purposefully selected to represent different regions of the country. The selected sites were located at Ghaziabad and Delhi (representing northern India), Indore (representing central India), Mumbai and Pune (representing western India), and Bengaluru (representing southern India). A combined sample size of 1400 across the six sites was fixed for each round of the survey. The total sample size was distributed across the six survey locations according to the total population of truckers in those sites.
Samples were drawn using a two-stage sampling process; in the first stage, clusters were formed based on the parking areas for trucks. In the second stage, respondents were randomly selected from selected clusters after screening them for eligibility. The eligibility criteria for participation in the study were males who were 18 years or older, had worked as a trucker for at least 2 years, and had worked in a truck with a national permit (ie, permission from the government to carry goods across the country). The number of interviews to be conducted in a cluster was decided proportionately according to the proportion share of number of truckers in the cluster with respect to the number estimated in the site. The registration number of trucks parked in each cluster on the day of the survey was listed and a systematic random sampling approach was used to select the trucks. The drivers or helpers of the selected trucks were approached to participate in the survey. If a respondent was not found to be eligible, he was replaced with another respondent selected from the same cluster following the systematic random sampling approach. The same process was followed in the event that a respondent refused to participate in the survey. At the end of the survey, 1403 and 1407 truckers, respectively, in round 1 and round 2, completed the questionnaire.
This behavioral study was conceived as routine program monitoring to improve the program implementation and its outcomes. Therefore, the study was not formally reviewed and approved by any institutional review board. However, ethical principles were followed in conducting the study, including the use of a consent form in the questionnaire. In order to protect the confidentiality of the respondents, we did not collect any identifiers (name or address) in the questionnaire or any other research document, and the participant was informed of the same. All participants were told the possible harms and benefits associated with their participation before the start of the interview. To maintain privacy, interviews were either conducted inside the truck or in a secluded public area such as road corners where others would not be able to listen to the interview. Participants were not given any monetary compensation for participation in the study. Only participants who consented voluntarily were interviewed in the study. Trained research investigators used a structured questionnaire to collect data after taking consent of individuals. Research investigators were graduates in social science and native speakers of the local language of the survey site. The questionnaires were developed in English and then translated into the local language of the survey site. Study investigators who were fluent in both English and the local language reviewed the translated questionnaires. These translated questionnaires were pretested in similar settings before the start of the survey.
Measures
The following key indicators from program monitoring data were used to examine program coverage and the extent of service utilization: number of truckers contacted per month per site, number of truckers visiting the Khushi clinic per month, number of condoms socially marketed, and number of condoms sold per trucker. Definitions of these indicators are presented in .
Table 1 Definition of program monitoring indicators
The behavioral tracking survey collected information on truckers’ sociodemographic characteristics, program coverage, and service utilization using a structured questionnaire. Single item questions were used to gather information on different program coverage and service utilization indicators. The key measures used to examine program coverage in the 12 months prior to the survey were: visited a Khushi clinic, watched street plays, participated in health exhibitions and film shows, and attended trucker festivals. Service utilization by truckers in the 12 months prior to the survey was assessed using the following measures: percentage of truckers who received health cards/condoms/one-one counseling, attended health camps, and were referred to an integrated counselling and testing center or detoxification center. All these measures were coded as “1” if respondents reported in the affirmative, or else coded as “0”. Three outcome indicators were assessed, ie, awareness of STI-related symptoms, experience of STI-related symptoms in the 12 months prior to the survey, and treatment-seeking from Khushi clinics for STI-related symptoms.
Spontaneous multiple response questions were asked to assess awareness of STI-related symptoms. Responses included commonly occurring STI symptoms among men, such as urethral discharge, genital ulcers, and sores, swelling in the scrotal (groin) area, burning/pain on urination, and inability to retract the foreskin. Respondents answering to any of these symptoms were classified as being aware of STI-related symptoms and coded as “1”, or else considered as not aware of STI symptoms (coded as 0). Respondents were categorized as having experienced STI-related symptoms (coded as 1) if they reported experience of any of the following STI symptoms in the 12 months prior to the survey: urethral discharge, genital ulcers, and sores, swelling in the scrotal (groin) area, burning/pain on urination, and inability to retract the foreskin, or else they were considered not to have experienced any STI symptoms and coded as “0”. Respondents who experienced any STI-related symptoms were asked if they had sought treatment for their symptoms. Responses to this question were multiple, with Khushi clinics as one of the response categories. Respondents who reported seeking treatment from a Khushi clinic provider were considered to have sought treatment from a Khushi clinic and coded as “1”.
Statistical analyses
Program monitoring data are presented either in terms of absolute numbers or a percentage relative to a base indicator. Bivariate and multivariate analyses were used to demonstrate the changes in program exposure, behavioral outcome, and service utilization from two rounds of behavioral tracking survey data. A pooled data set of round 1 and round 2 of the behavioral tracking survey was prepared, with an indicator variable indicating the survey round (round 1, 0; round 2, 1). Multiple logistic regression models were fitted, with the survey round as the key independent variable and exposure to communication activities and service utilization as the dependent variables. Multivariate models were adjusted for age, education, marital status, duration of trucking industry, and route category where the trucker operates, and the results are presented in terms of adjusted odds ratios (AOR) with the corresponding 95% confidence interval (CI). All bivariate and multivariate analyses were carried out using STATA version 12 (StataCorp, College Station, TX, USA).
Results
The intervention was started with eleven sites in 2004 and scaled up to 34 sites, with one clinic per site, in 2005 (). With the redesign of the program, the number of intervention sites was reduced to 17, with at least two clinics per site after the redesign process. Post redesign, the number of truckers contacted per month per site increased multi-fold each year. The proportion of truckers using clinical services also increased; initially, only about two-thirds of the individuals were truckers, which improved significantly after the redesign of intervention. Those reporting STI-related symptoms declined over the years from 44% in 2004 to 16% in 2010. A considerable increase in the number of condoms socially marketed was also noted (eight condoms sold per trucker in 2004 to 53 condoms sold per trucker in 2010).
Table 2 Program exposure and service utilization as observed in the program monitoring data, 2004–2010
The independent cross-sectional surveys support the observations made from the program monitoring data (). There was a seven-fold increase in visitors to Khushi clinics in the 12 months between January 2008 and July 2009 (21% to 63%, AOR 6.7, 95% CI 5.6–7.9). Exposure to different communication activities increased multi-fold from round 1 to round 2, including attendance at street plays (10% to 56%, AOR 11.3, 95% CI 9.2–14.0), participation in health exhibitions (6% to 35%, AOR 8.6, 95% CI 6.7–11.1), and participation in film shows (4% to 24%, AOR 7.8, 95% CI 5.8–10.6). A significant improvement was also observed in service utilization by truckers. More than one-tenth (13%) had received a health card at the time of the round 1 survey compared with more than one-fifth (22%) in round 2, indicating a two-fold increase between the survey rounds (AOR 1.8, 95% CI 1.5–2.2). Improvements in service utilization from round 1 to round 2 were also noted with regard to receipt of condoms from the program (13% to 22%, AOR 1.8, 95% CI 1.5–2.2) and attendance at one-one counseling sessions (15% to 21%, AOR 1.5, 95% CI 1.3–1.9).
Table 3 Change in level of program exposure and service utilization among long-distance truck drivers from January 2008 to July 2009, according to behavioral tracking surveys
suggests that the truckers surveyed in round 2 were 20% more likely to experience STI-related symptoms as compared with those in round 1 (27% versus 22%, AOR 1.2, 95% CI 1.0–1.5). During the two rounds of the survey, treatment-seeking from Khushi clinics for STI-related problems increased about six times from 16% in round 1 to 50% in round 2 (AOR 5.6, 95% CI 3.8–8.2).
Table 4 Change in level of awareness of STI-related symptoms, experience of STI-related symptoms, and treatment-seeking behavior from January 2008 to July 2009
Discussion
This redesigned intervention strategy has demonstrated an increase in program coverage and service utilization among long-distance truckers even though the number of intervening sites was reduced by half. The program’s redesigned approach offered services at selected trans-shipment locations, supported by uniform branding of clinical services and innovative communication activities. The two independent cross-sectional surveys supported by program monitoring data documented a multi-fold increase in program coverage and service utilization among truckers. The study findings on program exposure are supported by an independent evaluation of trucker programs in India, which indicates that truckers’ exposure to HIV prevention intervention increased from 14% in 2007 to 30% in 2009.Citation7 Another assessment of a truckers program in India suggests that communication activities such as mid-media and interpersonal communication used in the Kavach program contributed significantly to increased condom use with paid and unpaid female sexual partners.Citation22 The findings from this study corroborated by other studies suggest that optimum placement of service at few locations can yield better outcomes in HIV prevention programs among truckers.
This redesigned intervention demonstrates that successful business models can be adopted for health service delivery. Influenced by the business franchise model of McDonald’s,Citation20,Citation21 the Khushi clinics were branded with a uniform look and service across trans-shipment locations. Empirical evidence suggests that franchise models have the potential to increase access to services and ensure standardized quality of services through a recognized brand.Citation23–Citation26 Franchising models of clinics have been successfully adopted to provide reproductive health and family planning services.Citation23,Citation25,Citation26 A social franchising clinic model in Vietnam to provide reproductive health and family planning services demonstrated that such a social franchise model can help to increase the use of reproductive health and family planning services in smaller public sector clinics.Citation23 However, the use of franchise models in HIV prevention programs is rare. The branding of Khushi clinics in terms of uniform look and color helped truckers to identify these clinics in different intervention locations. Moreover, this strategy was very effective in drawing the attention of truckers given the low literacy and high frequency of mobility. Although the findings suggest that the franchise model of service provision can be highly successful in HIV prevention programs, it requires extensive advertising through innovative communication channels. Further, a similar approach has been used to provide STI services to female sex workers and clients of female sex workers in different parts of India. The findings of this intervention can serve as a stepping stone in evaluation of such interventions in the future. Moreover, providing STI services through a chain of uniform STI clinics may be highly successful among migrants in India, who are now being recognized as a major source of HIV infection transmission from destination areas to source areas.Citation27
The branding of Khushi clinic resulted in a sharp increase in the utilization of clinical services by truckers over the years, which is evident from both the program monitoring and survey data. In addition to the uniform look and feel of Khushi clinics, packaging of these clinics as general health clinics helped in reducing the stigma associated with STI clinics and could also have translated into increased clinical service utilization. The decision to establish clinics near brokers’ premises also resulted in an increase in the number of truckers accessing clinic services. The steady increase in the volume of truckers visiting clinics over the years indicates that truckers are strongly motivated to visit these clinics due to the quality of services being offered. Moreover, the existence of strong social networking among individuals would also have contributed to increased clinic outflow over the years.Citation23
Consistent with the increase in program coverage over the years, the two rounds of cross-sectional surveys also demonstrated a significant improvement in truckers’ participation in different communication activities, which is most likely due to systematic peer outreach activity in conjunction with a surround sound communication strategy. The use of peer educators has been demonstrated to be successful in previous interventions for truckers in India.Citation14–Citation17 Discussion between peer educators and fellow truckers helped in understanding the attitude and expectation of truckers towards STI/HIV services offered through the Kavach program. The concerns expressed in those discussions were addressed and helped in designing innovative communication materials according to the needs of the trucking community. One of the challenges faced by the program was the high turnover rate of peer educators; in cases where peer educators dropped out, new peer educators were immediately recruited and provided with the necessary training. Further, the increase in exposure to communication activities resulted in improved safe sex behavior.Citation22
The trend emerging from the program monitoring data suggests that there was a significant increase in program coverage and service utilization from 2004 to 2005. This is due to the increase in number of intervention sites which went from 11 in 2004 to 34 in 2005. However, with the redesigned strategy in place since 2006, most service utilization indicators have showed improvement or remained stable over the years. Further, the redesigned strategy ensured higher usage of services by trucker population rather than by individuals from the nontrucking community as was the situation prior to 2006. These trends suggest that approaches used in the redesigned intervention can be effective for increasing service utilization among truckers, who are recognized as a highly mobile population group in India and elsewhere.Citation7 Further, the services offered in Kavach program were aligned to guidelines prescribed by the National AIDS Control Program (NACP). Moreover, there was a change in guidelines for national HIV prevention programs during the intervention period, because there was a transition from NACP phase 2 (2000–2006) to phase 3 (2007–2012). The NACP-2 prioritized STI diagnosis and treatment services whereas in NACP-3 the focus was on referral to integrated counseling and testing centers alongside STI diagnosis and treatment.Citation3 As a result of these policy-level changes, the efforts towards referral to integrated counseling and testing centers was poor prior to 2006, and more intensive efforts were made starting only in 2007. These efforts resulted in a four-fold increase in referral to integrated counseling and testing centers from 2008 to 2009.
The findings of this study should be viewed in the light of certain limitations. The cross-sectional surveys used to assess service utilization were conducted after the redesign of the intervention; hence round 1 of the survey is not a true baseline. However, post hoc comparison with selected indicators for which information was collected prior to the redesign suggests that service utilization was poorer before the redesign, and improvement was significantly associated with the redesign process. For example, only 4% of truckers had visited a clinic in the 12 months prior to redesign compared with 21% and 63%, respectively, in survey round 1 and 2. Further, the intervention had no control group, so one can argue that the changes observed were merely temporal rather an outcome of the intervention. Post hoc analysis suggests that truckers who had never visited Khushi clinics were less likely to be exposed to communication activities and receive program services, indicating the role of the intervention in improving service utilization. There could also be some degree of bias because of use of program monitoring data. In the first year of intervention, although a standardized data collection tool was developed and shared with local nongovernmental organizations, some did not collect data as per the suggested guidelines, resulting in some bias. However, in subsequent years, training was conducted for personnel in charge of monitoring systems at local nongovernmental organizations, which improved data quality.
In summary, adoption of a business franchise model for an HIV prevention program among truckers resulted in better program coverage and utilization of services. Implementing the program among a highly mobile population like truckers in a limited number of high-impact locations in combination with branding and standardization of services could help in saturating the coverage and optimum utilization of available resources. The lessons learnt from this intervention could be extremely useful for HIV prevention programs throughout India and in other geographic settings. Similar franchise models for clinics can be established in HIV prevention programs targeted at migrant populations. Male migrants make both interstate and intrastate moves, and are prone to negative health effects, including STIs, in their destination areas. Establishing clinics with a uniform look and services will enable migrants to locate and access these clinics easily. Further, a consolidated national presence through network clinics and an integrated approach to programming rather than a stand-alone approach are crucial for maintaining sustained engagement with mobile populations, such as truckers and migrants.
Acknowledgment
This paper was written as part of the Knowledge Network Project of the Population Council, which is a grantee of the Bill and Melinda Gates Foundation through Avahan, its India AIDS initiative. The views expressed herein are those of the authors and do not necessarily reflect the official policy or position of the Bill and Melinda Gates Foundation or Avahan. We are grateful to the National AIDS Control Organization for providing the necessary guidelines on aspects of HIV prevention among truckers in India.
Disclosure
The authors report no conflicts of interest in this work.
References
- MorrisMPodhisitaCWawerMJHandcockMSBridge populations in the spread of HIV/AIDS in ThailandAIDS19961011126512718883589
- ChandrasekaranPDallabettaGLooVRaoSGayleHAlexanderAContaining HIV/AIDS in India: the unfinished agendaLancet Infect Dis20066850852116870529
- National AIDS Control OrganizationTargeted Interventions for Truckers: Operational GuidelinesNew Delhi, IndiaNational AIDS Control Organization, Minstry of Health and Family Welfare, Government of India2007
- DudeAOrugantiGKumarVMayerKHYeldandiVSchneiderJAHIV infection, genital symptoms and sexual risk behavior among Indian truck drivers from a large transportation company in South IndiaJ Glob Infect Dis200911212820300382
- ManjunathJVThappaDMJaisankarTJSexually transmitted diseases and sexual lifestyles of long-distance truck drivers: a clinico-epidemiologic study in south IndiaInt J STD AIDS200213961261712230925
- PandeyABenaraSKRoyNRisk behaviour, sexually transmitted infections and HIV among long-distance truck drivers: a cross-sectional survey along national highways in IndiaAIDS200822 Suppl 5S81S9019098482
- PandeyAMishraRSahuDHeading towards the Safer Highways: an assessment of the Avahan prevention programme among long distance truck drivers in IndiaBMC Public Health201111 Suppl 6S1522376295
- RaoANagMMishraKDeyASexual behaviour pattern of truck drivers and their helpers in relation to female sex workersIndian J Soc Work1994554603615
- SinghKSinghRRAlderferWHYourkavitchJRomanoKHealthy highways: reducing HIV/AIDS risk for truck driversThe XIV International AIDS ConferenceBarcelona, Spain Abstract TuPeF54512002
- Joint United Nations Programme on HIV/AIDSWorking with Men for HIV Prevention and CareGeneva, SwitzerlandJoint United Nations Programme on HIV/AIDS2001
- World Health OrganizationIntegrating Gender Into HIV/AIDS Programs: A Review PaperGeneva, SwitzerlandDepartment of Gender and Women’s Health, Family and Community Health, World Health Organization2003
- Department for International Development, Family Health InternationalSummary Report: Behavioural Surveillance Survey in Healthy Highways Project, IndiaNew Delhi, IndiaDepartment for International Development, Family Health International2001
- Department for International Development, Family Health InternationalSummary Report: Health Care Provider Survey in Healthy Highways Project, IndiaNew Delhi, IndiaDepartment for International Development, Family Health International2001
- MarckJLong-distance truck drivers’ sexual cultures and attempts to reduce HIV risk behaviour amongst them: a review of the African and Asian literatureCaldwellJCaldwellPAnarfiJResistances to Behavioural Change to Reduce HIV/AIDS Infection in Predominantly Heterosexual Epidemics in Third World CountriesCanberra, AustraliaHealth Transition Centre, National Centre for Epidemiology and Population Health, Australian National University1999
- MajumdarARaoAObstacles encountered in a sexual health intervention programme for truckers: the experience of Bhoruka Public Welfare Trust, IndiaCaldwellJResistances to Behavioural Change to Reduce HIV/AIDS Infection in Predominantly Heterosexual Epidemics in Third World CountriesCanberra, AustraliaHealth Transition Centre, National Centre for Epidemiology and Population Health, Australian National University1999
- RaoKSJyothiGurulakshmiIntervention strategies for reducing HIV risk behaviour among truck drivers in IndiaPaper presented at the Conference on Resistances to Behavioural Change to Reduce HIV/AIDS Infection in Predominantly Heterosexual Epidemics in Third World CountriesCanberra, AustraliaApril 28–30, 1999
- The Synergy Project, Center for Health Education and Research, University of WashingtonPutting On the Brakes: HIV Transmission Along Truck Routes in the Developing WorldSeattle, WAThe Synergy APDIME Toolkit2000
- Bhoruka Public Welfare TrustU-turn: Truckers on East Indian Highways were Unaware of the New Threat, till Uluberia HappenedKolkata, IndiaBhoruka Public Welfare Trust2004
- Bill and Melinda Gates FoundationOff the Beaten Track: Avahan’s Experience in the Business of Prevention among India’s Long-Distance TruckersNew Delhi, IndiaBill and Melinda Gates Foundation2008
- Franchise DirectThe Success of the McDonald’s Franchise2012 Available from: http://www.franchisedirect.com/information/trendsfacts/thesuccessofmcdonalds/8/1111/Accessed July 11, 2012
- RitzerGThe “McDonaldization” of societyJ Am Cult198361100107
- JunejaSRao TirumalasettiVMishraRMSethuSSinghIRImpact of an HIV prevention intervention on condom use among long distance truckers in IndiaAIDS Behav9252012 [Epub ahead of print.]
- NgoADAldenDLPhamVPhanHThe impact of social franchising on the use of reproductive health and family planning services at public commune health stations in VietnamBMC Health Serv Res2010105420187974
- MontaguDFranchising of health services in low-income countriesHealth Policy Plan200217212113012000772
- StephensonRTsuiAOSulzbachSFranchising reproductive health servicesHealth Serv Res2004396 Pt 22053208015544644
- LaVakeSDApplying Social Franchising Techniques to Youth Reproductive Health/HIV ServicesArlington, VAFamily Health International, YouthNet Program2003
- SaggurtiNMahapatraBSabarwalSGhoshSJohriAMale out-migration: a factor for the spread of HIV infection among married men and women in rural IndiaPloS One201279e4322222970120