Abstract
Background
We aimed to assess the relationship between gender and survival among adult patients newly enrolled on antiretroviral therapy (ART) in Uganda. We also specifically examined the role of antenatal services in favoring women’s access to HIV care.
Methods
From an observational cohort study, we assessed survival and used logistic regression and differences in means to compare men and women who did not access care through antenatal services. Differences were assessed on measures of disease progression (WHO stage and CD4 count) and demographic (age, marital status, and education), behavioral (sexual activity, disclosure to partner, and testing), and clinical variables (hepatitis B and C, syphilis, malaria, and anemia). A mediational analysis that considered gender as the initial variable, time to death as the outcome, initial CD4 count as the mediator, and age as a covariate was performed using an accelerated failure time model with a Weibull distribution.
Results
Between 2004 and 2011, a total of 4775 patients initiated ART, and after exclusions 4537 (93.2%) were included in analysis. Men initiating ART were more likely to have a WHO disease stage III or IV (odds ratio: 1.46, 95% confidence interval [CI]: 1.29–1.66), and lower CD4 cell counts compared to women (median baseline CD4 124 cells/mm3, interquartile range [IQR]: 43–205 versus 147 cells/mm3, IQR: 68–212, P-value < 0.0001). Men were at an increased risk of death compared to women (hazard ratio: 1.38, 95% CI: 1.03–1.83). Baseline CD4 cell counts accounted for 43% of the increased risk of death in men (95% CI: 22%–113%). Access to care via antenatal services did not explain differences in outcomes.
Conclusion
In this cohort there is a marked increase in risk of mortality for men and approximately half of it can be attributed to their later engagement in care. More effort is required to engage men in care in a timely manner.
Introduction
The provision of antiretroviral therapy (ART) in sub-Saharan Africa (SSA) has resulted in reduced mortality, morbidity, and an increase in life expectancy.Citation1,Citation2 Despite these successes, approximately 59% of all people in Africa remain without treatment despite being considered eligible.Citation3 Also, for those in care, improvements are required along every step of the care cascade to improve health outcomes for both individuals and the population.Citation4
The first entry point to care is HIV testing, which is often accessed through provider-initiated testing at the health center. In many settings, provider-initiated testing has favored women and children, usually in the antenatal care (ANC) period.Citation5,Citation6 There has been recent growing recognition that men are disadvantaged because no equivalent routine testing opportunity exists for them,Citation7 and this is considered at least partly to account for the fact that men initiate ART later than women,Citation8 and have worse outcomes on antiretroviral therapy compared to women.Citation9–Citation13
In this study, we aimed to determine mortality between sexes after initiation of ART in the greater Kampala area of Uganda. We further sought to determine whether differences in disease progression across the sexes could be explained by differential access to care via ANC services, and estimated how much of the increased risk of mortality in men can be explained by later ART initiation.
Method
Data and study population
All patient data for this study is from the Mildmay Uganda observational cohort (MUg).Citation14 Mildmay is a medical service organization providing ART and other healthcare services to the HIV-positive community in Uganda. The organization opened in 1998 in order to provide palliative outpatient care for people living with HIV/AIDS, and to be a teaching and training center for HIV/AIDS healthcare personnel. This study was restricted to patients who initiated ART between January 2004 and April 2011, were aged 14 years or older at baseline, and had completed the selection form. Selection forms contain baseline data including whether a woman was pregnant or eligible for ART for prevention of mother to child transmission (PMTCT). To the best of our knowledge, selection forms were missing completely at random (ie events leading to missing selection forms are independent of variables of interest). Patient level data are collected on all patients and recorded into a central server.
Outcome measures and prediction variables
The primary outcome was all-cause mortality throughout the study period that ended in October 2011 to ensure that patients had the possibility of at least 6 months of follow-up time. Most deaths were reported by family members or recorded at hospital locations. Time was measured beginning at first ART date and ending at either date of death, 6 months after last visit, or at end of study period, respectively. Follow-up time beyond the last visit is justified by the fact that death is externally observed. The Mildmay program engages community adherence supporters to assist with patient retention in care. The principal explanatory variables of interest were sex, baseline CD4-cell counts and World Health Organization disease stage. Baseline CD4 cell counts were obtained within 6 months before starting ART. During the observation period, the Ugandan national guidelines stipulated that patients were considered eligible for ART if they had a CD4 count ≤200 cells/mm3 (this was changed to ≤350 cells/mm3 in 2012). We also measured demographic (age, marital status, and education), behavioral (sexual activity, disclosure to partner, and testing), and clinical variables (hepatitis B and C, syphilis, malaria, and anemia). Women were deemed to be in antenatal care if they reported either being pregnant at baseline or being PMTCT eligible.
Analyses
To determine the existence of any important differences between men and women with respect to demographic, behavioral, and clinical variables in the full cohort, we used Fisher’s exact and Wilcoxon Rank Sum tests. Logistic regression and confidence intervals for difference in means were used to estimate the differences in disease progression, as defined by WHO disease stage and baseline CD4 cell counts, in men and women. These were applied to samples with and without women accessing care through ANC. We used Kaplan–Meier survival curves to demonstrate mortality over time in both the full and restricted cohorts. We applied a weighted analysis whereby 30% of patients lost to follow-up were assumed to be dead, weighted by baseline CD4 and age, as suggested by Egger et al.Citation15
Mediational modeling was conducted to estimate the proportion of increased risk of mortality in men attributable to later ART initiationCitation16 using recently developed methods for survival analysis.Citation17–Citation19 Mediator variables are distinguished from confounders in that they lie on the causal pathway. displays the pathways from initial variable to outcome. The effect of the initial variable (gender) summed across all pathways is its total effect. As shown in , the total effect can be partitioned into the direct effect and the indirect effect. As with any model, the model assumptions must be met and, particularly for models considering causal pathways, it is important that confounding be fully controlled. The ratio of indirect to total effects is the proportion of the effect attributable to the mediator. In this analysis we considered age as a confounder, gender as the initial variable, baseline CD4 as the mediator, and survival as the outcome.
Figure 1 Illustration of causal pathways.
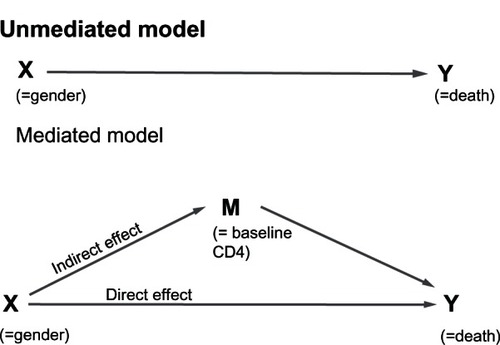
We opted for the “product method”Citation16 of estimating the indirect effect which required the construction of a linear regression model for baseline CD4 and an accelerated failure time model with a Weibull distribution using gender, baseline CD4 cell count, and age. The direct effect is immediately available from the survival model. Full details on the indirect effect estimation and the assumptions required for this model are available in the Appendix. Confidence intervals for the indirect and total effects as well as their quotient (the proportion of effect explained by CD4) were obtained by bootstrapping.Citation19–Citation22 All analyses were done in SAS version 9.3 (SAS Institute Inc, Cary, NC, USA) and R version 2.15 (Vienna, Austria).
Ethical approval
This study received ethical approval from the institutional review boards of the University of Ottawa and Mildmay Uganda. The Uganda National Council for Science and Technology provided additional approval.
Results
In total, 4775 patients aged 14 years or older initiated ART between January 2004 and April 2011. The median age was 33 (interquartile range [IQR] 27–39), and 1676 (35.1%) were men. During this time period there were 200 deaths over a median follow-up time of 3.25 years (IQR 2.50–4.25); 135 patients were lost to follow-up (42 males and 93 females). summarizes the comparison of men to women. Men tended to be older, were more likely to be married and sexually active, tended to be better educated, more likely to disclose their status to their partners, and more likely to be hepatitis B positive (odds ratio [OR]: 1.42, 95% confidence interval [CI]: 1.10 – 1.85). in the Appendix summarizes the comparison between patients according to vital status.
Table A1 A comparison of demographic, behavioral, and clinical characteristics across survival groups
Table 1 A comparison of demographic, behavioral, and clinical characteristics in men and women
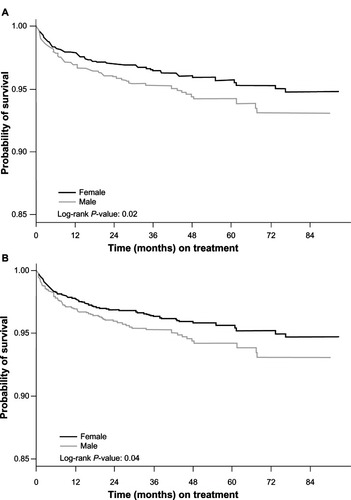
There were 84/1676 (5.0%) deaths among men and 116/3099 (3.7%) among women. When analyzing all patients, the P-value for the log-rank test was 0.02 indicating a higher rate of death among men (, Panel A). When we restricted this to the cohort involving only women who accessed care outside ANC services, the P-value for the log-rank test was similar at 0.04 (, Panel B).
Figure 2 Kaplan–Meier survival curves for full cohort (Panel A), and Kaplan–Meier survival curves for restricted cohort (Panel B).
Similarly, 42% of men compared to 32% of women presented for ART at WHO stage 3 or 4 (OR: 1.46; 95% CI: 1.29–1.66) and this did not change much when ANC cases were removed (OR: 1.54; 95% CI: 1.37–1.75). The median baseline CD4 cell count was lower in men than women. As shown in , the difference in CD4 cell count was only slightly larger, 23 versus 25, when ANC cases were included.
Table 2 Comparing disease progression at baseline between men and women with adjustments for antenatal care
The Weibull survival model shows that in univariate analysis, gender has a significant effect on survival (hazard ratio [HR]: 1.38; 95% CI: 1.03–1.83), but in the presence of the mediators and confounders its effect is no longer significant (adjusted hazard ratio: 1.20; 95% CI: 0.95–1.64; ). The scale coefficient of 1.87 indicates that the hazard of death is declining with time, in keeping with the fact that the majority of the deaths occur within months of initiating ART.Citation10 presents the partitioning of the effect of gender into direct and indirect effects. Approximately 43% (95% CI: 22%–113%) of the additional deaths seen in men are attributable to their lower CD4 cell counts at baseline (results for reduced cohort shown in ). A sensitivity analysis restricted to the sample of those not accessing care through ANC, is presented in in the Appendix. The results were very similar.
Table A2 Partitioning the effect of gender through the Weibull model for all four cases analyzed
Table A3 Survival analysis using an Accelerated Failure Time model with a Weibull distribution (sensitivity analyses)
Table 3 Survival analysis using an Accelerated Failure Time model with a Weibull distribution
Table 4 Partitioning the effect of gender through the Weibull model
When we examined whether single men had differing baseline risk, according to baseline CD4, compared with other groups, we found that single men had significantly lower CD4 (median 99, IQR 30–190) than married men (120, IQR 48–199) [P = 0.03] and compared to single women (144, IQR 68–209) [P < 0.0001].
Discussion
Although the international HIV/AIDS community has placed a particular emphasis on targeted ART of female patients, there is emerging evidence that less men engage in care for HIV/AIDS in SSA, and have less favorable outcomes. A proposed reason for this inconsistency is that antenatal care provides a platform through which women can access care more frequently and earlier in their disease progression.Citation23 Our study found that men had an increased risk of death and nearly half the additional deaths appear to be attributable to delayed engagement in care. In the multivariable model, we divided the effect of gender into the direct effect and the indirect effect (effect due to CD4 at baseline). Therefore, the fact that gender is not significant in the multivariable model, implies that the increased risk observed in men is not due to their gender, but mostly due to their lower baseline CD4 cell counts. ANC accounted for only a small fraction of this inconsistency. A sustained effort to reduce this discrepancy could have an important impact both on the individuals and the community.
Our study has several strengths and limitations. Our study had low rates of death and low rates of loss to follow-up. The Mildmay program puts emphasis on community care that may explain the high retention to care, an observation mirrored in other community-based care programs.Citation24 Although there is accumulating evidence that men across SSA are at increased risk of morbidity and mortality in comparison to women,Citation25 our study was restricted to a single cohort in Uganda. Our sample is not random and may not be representative. Our bivariate analyses reveal that our cohort has a relatively higher number of married men, suggesting that the engagement of women has led them to bring their husbands into care. Consequently the differences in disease progression reported in this cohort may underestimate the discrepancy in the community.
The role of antenatal care in the discrepancy between how men and women seek access to healthcare is often acknowledged, but seldom analyzed in detail. Our study clearly shows the existence of other, more important factors at the source of the divide. It is well known that initiating care at a lower CD4 cell count increases the risk of mortality.Citation26 Therefore it is not surprising that our results show that the increased mortality in men can in part be explained by later initiation. Nonetheless, by quantifying the proportion of increased mortality attributable to later initiation we have highlighted the urgency of increasing engagement to care.
SSA continues to be the epicenter of the HIV/AIDS pandemic. Engagement in care remains an important challenge in the fight against HIV. Men are seldom targeted because they do not fall into our conventional definitions of vulnerability and marginality.Citation27 On the contrary, in general, men are recognized for having poor health-seeking behavior, so that efforts to engage them are even more critical.
Efforts to engage men do exist. In Swaziland, the Ministry of Health has initiated men’s health days.Citation28 Studies have shown that home-based testing programs are allowing men to test earlier, giving them a chance to engage in a timely fashion.Citation29 Encouraging men to accompany women in antenatal care, as recommended by WHO in Uganda, has had some success in Rwanda and may have a role in other settings,Citation30 although this would only target couples with active relationships. Circumcision clinics may represent a one-time testing opportunity for single men. The implementation of programs to encourage further participation by men in care is a difficult task, but earlier recruitment into care remains the best method to align the health outcomes of men with those of women.
Conclusion
A growing number of studies are reporting that among HIV-positive individuals on ART in SSA, men tend to be at higher risk of death as was the case in our cohort. Little has been done to determine the underlying causes that are crucial to making changes to the health systems that create them. Our study found that among the leading causes, and quite possibly the leading cause, is the lower CD4 cell counts at which men on average present themselves for ART initiation. Targeted campaigns need to continue to be evaluated, to reduce the gender disparity and improve testing, linkage to care, and ultimately health outcomes for men. This study can contribute to the growing body of evidence designed to inform evidence-based policy, to reduce barriers to healthcare experienced by men. Finally, antenatal care programs are a key difference in how men and women access care and are often cited as a plausible cause for observed differences in health outcomes, yet this difference did not appear to have a large impact in our cohort. Our findings suggest that further investigation is needed as access to care through antenatal care may play a more muted role than believed in explaining the differences in ART uptake between men and women.
Author contributions
The study design was conceived by SK, NF, EJM, and ED. Data were acquired by SK, MN, DM, MO, MK, WM, SY and AF. The analyses were conducted by SK, AF, and EJM. SK wrote the manuscript and all contributed to writing. The final manuscript was approved by all.
Funding
The Canadian Institutes of Health Research (CIHR) provided funding for this analysis. No funding agency has seen this study.
Disclosure
No authors have any competing interests.
References
- FordNCalmyAMillsEJThe first decade of antiretroviral therapy in AfricaGlobal Health201173321958478
- MillsEJBakandaCBirungiJLife expectancy of persons receiving combination antiretroviral therapy in low-income countries: a cohort analysis from UgandaAnn Intern Med201115520921621768555
- WHOUNAIDSUNICEFGlobal HIV/AIDS Response: Epidemic Update and Health Sector Progress Towards Universal AccessGeneva, SwitzerlandWorld Health Organization2011
- MillsEJFordNHome-based HIV counseling and testing as a gateway to earlier initiation of antiretroviral therapyClin Infect Dis20125428228422156849
- ExnerTGardosPSealDEhrhadrtAHIV sexual risk interventions with hetersexual men: the forgotten groupAIDS Behaviour19993347358
- HigginsJAHoffmanSDworkinSLRethinking gender, heterosexual men, and women’s vulnerability to HIV/AIDSAm J Public Health201010043544520075321
- MillsEJFordNMugyenyiPExpanding HIV care in Africa: making men matterLancet200937427527619632481
- MillsEJBakandaCBirungiJMale gender predicts mortality in a large cohort of patients receiving antiretroviral therapy in UgandaJ Int AIDS Soc2011145222050673
- BraitsteinPBoulleANashDGender and the use of antiretroviral treatment in resource-constrained settings: findings from a multicenter collaborationJ Womens Health (Larchmt)200817475518240981
- BraitsteinPBrinkhofMWDabisFMortality of HIV-1-infected patients in the first year of antiretroviral therapy: comparison between low-income and high-income countriesLancet200636781782416530575
- DruytsEDybulMKantersSMale gender and the risk of mortality among individuals enrolled in antiretroviral treatment programs in Africa: a systematic review and meta-analysisAIDS20132741742522948271
- JohannessenAAre men the losers of the antiretroviral treatment scale-up?AIDS2011251225122621593620
- MayMBoulleAPhiriSPrognosis of patients with HIV-1 infection starting antiretroviral therapy in sub-Saharan Africa: a collaborative analysis of scale-up programmesLancet201037644945720638120
- FunkAKantersSNansubugaMCohort Profile: The MUg Observational CohortInt J Epidemiol20124161594159423171870
- EggerMSpycherBDSidleJCorrecting mortality for loss to follow-up: a nomogram applied to antiretroviral treatment programmes in sub-Saharan AfricaPLoS Med20118e100039021267057
- BaronRMKennyDAThe moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerationsJ Pers Soc Psychol198651117311823806354
- LangeTHansenJVDirect and indirect effects in a survival contextEpidemiology20112257558121552129
- TeinJ-YMacKinnonDYanaiHEstimating mediated effects with survival dataNew Developments on PsychometricsTokyoSpringer-Verlag Tokyo Inc2003405412
- VanderWeeleTJCausal mediation analysis with survival dataEpidemiology20112258258521642779
- EfronBBootstrap methods: another look at the jackknifeAnnals of Statistics19797126
- EfronBRJTAn Introduction to the BootstrapNew YorkChapman and Hall1993
- VanderweeleTJVansteelandtSOdds ratios for mediation analysis for a dichotomous outcomeAm J Epidemiol20101721339134821036955
- KuwaneBAppiahKFelixMGrantAChurchyardGExpanding HIV care in Africa: making men matter in JohannesburgLancet2009374132919837252
- DecrooTTelferBBiotMDistribution of antiretroviral treatment through self-forming groups of patients in Tete province, MozambiqueJ Acquir Immune Defic Syndr201156e39e4421084990
- DruytsEDybulMKantersSMale gender and the risk of mortality among individuals enrolled in antiretroviral treatment programs in Africa: A systematic review and meta-analysisAIDS201327341742522948271
- MillsEJBakandaCBirungiJYayaSFordNTASO-CAN Writing GroupThe prognostic value of baseline CD4 cell count beyond 6 months of antiretroviral therapy in HIV positive patients in UgandaAIDS2012261425142922526520
- MillsEJBeyrerCBirungiJDybulMREngaging men in prevention and care for HIV/AIDS in AfricaPLoS Med20129e100116722346735
- Swaziland US Global Health Initiative Country Strategy: Government of the Kingdom of Swaziland – United States Government2102012
- WachiraJKimaiyoSNdegeSMamlinJBraitsteinPWhat is the impact of home-based HIV counseling and testing on the clinical status of newly enrolled adults in a large HIV care program in Western Kenya?Clin Infect Dis20125427528122156847
- AsiimweAHIV Treatment for prevention: a view from the ground20th Conference on Retroviruses and Opportunistic Infections (CROI)March 5–8, 2012Atlanta, Ga, USA
- RobinsJMGreenlandSIdentifiability and exchangeability for direct and indirect effectsEpidemiology1992321431551576220
- PearlJDirect and indirect effectsSeventeenth Conference on Uncertainty and Artificial Intelligence2001San Francisco
Appendix
The “product method” of estimating the indirect effect requires the construction of a linear regression model for baseline CD4 cell count and an accelerated failure time model with a Weibull distribution using gender, baseline CD4 cell count and age. The baseline CD4 cell count was transformed using a fourth root in order to meet the conditions required for linear regression. Let β1 be the coefficient of gender in this model. The Weibull model was chosen over Cox proportional-hazards regression because the latter does not allow for the partitioning of a direct and indirect effect. The conditions required for the Weibull model were also verified and met. The survival model was fit using gender, baseline CD4 cell count, and age. The coefficient for gender is the direct effect and a confidence interval is readily available. The indirect effect is estimated by the product β1θ2, where θ2 is the coefficient for baseline CD4 cell count. This approach to mediational modeling is built upon the counterfactual paradigm as established by Robins and GreenlandCitation31 and more directly by Pearl.Citation32 Four assumptions are listed as requirements to these methods: (i) no confounding for the exposure-outcome relationship, (ii) no confounding for the mediator-outcome relationship, (iii) no confounding for the exposure-mediator relationship, and (iv) no mediator-outcome confounder that is an effect of the exposure. As opposed to studies where the exposure is a treatment, in this study there is no interest in estimating the direct effect of gender on survival. The total effect of gender is comprised of many pathways including: disease progression at initiation, retention to care, and adherence to treatment. The objective here is to tease out the proportion of total effect on the baseline CD4 pathway. As such, some confounders to the exposure-outcome relationship were not considered. Age is always a confounder when survival is the outcome and was included in all models. To the best of our knowledge, there are no reported confounders to the relationship between baseline CD4 and survival in the literature. Thus, assumptions (ii) and (iii) seem fair. Given that the mediator is a baseline variable, assumption (iv) should also be met.