
Abstract
Long-distance truckers (LDTDs) are vulnerable to human immunodeficiency virus infection and other sexually transmitted infections due to the nature of their work, working environment, and frequent mobility. This paper examines and comments on the health care coverage provisioned under “Kavach” Project. Data from the Integrated Behavioural and Biological Survey, National Highway gathered from 2,066 LDTDs in Round 1 and 2,085 LDTDs in Round 2, who traveled in four extreme road corridors travelled by LDTDs in India, were used for analysis. Analysis reveals that service capacity in terms of socially marketed condoms per thousand LDTDs has increased from Round 1 to Round 2 (4,430 to 6,876, respectively). Accessibility coverage in terms of knowledge about the Khushi clinic has significantly decreased between Rounds 1 and 2 (60.9% to 54.6%; P<0.001). Acceptability coverage has increased between the two rounds (13.8% to 50.6%; P<0.001). Contact coverage has also increased between the rounds (12.7% to 22.3%; P<0.001). Effectiveness coverage for preventive and curative care has also increased significantly. This paper comments on the gaps in accessibility and acceptability of health care coverage and emphasizes the need for further studies to assess the contextual factors that influence the effectiveness and efficiency of interventions designed to address access barriers and to identify what combination of interventions may generate the best possible outcome.
Introduction
Workers in the transport sector are vulnerable to human immunodeficiency virus (HIV) infection and other sexually transmitted infections (STIs) due to the nature of their occupation, difficult work environment, and poor economic and living conditions.Citation1 Studies have reported the spread of HIV along major truck routes, and the crucial role played by long-distance truckers (LDTDs) (LDTDs include truck drivers and their helpers traveling 800 km or more in a single direction) in carrying HIV infection from one place to another and transmitting infection from high-risk populations (high-risk population includes female sex workers, men who have sex with men, and injecting drug users) to low-risk populations (low-risk population primarily includes spouses of migrant/mobile population).Citation2–Citation4 Multiple sex partners, ignorance about the use of condoms, and inconsistent or no condom use during sexual acts are commonly reported behavior patterns among LDTDs.Citation5–Citation9 In addition, LDTDs lack complete and correct information about HIV and other STIs, resulting in low self-perceived risk of HIV infection and other STIs.Citation10–Citation12
Due to frequent mobility, LDTDs lack access to general health care, and low contact with HIV intervention programs restricts their demand in seeking health care in general and sexual and reproductive health care in particular.Citation13–Citation15 Labeling of truck drivers as a high-risk group has marginalized them socially, thus affecting their willingness to access sexual and reproductive health services, and accordingly, their health needs remain uncared for.Citation16–Citation18 Intensive exposure to interventions may promote better access to health care, leading to safer sexual behavior and limiting the incidence of STIs and HIV infection.Citation5,Citation6,Citation15 Various studies have reiterated the need for focused interventions among this group, such as intensive engagements, community mobilization, social vaccine (involves disseminating information and awareness regarding safer sexual behavior, 100% condom use, and behavior change communication), and non-governmental organization sector facilitations.Citation6,Citation19–Citation21
There are approximately 5–6 million truck drivers and their helpers in India.Citation22 Of these, almost, 3–3.5 million are LDTDs and of them, nearly a third (36%) are clients of commercial sex workers.Citation3,Citation23,Citation24 HIV prevalence among truckers in India is more than 1% (1.48%).Citation25 Moreover, a high HIV prevalence is reported among antenatal clinic attendees whose spouses are truck drivers/helpers (1.14% and 0.74% in urban and rural India, respectively).Citation25 High HIV prevalence is also reported among STI patients who are truck drivers (3.6% and 5.9% in urban and rural areas, respectively).Citation25 Nationally, a variety of interventions have been initiated to reduce HIV prevalence among this group. The United Kingdom Department for International Development (DFID) commissioned the “Healthy Highways” program in 1995 as a consolidated national program, which was launched in 1996 across 200 sites spread over 19 states in India.Citation5,Citation26 The intervention sites were either trans-shipment locations (TSLs) or roadside cafes along the highway.Citation26 Likewise, in the late 1990s, the Bhoruka Public Welfare Trust established “free tea parlors” at major truck halt points where truckers were encouraged to utilize STI clinic services.Citation5 The major focus of these programs and interventions has been promotion of consistent condom use and behavior change communication among this vulnerable group.Citation26,Citation27
The success or failure of any health care intervention depends on various demand- and supply-side factors. The success of a health care service or intervention is measured by the ability of the service to interact with the people that it covers (target population), and to successfully convert intention into action to make the intervention truly successful.Citation28 Therefore, it is important for the executing organizations/agencies/government to pay attention to the entire process of access to health care to ensure an effective service delivery to vulnerable groups.Citation29
In this paper, an attempt is made to investigate various stages of health care coverage, health care provisions/entitlements, and use of health care services/benefits by LDTDs, with reference to the structure inferred by Tanahashi (1978). Given the framework of health care coverage and its evaluation,Citation28 the paper comments on the gaps/bottlenecks (demand- and supply-side) that may have influenced the ease of use/access to health care services, provisioned under the Kavach project funded by the Bill and Melinda Gates Foundation (BMGF) under the Avahan India AIDS (acquired immunodeficiency syndrome) Initiative.Citation26
Access to health care coverage
Access to health care coverage is a complex concept to characterize. It includes different dimensions of effective service delivery, extending from the availability to an effective utilization of service by the target population. If health services are to be utilized, they must be available, accessible, and affordable. Tanahashi mentioned different stages for the measurement of health care coverage, which are vital conditions for provisioning the service. Assessment of the coverage can enable health system management to recognize the issues in the operation of the services, to analyze the constraining components for these issues, and to select measures for service improvement. Tanahashi described five coverage or access issues that encourage/hinder an individual’s use of health care services (availability, accessibility, acceptability, contact, and effectiveness coverage).Citation28
Availability coverage refers to the availability of a service to cover the health needs of the target group measured either in terms of the infrastructure or availability of manpower, drugs, and supplies. It measures the service capacity. The health services should be located within a reasonable reach of the people, ie, physical location of the health facility. Location of service defines the accessibility coverage. Once accessibility is ensured, service usage is assessed by the number of individuals who are willing to use it, ie, the service should be acceptable in the socioeconomic and cultural setup of the target community. Contact coverage estimates the number of individuals in the target population who have reached the facility at their time of requirement. Effectiveness coverage measures the proportion of the target population that has actually used the services. This coverage assesses the effectiveness of the intervention in providing a valid solution/valid treatment for the target population.Citation28
Using the above analytical framework, an attempt is made in this paper to assess the health care coverage of Khushi clinics among LDTDs. Khushi clinics were established at identified trans-shipment sites to provide LDTDs access to promotive, preventive, and curative services to meet their health needs.Citation30
Kavach project–Khushi clinics
With the support of the Avahan India AIDS initiative of BMGF, Transport Corporation of India Foundation (TCIF) launched project Kavach (Kavach means “shield”) in 2003. The project was aimed at reaching the maximum number of LDTDs in the four main corridors to reduce the spread of HIV and other STIs among the mobile truckers.Citation30,Citation31 The project provided promotive, preventive, and clinical services through Khushi clinics (Khushi means “happiness”) located at 17 major truckers’ halt points (total numbers of clinics have been reduced lately) in nine states in India.Citation5,Citation31 The Kavach project was initiated at 36 TSLs in India covering major national highways in four corridors, ie, the North–West (NW), North–East (NE), North–South (NS), and South–East (SE) corridors. However, program monitoring data in the first 18 months showed low service utilization by the truckers. Hence, the program was redesigned in 2006 by selecting 17 (15 TSLs and two check posts) for intensive intervention.Citation26 Among these Khushi clinics, Sanjay Gandhi Transport Nagar, Delhi, intercepts LDTDs plying on the NE, NW, and NS corridors; Ghaziabad Transport Nagar, Uttar Pradesh, intercepts truckers plying on the NE, NW, and NS routes; and Neelamangala, Bangalore, intercepts truckers plying on the SE and NS routes. Apart from these intercepting junctions, there were five other clinics established on the NE route (Agra, Kanpur, Varanasi, Jamshedpur, and Dhanbad); four on the NW route (Jaipur transport Nagar in Jaipur, Kalamboli in Mumbai, Nigdi in Pune and Hubali/ Dharwad in Karnataka); three on the SE route (Ichachapuram, Andhra Pradesh; Hyderabad Autonagar, Andhra Pradesh; and Jamsola, Orissa); and two along the NS corridor (Nagpur Pardi with a satellite clinic at Wadi, Maharashtra, and Indore, Madhya Pradesh, respectively). On average, there is a distance of 200–600 km between any two Khushi clinics on the specified corridors. Assuming that the LDTD travels more than 800 km one way (by definition), it may be argued that he may have come across at least one Khushi clinic during the trip. Various events, programs, and sets of interventions (eg, nukkad natak or street corner plays, film shows, exhibitions, Seena Taan ke (bravery award) Bahaduri Puraskar and truckers’ utsav (truckers’ festival), free consultation, social marketing of condoms, various outreach activities, peer educators, etc) were launched under the intervention. The intervention aimed at raising self-esteem among LDTDs through communication, eg, trained outreach workers accepting a lift along the highways to discuss general health and raise awareness regarding Khushi clinics; promoting safer sexual conduct, eg, promoting consistent condom use and counseling; and positioning Khushi clinics as solution providers, eg, as health clinics for all LDTDs’ health needs.Citation30
Material and methods
The data used to assess the health care coverage at Khushi clinics under the Tanahashi analytical framework were drawn from two rounds of Integrated Behavioural and Biological Assessment, National Highway (IBBA-NH) survey. The IBBA-NH survey was conducted on the four defined route categories NE, NS, NW, and SE, where the Avahan program operated. The route categories were the extreme road corridors travelled by LDTDs.
Survey sites
TSLs were selected as study locales. In Round 1, seven trans-shipment areas (Sanjay Gandhi Transport Nagar (SGTN), New Delhi; Ghaziabad Transport Nagar, Uttar Pradesh; Kalamboli, Mumbai; Narol Chowkdi, Ahmedabad; Gandhidham, Kandla; Neelamangala, Bangalore; and Territy bazar, Kolkata) and in Round 2, six trans-shipment areas (except Kandala) were selected. In the second round of the survey, Kandala was dropped as only 46 interviews had been conducted in Round 1, and it was not logistically and technically efficient to conduct a survey there again.Citation31
Respondents
LDTDs were the respondents in both rounds of the survey. An LDTD was defined as a trucker who takes a consignment from one place to another destination located along the national highways and who travels more than 800 km one-way before returning back to the place of origin.
Sample size estimation
Two stage time, location cluster sampling approach in which trans-shipment establishments as primary sampling unit (PSU) and truck drivers as the secondary sampling unit was used, to draw a representative sample in both rounds. PSU in IBBA-NH had both a location as well as time dimension. The location dimension was taken as trans-shipment establishments and the time dimension was taken as 1 day (ie, 24 hours). The PSUs were selected at the first stage by probability proportional to size methodology followed by random selection of LDTDs (the respondents of the study) in the second stage. A total of 2,066 LDTDs in Round 1 and 2,085 LDTDs in Round 2 were interviewed.Citation31 The data were collected from June 2007 to September 2007 for Round 1 and from September 2009 to January 2010 for Round 2. Detailed methodology is explained elsewhere.Citation31
Data instruments
Data were collected from a well-designed, structured interview schedule in both rounds of the survey. Information related to socio-demographic profiles of LDTDs, work and mobility, sexual behavior with different sex partners, knowledge about HIV and other STIs, and exposure to interventions were collected. In addition, behavioural aspects for biological assessment, and blood and urine samples of consenting LDTDs were collected for estimating the prevalence of HIV and other STIs.
Ethical approval
Clearance for the IBBA-NH survey was obtained from the Health Ministry Screening Committee (HMSC), Government of India. The IBBA-NH protocol was approved by the Scientific Advisory Committee (SAC) of the National AIDS Research Institute (NARI) and the Protection of Human Subjects Committee (PHSC) of Family Health International (FHI). Ethical approval for IBBA-NH was obtained from Scientific Advisory Committee (SAC) of the National Institute of Medical Science (NIMS), which had additionally reviewed and approved the protocol, consent forms, study instruments, standard operating procedures, and field manuals.Citation31
Framework for analysis
With the given information set and the flexibility in the definition of coverage, according to the Tanahashi framework for health care coverage,Citation28 a matrix () was used to characterize the indicators used as a part of this paper. The Tanahashi framework explains five coverages and indicators, which define service delivery and access to health care coverage. Without the program information, it is difficult to measure service capacity and availability coverage. For the purpose of this paper, it is assumed that the service is available for all LDTDs involved in the IBBA-NH survey (as the intervention was expected to reach about 1.4 million truckers). However, an attempt is made to estimate only a few indicators of service capacity, given the aggregate data in the published literature related to the intervention. With the limited information in the IBBA-NH survey, accessibility coverage is difficult to measure in terms of physical location of the health care service. Accessibility coverage is characterized as “accessibility of information,” which may influence usage considerably. It is assumed that LDTDs who have known about Khushi clinic and seen the logo of the Khushi clinic, are aware of the services provided in the clinic, and can access the services. As referred to in various studies, lower levels of awareness may have implications for access to care, and may impact equitable access to services.Citation32,Citation33 Accordingly, awareness and knowledge may be viewed as a fair indicator of accessibility. In the process of service provisioning, association with the Khushi clinic is considered to be an indicator of acceptability. The individuals who have known about the clinic for more than or equal to 6 months are assumed to be connected with the activities of the clinic and hence, fairly accepting of clinic activities. To measure the contact coverage, visits to Khushi clinic (including a visit to the doctor at the clinic, a visit for general ailments, and a visit for STI) are taken as an indicator. The individuals who have gone to the Khushi clinic for any purpose are expected to have effective contact coverage. For effectiveness coverage, two separate measures were used to quantify: 1) preventive and 2) curative care. As the intervention focused on promotive, preventive, and curative care, it bodes well for assessing the effectiveness coverage based on these two measurements. Both responses (spontaneous and aided) in the IBBA-NH survey are used while estimating this coverage. To estimate the different coverage in both rounds, total number of LDTDs interviewed in each round was taken as the denominator.
Table 1 A framework for analysis of access to health care coverage under the Kavach Project, a part of the Avahan India initiative funded by the BMGF
Statistical analysis
Bivariate analysis was used to assess the change in different coverage indicators, to evaluate the impact of intervention. A pooled information set (from Round 1 and Round 2) was generated with required variables from the IBBA-NH survey. Data were presented in percentages/proportions with respect to a base indicator. The chi-square (χ2) test was used to check the statistical strength of the analysis at a 95% confidence interval. Sampling weights were applied accordingly to correct for unequal probabilities of selection.Citation31 All the analyses were carried out using SPSS version 20 (IBM Corporation, Armonk, NY, USA).
Results
It is assumed that each of the LDTDs who responded to the IBBA-NH survey could avail themselves of the services available under the Kavach project. Hence, availability coverage is assumed to be 100% in both rounds. However, to estimate the correct and actual nature of service capacity, program data are needed. Information extracted from available literature and Avahan centralized management information system (CMIS) data provides a glimpse of service capacity under the intervention in both rounds of analysis.Citation34 Socially marketed number of condoms per thousand targeted beneficiaries increased from Round 1 to Round 2 (4,430 to 6,876, respectively). However, the number of sites per 100,000 beneficiaries diminished from six to four between Round 1 and Round 2, respectively. provides the indicators of service capacity.
Table 2 Service capacity under the Kavach project
The percentage of those who had heard about Khushi clinics significantly increased from Round 1 to Round 2 (46.1% vs 53.8%, respectively; χ2, 24.22; P<0.001). However, the percentage of those who had seen the logo of the Khushi clinic diminished (58.5% vs 45.4%; χ2, 74.07, respectively; P<0.001). By and large, the percentage of those who had either heard of or seen the logo significantly diminished between the two rounds (60.9% vs 54.6%, respectively; χ2, 16.467; P<0.001). This indicator describes the accessibility coverage in both rounds of analysis.
The percentage of LDTDs who were associated with the Khushi clinic for more than or equal to 6 months had increased between Round 1 and Round 2 (13.8% vs 50.6%, respectively; χ2, 645.458; P<0.001). Association with a Khushi clinic indicates acceptability coverage among LDTDs. Here, availability, accessibility, and acceptability coverage define the potential coverage, whereas contact and effectiveness coverage are associated with actual coverage.
Contact is characterized as a visit to the Khushi clinic for any reason (a visit to the doctor, to seek care for general ailments, and/or to seek advice/care for an STI). The percentage of individuals who visited Khushi clinics for any purpose significantly increased between Round 1 and Round 2 (12.7% vs 22.3%, respectively; χ2, 65.521; P<0.001). This highlights the contact coverage under the analytical frame of analysis.
As discussed, for effectiveness coverage, two separate measures were used: 1) preventive and 2) curative coverage. Preventive needs are the essential or intrinsic needs, and are controlled by demographic factors. In contrast, curative needs are care-oriented and controlled by demographic and epidemiological aspects. Findings show that percentage of LDTDs who utilized any important preventive service (eg, received condoms or counseling) significantly increased between Rounds 1 and 2 (11.5% vs 22.4%, respectively; χ2, 85.711; P<0.001). This result highlighted prevention-oriented effectiveness coverage. Similarly, the percentage of those who received advice/medicine from the Khushi clinic for any STI significantly increased from Round 1 to 2 (0.4% vs 1.4%, respectively; χ2, 10.421; P=0.002). This result defines care-oriented effectiveness coverage. summarizes the results of health care coverage under the Kavach intervention.
Table 3 Evaluation of health care coverage among truckers under the Kavach project, IBBA-NH (Rounds 1 and 2)
Likewise, a route-specific analysis of health care coverage shows route-specific differentials in health care coverage between the two rounds of the IBBA-NH survey. Accessibility coverage significantly increased in the NW corridor between the two rounds of the IBBA-NH (49.2% vs 62.5%, respectively; χ2, 18.73; P<0.001). In other corridors, accessibility coverage significantly decreased between the two rounds. Acceptability coverage significantly increased in all national highway corridors. However, the SE corridor recorded the least significant increases between the two rounds (9.6% vs 20.1%, respectively). Contact coverage increased significantly in the NW corridor between Round 1 and Round 2 (10.5% vs 30.4%, respectively; χ2, 63.30; P<0.001). However, no significant change was seen in other corridors. Effectiveness coverage (preventive or curative) significantly increased in the NE corridor (11.5% vs 25.0%, respectively; χ2, 31.08; P<0.001) and the NW corridor (10.5% vs 29.3%, respectively; χ2< 57.47; P<0.001). shows the route-specific health care coverage under the Kavach project.
Table 4 Evaluation of route-specific health care coverage under the Kavach project, IBBA-NH (Rounds 1 and 2)
The Tanahashi framework permits variation and flexibility in the definition and estimation of coverage.Citation28 A specific subgroup of the total target population can also be chosen for estimation as the denominator in different coverage ratios. Resulting coverage measurements highlight an alternate aspect of interaction between the service and the populace. This may be called “specific coverage”. The actual coverage among people with adequate accessibility to the service can be considered to measure provision-specific coverage. Here, total number of LDTDs in each round – those who had either heard about the Khushi clinic or seen the logo of the Khushi clinic – was taken as the denominator to estimate specific coverage. highlights the provision-specific coverage based on adequate accessibility.
Table 5 Evaluation of provision-specific coverage under the Kavach project, IBBA-NH (Rounds 1 and 2)
Considering provision-specific coverage, acceptability to LDTDs significantly increased between Rounds 1 and 2 (22.6% to 92.8%; χ2, 1193.365; P<0.001) among LDTDs who had heard of/seen the logo of the Khushi clinic. In a like manner, among LDTDs who accepted the services, contact coverage significantly increased (20.9% to 40.8%; P<0.001). Prevention- and care-oriented effectiveness coverage among LDTDs who had access to the service also increased considerably (18.9% to 40.8%; χ2, 111.645; P<0.001, and 0.7% to 2.5%; χ2, 12.804; P<0.001, respectively).
Discussion
The analysis highlights that there is a significant difference in various indicators of service coverage between the two rounds of the IBBA-NH survey. A detailed analysis of the shape of the operation/coverage curve (the locus of different points of various stages of health care coverage) facilitates in identifying issues related to the service delivery at different stages of health care coverage.
TanahashiCitation28 defined these stages/this coverage in such a way that there exists a certain gap between them. A large gap between adjacent pairs of coverage measures shows that, for a proportion of the target population, service provisioning is not meeting their needs. For example, all those who have access to service have not accepted the service, and all those who have accepted the service have not utilized the service. The large differences exhibit the issues in service provision to LDTDs, and show a sharp shift in the operation/coverage curve to the left. highlight the shape of the operation/coverage curve.
Figure 1 Coverage curves for the provision of health care to LDTDs through the Kavach project. Coverage curves based on all LDTDs (A), and provision-specific coverage curves (B).
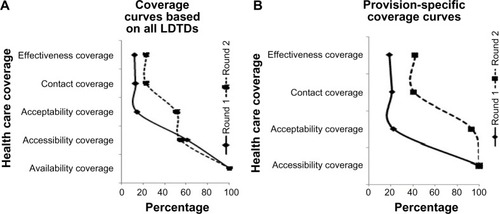
shows that the coverage curve in Round 2 shifts sharply to the left when compared with Round 1 from availability to accessibility coverage portion. Tanahashi described this sharp shift as the result of inefficient allocation and use of resources and facilities.Citation28 However, the intervention is better accepted in Round 2 among LDTDs than in Round 1. A sharp shift in the coverage curve in Round 1 from accessibility to acceptability coverage portion shows the issues related to acceptability of service due to poor acknowledgement of the service among LDTDs, ie, more LDTDs were not going to Khushi clinics in Round 1. These sharp shifts highlight difficulties in the service provision; however, these shifts do not underline the components responsible for the poor coverage. Comprehensive understanding of health services and conditions of the target population is needed to examine the components responsible for poor coverage. Multiple factors play a significant role in access to health care. These factors are identified as demand- and supply-side components/factors. As the analysis highlights the issues of accessibility and acceptability coverage, these barriers are illustrated as the demand- and/or supply-side factors.Citation35,Citation36 Demand-side factors influence ability to use the service. The geographical location of a service plays a crucial role in accessing the service; all the same, comprehensive knowledge and awareness about services can influence accessibility considerably. Supply-side factors are inbuilt into the system and decide service uptake. They may be identified with managerial shortcomings or inefficient allocation of resources. Various demand- and supply-side interventions (monetary and non-monetary) can address these barriers/issues and significantly increase access to health care. Under the Kavach project, various interventions were initiated to provide access to care.
Low acceptability of the service in Round 1 shows the issues regarding acceptability coverage. The demand-side factors which may have influenced this may be related to low self-esteem or lack of health consciousness among LDTDs, which increases the challenge of accessing health care.Citation37 At the supply side, factors influencing acceptability may relate to awareness generation costs of the service or inability of staff to build a trust association or rapport with the beneficiary.Citation38
Coverage curves in both rounds, however, do not reveal issues in effectiveness coverage. This highlights the quality of service provided by the intervention/health care facility, ie, that those who have accepted the services, have utilized them as well. Likewise, in , provision-specific coverage curves reveal that acceptance of service was a major issue in service delivery in Round 1.
To overcome demand- and supply-side obstacles in service provisioning, various interventions may be initiated. These interventions can be monetary and non-monetary. Demand-side (non-monetary) interventions include counseling and provision of information, community participation, and social marketing.Citation39 Under HIV prevention interventions, these have been applied to promote condom use and improve treatments for selected STIs.Citation40 Measures like peer educators, outreach activities, etc, also attempt to overcome community and cultural preferences and prompt acceptability of services.Citation40 A study in the past have also cited that a range of preventive interventions implemented through non-professional health workers, and recruitment of them from within the community, reduces many acceptability barriers.Citation41 Under the Kavach project, various demand-side (non-monetary) interventions were introduced, eg, peer educators, counseling, and social marketing of condoms, etc, which were attempts to fill the gaps in health care coverage. Demand-side monetary interventions were not introduced under the Kavach project. However, free consultation for health-related issues (general ailments, STIs, and HIV infection) and referrals may be considered incentives that may have facilitated acceptability and contact (by increasing affordability). The multi-media communication plan under the Kavach program has resulted in a doubling of monthly reach across the program (in terms of monthly contacts through peer-led interpersonal communication and participation in mid-media activities).Citation26 Recall of the Khushi brand also significantly increased among the targeted LDTDs, resulting in significant uptake of services by Round 2 survey time.Citation26
Similarly, supply-side non-monetary interventions are identified, with provisioning of essential services at health facilities (preventive and curative care) at cost. These interventions address availability and affordability, to an extent. Provision of preventive care services meets the expectations of individuals. If the services are provided at the facility, they are mostly used by individuals (acceptability). Provision of improved access to services has resulted in uptake of clinical services by a factor of 2.5 across 17 intervention sites.Citation26 Similarly, regulation of the health and non-health sectors of public–private service provision may address issues related to affordability. The provision of integrated outreach activities tackles the issue related to accessibility, although the range may be limited. The provision of culturally sensitive health care can be improved through specific courses or by employing members of the same ethnic groups (acceptability). Improved management, and system-inbuilt supervision and feedback mechanisms, possibly provide the best guarantee as they can effectively address all four dimensions related to access barriers, and amend each associated aspect, as long as sufficient resources are available. Management can thoroughly deal with issues identified with human resources, finances, and service organization and delivery. Furthermore, there are ranges of monetary interventions which can enhance access to health care and reduce barriers.
The Kavach project, with a mix of different demand-side and supply-side interventions, provided access to health care coverage. The analysis in this paper reflects the gaps in the health care coverage under the intervention. However, all these interventions under the project were not able to provide a solution for all access-related issues. This gives an opportunity for policy makers and implementing agencies to improve access considerably by taking into account the lessons learnt from various initiatives under the project. As suggested by O’DonnellCitation36 and De Brouwere et al,Citation42 various demand-side and supply-side barriers must be addressed to realize the optimal impact of any intervention. Adequate selection of interventions will facilitate the access to health care given the political, cultural and geographical environment and historical development of the health sector.
The findings of this paper should be read with certain caveats. Definitions of coverage and identification of corresponding indicators were confined to the questions asked in the IBBA-NH survey. Wherever possible, different indicators are taken as a close proxy to accurate indicators. This may have resulted in some aspects of coverage being inadequately explored.
Conclusion
This paper emphasizes the need for further studies to assess contextual factors that influence the effectiveness and efficiency of interventions designed to address access barriers and to identify what combination of interventions may generate the best possible outcome. It comments on the gaps in accessibility and acceptability of health care coverage. The analysis based on the Tanahashi framework of evaluation of health care coverage can be used to identify the gaps in different stages of service delivery, and then can be used to analyze the constraining factors, taking into account interventions under consideration. This may facilitate the better implementation of any intervention and uptake of other interventions of comparable nature.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
This paper was written as a part of the Knowledge Network Project of the Population Council, as a grantee from the BMGF through Avahan, its India AIDS Initiative. The authors would like to thank Professor Indrani Gupta, Institute of Economic Growth, New Delhi, India for giving her invaluable comments on the earlier draft of this paper. However, the views expressed in this paper are of the author(s) alone and do not necessarily reflect the official policy or position of the BMGF and Avahan.
Disclosure
The authors report no conflicts of interest, financial or otherwise, in this work.
References
- The World BankTransport Against HIV/AIDS: Synthesis of Experience and Best Practice GuidelinesWashington, DCThe World Bank2009 Available from: http://siteresources.worldbank.org/INTTRANSPORT/Resources/336291-1227561426235/5611053-1229359963828/tp-25-HIV-AIDS.pdfAccessed January 3, 2015
- ChandrasekaranPDallabettaGLooVRaoSGayleHAlexanderAContaining HIV/AIDS in India: the unfinished agendaLancet Infect Dis20066850852116870529
- RaoKSPilliRDRaoASChalamPSSexual lifestyle of long distance lorry drivers in India: questionnaire surveyBMJ199931871771621639888910
- HudsonCPAIDS in rural Africa: a paradigm for HIV-1 preventionInt J STD AIDS1996742362438876353
- RaoVTMahapatraBJunejaSSinghIREvaluating the McDonald’s business model for HIV prevention among truckers to improve program coverage and service utilization in India, 2004–2010HIV AIDS (Auckl)20135516023439724
- PandeyAMishraRMSahuDHeading towards the Safer Highways: an assessment of the Avahan prevention programme among long distance truck drivers in IndiaBMC Public Health201111Suppl 6S1522376295
- SanjeevKGSKBSKA study of knowledge, sexual behaviour and practices regarding HIV/AIDS among long distance truck driversIndian J Public Health200953424324520469766
- CornmanDHSchmiegeSJBryanABenzigerTJFisherJDAn information-motivation-behavioral skills (IMB) model-based HIV prevention intervention for truck drivers in IndiaSoc Sci Med20076481572158417257724
- SinghYNMalaviyaANLong distance truck drivers in India: HIV infection and their possible role in disseminating HIV into rural areasInt J STD AIDS1994521371388031917
- BhallaSChandwaniHSinghDSomasundaramCRasaniaSKSinghSKnowledge about HIV/AIDS among senior secondary school students in Jamnagar, GujaratHealth Popul Perspect Issues200528178188
- MohamedAPaccaJCCAP study on truck drivers in Maputo/Mozambique: prevention roadblocks in a group passing through high prevalence zonesInternational Conferences on AIDSJul 7–12, 200214 abstract no. D11169
- SohailASexual behaviour among truck drivers in PakistanCulture, Health and Sexuality200242191206
- International Labour OrganisationReport and analysis of “A Truck Driver’s Life: Working Conditions and Sexual Health”. HIV and Long-distance Transport in ParaguaySantiagoInternational Labour Organisation http://www.ilo.org/wcmsp5/groups/public/@ed_protect/@protrav/@ilo_aids/documents/publication/wcms_184517.pdf.2012Accessed January 3, 2015
- McCreeDHCosgroveSStratfordDSexual and drug use risk behaviors of long-haul truck drivers and their commercial sex contacts in New MexicoPublic Health Rep20101251526020402196
- Prem KumarSGKumarGAPoluruRContact with HIV prevention programmes and willingness for new interventions among truckers in IndiaIndian J Med Res201313761061107123852287
- PalK“Fearless”: Improving Sexual and Reproductive Health of Female Sex WorkersIndia HIV/AIDS Alliance http://www.allianceindia.org/fearless-improving-sexual-reproductive-health-of-female-sex-workers/Accessed Feb 1, 2014
- ChakrapaniVNewmanPAShunmugamMKurianAKDubrowRBarriers to free antiretroviral treatment access for female sex workers in Chennai, IndiaAIDS Patient Care STDS2009231197398019821725
- PulerwitzJMichaelisAPLippmanSAChinagliaMDíazJHIV-related stigma, service utilization, and status disclosure among truck drivers crossing the Southern borders in BrazilAIDS Care200820776477018767210
- SaggurtiNMishraRMProddutoorLCommunity collectivization and its association with consistent condom use and STI treatment-seeking behaviors among female sex workers and high-risk men who have sex with men/transgenders in Andhra Pradesh, IndiaAIDS Care201325Suppl 1S55S6623745631
- BaquiAHRosecransAMWilliamsEKNGO facilitation of a government community-based maternal and neonatal health programme in rural India: improvements in equityHealth Policy Plan200823423424318562458
- UbaidullahMSocial vaccine for HIV prevention: a study on truck drivers in South IndiaSoc Work Health Care2004393–439941415774403
- National AIDS Control Organisation (NACO)Targeted Interventions Under NACP III. Operational GuidelinesNew DelhiNACO, Ministry of Health & Family Welfare, Government of India2007 Available from: http://www.naco.gov.in/upload/Publication/NGOs%20and%20targetted%20Intervations/NACP-III.pdfAccessed January 3, 2015
- National AIDS Control Organisation (NACO)Annual HIV Sentinel Surveillance Country Report 2006New DelhiNational Institute of Health & Famliy Welfare, NACO, Ministry of Health & Family Welfare2007 Available from: http://naco.gov.in/upload/NACO%20PDF/HIV%20Sentinel%20Surveillance%202006_India%20Country%20Report.pdfAccessed January 3, 2015
- RaoANagMMishraKDeyASexual behaviour pattern of truck drivers and their helpers in relation to female sex workersInd J Soc Work1994554603615
- National AIDS Control Organisation (NACO)Annual HIV Sentinel Surveillance: Country Report 2008–09New DelhiNational Institute of Health & Famliy Welfare, NACO, Ministry of Health & Family Welfare2011 Available from: http://naco.gov.in/upload/Surveillance/Reports%20&%20Publication/HIV%20Sentinel%20Surveillance%20India%20Country%20Report,%202008-09.pdfAccessed January 3, 2015
- Bill and Melinda Gates FoundationOff the Beaten Track: Avahan’s Experience in the Business of Prevention among India’s Long-Distance TruckersNew DelhiBill and Melinda Gates Foundation2008 Available from: https://docs.gatesfoundation.org/Documents/Avahan_OffTheBeatenTrack.pdfAccessed January 3, 2015
- GelmonLJSinghKSinghPBhattacharjeePMosesSCostiganABlanchardJSexual Networking and HIV Risk in Migrant Workers in IndiaXVIth International AIDS ConferenceToronto, CanadaAugust 2006 Abstract MOAC0304, Abstract volume 1
- TanahashiTHealth service coverage and its evaluationBul WHO1978562295303
- MaruDSKhakhaDCTahirMBasuSSharmaSKPoor follow-up rates at a self-pay northern Indian tertiary AIDS clinic.Int J Equity Health200761417958898
- World BankCorporate Responses to HIV/AIDS: Case Studies from IndiaWashington, DCThe World Bank2007
- National Institute of Medical ScienceIntegrated Behavioural and Biological Assessment – National HighwaysNew Delhi, IndiaNational Institute of Medical Statistics, Indian Council of Medical Research, Department of Health Research, Ministry of Health & Family Welfare, Government of India2011 Available from: http://www.ibbainfo.in/keydoc/reports/SR_NH.pdfAccessed January 3, 2015
- McIlfatrickSHassonFMcLaughlinDPublic awareness and attitudes toward palliative care in Northern IrelandBMC Palliat Care20131213424044631
- KrishbaunMCareyIPurcellBNashSTalking About Dying and Death: A Focus Group Study to Explore a Local Community PerspectiveNursing Reports20111e82934
- Avahan CMIS Data [database on the Internet]. FHI 360:V6 Available from: http://dx.doi.org/10.7910/DVN/24631Accessed February 4, 2015
- EnsorTCooperSOvercoming barriers to health service access: influencing the demand sideHealth Policy and Planning32004192697914982885
- O’DonnellOAccess to health care in developing countries: breaking down demand side barriersCadernos de saude publica200723122820283418157324
- PaphassarangCPhilavongKBouphaBBlasEEquity, privatization and cost recovery in urban health care: the case of Lao PDRHealth Policy Plan200217Suppl728412477744
- OzawaSWalkerDGTrust in the context of community-based health insurance schemes in Cambodia: villagers’ trust in health insurersAdv Health Econ Health Serv Res20092110713219791701
- PriceNThe performance of social marketing in reaching the poor and vulnerable in AIDS control programmesHealth Policy Plan200116323123911527863
- JacobsBKambuguFSWhitworthJASocial marketing of pre-packaged treatment for men with urethral discharge (Clear Seven) in UgandaInt J STD AIDS200314321622112665447
- HainesASandersDLehmannUAchieving child survival goals: potential contribution of community health workersLancet200736995792121213117586307
- De BrouwereVRichardFWitterSAccess to maternal and perinatal health services: lessons from successful and less successful examples of improving access to safe delivery and care of the newbornTrop Med Int Health201015890190920545915