
Abstract
Hepatic encephalopathy (HE) is a common complication of liver dysfunction, including acute liver failure and liver cirrhosis. HE presents as a spectrum of neuropsychiatric symptoms ranging from subtle fluctuating cognitive impairment to coma. It is a significant contributor of morbidity in patients with liver disease. HE is observed in acute liver failure, liver bypass procedures, for example, shunt surgry and transjugular intrahepatic portosystemic shunt, and cirrhosis. These are classified as Type A, B and C HE, respectively. HE can also be classified according to whether its presence is overt or covert. The pathogenesis is linked with ammonia and glutamine production, and treatment is based on mechanisms to reduce the formation and/or removal of these compounds. There is no specific diagnostic test for HE, and diagnosis is based on clinical suspicion, excluding other causes and use of clinical tests that may support its diagnosis. Many tests are used in trials and experimentally, but have not yet gained universal acceptance. This review focuses on the definitions, pathogenesis and treatment of HE. Consideration will be given to existing treatment, including avoidance of precipitating factors and novel therapies such as prebiotics, probiotics, antibiotics, laxatives, branched-chain amino acids, shunt embolization and the importance of considering liver transplant in appropriate cases.
Introduction
Hepatic encephalopathy (HE) is a hallmark of liver failure and affects up to 40% of patients with liver cirrhosis.Citation1 It is defined as a multifactorial neuropsychiatric disorder presenting with a broad spectrum of cognitive impairment and neuromuscular dysfunction.Citation1 HE is a significant contributor to repeated hospitalizations for patients with liver cirrhosis and severely impacts on the quality of life of both patients and caregivers.Citation2 It is a marker of poor prognosis in cirrhotic patients, with reported rates of survival of only 36% at 1 year from its first presentation.Citation3
Chronic liver disease is the fifth most common cause of death in the UK, with the mortality expected to rise due to increase in cirrhosis caused by alcohol-related liver disease, chronic hepatitis C and nonalcoholic fatty liver disease.Citation4,Citation5 Patients commonly present to primary and secondary care services with complications such as HE with or without a prior diagnosis of chronic liver disease. A milder form of the disorder, covert hepatic encephalopathy (CHE) or covert encephalopathy with subtle alterations of cognitive function, also exists.Citation6 Although less severe, patients with CHE are at significant risk of interference with their quality of life, including increased falls, hospitalizations and progression to overt HE.Citation6–Citation8
The aims of this review are to provide a comprehensive, “state of the art”, account of the pathophysiology, clinical manifestations (classification, symptoms, signs and investigations), current treatments and future targets for the management of patients with HE. The review is targeted to physicians in primary or secondary care and also to health care professionals who are likely to encounter patients with liver disease in their professional roles.
Pathogenesis of HE
HE can be classified as three separate clinical entities. Type A HE is due to acute liver failure, Type B due to portosystemic shunting (e.g., transjugular intrahepatic portosystemic shunting procedures) and Type C results as a complication of liver cirrhosis.Citation9
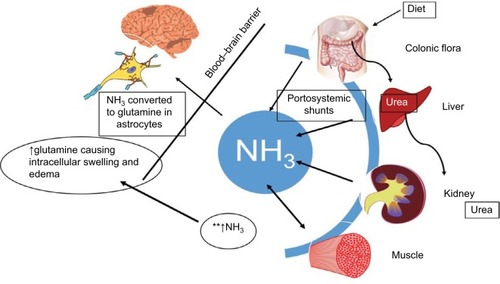
Type A HE is associated with an increased intracranial pressure that progresses rapidly and may lead to brain herniation. The pathophysiology of Type B and C HE is complex and remains under investigation. The main hypothesis involves the limited ability of the liver to effectively remove nitrogenous waste products, resulting in their accumulation and the deleterious effects on the brain due to portosystemic shunting.Citation10,Citation11 The key substrates implicated are ammonia and glutamine. Several studies have demonstrated that cirrhotic patients who had or were experiencing significant neuropsychiatric symptoms had elevated blood ammonia concentration.Citation12,Citation13 However, the levels were not predictive or consistent with the severity of HE.Citation14,Citation15 The exception is in type A HE, where Bernal et al have shown that a cut-off level of ammonia >200 µmol/LCitation16 is predictive of raised intracranial pressure and death.Citation16,Citation17
Glutamine is a key amino acid that plays an important signaling role for processes including gene expression, cytokine production and cell proliferation. Enhanced activity of glutamine is primarily noted in skeletal muscle, brain, heart and hepatocytes. Glutamine is metabolized in the gut and kidney to ammonia and glutamate. Ammonia is then detoxified in the kidneys and liver and excreted as urea. In liver failure, ammonia escapes the urea cycle and is detoxified to glutamine in various tissues. A vicious cycle is formed, whereby increased ammonia concentration due to impaired detoxification in the liver further activates glutamine synthesis, leading to increased glutamine catabolism resulting in hyperammonemia. The enhanced activity of glutamine has been shown to exert adverse effects such as swelling of astrocytes in the brain and increases the catabolism of branched-chain amino acids (BCAAs) in skeletal muscles.Citation18
Manganese has also been implicated in the pathogenesis of HE, with elevated plasma levels due to inability of excretion by the liver causing deposition in the basal ganglia.Citation19 This has been shown to correlate with pallidal signal hyperintensity observed on magnetic resonance imaging of cirrhotic patients.Citation19,Citation20 Furthermore, an animal study by Rivera-Mancia et al showed that manganese favored ammonia and glutamine accumulation in the brain.Citation21
Additional factors involved in the pathogenesis of HE include gut microbiota dysbiosis and small intestinal bacterial overgrowth (SIBO). This pathway has gained interest for novel therapies. SIBO in patients with cirrhosis is a consequence of reduced gut motility, reduced gastric acid secretion, luminal IgA deficiency and malnutrition.Citation22 SIBO results in impairment of intestinal barrier integrity, therefore increasing bacterial translocation and release of ammonia and endotoxins into the circulation.Citation22 Zhang et alCitation24 and Bajaj et al,Citation23 in several well-designed studies, have found a distinct variation in the population of microbiota between cirrhotics and noncirrhotics. Cirrhotics were shown to have an increased Bacteriodes/Firmicutes ratio at the expense of commensal bacteria.Citation25 Dominant species in cirrhotic patients included those of Streptococcaceae, Veillonellaceae, Alcaligenaceae and Porphyromonadaceae. These correlated significantly with ammonia levels and decreased cognitive function. Also, several other bacterial species demonstrated an association with increased inflammatory responses in patients with CHE.Citation26 Tsai et al have recently shown that cirrhotic patients using proton-pump inhibitors (PPIs) were more likely to develop HE. It is hypothesized that PPIs cause gut dysbiosis leading to HE, from the previous findings of the association between PPI use and SIBO.Citation27
Sarcopenia (muscle volume depletion) has been shown to predict the development of encephalopathy in cirrhotic patients.Citation28 Skeletal muscle represents an alternative site of ammonia detoxification; therefore, reduced muscle volume results in hyperammonemia. The consumption of BCAAs in the detoxification of ammonia to glutamine in skeletal muscle results in low levels of BCAAs in blood plasma. Hanai et al demonstrated that patients with sarcopenia and HE due to cirrhosis have low levels of BCAA.Citation28–Citation31 The theory is that therapeutic supplementation with BCAAs can, therefore, reduce malnutrition and revert the loss of muscle cell mass and breakdown of protein driving hyperammonemia.Citation31 An increase in muscle mass will also help drive increased extrahepatic ammonia detoxification. Another main driver of sarcopenia is thought to be myostatin, a negative regulator of satellite cell differentiation and proliferation. There are higher levels of serum and muscle myostatin in cirrhotic patients, and ammonia has been shown to stimulate myostatin expression.Citation32
There are additional factors that can precipitate HE and act synergistically with ammonia in its pathogenesis (). For example, hyponatremia can exacerbate HE due to its osmotic effects on astrocytes,Citation33,Citation34 and patients with systemic inflammatory response syndrome are predisposed to HE. In patients with HE, there is an alteration in cerebral blood flowCitation35 and enhanced sensitization of the brain to inflammatory cytokines by ammonia.Citation36 Moreover, there is an increased oxidative stress caused by augmented permeability of the blood–brain barrier contributing to altered mental status.Citation37–Citation39
Table 1 Precipitating factors to HE
It is becoming increasingly recognized that no single entity is responsible for HE, but rather it is a synergistic effect of multiple mechanisms ().
Figure 1 Contributing factors toward pathophysiology of HE.
Abbreviation: HE, hepatic encephalopathy.
Diagnosis of HE
Clinical features
HE presents with a wide spectrum of neuropsychiatric symptoms which typically begin with subtle psychomotor changes.Citation40 This progresses to confusion with the presence of asterixis, somnolence and, finally, its most severe form, coma. The most common clinical classification used to describe this continuum is the West Haven Criteria ().Citation9
Table 2 West Haven Criteria for hepatic encephalopathy and symptoms
CHE or covert encephalopathy represents the initial stages of the disorder that can only be recognized by psychometric testing.Citation41 The first feature to emerge is psychomotor slowing and difficulties in performing activities of daily living.Citation42,Citation43 Up to 50% of cirrhotic patients are affected by CHE.Citation42 As HE progresses, symptoms become more apparent and can be detected clinically. There is alteration in conscious levels and disorientation, and disturbance of the sleep–wake cycle is often a feature.Citation43 Personality changes may emerge, and there can also be motor system abnormalities including hypertonia, hyper-reflexia, dystonia, dyskinesia, upgoing plantars and asterixis. Asterixis or “flapping tremor” is a negative myoclonus with a loss of postural tone frequently seen in the hands, but can affect other parts of the body.Citation44 The onset of disorientation and asterixis is described as overt encephalopathy.
The American and European Associations for the Study of the Liver 2014 practice guidelines recommend that HE be classified according to four factors:Citation1
the underlying etiology as described previously – Type A, B or C;
severity – using grading system such as West Haven Criteria;
time course – episodic, recurrent (>1 episode in 6 months) or persistent (symptoms always present and can have episodes of acute exacerbations); and
nonprecipitated or precipitated by factors such as infections, medications or electrolyte disorders.
Investigations
Diagnosis of HE should be made on a clinical basis after exclusion of various conditions that can mimic HE. These are outlined in . Arterial or venous ammonia levels can be helpful, but should not be used alone in diagnosis as they are often inconsistent, as outlined previously. Electroencephalography is valuable to investigate for the presence of subclinical seizures. Characteristic triphasic wave changes can be seen in HE, alongside subtle signs in CHE.Citation45,Citation46
Table 3 Differential diagnosis of HE
Imaging modalities such as computed tomography and magnetic resonance imaging should be performed to exclude differential diagnosis.Citation1,Citation47 In patients with normal neurologic examinations, brain imaging is unlikely to be beneficial; also, there is probably an overuse of computed tomography scans in patients with cirrhosis and altered mental status alone.Citation48 The main concern in patients with cirrhosis is intracranial bleeds due to coagulopathy; yet, this is rare in the absence of focal neurologic deficits.Citation49 Other imaging abnormalities on magnetic resonance imaging include basal ganglia hyperintensity, and this may be a possible marker for HE and severity of liver failure.Citation50–Citation52 In the literature, there is a case describing a patient with recurrent HE associated with dynamic changes in the basal ganglia hyperintensity pre- and posttreatment.Citation53 Similar changes have been seen using positron emission tomography, but this is currently used as an experimental tool to elucidate underlying pathophysiology.Citation54
Diagnosing CHE remains a challenge, and clinicians should suspect presence of CHE from inquiring about the presence of signs and symptoms. It should be considered in patients complaining of difficulties with activities of daily living, loss of concentration, lack of ability to function at work or with relatives having noted change in cognition.Citation47 Assessment is done by using validated psychometric tests, the gold standard being a combination of the psychometric hepatic encephalopathy score,Citation46 but a combination of tests may be more accurate.Citation55 A summary of the most established tests is highlighted in .
Table 4 Psychometric tests used in the evaluation of MHE
In an era of technologic advance, development of smart-phone applications, such as the EncephalAppCitation56 and Stroop App,Citation57 are making these tests more accessible and user-friendly for clinicians and patients.
There are multiple other tools in development for a more accurate diagnosis of HE that are not yet validated, but are promising. The challenge is to keep the test simple for patients, but, at the same time, maintain its accuracy in diagnosing HE. Examples of these include the animal naming test (maximum number of animals listed in 1 minute), one study showed that scores obtained in the animal naming test directly correlated to grade of encephalopathy.Citation58
Recently, a pilot study from Arasaradnam et al demonstrated the potential use of exhaled volatile organic compounds to detect HE.Citation59
Management of HE
Patients presenting with overt HE typically will have an underlying precipitant such as infection, medications, gastrointestinal bleeding or other precipitating factors. The acute management relies on detailed history and examination to identify and treat these as appropriate. Ninety percent of patients can be treated by correcting the precipitating factor.Citation47 It is important to recognize that a proportion of patients will have no underlying precipitant of HE.
Patients with CHE do not usually require treatment unless the condition is thought to be adversely affecting their quality of life. Current American Association for the Study of Liver Diseases (AASLD) guidelines focus on management strategies for overt HE. Patients should be managed empirically for HE, while the investigations for precipitating factors or mimics of HE are ongoing.Citation47
Prebiotics, probiotics and symbiotics
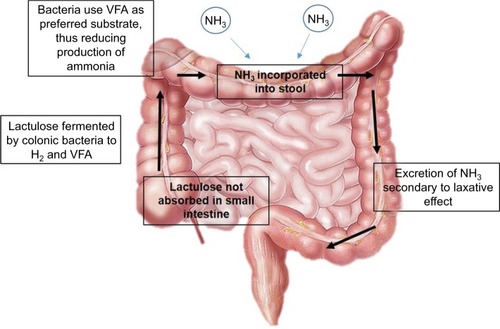
Lactulose, a prebiotic, is the most widely used nonabsorbable disaccharide (NAD) in clinical practice and is recommended by AASLD/European Association for the Study of the Liver (EASL) guidelines as the first-line treatment for episodes of HE. Treatment should continue on resolution of symptoms to prevent further episodes. In the colon, lactulose is converted to lactic and acetic acid, reducing intraluminal pH and promoting the utilization of ammonia in the metabolism of gut bacteria (). A 2016 Cochrane meta-analysis of 38 randomized clinical trials showed that when compared with placebo or no intervention, NAD may be associated with a beneficial effect on HE. In addition, it showed that NAD treatment can reduce serious adverse events associated with liver disease, including liver failure, hepatorenal syndrome and variceal bleeding.Citation60 The analyses included data for treatment and prevention of HE. Lacitiol is a second-generation NAD that has been suggested to have similar effectiveness and better tolerance than lactulose,Citation61 although a Cochrane review showed that it had no beneficial effects when compared to lactulose. The quality of evidence for lacitiol is poor and further research is needed.Citation60
Figure 2 Mechanism of action of nonabsorbable disaccharides.
Abbreviation: VFA, volatile fatty acids.
Probiotics are live microorganisms that are believed to confer health benefits in a variety of clinical settings.Citation62 In HE, probiotics have been shown to act by modulating gut microbiota to reduce ammonia levels by several mechanisms, including decreased bacterial urease activity, decreased ammonia absorption by decreasing the pH and improved nutritional status of gut epithelium.Citation63 The most commonly used probiotic currently is VSL#3. At present, all evidence relating to use of probiotics in the treatment of HE is of poor quality, as highlighted by the 2017 Cochrane review of 21 trials.Citation64 Probiotics had no effect on all-cause mortality, when compared to placebo or no treatment. Probiotics may lead to improvements in the development of overt HE, quality of life and plasma ammonia concentrations, with minimal adverse effects. Yet, the review was unable to conclude if probiotics were superior to lactulose in the treatment of HE. The optimal dose, delivery and species of probiotics to use have not been determined.Citation65
Symbiotics are a combination of prebiotics and probiotics and their clinical significance in HE remains uncertain. There are several randomized controlled trials that demonstrate the possible beneficial effects.Citation25,Citation66,Citation67
Polyethylene glycol is a purgative laxative agent which has been shown in a randomized controlled trial by Rahimi et al to be superior to lactulose in improving HE with a quicker time for resolution.Citation68 But, more data is required before it can be routinely recommended in preference to lactulose.
Nutrition
Nutritional therapy is relevant in HE as a modulator of nitrogen metabolism. Historically, dietary protein restriction had been advised to reduce intestinal ammonia production. But, this may contribute to sarcopenia and actually worsen HE.Citation69 Thus, it was recommended by the International Society for Hepatic Encephalopathy and Nitrogen Metabolism that 1.2–1.5 g/kg of protein be given in small meals distributed throughout the day with a late night snack of complex carbohydrates.Citation70 A nasogastric feeding tube should be considered if the patient is unable to achieve their dietary targets.
If patients are unable to maintain dietary protein intake, supplementation with BCAA is an alternative. Oral BCAA supplements consist of several essential amino acids thought to improve ammonia detoxification. A recent 2015 Cochrane review of 16 randomized clinical trials found high-quality evidence of clinical benefit, but no effect on mortality, quality of life or nutrition parameters.Citation31
Deficiencies of vitamins and electrolytes should also be addressed, as they can be associated with a wide range of neuropsychiatric symptoms.Citation71 Although not directly implicated in the pathophysiology of HE, they can compound or mimic symptoms. The use of additional zinc supplementation has been previously studied; a systematic review showed a potential improvement in psychometric tests, but its use did not affect the recurrence rates of HE.Citation72 More recently, Mousa et al conducted a randomized trial which demonstrated that antioxidant and zinc supplementation led to a significant improvement in baseline neuropsychometric tests in patients with CHE, when compared to lactulose therapy.Citation73
Antimicrobials
The use of oral antibiotics to modulate gut flora and reduce ammonia production has been researched as a tool to treat HE. Neomycin, an aminoglycoside antibiotic which is poorly absorbed and reaches high concentrations in the gut, acts as a glutaminase inhibitor, thereby reducing ammonia levels.Citation74 It was the first antibiotic agent to be widely used in HE. However, the adverse effects associated with neomycin and the development of newer agents preclude its use in current clinical practice.
Rifaximin is a semi-synthetic nonabsorbable antibiotic derived from rifamycin. When compared with neomycin, rifaximin was found to be at least as effective in reducing blood ammonia levels, while having less adverse effects such as ototoxicity and nephrotoxicity.Citation75–Citation77 It exerts its effects by several mechanisms – modulating gut microbiota composition and metabolism and also exhibiting anti-inflammatory properties.Citation78 EASL and AASLD guidance recommends the use of rifaximin for secondary prophylaxis of overt HE in patients who have had further episodes while on lactulose therapy. These recommendations are based on evidence from a large well-conducted randomized controlled trial.Citation79 Combination therapy of rifaximin with lactulose has been shown to be more effective than the use of rifaximin alone.Citation80
Sidhu et al demonstrated in a randomized open-label trial that there was no difference in improvement of cognitive function or quality of life in patients with CHE treated with rifaximin alone versus lactulose alone.Citation81 An upcoming clinical trial, RiMINI, aims to assess the influence of rifaximin versus combination therapy of rifaximin and lactulose on the microbiota in patients with CHE.Citation82 Currently, there is no evidence for primary or secondary prophylaxis for patients with CHE.
Other antimicrobials such as metronidazole and vancomycin have been investigated, but their significant adverse effect profile limits their use.Citation83,Citation84
Other therapies
Several other therapies are currently under investigation for use as treatment for HE, most of which aim to lower serum ammonia levels. l-Ornithine-l-aspartate is used as a supplement that acts by stimulating the urea cycle and glutamine synthesis, an important mechanism in the detoxification of ammonia.Citation85 Good-quality data from meta-analyses have demonstrated that l-ornithine-l-aspartate is more effective in improvement of symptoms and reduction in serum ammonia levels in cirrhotic patients with CHE and HE, when compared to placebo or no intervention control.Citation86
Intravenous albumin infusion is commonly used in patients with cirrhosis after reports showed that it improves outcomes in cirrhotic patients with spontaneous bacterial peritonitis or hepatorenal syndrome. The mechanism of action is thought to be improvement in circulatory dysfunction by plasma expansion and reduction of oxidative stress.Citation87 Two randomized clinical trials have, however, demonstrated that albumin infusion does not have a significant impact on HE in cirrhotics.Citation88,Citation89
A more promising development is the use of ammonia scavengers, such as glycerol phenylbutyrate (GPB) and ornithine phenylacetate, which lowers ammonia levels by providing substrates as an alternative pathway to urea for nitrogen metabolism.Citation90 The Phase IIb study (HALT-HE [NCT00999167]) on the potential treatment with GPB and ornithine phenylacetate is now complete, and results are awaited along with the Phase III study (not yet registered with clinicaltrials.gov).
See for a summary of other potential therapies for HE.
Table 5 Summary of other potential therapies for HE
Treatment-resistant HE
HE resistant to optimal medical treatment should raise the suspicion of large portosystemic shunts, and these can be treated by embolization therapy.Citation91 Evidence from studies suggest that the procedure decreases hospital admissions and improves survival, despite the risks of de novo gastroesophageal varices, worsening ascites and renal dysfunction due to contrast-induced nephropathy.Citation92,Citation93 In Type B HE caused by iatrogenic shunts created via transjugular intrahepatic portosystemic shunt (TIPS) procedure, a reduction of the stent, that is, reducing caliber of the TIPS, can lead to clinical improvement and should be considered in patients with severe post-TIPS HE.
Liver transplantation is the only definitive treatment option for resistant HE and should be considered in suitable candidates presenting with HE. Discussions with transplant centers should be initiated early. Strict criteria apply and liver transplantation is not without risk, but an assessment should be considered in all patients with HE, provided that investigations for potential neurodegenerative disorders that may worsen posttransplant have been undertaken.Citation47
Unfortunately, there are some patients (e.g., with significant comorbidities such as heart failure and disease, renal disease and coexisting malignancy) with resistant HE who are not suitable candidates for liver transplantation. In these patients, the emphasis of care should then be switched to controlling distressing symptoms and providing holistic support for the patient and caregivers. Multidisciplinary team input is needed, and support should be provided for both patients and caregivers.Citation69 Education about preventing constipation is paramount, and it may be necessary for administration of phosphate enemas in the community. Despite their relative contraindication in end-stage liver disease, benzodiazepines and opioids may be required, as priorities change to reduce distress rather than preserve lucency.Citation94
Future prospects
The management of HE has evolved over the last 10 years with the addition on rifaximin into current treatment guidelines. There has been an increase in the number of randomized controlled trials with good-quality evidence describing the use of lactulose, rifaximin, GPB and others. More studies are needed to ascertain the pathophysiology that will lead to new treatment options of HE. Results of several randomized clinical trials, such as HALT-HE and STOP-HE, are awaited.
In terms of pathophysiology, there should be an emphasis to discover how the different concepts act synergistically to lead to development of HE. The research into gut microbiota seems promising, and perhaps a look into the role of nutritional therapy in modulating gut microbiota would be of interest.
There is some evidence for the use of liver support systems such as the Molecular Adsorbent Recirculating System and Prometheus device. They act by removing circulating toxins that accumulate in the blood due to liver dysfunction.Citation95 Both devices were well tolerated by patients in liver failure, and their effects on HE have been investigated in randomized trials.Citation96 The MARS study showed that using the MARS system caused significant improvement in HE and responded significantly faster when compared to standard medical therapy.Citation97 The Relief study also showed similar benefits, although survival benefits were not demonstrated.Citation98 These devices may have a role in patients with incapacitating HE as a bridge to transplantation, but may not be appropriate in all causes, given the requirement for central venous access and the nonfinite timeline for treatment. More studies into the cost-effectiveness are needed, together with concerns over the development of sepsis.
Conclusion
HE is a significant contributor to morbidity in patients with cirrhosis associated with end-stage liver disease. The unpredictable nature of HE severely impacts on the quality of life for patients and relatives. Research into the complexities of HE has led to development of new and upcoming treatment options. Avoiding the precipitants of HE and combination treatment with lactulose and rifaximin remain the mainstay of treatment. Future studies should aim to further identify novel mechanisms and targets for future treatments with the hope of translating this into real benefit for patients with HE.
Disclosure
The authors report no conflicts of interest in this work.
References
- American Association for the Study of Liver DiseasesEuropean Association for the Study of the LiverHepatic Encephalopathy in Chronic Liver Disease: 2014 Practice Guideline by the European Association for the Study of the Liver and the American Association for the Study of Liver DiseasesJ Hepatol201461364265925015420
- NabiEThackerLRWadeJBDiagnosis of covert hepatic encephalopathy without specialized testsClin Gastroenterol Hepatol201412813841389.e224362049
- JepsenPOttPAndersenPKSorensenHTVilstrupHClinical course of alcoholic liver cirrhosis: a Danish population-based cohort studyHepatology20105151675168220186844
- MokdadAALopezADShahrazSLiver cirrhosis mortality in 187 countries between 1980 and 2010: a systematic analysisBMC Med201412114525242656
- Public Health England. [webpage on the Internet]Deaths from Liver Disease: Implications for end of life care in England2017Accessed September 28, 2017
- PatidarKRThackerLRWadeJBCovert hepatic encephalopathy is independently associated with poor survival and increased risk of hospitalizationAm J Gastroenterol2014109111757176325178701
- BajajJSSaeianKSchubertCMMinimal hepatic encephalopathy is associated with motor vehicle crashes: the reality beyond the driving testHepatology20095041175118319670416
- RomanECordobaJTorrensMMinimal hepatic encephalopathy is associated with fallsAm J Gastroenterol2011106347648220978484
- DharelNBajajJSDefinition and nomenclature of hepatic encephalopathyJ Clin Exp Hepatol20155Suppl 1S37S4126041955
- ShawcrossDJalanRThe pathophysiologic basis of hepatic encephalopathy: central role for ammonia and inflammationCell Mol Life Sci20056219-202295230416158192
- DesjardinsPDuTJiangWPengLButterworthRFPathogenesis of hepatic encephalopathy and brain edema in acute liver failure: role of glutamine redefinedNeurochem Int201260769069622382077
- STAHLJStudies of the blood ammonia in liver disease. Its diagnostic, prognostic, and therapeutic significanceAnn Intern Med19635812413978712
- PhearEASherlockSSummerskillWHBlood-ammonium levels in liver disease and hepatic comaLancet1955268686983684014368880
- OngJPAggarwalAKriegerDCorrelation between ammonia levels and the severity of hepatic encephalopathyAm J Med2003114318819312637132
- KundraAJainABangaABajajGKarPEvaluation of plasma ammonia levels in patients with acute liver failure and chronic liver disease and its correlation with the severity of hepatic encephalopathy and clinical features of raised intracranial tensionClin Biochem200538869669915963970
- BernalWHallCKarvellasCJAuzingerGSizerEWendonJArterial ammonia and clinical risk factors for encephalopathy and intracranial hypertension in acute liver failureHepatology20074661844185217685471
- KumarRShalimarSharmaHPersistent hyperammonemia is associated with complications and poor outcomes in patients with acute liver failureClin Gastroenterol Hepatol201210892593122521861
- HolecekMEvidence of a vicious cycle in glutamine synthesis and breakdown in pathogenesis of hepatic encephalopathy-therapeutic perspectivesMetab Brain Dis201429191723996300
- RoseCButterworthRFZayedJManganese deposition in basal ganglia structures results from both portal-systemic shunting and liver dysfunctionGastroenterology1999117364064410464140
- SpahrLButterworthRFFontaineSIncreased blood manganese in cirrhotic patients: relationship to pallidal magnetic resonance signal hyperintensity and neurological symptomsHepatology1996245111611208903385
- Rivera-ManciaSRiosCMontesSManganese and ammonia interactions in the brain of cirrhotic rats: effects on brain ammonia metabolismNeurochem Res20123751074108422290316
- RaiRSaraswatVADhimanRKGut microbiota: its role in hepatic encephalopathyJ Clin Exp Hepatol20155Suppl 1S29S3626041954
- BajajJSHylemonPBRidlonJMColonic mucosal microbiome differs from stool microbiome in cirrhosis and hepatic encephalopathy and is linked to cognition and inflammationAm J Physiol Gastrointest Liver Physiol20123036G675G68522821944
- ZhangZZhaiHGengJLarge-scale survey of gut microbiota associated with MHE Via 16S rRNA-based pyrosequencingAm J Gastroenterol2013108101601161123877352
- LiuQDuanZPHaDKBengmarkSKurtovicJRiordanSMSynbiotic modulation of gut flora: effect on minimal hepatic encephalopathy in patients with cirrhosisHepatology20043951441144915122774
- BajajJSHeumanDMHylemonPBAltered profile of human gut microbiome is associated with cirrhosis and its complicationsJ Hepatol201460594094724374295
- TsaiCFChenMHWangYPProton pump inhibitors increase risk for hepatic encephalopathy in patients with cirrhosis in a population studyGastroenterology2017152113414127639806
- HanaiTShirakiMWatanabeSSarcopenia predicts minimal hepatic encephalopathy in patients with liver cirrhosisHepatol Res Epub2017215
- DavuluriGKrokowskiDGuanBJMetabolic adaptation of skeletal muscle to hyperammonemia drives the beneficial effects of l-leucine in cirrhosisJ Hepatol201665592993727318325
- LesIDovalEGarcia-MartinezREffects of branched-chain amino acids supplementation in patients with cirrhosis and a previous episode of hepatic encephalopathy: a randomized studyAm J Gastroenterol201110661081108821326220
- GluudLLDamGLesIBranched-chain amino acids for people with hepatic encephalopathyCochrane Database Syst Rev20159CD001939
- QiuJThapaliyaSRunkanaAHyperammonemia in cirrhosis induces transcriptional regulation of myostatin by an NF-kappaB-mediated mechanismProc Natl Acad Sci U S A201311045181621816724145431
- GuevaraMBaccaroMETorreAHyponatremia is a risk factor of hepatic encephalopathy in patients with cirrhosis: a prospective study with time-dependent analysisAm J Gastroenterol200910461382138919455124
- CórdobaJGottsteinJBleiATChronic hyponatremia exacerbates ammonia-induced brain edema in rats after portacaval anastomosisJ Hepatol19982945895949824268
- JalanROlde DaminkSWHayesPCDeutzNELeeAPathogenesis of intracranial hypertension in acute liver failure: inflammation, ammonia and cerebral blood flowJ Hepatol200441461362015464242
- AggarwalSKramerDYonasHCerebral hemodynamic and metabolic changes in fulminant hepatic failure: a retrospective studyHepatology199419180878276371
- MariniJCBroussardSRHyperammonemia increases sensitivity to LPSMol Genet Metab200688213113716497529
- BaiGRama RaoKVMurthyCRPanickarKSJayakumarARNorenbergMDAmmonia induces the mitochondrial permeability transition in primary cultures of rat astrocytesJ Neurosci Res200166598199111746427
- AldridgeDRTranahEJShawcrossDLPathogenesis of hepatic encephalopathy: role of ammonia and systemic inflammationJ Clin Exp Hepatol20155Suppl 1S7S2026041962
- FerenciPLockwoodAMullenKTarterRWeissenbornKBleiATHepatic encephalopathy–definition, nomenclature, diagnosis, and quantification: final report of the working party at the 11th World Congresses of Gastroenterology, Vienna, 1998Hepatology200235371672111870389
- AmodioPMontagneseSGattaAMorganMYCharacteristics of minimal hepatic encephalopathyMetab Brain Dis2004193-425326715554421
- WeissenbornKEnnenJCSchomerusHRuckertNHeckerHNeuropsychological characterization of hepatic encephalopathyJ Hepatol200134576877311434627
- BajajJSMinimal hepatic encephalopathy matters in daily lifeWorld J Gastroenterol200814233609361518595126
- BajajJSWadeJBSanyalAJSpectrum of neurocognitive impairment in cirrhosis: implications for the assessment of hepatic encephalopathyHepatology20095062014202119787808
- StewartJSarkelaMKoivusaloAMFrontal electroencephalogram variables are associated with the outcome and stage of hepatic encephalopathy in acute liver failureLiver Transpl201420101256126524975240
- NardoneRTaylorACHöllerYBrigoFLochnerPTrinkaEMinimal hepatic encephalopathy: A reviewNeurosci Res201611111227153746
- VilstrupHAmodioPBajajJHepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the LiverHepatology201460271573525042402
- RahimiRSRockeyDCOveruse of Head Computed Tomography in Cirrhosis With Altered Mental StatusAm J Med Sci2016351545946627140703
- DonovanLMKressWLStrnadLCLow likelihood of intracranial hemorrhage in patients with cirrhosis and altered mental statusClin Gastroenterol Hepatol201513116516924907500
- InoueEHoriSNarumiYPortal-systemic encephalopathy: presence of basal ganglia lesions with high signal intensity on MR imagesRadiology199117925515552014310
- PujolAPujolJGrausFHyperintense globus pallidus on T1-weighted MRI in cirrhotic patients is associated with severity of liver failureNeurology199343165698423913
- GroverVPCrosseyMMFitzpatrickJAQuantitative magnetic resonance imaging in patients with cirrhosis: a cross-sectional studyMetab Brain Dis20163161315132526251205
- JiangMWangZTsauoJLiXBasal ganglia hyperintensity may be a marker of hepatic encephalopathy secondary to portosystemic shuntingClin Res Hepatol Gastroenterol2015391e5e625239699
- StewartCAReivichMLuceyMRGoresGJNeuroimaging in hepatic encephalopathyClin Gastroenterol Hepatol20053319720715765437
- Giménez-GarzóCGarcésJJUriosAThe PHES battery does not detect all cirrhotic patients with early neurological deficits, which are different in different patientsPLoS One2017122e017121128146589
- AllampatiSDuarte-RojoAThackerLRDiagnosis of minimal hepatic encephalopathy using stroop encephalApp: a multicenter US-Based, Norm-Based StudyAm J Gastroenterol20161111788626644276
- BajajJSThackerLRHeumanDMThe Stroop smartphone application is a short and valid method to screen for minimal hepatic encephalopathyHepatology20135831122113223389962
- CampagnaFMontagneseSRidolaLThe animal naming test: an easy tool for the assessment of hepatic encephalopathyHepatology201766119820828271528
- ArasaradnamRPMcFarlaneMLingKBreathomics–exhaled volatile organic compound analysis to detect hepatic encephalopathy: a pilot studyJ Breath Res2016101016s012
- GluudLLVilstrupHMorganMYNon-absorbable disaccharides versus placebo/no intervention and lactulose versus lactitol for the prevention and treatment of hepatic encephalopathy in people with cirrhosisCochrane Database Syst Rev20165CD003044
- CammaCFiorelloFTineFMarchesiniGFabbriAPagliaroLLactitol in treatment of chronic hepatic encephalopathy. A meta-analysisDig Dis Sci19933859169228482191
- DhimanRKGut microbiota and hepatic encephalopathyMetab Brain Dis201328232132623463489
- PohZChangPEA current review of the diagnostic and treatment strategies of hepatic encephalopathyInt J Hepatol2012201248030923133760
- DalalRMcGeeRGRiordanSMWebsterACProbiotics for people with hepatic encephalopathyCochrane Database Syst Rev20172CD00871628230908
- Viramontes HörnerDAveryAStowRThe effects of probiotics and symbiotics on risk factors for hepatic encephalopathy: a systematic reviewJ Clin Gastroenterol201751431232328059938
- MalaguarneraMGrecoFBaroneGGarganteMPToscanoMABifidobacterium longum with fructo-oligosaccharide (FOS) treatment in minimal hepatic encephalopathy: a randomized, double-blind, placebo-controlled studyDig Dis Sci200752113259326517393330
- Pratap MouliVBenjaminJBhushan SinghMEffect of probiotic VSL#3 in the treatment of minimal hepatic encephalopathy: a non-inferiority randomized controlled trialHepatol Res201545888088925266207
- RahimiRSSingalAGCuthbertJARockeyDCLactulose versus polyethylene glycol 3350–electrolyte solution for treatment of overt hepatic encephalopathy: the HELP randomized clinical trialJAMA Intern Med2014174111727173325243839
- CrossTJLiver disease in clinical practiceSpringer International PublishingUK2017
- Atif ZamanMMPHNutritional Management of Patients with Cirrhosis and Hepatic Encephalopathy2013 Available from http://www.jwatch.org/na31703/2013/07/19/nutritional-management-patients-with-cirrhosis-and-hepaticAccessed September 28, 2017
- AmodioPBemeurCButterworthRThe nutritional management of hepatic encephalopathy in patients with cirrhosis: international society for hepatic encephalopathy and nitrogen metabolism consensusHepatology2017581325336
- Chavez-TapiaNCCesar-ArceABarrientos-GutiérrezTVillegas-LópezFAMéndez-SanchezNUribeMA systematic review and meta-analysis of the use of oral zinc in the treatment of hepatic encephalopathyNutr J2013127423742732
- MousaNAbdel-RazikAZaherAThe role of antioxidants and zinc in minimal hepatic encephalopathy: a randomized trialTherap Adv Gastroenterol201695684691
- HawkinsRAJessyJMansAMChedidADeJosephMRNeomycin reduces the intestinal production of ammonia from glutamineAdv Exp Med Biol19943681251347741004
- MullenKDSanyalAJBassNMRifaximin is safe and well tolerated for long-term maintenance of remission from overt hepatic encephalopathyClin Gastroenterol Hepatol201412813901397.e224365449
- PedrettiGCalzettiCMissaleGFiaccadoriFRifaximin versus neomycin on hyperammoniemia in chronic portal systemic encephalopathy of cirrhotics. A double-blind, randomized trialItal J Gastroenterol19912341751781751811
- SharmaBCSharmaPLuniaMKSrivastavaSGoyalRSarinSKA randomized, double-blind, controlled trial comparing rifaximin plus lactulose with lactulose alone in treatment of overt hepatic encephalopathyAm J Gastroenterol201310891458146323877348
- BajajJSReview article: potential mechanisms of action of rifaximin in the management of hepatic encephalopathy and other complications of cirrhosisAliment Pharmacol Ther201643Suppl 1112626618922
- BassNMMullenKDSanyalARifaximin treatment in hepatic encephalopathyN Engl J Med2010362121071108120335583
- MohammadRARegalREAlanizCCombination therapy for the treatment and prevention of hepatic encephalopathyAnn Pharmacother201246111559156323092866
- SidhuSSGoyalOParkerRAKishoreHSoodARifaximin versus. lactulose in treatment of minimal hepatic encephalopathyLiver Int201636337838526201713
- SchulzCSchütteKKropfSRiMINI – the influence of rifaximin on minimal hepatic encephalopathy (MHE) and on the intestinal microbiome in patients with liver cirrhosis: study protocol for a randomized controlled trialTrials201617111126926775
- BajajJSO’LearyJGReddyKRSecond infections independently increase mortality in hospitalized patients with cirrhosis: the North American consortium for the study of end-stage liver disease (NACSELD) experienceHepatology20125662328233522806618
- LoftSSonneJDossingMAndreasenPBMetronidazole pharmacokinetics in patients with hepatic encephalopathyScand J Gastroenterol19872211171233563404
- NdrahaSHasanISimadibrataMThe effect of L-ornithine L-aspartate and branch chain amino acids on encephalopathy and nutritional status in liver cirrhosis with malnutritionActa Med Indones2011431182221339541
- BaiMYangZQiXFanDHanGl-ornithine-l-aspartate for hepatic encephalopathy in patients with cirrhosis: a meta-analysis of randomized controlled trialsJ Gastroenterol Hepatol201328578379223425108
- SortPNavasaMArroyoVEffect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bacterial peritonitisN Engl J Med1999341640340910432325
- Simon-TaleroMGarcia-MartinezRTorrensMEffects of intravenous albumin in patients with cirrhosis and episodic hepatic encephalopathy: a randomized double-blind studyJ Hepatol20135961184119223872605
- RiggioONardelliSPasqualeCNo effect of albumin infusion on the prevention of hepatic encephalopathy after transjugular intrahepatic portosystemic shuntMetab Brain Dis20163161275128126290375
- RockeyDCVierlingJMMantryPRandomized, double-blind, controlled study of glycerol phenylbutyrate in hepatic encephalopathyHepatology20145931073108323847109
- WijdicksEFHepatic encephalopathyN Engl J Med2016375171660167027783916
- LalemanWSimon-TaleroMMaleuxGEmbolization of large spontaneous portosystemic shunts for refractory hepatic encephalopathy: a multicenter survey on safety and efficacyHepatology20135762448245723401201
- AnJKimKWHanSLeeJLimYSImprovement in survival associated with embolisation of spontaneous portosystemic shunt in patients with recurrent hepatic encephalopathyAliment Pharmacol Ther201439121418142624754260
- EllulMAGholkarSACrossTJHepatic encephalopathy due to liver cirrhosisBMJ2015351h418726265724
- HassaneinTISchadeRRHepburnISAcute-on-chronic liver failure: extracorporeal liver assist devicesCurr Opin Crit Care201117219520321346566
- HassaneinTCurrent state of knowledge of hepatic encephalopathy (part IV): management of hepatic encephalopathy by liver support systemsMetab Brain Dis201732230330628013444
- HassaneinTIToftengFBrownRSJrRandomized controlled study of extracorporeal albumin dialysis for hepatic encephalopathy in advanced cirrhosisHepatology20074661853186217975845
- BanaresRNevensFLarsenFSExtracorporeal albumin dialysis with the molecular adsorbent recirculating system in acute-on-chronic liver failure: the RELIEF trialHepatology20135731153116223213075
- PanthamGPostAVenkatDEinstadterDMullenKDA new look at precipitants of overt hepatic encephalopathy in cirrhosisDig Dis Sci20176282166217328560484
- Romero-GomezMCordobaJJoverRValue of the critical flicker frequency in patients with minimal hepatic encephalopathyHepatology200745487988517393525
- LauridsenMMThieleMKimerNVilstrupHThe continuous reaction times method for diagnosing, grading, and monitoring minimal/covert hepatic encephalopathyMetab Brain Dis201328223123423299303
- AmodioPDel PiccoloFMarchettiPClinical features and survivial of cirrhotic patients with subclinical cognitive alterations detected by the number connection test and computerized psychometric testsHepatology19992961662166710347105
- BajajJSHafeezullahMFrancoJInhibitory control test for the diagnosis of minimal hepatic encephalopathyGastroenterology2008135515911600.e159118723018
- ZhuGQShiKQHuangSSystematic review with network meta-analysis: the comparative effectiveness and safety of interventions in patients with overt hepatic encephalopathyAliment Pharmacol Ther201541762463525684317
- KeQYangRNYeFImpairment of liver regeneration by the histone deacetylase inhibitor valproic acid in miceJ Zhejiang Univ Sci B201213969570622949360
- Brunetti-PierriNLanpherBErezAPhenylbutyrate therapy for maple syrup urine diseaseHum Mol Genet201120463164021098507
- HolecekMVodenicarovovaMPhenylbutyrate exerts adverse effects on liver regeneration and amino acid concentrations in partially hepatectomized ratsInt J Exp Pathol201697327828427381898
- Ventura-CotsMArranzJASimon-TaleroMSafety of ornithine phenylacetate in cirrhotic decompensated patients: an open-label, dose-escalating, single-cohort studyJ Clin Gastroenterol2013471088188723751856
- PatidarKRBajajJSCovert and Overt Hepatic Encephalopathy: Diagnosis and ManagementClin Gastroenterol Hepatol201513122048206126164219
- FerenciPHepatic encephalopathyGastroenterology Report20175213814728533911