 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Arterial stiffness has been identified as an independent predictor of prognostic outcomes for patients with cardiovascular disease. Although measurement of pulse wave velocity has been a widely accepted noninvasive approach to the assessment of arterial stiffness, its accuracy is hampered by changes in blood pressure. Taking the exponential relation between intravascular pressure and arterial diameter into consideration, a stiffness parameter can be obtained by plotting the natural logarithm of systolic–diastolic pressure ratio against the arterial wall extensibility. Cardio-ankle vascular index (CAVI), which is calculated based on the stiffness parameter thus obtained, is theoretically independent of changes in blood pressure. With this distinct advantage, CAVI has been widely applied clinically to assess arterial stiffness in subjects with known cardiovascular diseases including those with diagnosed atherosclerosis, coronary heart disease, and stroke as well as those at risk, including those with hypertension, diabetes, the elderly, and the obese. Because of its enhanced sensitivity, not only has the index been used to discern subtle changes in the disease process, it has also been utilized in studying normal individuals to assess their potential risks of developing cardiovascular diseases. The primary aims of assessing arterial stiffness using CAVI are not only to aid in early detection of arteriosclerosis to allow timely treatment and change in lifestyle, but also to quantitatively evaluate the progression of disease and the effectiveness of treatment. Despite its merit of being unaffected by blood pressure, discretion in data interpretation is suggested because an elevated CAVI represents not just vascular stiffness caused by pathological changes in the arterial wall, but can also be attributed to an increased vascular tone brought about by smooth muscle contraction. Moreover, certain patient populations, such as those with an ankle-brachial index < 0.9, may give falsely low CAVI and are suggested to be excluded from study.
Background: history and development
Arterial stiffness as an indicator of systemic diseases
“Stiffness” of the artery depends on its intrinsic elasticity. One commonly used indicator is pulse wave velocity (PWV) which increases with stiffness of the arterial wall. Although the major contributor to arterial stiffness is believed to be atherosclerosis, it has been shown that there is no notably significant correlation between PWV and the established risk factors for atherosclerosis with the exception of age and blood pressure.Citation1 Besides, PWV does not reflect early pathological changes of atherosclerosis until at its advanced stage when calcification develops in the atherosclerotic plaque.Citation2 The impact of age on the development of arterial stiffness, therefore, has aroused much interest.Citation3 Indeed, age-related increase in arterial stiffness has been shown to involve mainly the major arteries rather than the peripheral ones.Citation4 Interestingly, it has been found that the pathogenic mechanisms that contribute to arterial stiffness are different for atherosclerosis and aging. While the former affects mainly the arterial intima resulting in an increase in intima-media thickness and the formation of atherosclerotic plaques, the latter causes “medial degeneration” that involves increase in collagen and calcium deposits as well as fragmentation of elastin lamellae in the medial layer as a result of upregulation of proteolytic enzymes and possible repetitive cyclic stress on the arterial wall over a life span.Citation5,Citation6 Another chronic disease, diabetes mellitus, has also been shown to enhance the production of advanced glycation end-products (AGEs) that causes collagen crosslinking in the arterial medial layer which has been shown to be a significant contributor to arterial stiffness.Citation7
Arterial stiffness reflected in increased pulse wave velocity as a parameter for assessing vascular health
Arterial stiffness refers to the reduced distensibility and contractility of the arterial wall in response to pressure changes. The distensibility, which is defined as the relative change in volume in response to a change in blood pressure, is the ability of the artery to expand during systole.Citation8 PWV, on the other hand, is the velocity of propagation of the pressure wave along the arterial tree and is calculated by dividing the distance between two set points by the transit time needed for the wave to cover this distance.Citation9 PWV is increased by a reduction in the intrinsic elasticity of the arterial wall (ie, “stiffer” arteries) as in arteriosclerosis. Indeed, arterial stiffness, as measured by carotid-femoral PWV, has been reported to be an independent predictor of cardiovascular mortality and morbidity in patients with hypertension, type 2 diabetes, end-stage renal disease, and in the elderly.Citation10 Moreover, because of its noninvasiveness and high reproducibility of results,Citation11 it has been widely accepted as a clinical tool for diagnosing hypertension and following treatment outcomes.Citation12
Current methods of pulse wave velocity measurement and their limitations
By definition, PWV is the distance traveled by the wave divided by the time for the wave to cover that distance. However, this is the case only in a system with zero wave reflections. Actually, the transmission of the arterial pressure pulse does not reflect a true PWV because the former is a sum of vectors of the incident and reflected waves. To minimize the error in the calculation of the forward pulse velocity, one of the measuring points is typically chosen near the foot which is the lowest point of the flow wave relatively free of arterial wave reflection.Citation13 An alternate approach to measuring PWV takes advantage of the minimal interference with the incident pressure wave by the reflected wave during late diastole and early systole.Citation14 Based on the assumption, PWV can be determined by dividing the distance between two sites with the transit time between the foot points of an arterial pressure waveform captured at the two points of reference. Nevertheless, precise determination of the location of the foot points can be problematic.Citation15 Moreover, the original PWV involved velocity measurement between the carotid and femoral artery. However, acquisition of an accurate waveform with the procedure is somewhat complicated.Citation16 Therefore, instead of capturing the pressure wave, the use of Doppler ultrasound for measuring the flow wave has been suggested.Citation17 On the other hand, brachial-ankle pulse wave velocity (baPWV), which is a simplified approach with the use of air pressure and a volume plethysmograph that measures the PWV of the brachial artery (ba) and the ankle, was introduced.Citation16
One of the innate limitations of using PWV in the assessment of vascular pathologies is the fact that the measured or “functional” stiffness as reflected in the magnitude of PWV depends on the pressure of blood exerted on the arterial wall. Indeed, it has been demonstrated that the measured stiffness increases with a rise in loading pressure without any structural change.Citation18 For instance, baPWV is affected by blood pressure which is not compensated for during measurement.Citation19,Citation20 In addition, since the pulse pressure is measured by air pressure, any stimulus that creates pressure on an artery may affect the results.Citation16 Furthermore, albeit not substantial, PWV is lower during inspiration than expiration which causes a slight elevation in blood pressure.Citation21
Introduction of the cardio-ankle vascular index (CAVI) and its features
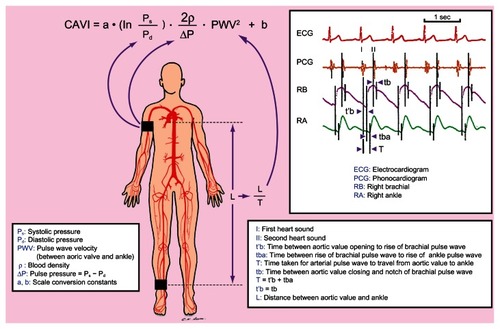
Taking the above issues into consideration, a CAVI, which is a stiffness and arteriosclerosis indicator of thoracic, abdominal, common iliac, femoral, and tibial arteries independent of arterial blood pressure, was proposed.Citation16,Citation22 Basically, CAVI is obtained by recording the distance from the level of the aortic valve (ie, brachial level) to the measuring point (ie, the ankle) and the time delay between the closing of the aortic valve to the detected change in arterial pressure wave at the set point.Citation16 Information for CAVI computation, including PWV, systolic and diastolic blood pressure as well as arterial pulse waveforms, can then be acquired through the electrocardiogram, cardiac phonogram, and the pressure cuffs on the testing subject at the reference points.
In comparison to baPWV, CAVI has two distinctive features. First, CAVI changes over a short period of time in response to alterations in circulatory condition. Second, CAVI reflects the state of smooth muscle contraction rather than changes in blood pressure.Citation23 CAVI has also been reported to represent both “functional” and “organic” stiffness.Citation24 The former represents the state of smooth muscle contraction that is subjected to changes in sympathetic tone and also pharmacological influence, whereas the latter signifies the physical properties such as sclerotic change of the arterial wall. While the administration of a selective beta 1-blocker, which decreases the contraction of cardiac muscle and blood pressure without affecting the vascular tone of arterial wall, led to a reduction in baPWV in human subjects, the CAVI stayed unchanged. On the other hand, infusion of an alpha-1 adrenergic receptor blocker, which decreases blood pressure through a relaxation of the smooth muscle of peripheral arteries, caused a diminished CAVI score.Citation25 The findings, therefore, highlight the influence of vascular tone on the magnitude of CAVI in spite of its blood pressure independence.
CAVI: theories and computation
In 1926, Otto FrankCitation26 defined the propagating velocity of the arterial pressure pulse, ΔP, as “characteristic pulse wave velocity (PWVc)” ie,
where K is the elastic modulus of luminal volume change per unit length of artery and ρ is the density of blood.
On the other hand, arterial stiffness can be defined by its distensibility, or preferably “compressibility”,Citation27 which is the relative change in volume in response to a change in blood pressure. That is: Compressibility = (ΔV/V)/ ΔP, where ΔV = change in volume; V = original volume; ΔP = change in pressure.
Since the elastic modulus, K, is defined as the ratio of stress (ie, the pulse pressure) to strain (ie, the fractional volume change) per unit length of artery, it is the inverse of compressibility. That is:
Since V = πR2 (where R: luminal radius), then dV = 2πRdR, and if ΔV (ie, luminal volume change per unit length of artery) is small, dV/V = ΔV/V = 2ΔR/R = 2ΔD/D (where D: luminal diameter), then Equationequation 2(2) may be written as:
In 1961, BergelCitation18 proposed that the hoop tension, T, in the artery wall of thickness, h, was related to the luminal pressure, P, by the equation:
Suppose that the changes in luminal radius, R, and arterial wall thickness, h, are negligible, then the relation between a small change in luminal pressure, ΔP, and the corresponding change in stress, ΔT, can be given by ΔT = ΔPR/h. The circumferential strain caused by ΔT will be [2π(R + ΔR) − 2πR]/2πR, giving ΔR/R.
Therefore, Einc, the static incremental Young’s modulus, which is stress/strain for the material of the arterial wall, can be defined as:
Hence, Einc, the static incremental Young’s modulus, can be rewritten as:
The equation was based on the assumption of blood flow inside an infinitely long, thin-walled elastic tube with an incompressible fluid and with the elasticity of the tube wall considered to be isotropic in the absence of any pressure reflections from the periphery.
Combining (Equation1(1) ), (Equation3
(3) ), and (Equation5
(5) ) gives:
The equation was commonly referred to as the Moens–Korteweg equation.Citation28
Alternatively, substituting (Equation2(2) ) into (Equation5
(5) ) gives: PWVc = √ΔP · D/(2ρ · ΔD), which can be rewritten as:
where PWV: pulse wave velocity; ΔP: pulse pressure; ρ: density of blood; D: luminal diameter; ΔD: change in luminal diameter.
EquationEquation (7)(7) thus derived provides a theoretical model that links the PWV, compressibility, pulse pressure, and blood density, it was first proposed by Bramwell and Hill.Citation29 Although the Bramwell and HillCitation29 equation was based on the Moens–Korteweg model, the former is believed to be more general because it does not assume thin-walled and homogeneous elastic arteries, as in the Moens–Korteweg model.Citation9
On the other hand, CAVI is calculated based on a stiffness parameter, β, which was first proposed by Hayahi et al in 1975 to assess the local stiffness of a blood vessel according to the change in vascular diameter in response to arterial pressure variance.Citation30 To fit into clinical practice, this blood pressure-independent parameter was later defined by Kawasaki et alCitation31 as:
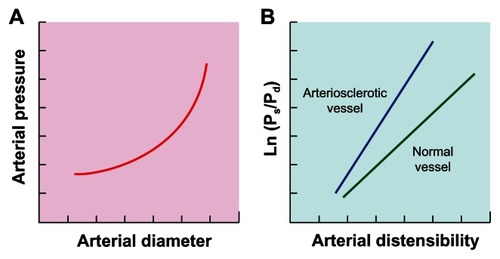
Using an echo phase tracing system, the proportional change in luminal diameter (ie, ΔD/D) can be obtained. Provided that an exponential relation exists between intravascular pressure and arterial diameter under stable physiological condition theoretically because of the transfer of stress from the stretchable elastin to the stiff collagen fibers in the arterial wall as blood pressure increases (),Citation32 plotting the natural logarithm of systolic–diastolic pressure ratio (In Ps/Pd) against the arterial wall extensibility (ΔD/D) would give a linear relation (). Therefore, the stiffness parameter β, which is the slope of the plot (), is theoretically independent of blood pressure at the time of measurement.Citation31 Hence, the higher the value of β the lower the compressibility (ie, the higher the stiffness) of the arterial wall, and the steeper the plot (). Clinically, since accurate assessment of arterial stiffness according to the change in vascular luminal diameter is hampered by the measurement on merely a local segment of artery and also the requirement for specific sonographic equipment, the proportional change in luminal diameter in EquationEquation 8(8) can be replaced by substituting (Equation7
(7) ) into (Equation8
(8) ):
Figure 1 (A) An exponential relation between blood pressure and arterial diameter under stable physiological condition. (B) Linear relation between natural logarithm of systolic (Ps) – diastolic (Pd) pressure ratio (In Ps/Pd) and arterial wall distensibility.
For scale conversion from PWV, the following formula can be applied:
where a and b are scale conversion constants.Citation22,Citation33
Hence, substituting (Equation9(9) ) into (Equation10
(10) ) gives:
PWV: pulse wave velocity from valve orifice to ankle; Ps: systolic blood pressure; Pd: diastolic blood pressure; ΔP: change in blood pressure; ρ: blood density.Citation22
CAVI: data acquisition in testing subjects
Equipment
The currently available equipment for measuring CAVI is model VaSera VS-1000 (Fukuda-Denshi Company, LTD, Tokyo, Japan) which is a portable machine resembling a cardiograph of dimensions 34.6 cm (W) × 24.0 cm (D) × 15.4 cm (H) and weight 7.2 kg with print-out function. The ankle-brachial index (ABI) and PWV can also be obtained through the machine that has been reported to be able to achieve 3.8% of the average coefficient of variation among five repeated measurements.Citation22
Procedure and parameters of measurement
A subject is allowed to assume a supine position with simultaneous blood pressure, electrocardiographic, and cardiac phonographic monitoring. Components required for the computation of CAVI can then be obtained, including systolic and diastolic blood pressures through the sphygmomanometer cuffs on the upper arm and ankle as well as PWV through dividing the distance between the aortic valve and the ankle (ie, L) by the time during which PWV propagates that distance (ie, T) (). T, in turn, can be calculated by the addition of the time between the opening of aortic valve detected on cardiac phonogram and the rise of the brachial pulse wave, t’b, and the time between the rise of the brachial pulse wave and the rise of the ankle pulse wave, tba. It is noteworthy that t’b and the time between the closing of aortic valve and the notch of the brachial pulse wave, tb, are theoretically equal ().Citation22 The scale conversion constants, a and b, in EquationEquation 11(11) on previous page are computed automatically in the equipment.
Figure 2 Schematic illustration of the acquisition of study parameters for computation of Cardio-Ankle Vascular Index (CAVI).
CAVI: data interpretation and precautions
Significance of results
EquationEquation 8(8) on previous page indicates that, theoretically, soft and flexible artery, which is considerably inflated by increased blood pressure, gives a low CAVI. Conceivably, arteriosclerotic artery, which is less inflated by an increase in blood pressure, gives a high value.
To establish the baseline CAVI scores according to age and gender in cardiovascular disease risk-free individuals as well as to compare the impact of cardiovascular pathologies on CAVI values, Namekata et al conducted a large-scale study on over 32 thousand individuals of age between 20 and 74 in Japan, including both sexes and those at different levels of risk for cardiovascular diseases after excluding those with history of heart disease, hypertension, stroke, diabetes, nephritis, and gout in 2011.Citation33 The study concluded that the baseline CAVI scores from the cardiovascular disease risk-free group are useful to serve as normal control values for subsequent studies and that CAVI is a meaningful parameter to screen individuals with moderate to advanced arteriosclerosis.Citation33
According to the manufacturer’s instructions, a CAVI less than 8.0 is supposed to be normal, whereas a value less than 9.0 but more than (or equal to) 8.0 is considered “borderline”. At the other end of the spectrum, a CAVI equal or more than 9.0 leads to the diagnosis of suspected arteriosclerosis.Citation34
Special circumstances in data interpretation
It is noteworthy that while an elevated CAVI is considered pathological, a reduced value does not necessarily represent superior vascular function and may be pathognomonic of certain diseases. For instance, it has been reported that a negative correlation exists between CAVI and serum insulin-like growth factor-I level which is increased in acromegalic patients. The authors, therefore, concluded that CAVI may serve as a useful parameter for the assessment of therapeutic outcomes in patients with acromegaly.Citation35
On the other hand, subjects with a low ankle-brachial index (ABI) <0.9 may have a severe arteriosclerotic femoral artery. These individuals may give a falsely low CAVI scoreCitation22 and, therefore, should be excluded from CAVI study. Under these circumstances, other noninvasive indices for the assessment of vascular function such as conventional or modified PWVCitation36 and those involving evaluation of vascular endothelial function including forearm-mediated vasodilation (FMD)Citation37 and dilatation index (DI)Citation38 may be utilized to provide additional information.
CAVI: clinical and research applications
Application in patients with known cardiovascular diseases and those at risk
Since its first introduction in 2004, CAVI has been widely applied to a variety of clinical studies particularly those involving the assessment of arterial stiffness in patients with established cardiovascular diseases and those at high risks for disease development.Citation39
Coronary heart disease
CAVI has been used to study patients with coronary heart disease which is the most notorious life-threatening condition in the developed world. Not only has CAVI been found to reflect plaque burden in the coronary artery of patients with an established diagnosis of coronary heart disease,Citation40,Citation41 it has also been demonstrated to be an independent parameter positively associated with coronary artery calcium score (CACS) and the degree of stenosis which reflects coronary atherosclerosis in asymptomatic subjects with abnormal glucose metabolism.Citation42 The clinical significance of CAVI in the assessment of patients with coronary heart disease has been further augmented by the discovery of its independent association with the Syntax score, which is a prognostic marker in patients with acute coronary syndrome, while neither traditional cardiovascular risk factor nor thrombolysis in myocardial infarction (TIMI) risk score was independent determinant of the Syntax score.Citation43 The findings, therefore, suggest that CAVI can be a useful tool not only to assess plaque burden in the coronary artery of patients with known coronary heart disease,Citation40,Citation41 but also to evaluate their prognosis and also the risk for subclinical coronary atherosclerosis in asymptomatic subjects.Citation42,Citation43 Finally, compared to baPWV, CAVI has been reported to be superior because of its significant correlation with left ventricular function and serum lipid profile as well as its discriminating ability for patients with angina pectoris out of all subjects with the complaint of chest pain.Citation44
Cerebrovascular disease
Cerebrovascular disease, another flagrant killer in the industrialized nations, has also been studied with CAVI. The clinical significance of CAVI in this aspect is not the evaluation of the severity of a full-blown disease, but its capability of detecting subtle and subclinical intracranial vascular pathologies instead. In addition to being an independent factor associated with cerebral microbleeds in patients with acute ischemic stroke,Citation45 CAVI has also been shown to be independently correlated with silent brain infarct.Citation46 Moreover, the presence of cerebral small vessel diseases in asymptomatic young and middle-aged subjects has also been found to be significantly associated with their CAVI scores.Citation47 Hence, the results of these studies indicate that, although CAVI is considered an indicator of arteriosclerosis in the major arteries between the aortic valve and the ankle, it may reflect the severity of cerebral arteriolosclerosis. It is noteworthy that CAVI has also been successfully applied to the evaluation of vascular recovery after intensive rehabilitation in chronic stroke patients.Citation48
Hypertension
Other than the potentially life-threatening diseases mentioned above, CAVI has also been utilized in the assessment of vascular health for those at risk of developing subsequent adverse cardiovascular outcomes. Hypertension, for instance, is by far one of the most frequently mentioned conditions associated with vascular stiffness and occupies the contents of nearly one-third of all CAVI-related literature. Positive correlations of CAVI with causative factors such as markers of inflammation and oxidative stress,Citation49–Citation51 indicator of left ventricular afterload,Citation52 and dysfunctions of other organ systemsCitation53 in hypertensive patients have already been reported. In addition, CAVI has also been used to investigate special populations at risk of developing hypertension. For example, Yoshida et al showed the superiority of CAVI over the conventional baPWV in differentiating preeclamptic from chronic hypertensive pregnant women.Citation54 Accordingly, CAVI has been adopted as a parameter for following treatment outcomes in hypertensive patients.Citation55–Citation57 The therapeutic potential of alternative treatment strategies against hypertension has also been evaluated with CAVI.Citation58
Diabetes mellitus
The association of CAVI with the disease progression of diabetes mellitus, which is another well-known condition that contributes to vascular stiffness, has also been extensively studied. Indeed, nearly one-fourth of CAVI-related publications retrieved from the PubMed database have mentioned diabetes in their contents. Not only has CAVI been proposed to better reflect the status of diabetes control compared to baPWV,Citation20 it has also been reported to be sensitive in detecting diabetes-associated complications. For instance, diabetic peripheral neuropathy was found to be significantly associated with an elevated CAVI without notable carotid intimal changes in patients with type 2 diabetes.Citation59 Moreover, an increased CAVI has also been shown to be correlated with microalbuminuria in type 2 diabetic patients,Citation60 underscoring the ability of CAVI in reflecting diabetes-related microvascular complications. In terms of the etiologies of diabetes-related arterial stiffness, not only has CAVI been demonstrated to be significantly correlated with the duration of diabetes, blood pressure, and serum total cholesterol level, but it has also been found to be positively associated with the concentrations of acute-phase reactants including high-sensitivity C-reactive protein, amyloid A protein, sialic acid, fibrinogen, and white blood cells that are known contributors to atherosclerosis in patients with type 2 diabetes mellitus.Citation61 Furthermore, CAVI has been utilized in assessing the effectiveness of pharmacological strategies against arterial stiffness in patients with type 2 diabetes.Citation62,Citation63
Metabolic syndrome and obesity
On the other hand, CAVI has also been shown to correlate positively with waist circumference and the number of components for the diagnosis of metabolic syndrome.Citation64 In addition, another study designed to identify the missing link between patients with obstructive sleep apnea and their elevated cardiovascular risks demonstrated that plasma level of pentraxin3, an indicator of inflammation, was independently correlated with CAVI.Citation65 The value of CAVI in monitoring the treatment outcomes for these patients has also been demonstrated.Citation64–Citation66 Furthermore, CAVI has been reported to reflect the positive therapeutic impact of diet supplement on vascular health in obese subjects.Citation67
Aging
Beside hypertension and diabetes, age is a well-known factor that contributes to an increased CAVI.Citation33,Citation68,Citation69 Age-related widening of pulse pressure is believed to be the major cause of age-related increase in prevalence of hypertension and has been attributed to arterial stiffening.Citation8 The results of a study on over 32 thousand Japanese subjects of age between 20 and 74 including both genders in 2011 not only showed that the proportion of cardiovascular disease risk-free subjects to all subjects decreased as age increased, but also a linear increase in the average age-specific baseline scores of CAVI in the cardiovascular disease risk-free group in both genders as their age advanced. Moreover, the average age-specific baseline scores of CAVI in the cardiovascular disease risk-free group were significantly greater among men than among women. Furthermore, as expected, the average age-specific baseline scores of CAVI in the cardiovascular disease high-risk group were significantly higher than those in the cardiovascular disease risk-free group in both genders of age over 40.Citation33 Another study conducted in patients under general anesthesia showed that CAVI was not reduced significantly in patients of age over 65 in comparison with their younger counterparts.Citation23 As CAVI is affected by a change in vascular tone, the sluggishness of the arterial wall to relax more likely represents age-related sclerosis of the arterial wall in the aged population after exclusion of possible smooth muscle contraction after general anesthesia.Citation70 Regarding the topic of aging in occupational and rehabilitation medicine, CAVI has been successfully applied to both longitudinalCitation73 and cross-sectionalCitation72 studies that focused on the elderly population.
Chronic kidney disease
Since cardiovascular diseases are the major causes of death in patients with chronic kidney diseases, monitoring arterial stiffness helps in detecting the presence and following the progression of cardiovascular pathologies in this patient population. However, the accuracy of conventional non-invasive arterial stiffness parameters such as PWV and baPWV are confounded by the elevated blood pressure in patients with renal diseases. CAVI, on the other hand, appears to be the parameter of choice because of its independence of blood pressure changes. A study on patients under chronic hemodialysis established a CAVI score of 7.55 as the cut-off value for suspecting the presence of cardiovascular diseases,Citation73 highlighting the use of CAVI as a screening parameter that would help in guiding subsequent treatment. Another investigation of cardiac dysfunction in patients on chronic hemodialysis demonstrated the successful application of CAVI in distinguishing patients with significant diastolic dysfunction from those without.Citation74
Taken together, it is obvious that not only has CAVI been adopted to quantitatively assess the severity of atherosclerosis in patients with known cardiovascular diseases, it also plays a significant role in following disease progression and treatment outcomes at a subclinical level for those at risk.
Extension of application
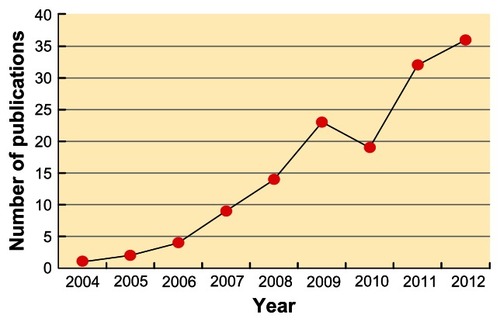
On the other hand, using the term “Cardio-Ankle Vascular Index” to search for the relevant literature in the PubMed database showed that the number of publications related to CAVI has been on the rise in recent years,Citation16 highlighting its increasing popularity as a reliable indicator of arterial stiffness (). Indeed, CAVI-related publications are even more when those not included in the PubMed domain are taken into consideration.
Figure 3 Changes in the number of Cardio-Ankle Vascular Index (CAVI)-related publications in the PubMed database since 2004.
The boost in literature can also be explained by the expanding application of CAVI not just to the evaluation of vascular function in subjects with established diagnoses of cardiovascular diseases and those at risk as mentioned previously, but also in other conditions that increased arterial stiffness at an early stage, such as large vessel vasculitis.Citation75 Moreover, the application has further been extended to include normal subjects exposed to factors of unknown cardiovascular influence. For instance, CAVI has been used to assess the vascular status in healthy individuals with a genetic predisposition to cardiovascular diseases, such as heterozygous familial hypercholesterolemia.Citation76 Other interesting studies also include the use of CAVI in comparing arterial stiffness between subjects of different ethnicitiesCitation77,Citation78 and those of the same ethnic group but of different geographical locations.Citation79
Furthermore, other than arterial stiffness, the scope of CAVI-related investigation goes further to include the general population. Not only has it been proposed to be a screening tool for atherosclerosis by Kadota et al based on their findings from over a thousand adults who showed strongly significant associations of CAVI scores with carotid intima-media thickness and homocysteine after adjustment for age and sex,Citation69 it has also been demonstrated to display significant negative correlation with renal function in apparently healthy subjects.Citation80 In addition, the correlation between CAVI and chronic inflammation has also been investigated in asymptomatic subjects who were found to exhibit a positive association between a subclinical impairment in vascular health represented by an elevated CAVI and a chronic inflammatory state as reflected in their increased concentrations of serum amyloid ACitation81 as well as high-sensitivity C-reactive protein.Citation82 Besides, CAVI has been successfully applied to the evaluation of the impact of extrinsic factors such as environmental particles in normal individuals.Citation83
Despite the lack of difference in arterial stiffness between the study groups as measured by conventional parameters, CAVI has been shown to reflect subtle differences at metabolicCitation20,Citation64 and cellular levels.Citation19 It is, therefore, not surprising that it can be used in the general population for detecting and assessing the severity of subclinical vascular anomalies. Being blood pressure-independent may be one of the bestowed merits that enhance its sensitivity and extend its applicability for these purposes.
Clinical and research significance
Provided that CAVI is sensitive in discerning subtle functionalCitation19 and organicCitation84 changes in major arteries before actual functional impairment, it is invaluable in preventive medicine. Not only can it be used to quantitatively assess the extent of arteriosclerosis in the major arteries between the aortic valve and the ankle in patients with known cardiovascular diseases, but it can also be applied to the screening of individuals at a subclinical stage.Citation33 After a baseline value has been established, subsequent follow-ups of the CAVI scores can then serve as reliable indicators of disease progression that are valuable in evaluating the outcomes after physicalCitation48 or pharmacologicalCitation85–Citation87 treatment. The cardiovascular impact of intrinsicCitation35,Citation76 or extrinsicCitation58,Citation67,Citation83 factors can also be evaluated in well-controlled studies.
CAVI: limitations in application
Potential variations and errors in data interpretation
A study on over 200 healthy Japanese and an equivalent number of Russian counterparts has demonstrated a significantly elevated CAVI in the Russian subjects.Citation77 Although it seems reasonable to conclude that the Russian examinees were at an increased risk for cardiovascular diseases when higher disease prevalence in Russia compared to that in Japan was taken into account,Citation77 anthropometric and genetic variations of ethnic origins that may contribute to the difference in CAVI scores between the two groups cannot be completely ruled out. In addition, genetic difference in disease susceptibility and response among different ethnic groups may exist. Two other studies involving the comparison of CAVI between healthy Mongolian and Japanese subjectsCitation78 and those with hypertension and diabetes mellitusCitation88 also raise the same concern. Indeed, of the 140 CAVI-related publications retrieved from the PubMed database, the vast majority are of Asian origins, mostly Japan. In addition to the novelty and limited availability of the equipment, a lack of reliable databases of specific ethnic groups for reference may be another reason for the dearth of CAVI-related research in non-Asian countries.
Limitations
Since CAVI reflects both organic and functional stiffness, it is inappropriate to consider it a pure indicator of organic changes in the arterial wall as in arteriosclerosis and aging.Citation25 Although the index is independent of blood pressure, it is affected by the state of smooth muscle contraction as reflected in the changes in vascular tone.Citation26 Caution, therefore, has to be taken in data interpretation. On the other hand, since an increased sympathetic tone is characteristic of some disease entities as in resistant hypertension and heart failure,Citation89 the ability of CAVI to record the changes may be a distinct advantage rather than a limitation under these circumstances.
CAVI: future direction and speculations
In addition to being a validated blood pressure-independent parameter for assessing arterial stiffness, CAVI has also served as a useful tool for supporting the reliability and validity of novel methodologies in the evaluation of arterial stiffness and cardiovascular risks.Citation36,Citation90–Citation93 In this way, CAVI helps in the development of new diagnostic technologies in cardiovascular medicine.
On the other hand, provided that significant ethnic differences exist in CAVI,Citation33,Citation77,Citation78 anthropometrical variations among individuals of different ethnic origins may have to be taken into account. Thus, reliable database from studies on large populations of different ethic groups other than that of Asians may have to be established to extend the application of CAVI as a reliable tool for assessing arterial stiffness to a global scale. This is of importance especially when considering the fact that an industrialized western nation like the United States has a remarkably higher mortality from coronary heart disease compared to that in Japan where the available database was built.Citation33
The acceptance of CAVI as a reliable tool for early identification of cardiovascular diseases worldwide may be a major breakthrough in preventive medicine because it triggers the alarm at an early stageCitation43 and allows timely treatment as well as modification in lifestyle.Citation94 Furthermore, for subjects with known cardiovascular diseases and also those at high risk, CAVI may be a sensitive indicator in following disease progressionCitation80,Citation95 and monitoring treatment outcomes.Citation48,Citation85–Citation87 Since a large-scaled study has only been recently performed to establish a reliable database for the Asian population,Citation33 it is anticipated that CAVI-related research will continue to bloom for the coming years.
Conclusion
CAVI has been widely applied clinically to assess arterial stiffness in myriad populations with known cardiovascular diseases including subjects with diagnosed atherosclerosis, coronary heart disease, and stroke as well as those at risk, including those with hypertension, diabetes, the elderly, and the obese. Because of its sensitivity, not only has the index been used to discern subtle changes in the disease process, it has also been utilized in studying normal individuals to assess their potential risks of developing cardiovascular diseases. The primary aims of assessing arterial stiffness using CAVI are not merely to aid in early detection of arteriosclerosis to allow timely treatment and change in lifestyle, but also to quantitatively evaluate the progression of disease and the effectiveness of treatment. In spite of its merit of being unaffected by blood pressure, discretion in data interpretation is suggested because an elevated CAVI represents not just vascular stiffness caused by pathological changes in the arterial wall, it can also be attributed to an increased vascular tone brought about by smooth muscle contraction. Finally, certain patient populations, such as those with an ABI < 0.9, may give falsely low CAVI and are suggested to be excluded from study.
Disclosure
The author reports no conflicts of interest in this work.
References
- CeceljaMChowienczykPDissociation of aortic pulse wave velocity with risk factors for cardiovascular disease other than hypertension: a systematic reviewHypertension20095461328133619884567
- van PopeleNMGrobbeeDEBotsMLAssociation between arterial stiffness and atherosclerosis: the Rotterdam StudyStroke200132245446011157182
- AvolioAPChenSGWangRPZhangCLLiMFO’RourkeMFEffects of aging on changing arterial compliance and left ventricular load in a northern Chinese urban communityCirculation198368150586851054
- MitchellGFPariseHBenjaminEJChanges in arterial stiffness and wave reflection with advancing age in healthy men and women: the Framingham Heart StudyHypertension20044361239124515123572
- YasminMcEnieryCMO’ShaughnessyKMVariation in the human matrix metalloproteinase-9 gene is associated with arterial stiffness in healthy individualsArterioscler Thromb Vasc Biol20062681799180516709939
- O’RourkeMFHashimotoJMechanical factors in arterial aging: a clinical perspectiveJ Am Coll Cardiol200750111317601538
- CormanBDuriezMPoitevinPAminoguanidine prevents age-related arterial stiffening and cardiac hypertrophyProc Natl Acad Sci U S A1998953130113069448326
- CeceljaMChowienczykPRole of arterial stiffness in cardiovascular diseaseJ R Soc Med Cardiovasc Dis2012111
- DoguiAKachenouraNFrouinFConsistency of aortic distensibility and pulse wave velocity estimates with respect to the Bramwell-Hill theoretical model: a cardiovascular magnetic resonance studyJ Cardiovasc Magn Reson2011131121272312
- LaurentSCockcroftJVan BortelLExpert consensus document on arterial stiffness: methodological issues and clinical applicationsEur Heart J200627212588260517000623
- BlacherJAsmarRDjaneSLondonGMSafarMEAortic pulse wave velocity as a marker of cardiovascular risk in hypertensive patientsHypertension19993351111111710334796
- ManciaGDe BackerGDominiczakA2007 Guidelines for the Management of Arterial Hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC)J Hypertens20072561105118717563527
- McDonaldDABlood Flow in Arteries2nd edEdward Arnold1974
- BramwellJCHillAVVelocity transmission of the pulse wave and elasticity of arteriesLancet19221995149891892
- MilnorWRHemodynamics2nd edWilliams and WilkinsBaltimore1989
- YambeTYoshizawaMSaijoYBrachio-ankle pulse wave velocity and cardio-ankle vascular index (CAVI)Biomed Pharmacother200458Suppl 1S95S9815754845
- LaogunAANewmanDLGoslingRGComparison of pulse wave velocity measured by Doppler shifted ultrasound and electromagnetic flowmetryUltrasound Med Biol197834367371148762
- BergelDHThe static elastic properties of the arterial wallJ Physiol1961156344545716992075
- TakahashiMShibaTHiranoKHitsumotoTShiraiKAcute decrease of cardio-ankle vascular index with the administration of beraprost sodiumJ Atheroscler Thromb201219547948422659532
- IbataJSasakiHKakimotoTCardio-ankle vascular index measures arterial wall stiffness independent of blood pressureDiabetes Res Clin Pract200880226527018242761
- AsmarRArterial Stiffness and Pulse Wave Velocity: Clinical ApplicationsAmsterdam, The NetherlandsElsevier1999
- ShiraiKUtinoJOtsukaKTakataMA novel blood pressure-independent arterial wall stiffness parameter; cardio-ankle vascular index (CAVI)J Atheroscler Thromb200613210110716733298
- KimBTakadaKOkaSMisakiTInfluence of blood pressure on cardio-ankle vascular index (CAVI) examined based on percentage change during general anesthesiaHypertens Res201134677978321471974
- ShiraiKAnalysis of vascular function using the cardio-ankle vascular index (CAVI)Hypertension Research20113468468521642994
- ShiraiKSongMSuzukiJContradictory effects of beta1- and alpha1- aderenergic receptor blockers on cardio-ankle vascular stiffness index (CAVI) – CAVI independent of blood pressureJ Atheroscler Thromb2011181495521071883
- FrankODDie Theorie de PulswellenThe Pulsewellen TheoryZtschr Biol19268591130 German
- GoslingRGBudgeMMTerminology for describing the elastic behavior of arteriesHypertension20034161180118212756217
- BramwellJCHillAVThe velocity of the pulse wave in manProc R Soc Lond B192293298306
- MerillonJPFontenierGJLerallutJFAortic input impedance in normal man and arterial hypertension: its modification during changes in aortic pressureCardiovasc Res19821611646567168841
- HayashiGSatoNNiimiHHandaHMoritakeKOkumuraAAnalysis of vascular wall constitutive law with finite deformation theoryMedical Electronics and Biological Engineering197513293297
- KawasakiTTakeuchiKHasegawaMYagiSNakayamaSTakayamaYNoninvasive measurement of common carotid artery effect with echo phase tracking systemJournal of Japanese College of Angiology198222241248
- RoachMRBurtonACThe reason for the shape of the distensibility curves of arteriesCan J Biochem Physiol195735868169013460788
- NamekataTSuzukiKIshizukaNShiraiKEstablishing baseline criteria of cardio-ankle vascular index as a new indicator of arteriosclerosis: a cross-sectional studyBMC Cardiovasc Disord2011115121831311
- Fukuda-Denshi Company L, Tokyo, Japan http://www.fukuda.co.jp/english/products/special_features/vasera/cavi.htmlAccessed April 16, 2013
- MatsudaYKawateHMatsuzakiCReduced arterial stiffness in patients with acromegaly: non-invasive assessment by the cardio-ankle vascular index (CAVI)Endocr J2012
- WuHTHsuPCLiuABSix-channel ECG-based pulse wave velocity for assessing whole-body arterial stiffnessBlood Press201221316717622519467
- HuckCJBronasUGWilliamsonEBDraheimCCDuprezDADengelDRNoninvasive measurements of arterial stiffness: repeatability and interrelationships with endothelial function and arterial morphology measuresVasc Health Risk Manag20073334334917703642
- WuHTLeeCHLiuABArterial stiffness using radial arterial waveforms measured at the wrist as an indicator of diabetic control in the elderlyIEEE Trans Biomed Eng201058224325220923726
- HayashiSSignificance of plasma D-dimer in relation to the severity of atherosclerosis among patients evaluated by non-invasive indices of cardio-ankle vascular index and carotid intima-media thicknessInt J Hematol2010921768220559761
- HorinakaSYabeAYagiHCardio-ankle vascular index could reflect plaque burden in the coronary arteryAngiology201162540140821421633
- NakamuraKTomaruTYamamuraSMiyashitaYShiraiKNoikeHCardio-ankle vascular index is a candidate predictor of coronary atherosclerosisCirc J200872459860418362432
- ParkHEChoiSYKimMKOhBHCardio-ankle vascular index reflects coronary atherosclerosis in patients with abnormal glucose metabolism: Assessment with 256 slice multi-detector computed tomographyJ Cardiol201260537237622890071
- KorkmazLAdarAKorkmazAAAtherosclerosis burden and coronary artery lesion complexity in acute coronary syndrome patientsCardiol J201219329530022641549
- TakakiAOgawaHWakeyamaTCardio-ankle vascular index is superior to brachial-ankle pulse wave velocity as an index of arterial stiffnessHypertens Res20083171347135518957805
- ShimoyamaTIguchiYKimuraKStroke patients with cerebral microbleeds on MRI scans have arteriolosclerosis as well as systemic atherosclerosisHypertens Res2012351097597922739424
- SajiNKimuraKShimizuHKitaYSilent brain infarct is independently associated with arterial stiffness indicated by cardio-ankle vascular index (CAVI)Hypertens Res201235775676022378472
- ChoiSYParkHESeoHKimMChoSHOhBHArterial Stiffness Using Cardio-Ankle Vascular Index Reflects Cerebral Small Vessel Disease in Healthy Young and Middle Aged SubjectsJ Atheroscler Thromb2012
- TakatoriKMatsumotoDOkadaYNakamuraJShomotoKEffect of intensive rehabilitation on physical function and arterial function in community-dwelling chronic stroke survivorsTop Stroke Rehabil201219537738322982824
- OkuraTWatanabeSKurataMRelationship between cardio-ankle vascular index (CAVI) and carotid atherosclerosis in patients with essential hypertensionHypertens Res200730433534017541212
- MasugataHSendaSMuraoKAssociation between Urinary 8-Hydroxydeoxyguanosine, an Indicator of Oxidative Stress, and the Cardio-Ankle Vascular Index in Hypertensive PatientsJ Atheroscler Thromb201219874775522576471
- KotaniKYamadaSYamadaTKarioKTaniguchiNOxidized lipoprotein(a) and cardio-ankle vascular index (CAVI) in hypertensive subjectsHeart Vessels2012 [Epub ahead of print.]
- MasugataHSendaSInukaiMAssociation of cardio-ankle vascular index with brain natriuretic peptide levels in hypertensionJ Atheroscler Thromb201219325526222056595
- MasugataHSendaSOkadaHAssociation between arterial stiffness and pulmonary function in hypertensive patientsHypertens Res201235438839222113357
- YoshidaASugiyamaTSagawaNAssessment of the cardioankle vascular index in pregnant women complicated with hypertensive disordersISRN Obstet Gynecol2011 Article ID 91981615
- IshimitsuTNumabeAMasudaTAngiotensin-II receptor antagonist combined with calcium channel blocker or diuretic for essential hypertensionHypertens Res2009321196296819696778
- KinouchiKIchiharaABokudaKKurosawaHItohHDifferential Effects in Cardiovascular Markers between High-Dose Angiotensin II Receptor Blocker Monotherapy and Combination Therapy of ARB with Calcium Channel Blocker in Hypertension (DEAR Trial)Int J Hypertens2011284823
- KinouchiKIchiharaASakodaMKurauchi-MitoAMurohashi-BokudaKItohHEffects of telmisartan on arterial stiffness assessed by the cardio-ankle vascular index in hypertensive patientsKidney Blood Press Res201033430431220664284
- XuYYanHYaoJCardio Ankle Vascular Index evaluations revealed that co-treatment of ARB Anti-hypertension medication with Traditional Chinese Medicine improved arterial functionalityJ Cardiovasc Pharmacol2012
- KimESMoonSDKimHSDiabetic peripheral neuropathy is associated with increased arterial stiffness without changes in carotid intima-media thickness in type 2 diabetesDiabetes Care20113461403140521515840
- KimKJLeeBWKimHMAssociations between cardio-ankle vascular index and microvascular complications in type 2 diabetes mellitus patientsJ Atheroscler Thromb201118432833621224525
- WakabayashiIMasudaHAssociation of acute-phase reactants with arterial stiffness in patients with type 2 diabetes mellitusClin Chim Acta20063651–223023516199026
- UeharaGTakedaHRelative effects of telmisartan, candesartan and losartan on alleviating arterial stiffness in patients with hypertension complicated by diabetes mellitus: an evaluation using the cardio-ankle vascular index (CAVI)J Int Med Res20083651094110218831906
- MiyashitaYEndoKSaikiAEffect of ezetimibe monotherapy on lipid metabolism and arterial stiffness assessed by cardio-ankle vascular index in type 2 diabetic patientsJ Atheroscler Thromb201017101070107620644331
- LiuHZhangXFengXLiJHuMYambeTEffects of metabolic syndrome on cardio-ankle vascular index in middle-aged and elderly ChineseMetab Syndr Relat Disord20119210511021091187
- KasaiTInoueKKumagaiTPlasma pentraxin3 and arterial stiffness in men with obstructive sleep apneaAm J Hypertens201124440140721193850
- YoshihisaASuzukiSYamakiTImpact of adaptive servo-ventilation on cardiovascular function and prognosis in heart failure patients with preserved left ventricular ejection fraction and sleep-disordered breathingEur J Heart Fail2012
- UsuiTTochiyaMSasakiYEffects of natural S-equol supplements on overweight or obesity and metabolic syndrome in the Japanese, based on sex and equol statusClin Endocrinol (Oxf)2012
- ShibaTTakahashiMHoriYMaenoTShiraiKOptic Nerve Head Circulation Determined by Pulse Wave Analysis is Significantly Correlated with Cardio Ankle Vascular Index, Left Ventricular Diastolic Function, and AgeJ Atheroscler Thromb2012
- KadotaKTakamuraNAoyagiKAvailability of cardio-ankle vascular index (CAVI) as a screening tool for atherosclerosisCirc J200872230430818219171
- ShiraiKAnalysis of vascular function using the cardio-ankle vascular index (CAVI)Hypertens Res201134668468521642994
- LindholmHPunakallioALusaSSainioMPonocnyEWinkerRAssociation of cardio-ankle vascular index with physical fitness and cognitive symptoms in aging Finnish firefightersInt Arch Occup Environ Health201285439740321789686
- KawanoHIemitsuMGandoYHabitual rowing exercise is associated with high physical fitness without affecting arterial stiffness in older menJ Sports Sci201230324124622150337
- TakenakaTHoshiHKatoNCardio-ankle vascular index to screen cardiovascular diseases in patients with end-stage renal diseasesJ Atheroscler Thromb200815633934419060424
- KimuraHTakedaKTsuruyaKLeft ventricular mass index is an independent determinant of diastolic dysfunction in patients on chronic hemodialysis: a tissue Doppler imaging studyNephron Clin Pract20111171c67c7320689327
- MasugataHSendaSHimotoTDetection of increased arterial stiffness in a patient with early stage of large vessel vasculitis by measuring cardio-ankle vascular indexTohoku J Exp Med2009219210110519776526
- SoskaVDobsakPDusekLCardio-ankle vascular index in heterozygous familial hypercholesterolemiaJ Atheroscler Thromb201219545346122659529
- LiuHSaijoYZhangXComparative analysis of cardio-ankle vascular index between Japanese and RussiansEsashiMKIOhuchiNOsumiNSatoMYamaguchiTFuture Medical Engineering Based on Bionanotechnology: Proceedings of the Final Symposium of the Tohoku University 21st Century Center of Excellence ProgramImperial College PressLondon2006411418
- UurtuyaSTaniguchiNKotaniKComparative study of the cardio-ankle vascular index and ankle-brachial index between young Japanese and Mongolian subjectsHypertens Res200932214014419262473
- HirasadaKNiimuraHKubozonoTValues of cardio-ankle vascular index (CAVI) between Amami islands and Kagoshima mainland among health checkup examineesJ Atheroscler Thromb2012191698022104173
- KubozonoTMiyataMUeyamaKAssociation between arterial stiffness and estimated glomerular filtration rate in the Japanese general populationJ Atheroscler Thromb200916684084520032588
- KotaniKYamadaTMiyamotoMKarioKIshibashiSTaniguchiNThe correlation between the cardio-ankle vascular index (CAVI) and serum amyloid A in asymptomatic Japanese subjectsHeart Vessels201227549950421892740
- HigashiyamaAWakabayashiIKubotaYDoes High-Sensitivity C-Reactive Protein or Low-Density Lipoprotein Cholesterol Show a Stronger Relationship with the Cardio-Ankle Vascular Index in Healthy Community Dwellers?: the KOBE StudyJ Atheroscler Thromb2012
- WuCFLiYRKuoICHsuSCLinLYSuTCInvestigating the association of cardiovascular effects with personal exposure to particle components and sourcesSci Total Environ201243117618222683757
- TaguchiMIshigamiMNishidaMMoriyamaTYamashitaSYamamuraTRemnant lipoprotein-cholesterol is a predictive biomarker for large artery atherosclerosis in apparently healthy women: usefulness as a parameter for annual health examinationsAnn Clin Biochem201148Pt 433233721652686
- ObayashiSTerauchiMKatoKAkiyoshiMKubotaTRaloxifene temporarily reduces arterial stiffnessJ Obstet Gynaecol Res20103661229123521040206
- NagayamaDSaikiAEndoKImprovement of cardio-ankle vascular index by glimepiride in type 2 diabetic patientsInt J Clin Pract201064131796180120946343
- MiyoshiTDoiMHirohataSOlmesartan reduces arterial stiffness and serum adipocyte fatty acid-binding protein in hypertensive patientsHeart Vessels201126440841321063874
- UurtuyaSKotaniKTaniguchiNComparative study of atherosclerotic parameters in Mongolian and Japanese patients with hypertension and diabetes mellitusJ Atheroscler Thromb201017218118820124737
- ParatiGEslerMThe human sympathetic nervous system: its relevance in hypertension and heart failureEur Heart J20123391058106622507981
- ParkHEChoiSYKimHSKimMKChoSHOhBHEpicardial fat reflects arterial stiffness: assessment using 256-slice multidetector coronary computed tomography and cardio-ankle vascular indexJ Atheroscler Thromb201219657057622472214
- KorkmazLErkanHKorkmazAARelationship of aortic knob width with cardio-ankle vascular stiffness index and its value in diagnosis of subclinical atherosclerosis in hypertensive patients: a study on diagnostic accuracyAnadolu Kardiyol Derg201212210210622281788
- HimenoASatoh-AsaharaNUsuiTSalivary cortisol levels are associated with outcomes of weight reduction therapy in obese Japanese patientsMetabolism201261225526121871641
- MasugataHSendaSGodaFTissue Doppler echocardiography for predicting arterial stiffness assessed by cardio-ankle vascular indexTohoku J Exp Med2009217213914619212107
- NoikeHNakamuraKSugiyamaYChanges in cardio-ankle vascular index in smoking cessationJ Atheroscler Thromb201017551752520215706
- MartiRParramonDGarcia-OrtizLImproving interMediAte risk managementMARK studyBMC Cardiovasc Disord2011116121992621