
Abstract
Purpose
The enzyme immunoassay (EIA) has lower sensitivity for Clostridium difficile toxins A and B than the polymerase chain reaction in the diagnosis of C. difficile-associated diarrhea (CDAD). Furthermore, toxin positivity with EIA performed on C. difficile isolates from stool cultures may be observed even in patients with EIA glutamate dehydrogenase (GDH)-positive and toxin-negative stool specimens. It is unclear whether such patients should be treated as having CDAD.
Methods
The present study retrospectively compared patient characteristics, treatment, and diarrhea duration among three groups of patients who underwent stool EIA testing for CDAD diagnosis: a toxin-positive stool group (positive stool group; n=39); a toxin-negative stool/toxin-positive isolate group (discrepant negative/positive group, n=14); and a dual toxin-negative stool and isolate group (dual negative group, n=15). All cases included were confirmed to be GDH positive on EIA test.
Results
Patients’ backgrounds and comorbidities were not significantly different among three groups. No difference was observed among the three groups with regard to antimicrobial drug use before diarrhea onset. Treatment was received by 82.1% of the positive stool group compared to 7.1% of the discrepant positive/negative group and 0% of the dual negative group, while mean diarrhea duration was 10.6 days compared to 7.9 days (P=0.6006) and 3.4 days (P=0.0312), respectively.
Conclusion
Even without treatment, patients with toxin-negative stool specimens had shorter diarrhea duration than those with toxin-positive stool specimens even with toxin-positive isolates. These findings may suggest a limited need for CDAD treatment for GDH-positive patients and toxin-negative stool specimens.
Introduction
The anaerobic Gram-positive bacillus Clostridium difficile is a leading cause of antibiotic-associated diarrhea. Antimicrobial drugs disrupt the normal intestinal flora, allowing C. difficile to flourish and release C. difficile toxin A and toxin B that induce C. difficile-associated diarrhea (CDAD).Citation1,Citation2 Although CDAD is the common health-care-associated infectious disease, treatment or infection countermeasures are not applied to patients who do not present with diarrhea, including the tens of percents of asymptomatic adults who carry C. difficile in their intestines.Citation3–Citation5
CDAD diagnosis widely uses an enzyme immunoassay (EIA) kit to detect glutamate dehydrogenase (GDH) and toxins A and B (CD toxins) released by the C. difficile cells.Citation6 However, the low detection sensitivity of EIA for the CD toxins has been reported.Citation7,Citation8 Compared to the ≥90% detection sensitivity of polymerase chain reaction (PCR) and cytotoxigenic culture, EIA detection sensitivity is usually thought to be ~70% and has been reported to be as low as 50% or below.Citation7,Citation8
CDAD diagnosis is based on EIA results in Japan, because PCR has not been clinically available. If EIA testing is performed on C. difficile isolates cultured from the same specimen, an EIA GDH-positive and toxin-negative stool specimen may give a toxin-positive result. Bacterial content is higher in specimens containing colonies in solution compared to stool; therefore, toxin concentration may also be markedly higher.
If a specimen is GDH positive, follow-up testing with a nucleic acid amplification test, such as PCR, is recommended to compensate for the low sensitivity of EIA.Citation9–Citation11 PCR detection of tcdA or tcdB genes is the evidence for the presence of toxigenic C. difficile. While PCR findings have been reported to correlate well with clinical symptoms,Citation12 bacterial toxin proteins are not detected; therefore, positive results may also include patients carrying C. difficile without CDAD.Citation13 There is currently no definite method of determining whether diarrhea is caused by CD toxins present at concentrations below the detection sensitivity of EIA in patients with EIA toxin-negative stool or whether diarrhea is due to a cause other than CD toxins, despite the presence of C. difficile in the stool. Patients with toxin-negative stool may be dismissed as non-CDAD and thus overlooked in terms of treatment and infection countermeasures.
The present study investigated patients who had submitted stool specimens for CDAD diagnosis using EIA. Differences in patient characteristics, diarrhea duration, antibiotics usage, and severity were compared among patients with toxin-positive stool, toxin-negative stool but toxin-positive isolates, and toxin-negative stool and isolates.
The aim of the study is to investigate clinical history and need for the treatment of patients with GDH-positive and toxin-negative stool specimens.
Methods
Subjects
The present study retrospectively investigated patients (age ≥2 years) whose stool specimens were submitted to the microbiology laboratory at our institution for CD toxin testing between March 2013 and June 2014. Patients with C. difficile growth on stool culture and stool specimens confirmed to be GDH positive on EIA were included. Patients were divided into three groups based on the EIA CD toxin results in stool specimens and isolates obtained from bacterial culture: a toxin-positive stool group (positive stool group), a toxin-negative stool/toxin-positive isolate group (discrepant negative/positive group), and a dual toxin-negative stool and isolate group (dual negative group).
Bacteriological examination
C. Diff Quik Chek Complete (TechLab, Inc., Blacksburg, VA, USA) EIA was performed according to the manufacturer’s instructions to determine stool specimen positivity or negativity for GDH and CD toxins. Samples of toxin-negative stool specimens were inoculated onto cycloserine-cefoxitin mannitol agar (CCMA; Nissui Pharmaceutical Co., Ltd., Tokyo, Japan) and cultured for 48 hours under anaerobic conditions. EIA was performed on isolates from colonies using the same method as for the stool specimens to confirm the presence or absence of GDH and CD toxins. Isolates that were also GDH positive were determined to be C. difficile.
Clinical data collection
Bowel movement status was investigated using the electronic medical records (EMRs) of bowel movement frequency and characteristics. Patients with diarrhea or muddy stool passed ≥once per day or loose stool passed ≥four times per day were identified as symptomatic. Clinical data relating to white blood cell (WBC) count, C-reactive protein levels, serum albumin (Alb) levels, and body temperature on the day the specimens were submitted to the microbiology laboratory or, if measurements were unavailable for that day, on the day before or after, were also obtained from the EMR.
Statistical analysis
Analyses were performed using JMP Pro 11 (SAS Institute Inc., Cary, NC, USA). One-way analysis of variance was performed to compare the continuous variables among the three groups, and the Tukey–Kramer honest significant difference test was performed for multiple comparisons. Fisher’s exact test was used to analyze differences in proportions between the groups.
Ethics statement
The Ethics Committee of The University of Tokyo Graduate School of Medicine approved this study and waived the need for obtaining written informed consent from each patient.
Results
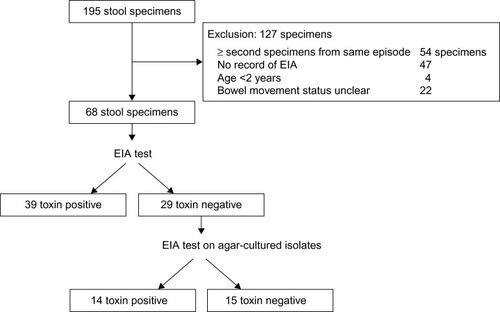
A flow chart of the study design and patient cohort is shown in . During the study period, 195 stool specimens were included. Of these, 127 specimens were excluded for the following reasons: ≥second of multiple specimens submitted during the same diarrhea episode (n=54), no record of EIA results for isolates obtained from stool culture (n=47), patient age <2 years (n=4), and bowel movement status unclear from EMR or fever chart (n=22). The remaining 68 specimens were included in the analysis. All specimens underwent EIA, identifying 39 toxin-positive and 29 toxin-negative stool specimens. EIA performed on agar-cultured isolates from toxin-negative stool specimens identified 14 toxin-positive and 15 toxin-negative isolates. All stool specimens and isolates (n=68) were GDH positive.
Figure 1 Flow chart of the study.
Note: All patients and isolates included in this study were GDH positive on EIA test.
Abbreviations: GDH, glutamate dehydrogenase; EIA, enzyme immunoassay.
shows the overall patient characteristics and clinical data for each group. No significant differences were observed in clinical characteristics such as the number of comorbidities, presence of malignant tumors, recent history of transplant, and use of tube feeding.
Table 1 Characteristics of patients
No significant differences were observed among the three groups with regard to number and respective administration frequencies of antimicrobial drugs received by patients within the 30 days prior to diarrhea onset ().
Table 2 Antimicrobial drugs received by patients within the 30 days prior to diarrhea
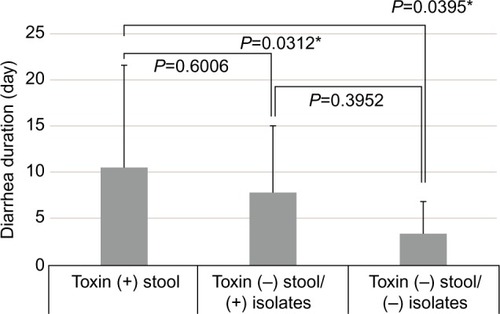
A significant difference was observed in mean diarrhea duration between the 39 patients in the positive stool group and the 29 patients with toxin-negative stool specimens (10.6 days vs 5.6 days; P=0.0179). Among the 29 patients with toxin-negative stool specimens, mean diarrhea durations were 7.9 days and 3.4 days for the discrepant negative/positive group and the dual-negative group, respectively. A significant difference was observed in diarrhea duration among the three groups (P=0.0395; ). Comparison between each group found a significant difference in diarrhea duration between the positive stool group and the dual-negative group (P=0.0312). No significant difference was observed between the positive stool group and the discrepant negative/positive group (P=0.6006); however, diarrhea duration tended to be longer in the positive stool group. No difference was observed in diarrhea duration between either of the groups with toxin-negative stool specimens (P=0.3952).
Figure 2 The mean duration of diarrhea for toxin (+) stool, toxin (−) stool/(+) isolates, and toxin (−) stool/(−) isolates.
Notes: P-values are P=0.0395 for all groups, P=0.6006 for toxin (+) stool vs toxin (−) stool/(+) isolates, P=0.3952 for toxin (−) stool/(+) isolates vs toxin (−) stool/(−) isolates, P=0.0312 for toxin (+) stool vs toxin (−) stool/(−) isolates. One-way analysis of variance was performed. *The significance level was P<0.05.
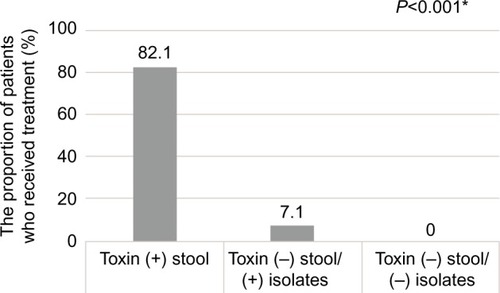
A significant difference was observed among the groups in the proportion of patients who received vancomycin or metronidazole treatment for CDAD: positive stool group, 82.1% (n=32); discrepant negative/positive group, 7.1% (n=1; vancomycin 500 mg three times daily for 13 days); and dual-negative group, 0% (n=0); P<0.001 (). In positive stool group, 27 patients received oral vancomycin, four received oral metronidazole, and one received oral metronidazole (250 mg four times daily for 11 days) followed by oral vancomycin (125 mg four times daily for 7 days). Of the patients receiving oral vancomycin alone in positive stool group, 70.4% received 125 mg four times daily, 18.5% received 500 mg four times daily, 7.4% received 500 mg three times daily, or 3.7% received 250 mg four times daily. The median duration of oral vancomycin was 11 days (range 1–25). Of the patients receiving oral metronidazole alone in positive stool group, 25% received 250 mg four times daily and 75% received 500 mg three times daily. The median duration of oral metronidazole was 14 days (range 10–15).
Figure 3 The rates of CDAD drug treatment in diarrhea for toxin (+) stool, toxin (−) stool/(+) isolates, and toxin (−) stool/(−) isolates.
Notes: Toxin (+) stool group was significantly higher rate than toxin (−) stool/(+) isolates and toxin (−) stool/(−) isolates groups. *P<0.001. Fisher’s exact test was used to analyze differences in proportions between the groups. The significance level was P<0.05.
Abbreviation: CDAD, Clostridium difficile-associated diarrhea.
The present findings demonstrated that, although significantly fewer patients in the discrepant negative/positive group received treatment compared to the positive stool group, diarrhea duration tended to be shorter.
No significant differences were observed among the groups with regard to inflammation findings, specifically WBC count, C-reactive protein levels, Alb levels, and body temperature, on the day stool specimens were submitted ().
Table 3 Comparison of clinical laboratory data and body temperature
Discussion
Of the 68 patients investigated in the present study, 39 (57.4%) had CD toxin-positive stool specimens, 14 (20.6%) had toxin-negative stool specimens but toxin-positive isolates, and 15 (22.1%) had both toxin-negative stool specimens and isolates.
Quinn et alCitation14 investigated 174 stool specimens and found that 133 (76.4%) were negative for both GDH and CD toxins, 18 (10.3%) were positive for both GDH and toxins, and 23 (13.2%) were positive for GDH but negative for toxins. In the present study, similar rates of GDH positivity were found in both toxin-positive and toxin-negative patients with regard to stool specimens. Similar results were obtained. These GDH-positive but toxin-negative patients represent the proportion of cases in which diagnosis and treatment requirements are unclear.
Symptom duration was significantly shorter in patients with toxin-negative rather than toxin-positive stool specimens, despite the lack of CDAD drug treatment in all but one of the 29 toxin-negative stool specimen patients. Furthermore, diarrhea duration also tended to be shorter in patients with toxin-negative stool specimens but toxin-positive isolates compared to those with toxin-positive stool specimens, despite significantly fewer discrepant negative/positive group patients receiving treatment. This suggests that patients who tested positive for C. difficile on culture but negative for toxins in their stool had milder symptoms, despite having toxin-positive isolates. Polage et alCitation15 found that EIA toxin-negative patients had significantly milder diarrhea, shorter diarrhea duration, and a lower mortality rate than toxin-positive patients. Patel et alCitation16 also reported that an infection with an EIA toxin-negative strain of C. difficile presents less severe clinical course, such as lower white blood cell counts and shorter length of hospital stay, than infection with EIA-positive C. difficile. Meanwhile, Baker et alCitation17 demonstrated that EIA toxin-negative patients present with milder clinical symptoms than toxin-positive patients. Conversely, other studies have reported no difference in clinical symptoms between toxin-negative and toxin-positive patients,Citation18 and a consensus has yet to be reached. The present analysis supported the reports of Polage et al,Citation15 Patel et al,Citation16 and Baker et al,Citation17 finding that mean diarrhea duration was significantly shorter in patients with toxin-negative (5.6 days) than toxin-positive (10.6 days) stool specimens, even with similar GDH positivity.
Furthermore, 13 of 14 patients with toxin-negative stool specimens but toxin-positive isolates did not receive CDAD treatment, and diarrhea duration in this group did not differ significantly from that in the dual-negative group. The group with toxin-negative isolates may have been infected with nontoxigenic C. difficile, while the toxin concentration in the stool and intestines of the group with toxin-positive isolates but toxin-negative stool specimens was likely too low to be detected by EIA, despite C. difficile toxigenicity. Akerlund et alCitation19 found that toxin concentrations in vitro from cultured C. difficile did not correlate with the toxin concentration in stool, which correlated with diarrhea frequency and abdominal pain. In addition to low toxin concentration, various intestinal factors, such as primary bile salt and human immunity, may contribute to lack of toxin detection in stool specimens in patients with discrepant negative/positive findings,Citation20–Citation26 because primary bile salts inhibit the growth of vegetative cells of C. difficile and human alpha-defensins cause loss of cytotoxicity of C. difficile toxin B. However, whatever the cause, diarrhea is comparatively mild in patients with toxin-negative stool, suggesting that severe symptoms are unlikely to develop at toxin concentrations below detection sensitivity. In this study, all cases were GDH positive. Toxin-negative patients with GDH positivity may be simply colonized with another cause of diarrhea, even if toxigenic C. difficile is isolated from stool.
Some classes of antibiotics, such as clindamycin, broad-spectrum cephalosporins, vancomycin, carbapenems, β-lactamase inhibitors combination antibiotics, and fluoroquinolones, are widely known risk factors for CDAD.Citation5,Citation27–Citation29 On the other hand, linezolid has been reported to have a potential protective role against the development of C. difficile infectionCitation30 and a good in vitro activity against C. difficile isolates in a human gut model of C. difficile infection.Citation31 In this study, 48% patients received β-lactamase inhibitors combination antibiotics and 25% patients received carbapenems. Linezolid was not used in the present study. Although cephamycin and fourth-generation cephalosporin tend to be more frequently used in toxin (+) stool group than other groups, there were no significant differences among the groups in antimicrobial drug use within the 30 days prior to toxin testing. Furthermore, no clear correlation was observed between type of antimicrobial drug administered prior to CDAD onset and the presence of toxins.
In the majority of patients, stool testing was conducted within several days of diarrhea onset, but no significant differences were observed among the groups with regard to clinical inflammation during the same period, suggesting no strong correlation between toxin detection and inflammation at the time of symptom onset. These findings indicate that it is difficult to predict toxin negativity or positivity prior to toxin testing based on drug use status or other test results.
The sensitivity of EIA for toxin detection is far inferior to that of PCR, which amplifies the toxin coding regions.Citation14,Citation32 However, PCR detects the presence of bacteria with toxin genes rather than toxin protein production; therefore, patients who are identified as toxin-positive on PCR may include carriers with diarrhea due to a cause other than toxin.Citation13 EIA directly measures the toxin proteins in stool and is thus more likely to reflect the patient’s actual disease status. While EIA is often associated with low sensitivity, it has a high positive predictive value,Citation14 making it an important test in determining treatment approach.
Limitations of the present study include the retrospective nature of the study, the small sample size, and the absence of molecular biological testing. Potential differences in the gene sequences related to toxin production between patients with toxin-positive stool and those with toxin-positive isolates were also not investigated. Hyper-virulent C. difficile strain, such as BI/NAP-1/027 strain, has emerged and causes severe and recurrent diseases. In Japan, the NAP-1 strain is low prevalence.Citation33 Recently, Polage et alCitation34 reported that patients with a positive molecular test result and a negative toxin immunoassay test result had outcomes that were comparable to patients without C. difficile by either method and that the prevalence of hypervirulent strain was 107 of 293 isolates. Thus, the strains may not affect the results of the study. However, further large number analysis is required to determine whether the patient groupings in the present study reflect bacterial genetic characteristics.
Conclusion
In this study, around half with toxin-negative stool specimens among the patients with EIA GDH-positive stool specimens had toxin-positive isolates. Since toxigenic C. difficile was thus present in their stool, these patients are at risk of transferring the bacteria to other patients and require care from the perspective of preventing hospital infection. However, from the perspective of treatment for individual patients, diarrhea duration is shorter in patients with toxin-negative stool specimens compared to those with toxin-positive stool specimens even without treatment. Nucleic acid amplification tests are recommended to detect toxinogenic C. difficile in stool for a diagnosis of CDAD; however, toxin production is not evaluated. These results may suggest a limited need for CDAD treatment for patients with GDH-positive and toxin-negative stool specimens.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this study.
References
- LyerlyDMKrivanHCWilkinsTDClostridium difficile: its disease and toxinsClin Microbiol Rev1988111183144429
- KellyCPPothoulakisCLaMontJTClostridium difficile colitisN Engl J Med199433042572628043060
- KellyCPLaMontJTClostridium difficile infectionAnnu Rev Med1998493753909509270
- BartlettJGClinical practice. Antibiotic-associated diarrheaN Engl J Med2002346533433911821511
- RupnikMWilcoxMHGerdingDNClostridium difficile infection: new developments in epidemiology and pathogenesisNat Rev Microbiol20097752653619528959
- SharpSERudenLOPohlJCHatcherPAJayneLMIvieWMEvaluation of the C. diff quik chek complete assay, a new glutamate dehydrogenase and A/B toxin combination lateral flow assay for use in rapid, simple diagnosis of Clostridium difficile diseaseJ Clin Microbiol20104862082208620375230
- PetersonLRMehtaMSPatelPALaboratory testing for Clostridium difficile infection: light at the end of the tunnelAm J Clin Pathol2011136337238021846912
- HumphriesRMUslanDZRubinZPerformance of Clostridium difficile toxin enzyme immunoassay and nucleic acid amplification tests stratified by patient disease severityJ Clin Microbiol201351386987323269736
- GoldenbergSDCliffPRSmithSMilnerMFrenchGLTwo-step glutamate dehydrogenase antigen real-time polymerase chain reaction assay for detection of toxigenic Clostridium difficileJ Hosp Infect2010741485419900734
- LarsonAMFungAMFangFCEvaluation of tcdB real-time PCR in a three-step diagnostic algorithm for detection of toxigenic Clostridium difficileJ Clin Microbiol201048112413019923482
- SurawiczCMBrandtLJBinionDGGuidelines for diagnosis, treatment, and prevention of Clostridium difficile infectionsAm J Gastroenterol20131084478498 quiz 49923439232
- BerryNSewellBJafriSReal-time polymerase chain reaction correlates well with clinical diagnosis of Clostridium difficile infectionJ Hosp Infect201487210911424795170
- KooHLVanJNZhaoMReal-time polymerase chain reaction detection of asymptomatic Clostridium difficile colonization and rising C. difficile-associated disease ratesInfect Control Hosp Epidemiol201435666767324799643
- QuinnCDSefersSEBabikerWC. diff quik chek complete enzyme immunoassay provides a reliable first-line method for detection of Clostridium difficile in stool specimensJ Clin Microbiol201048260360519955275
- PolageCRChinDLLeslieJLTangJCohenSHSolnickJVOutcomes in patients tested for Clostridium difficile toxinsDiagn Microbiol Infect Dis201274436937323009731
- PatelHRandhawaJNanavatiSMartonLRBaddouraWJDeBariVALaboratory and clinical features of EIA toxin-positive and EIA toxin-negative community-acquired Clostridium difficile infectionAnn Clin Lab Sci201545333333926116599
- BakerILeemingJPReynoldsRIbrahimIDarleyEClinical relevance of a positive molecular test in the diagnosis of Clostridium difficile infectionJ Hosp Infect201384431131523831282
- GuerreroDMChouCJuryLANerandzicMMCadnumJCDonskeyCJClinical and infection control implications of Clostridium difficile infection with negative enzyme immunoassay for toxinClin Infect Dis201153328729021765078
- AkerlundTSvenungssonBLagergrenABurmanLGCorrelation of disease severity with fecal toxin levels in patients with Clostridium difficile-associated diarrhea and distribution of PCR ribotypes and toxin yields in vitro of corresponding isolatesJ Clin Microbiol200644235335816455883
- SorgJASonensheinALBile salts and glycine as cogerminants for Clostridium difficile sporesJ Bacteriol200819072505251218245298
- SorgJASonensheinALInhibiting the initiation of Clostridium difficile spore germination using analogs of chenodeoxycholic acid, a bile acidJ Bacteriol2010192194983499020675492
- TaurYPamerEGHarnessing microbiota to kill a pathogen: fixing the microbiota to treat Clostridium difficile infectionsNat Med201420324624724603796
- GiesemannTGuttenbergGAktoriesKHuman alpha-defensins inhibit Clostridium difficile toxin BGastroenterology200813472049205818435932
- FurciLBaldanRBianchiniVNew role for human alpha-defensin 5 in the fight against hypervirulent Clostridium difficile strainsInfect Immun201583398699525547793
- GoldbergEAmirIZafranMThe correlation between Clostridium-difficile infection and human gut concentrations of Bacteroidetes phylum and clostridial speciesEur J Clin Microbiol Infect Dis201433337738324048726
- KyneLWarnyMQamarAKellyCPAsymptomatic carriage of Clostridium difficile and serum levels of IgG antibody against toxin AN Engl J Med2000342639039710666429
- LooVGPoirierLMillerMAA predominantly clonal multi-institutional outbreak of Clostridium difficile-associated diarrhea with high morbidity and mortalityN Engl J Med2005353232442244916322602
- JohnsonSSamoreMHFarrowKAEpidemics of diarrhea caused by a clindamycin-resistant strain of Clostridium difficile in four hospitalsN Engl J Med1999341221645165110572152
- GerdingDNClindamycin, cephalosporins, fluoroquinolones, and Clostridium difficile-associated diarrhea: this is an antimicrobial resistance problemClin Infect Dis200438564664814986247
- ValerioMPedromingoMMunozPPotential protective role of linezolid against Clostridium difficile infectionInt J Antimicrob Agents201239541441922445203
- BainesSDNoelARHuscroftGSEvaluation of linezolid for the treatment of Clostridium difficile infection caused by epidemic strains using an in vitro human gut modelJ Antimicrob Chemother20116671537154621504940
- SwindellsJBrenwaldNReadingNOppenheimBEvaluation of diagnostic tests for Clostridium difficile infectionJ Clin Microbiol201048260660820032256
- SenohMKatoHFukudaTPredominance of PCR-ribotypes, 018 (smz) and 369 (trf) of Clostridium difficile in Japan: a potential relationship with other global circulating strains?J Med Microbiol201564101226123626238868
- PolageCRGyorkeCEKennedyMAOverdiagnosis of Clostridium difficile infection in the molecular test eraJAMA Intern Med2015175111792180126348734