
Abstract
Introduction
Enterococci commonly inhabit the gastrointestinal tract of both human and animals; however, they have emerged as a leading cause of several infections with substantial morbidity and mortality. Their ability to acquire resistance combined with intrinsic resistance to various antimicrobials makes treatment of enterococcal infections challenging.
Materials and methods
The aim of the study was to evaluate the antimicrobial resistance pattern, and assess the prevalence of multidrug resistance (MDR) and extensive drug resistance (XDR) among enterococcal isolates, collected from different clinical sources, in Mansoura University Hospitals, Egypt.
Results
Antibiotic sensitivity testing revealed elevated levels of resistance among enterococcal clinical isolates (N=103). All E. faecium (N=32) and 74.6% of E. faecalis isolates(N=71) were MDR, while two E. faecalis and four E. faecium isolates were XDR. High level gentamicin resistance was detected in 79.6%, most of them carried the aac(6’)-Ie-aph(2’’)-Ia gene. High level streptomycin resistance was seen in 36.9%, of which 52.6% carried the ant(6’)-Ia gene. Resistance to macrolides and lincosamides were mediated by ermB (92.2%) and msrA/B (42.7%). tetK, tetL, andtetM genes were detected among tetracyclines resistant isolates. Resistance to vancomycin was detected in 15.5%, where vanB and vanC1 gene clusters were detected in VRE isolates. Ten isolates (9.7%) were resistant to linezolid, eight of which harbored the optrA gene. Vancomycin and linezolid resistant enterococci were more likely to exhibit strong/moderate biofilm formation than vancomycin and linezolid sensitive ones.
Conclusion
Elevated levels of resistance to different classes of antimicrobial agents and emergence of MDR and XDR strains pose a major threat with limited therapeutic options for infections caused by this emerging pathogen.
Introduction
Enterococci are Gram-positive, facultative-anaerobic cocci that are persistent in nature and can survive under adverse environmental conditions for prolonged periods of time.Citation1 They are considered commensal organisms and members of the healthy intestinal microbiota of humans and animals.Citation1,Citation2 However, in the last two decades, they have emerged as one of the leading causes of several hospital-acquired and community-acquired infections with substantial morbidity and mortality.Citation3 The most common infections caused by enterococci are urinary tract infections (UTIs), bacteremia, peritonitis, cholecystitis, meningitis, wound infections, endocarditis, and neonatal infections.Citation3 Enterococci are considered the second etiologic agent of UTIs and the third of nosocomial bacteremia.Citation1–Citation3 Although E. faecalis is not considered as a member of the healthy oral microbiota, it has been reported in common dental diseases as dental caries and peridontitis.Citation4–Citation6
E. faecalis and E. faecium are the most commonly reported enterococcal species, counting for up to 90% of enterococcal infections, while other enterococcal species are rarely reported to cause human infections.Citation2,Citation7 Being equipped with an array of virulence determinants and capability to survive in hospital setting makes infections difficult to manage.Citation1,Citation2 Antimicrobial therapy of infections caused by enterococci is problematic because of its intrinsic reduced susceptibility to several frequently used antimicrobial agents including: aminoglycosides (except for high level resistance), clindamycin, cephalosporins, and trimethoprim/sulfamethoxazole.Citation8,Citation9 Moreover, acquired resistance through lateral gene transfer to other available antimicrobial agents, including: beta-lactams, aminoglycosides (high level resistance), macrolides, glycopeptides, and oxazolidinones, makes it more challenging.Citation10 Vancomycin resistant enterococci (VRE) have been reported as a leading cause of outbreaks of hospital-acquired infections and in ICU-hospitalized patients.Citation11,Citation12 Linezolid was the drug of choice for management of infections caused by VRE; however, linezolid resistant enterococci have emerged and are reported.Citation13,Citation14
Clinicians may face very limited treatment options as a result of selection and spread of multidrug-resistant (MDR) and extensively drug resistant (XDR) strains.Citation10,Citation15 Magiorakos et alCitation16 have defined MDR as non-susceptibility to at least one agent in three or more antimicrobial classes, while XDR has been defined as non-susceptibility to at least one agent in all but two or fewer antimicrobial classes. Recently, enterococci have been ascribed in biofilm-associated infections of medical devices.Citation17 The ability of enterococci to form a biofilm amplifies the difficulty of treatment due to increased antimicrobial resistance in the biofilm.Citation18–Citation20 Therefore, antimicrobial susceptibility testing to all available antimicrobial agents is exceptionally elemental for deciding the proper treatment of enterococcal infections.
The aim of this study is to evaluate the antimicrobial resistance pattern and assess the prevalence of MDR and XDR among enterococcal isolates collected from different clinical sources in Mansoura University Hospitals, Egypt. Moreover, the study aims to explore the molecular basis of resistance to different classes of antimicrobial agents.
Materials and methods
Bacterial isolates
Enterococcal isolates (N=103) were recovered from different clinical sources in Mansoura university Hospitals, Egypt between January and August 2017. Identification of enterococcal isolates was based on standard biochemical tests,Citation21,Citation22 then confirmed by a multiplex PCR system.Citation23,Citation24
Antimicrobial susceptibility testing
The antimicrobial susceptibility profile of enterococcal isolates was determined using a disc diffusion method.Citation25 The inhibition zones were interpreted according to the recommendations of the Clinical and Laboratory Standard Institute.Citation26 Susceptibility to different classes of antimicrobial agents was tested, including: ampicillin (10 µg), ampicillin/sulbactam (20 µg/10 µg), Amoxicillin (20 µg), amoxicillin/clavulanic acid (20 µg/10 µg), Imipenem (10 µg), Meropenem (10 µg), vancomycin (30 µg), clindamycin (2 µg), erythromycin (15 µg), clarithromycin (15 µg), azithromycin (15 µg), ciprofloxacin (5 µg), Levofloxacin (5 µg), tertracycline (30 µg), doxycycline (30 µg), and Linezolid (30 µg) (Oxoid, Basingstoke, UK).
The minimum inhibitory concentration (MIC) for vancomycin and linezolid was also determined by standard broth microdilution method, as per Clinical & Laboratory Standards Institute (CLSI) guidelines.Citation26 High-level gentamicin resistance (HLGR, 500 µg/mL) and high-level streptomycin resistance (HLSR, 1000 µg/mL) were determined according to CLSI guidelines.Citation26
Biofilm assay
A quantitative assay of biofilm formation capacity of enterococcal isolates was carried out using a polystyrene microtiter plate assay, as described previously.Citation27,Citation28
Molecular assays
Multiplex PCR analysis of vancomycin-resistant enterococcus species
Total genomic DNA was prepared as described previously.Citation29 Multiplex PCR was used for the detection of vancomycin resistance determinants, including: vanA, vanB,vanC1, and vanC2/3 genes, besides primers for the detection of the ddl genes of E. faecium and E. faecalis and of 16S rRNA as a PCR control (), as described previously.Citation23,Citation24
Table 1 List of primers used in this study
Detection of antimicrobial resistance encoding genes by PCR
The prevalence of resistance determinants to different classes of antimicrobial agents among enterococcal clinical isolates was examined. Genes encoding aminoglycosides,Citation30,Citation31 tetra-cyclines,Citation32–Citation34 macrolide,Citation35 vancomycin,Citation23,Citation24 and linezolidCitation36,Citation37 resistance were detected by PCR. Primer pairs used and expected amplicon sizes are listed in .
Genotyping by random amplified polymorphic DNA (RAPD-PCR) analysis
All enterococcal isolates were genotyped by RAPD-PCR, as described previously.Citation38,Citation39 RAPD patterns were analyzed using gelJ software.Citation40 A similarity matrix was estimated using Dice’s coefficient, and a dendrogram was created based on the unweighted-pair group method with arithmetic averages (UPGMA).Citation41 Enterococcal isolates with a similarity coefficient ≥85% were considered as the same genotype/clonal.
Statistical analysis
Correlation between the capacity of enterococcal clinical isolates for biofilm formation, clinical source of collection, and resistance to different classes of antimicrobial agents were evaluated using Fisher’s exact test or chi-squared test, where a P-value<0.05 was considered statistically significant. Data were analyzed using the SPSS software (version 20.0; SPSS, Chicago, IL, USA).
Results
During the period of study, 103 enterococcal isolates were collected from Mansoura University Hospitals, Egypt from different clinical sources including: urine (56 samples, 54.4%), blood (36 samples, 35%), and wounds (11 samples, 10.7%). All isolates were identified as enterococci phenotypically and genotypically. Seventy-one isolates (68.9%) were identified as E. fecalis, while 32 isolates (31.1%) were identified as E. faecium.
Antimicrobials susceptibility of enterococcal isolates
Among the tested enterococcal isolates, resistance to β-lactam antibiotics was distributed as follows: ampicillin (51.5% R), ampicillin/sulbactam (50.5% R, 1% I), amoxicillin and amoxicillin/clavulanic acid (47.6% R, 3.9% I). There was significant difference in resistance to β-lactam antibiotics between different enterococcal species (P<0.001) (Table S1). All E. faecium isolates (N=32) were resistant β-lactam and β-lactam/β-lactamase inhibitor combinations, while only 29.6% of E. faecalis isolates (N=71) were resistant (). blaZ gene was not detected in any enterococcal isolate. E. faecalis resistance to imipenem was (21.1% R), and meropenem was (26.8% R, 4.2% I).
Table 2 Antibiotic susceptibility testing of enterococcal clinical isolates
Screening of high-level resistance to aminoglycosides has indicated that 82 isolates (79.6%) showed HLGR, while 38 isolates (36.9%) showed HLSR (). Among the isolates that showed HLGR, 75 isolates (91.5%) carried the aac(6’)-Ie-aph(2’’)-Ia gene (Figure S1). Among the isolates that showed HLSR, 20 isolates (52.6%) carried the ant(6’)-Ia gene. No significant difference was observed in prevalence of HLGR between both enterococcal species; however, E. faecium isolates showed a higher rate of HLSR than E. faecalis isolates (P<0.001) (Table S1).
Resistance to macrolides was distributed as follows: erythromycin (91.3% R, 8.7% I), azithromycin (74.6% R, 1.4% I), and clarithromycin (85.9% R, 0% I). All isolates were resistant to clindamycin (). Among the genes encoding macrolide resistance, ermB was detected in 95 isolates (92.2%), while msrA/B was detected in 44 isolates (42.7%) (Figure S1). Both ermB and msrA/B genes were detected in 40 isolates (38.8%). ermA and ermC were not detected in any enterococcal isolate ( and ).
Figure 1 Genotyping of E. faecalis clinical isolates using RAPD-PCR method.
Notes: Dendrogram was created using RAPD-PCR patterns of E. faecalis clinical isolates. Similarity clustering analysis was carried out using UPGMA and Dice coefficient. The dashed line is hypothetical, indicating 85% similarity. Antibiotic susceptibility, resistance determinants, and biofilm formation capacity among E. faecalis clinical isolates were reported. Antibiotic susceptibility: Black cell: Resistant, Gray cell: Intermediate, White cell: Sensitive. Biofilm formation: White cell: Biofilm Non-producer, Light gray cell: Weak Biofilm Producer, Dark gray cell: Moderate Biofilm Producer, Black cell: Strong Biofilm Producer. Resistance determinants: Black cell: Resistance gene detected, White cell: Resistance gene not detected.
Abbreviations: AM, Ampicillin; AMC, Amoxicillin/clavulanic acid; AX, Amoxicillin; AZM, Azithromycin; CIP, ciprofloxacin; CLR, Clarithromycin; DA, Clindamycin; DO, Doxycline; E, Erythromycin; HLGR, High Level Gentamicin Resistance; HLSR, High Level Streptomycin Resistance; IPM, Imipenem; LEV, Levofloxacin; LZD, Linezolid; MEM, Meropenem; ND, Not Determined; RAPD-PCR, random amplified polymorphic DNA-PCR; SAM, Ampicillin/Sulbactam; TE, Tetracycline; UPGMA, unweighted-pair group method with arithmetic averages; VA, Vancomycin.
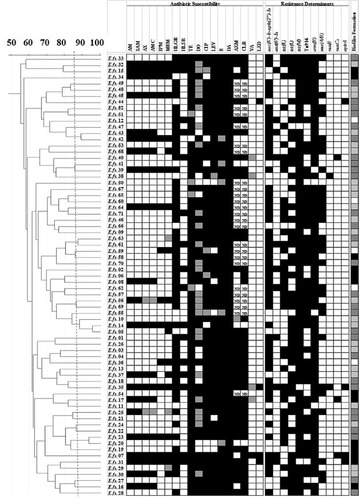
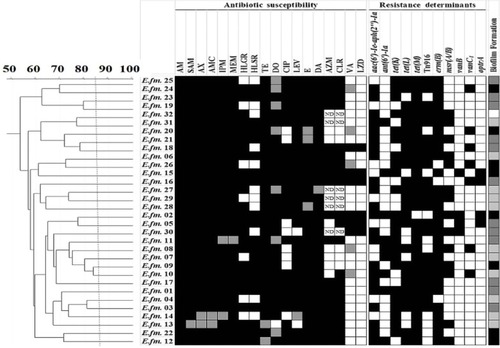
Figure 2 Genotyping of E. faecium clinical isolates using RAPD-PCR method.
Notes: Dendrogram was created using RAPD-PCR patterns of E. faecium clinical isolates. Similarity clustering analysis was carried out using UPGMA and Dice coefficient. The dashed line is hypothetical, indicating 85% similarity. Antibiotic susceptibility, resistance determinants, and biofilm formation capacity among E. faecalis clinical isolates were reported. Antibiotic susceptibility: Black cell: Resistant, Gray cell: Intermediate, White cell: Sensitive. Biofilm formation: White cell: Biofilm Non-producer, Light gray cell: Weak Biofilm Producer, Dark gray cell: Moderate Biofilm Producer, Black cell: Strong Biofilm Producer. Resistance determinants: Black cell: Resistance gene detected, White cell: Resistance gene not detected.
Abbreviations: AM, Ampicillin; AMC, Amoxicillin/clavulanic acid; AX, Amoxicillin; AZM, Azithromycin; CIP, Ciprofloxacin; CLR, Clarithromycin; DA, Clindamycin; DO, Doxycline; E, Erythromycin; HLGR, High Level Gentamicin Resistance; HLSR, High Level Streptomycin Resistance; IPM, Imipenem; LEV, Levofloxacin; LZD, Linezolid; MEM, Meropenem; ND, Not Determined; RAPD-PCR, random amplified polymorphic DNA-PCR; SAM, Ampicillin/Sulbactam; TE, Tetracycline; UPGMA, unweighted-pair group method with arithmetic averages; VA, Vancomycin.
Resistance to tetracycline was (93.2% R, 5.8% I), while resistance to doxycycline was (55.3% R, 31.1% I) (). E. faecium isolates showed a higher rate of resistance to doxycycline than E. faecalis isolates (P=0.016) (Table S1). The tetK gene was detected in 62 isolates (60.2%), the tetL gene in 71 isolates (68.9%), and tetM in 99 isolates (96.1%) (Figure S1). tetK, tetL, and tetM were detected in 37 isolates (35.9%), while two out of the three tested genes were detected in 55 isolates (53.4%) ( and ).
Determination of MIC by broth microdilution method has indicated that seven isolates (6.8%) were resistant to vancomycin (MIC≥32 µg/mL), while nine isolates (8.7%) were intermediately resistant (MIC=8–16 µg/mL) (). A higher rate of vancomycin resistance was observed among E. faecium isolates compared to E. faecalis (P<0.001) (Table S1). Multiplex PCR analysis of vancomycin resistant enterococci has indicated that six isolates carried the vanB gene cluster (MIC=8–>256 µg/mL), while 10 isolates carried vanC1 (MIC=8–32 µg/mL) (Figure S1). VanAandvanC2/3 gene clusters were not detected in any isolate ( and ).
Ten isolates (9.7%) were resistant to linezolid (MIC≥8 µg/mL). Among linezolid resistant strains, eight isolates carried the optrA gene (Figure S1), while the cfr gene was not detected in any isolate. Prevalence of quinolone resistance among enterococcal isolates was (81.6% R, 3.9% I) for ciprofloxacin and (89.3% R, 2% I) for levofloxacin ().
Biofilm formation among enterococcal isolates
The capacity of enterococci isolated from different clinical sources to form a biofilm was evaluated by polystyrene microtiter plate assay, as previously described, and divided into strong, moderate, weak biofilm producers, and non-biofilm producers.Citation27,Citation28 The ability to form a biofilm was detected in almost all clinical isolates examined (97 isolates, 94.2%). Only six isolates (5.8%) were biofilm non-producers (Table S2). Among the biofilm forming isolates, 21 isolates (20.4%) were strong biofilm producers, 41 isolates (39.8%) were moderate biofilm producers, while 35 isolates (34%) were classified as weak biofilm producers. No significant difference in biofilm formation capacity was observed between E. faecalis and E. faecium isolates (P>0.05) (Table S2). Bio-film formation capacity was similar between different clinical sources from which the isolates were collected (P>0.05).
Correlation between biofilm formation capacity and resistance to different classes of antimicrobials has indicated that vancomycin-resistant isolates were more likely to exhibit a strong or moderate biofilm formation capacity than vancomycin-sensitive isolates (P=0.034) (Table S3). Moreover, all linezolid-resistant strains exhibited strong or moderate biofilm formation capacity (P=0.032). Resistance to β-lactam antibiotics and β-lactam/β-lactamase combinations significantly correlated with biofilm formation capacity among enterococcal clinical isolates (P=0.039) (Table S3). However, there was no significant correlation between biofilm formation ability and resistance/sensitivity to other classes of antimicrobial agents.
Clonal relationship analysis by RAPD-PCR
Enterococcal isolates recovered from different clinical sources were genotyped by the RAPD-PCR approach. Great diversity was observed in RAPD-PCR profiles of both E. faecalis () and E. faecium () isolates recovered from different clinical sources at an 85% cutoff. Some E. faecalis isolates showed a similarity coefficient higher than 85% and were considered clonal (for example: E.fs.43 and E.fs.42), however, their antibiotic susceptibility profiles and resistance determinants detected were different (). No clustering of the enterococcal isolates was observed based on the clinical source from which they were recovered or their biofilm formation capacity.
Discussion
Enterococci colonize the gastrointestinal tract of both humans and animals and are considered a part of its normal beneficial flora;Citation1 however, it has emerged as a nosocomial pathogen in the last few decades.Citation2 E. faecalis is the most commonly reported species accounting for more than 80% of enterococcal infections; however, E. faecium has also been increasingly reported which could be attributed to its resistance to multiple classes of antibiotics.Citation1,Citation2 In our study, E. faecalis was the most prevalent species detected, accounting for 68.9%, while 31.1% were identified as E. faecium. Most of the enterococcal isolates (54.4%) were collected from urine, followed by blood (35%), and wound (10.7%). Previous reports have also indicated that UTI is the most common infection caused by enterococci, followed by surgical site infections (SSI), bacteremia, and endocarditis.Citation42–Citation44
Recent reports have indicated that HLGR among enterococcal isolates ranged from 50% to 65%, while HLSR was less common than HLGR, ranging from 29% to 38%.Citation43,Citation45,Citation46 Similarly, we had observed HLGR to be more predominant than HLSR. However, our study has indicated a higher rate of HLGR (79.6%) among enterococcal isolates in Egypt. Although enterococci have intrinsic resistance to low levels of aminoglycosides, high-level resistance is mediated by acquisition of aminoglycoside-modifying enzymes (AMEs) encoding genes. HLGR (MIC≥500 mg/mL) in enterococci is mostly mediated by the aac(6’)-Ie-aph(2’’)-Ia gene that encodes the bifunctional aminoglycoside modifying enzyme AAC(6’)-APH(2’’) and confers high-level resistance to aminoglycosides except streptomycin, while HLSR in enterococci are mediated by ant(6’)-Ia gene. In enterococci, AMEs eliminate the synergistic activity of aminoglycosides when combined with a cell wall active agent, such as ampicillin or vancomycin.Citation43,Citation45,Citation46
Increased resistance to macrolides, lincosamides, and streptogramin B (MLSB resistance) among enterococcal clinical isolates may be attributed to the wide use of this class of antimicrobials for treatment of enterococcal infections, except UTIs.Citation47 MLSB resistance is attributed to active efflux, target modification, or inactivating enzymes.Citation48 Methylation of 23S rRNA, mediated by erm gene, mediates resistance to macrolides, lincosamides, and streptogramin B. ermB is the most commonly reported gene among enterococcal isolates, while ermA and ermC are occasionally reported.Citation49 msrA/B gene encodes efflux pump for macrolides and streptogramin B.Citation47 Similar to previous reports, ermB and msrA/B genes were present in most macrolide resistant enterococcal isolates tested.Citation45,Citation47,Citation49
Tetracyclines are broad-spectrum antibiotics and one of the most frequently used antimicrobials in Europe and in veterinary medicine.Citation47 Tetracycline resistance determinants (tet genes) mediate ribosomal protection, enzymatic inactivation, and efflux of tetracyclines. tetK and tetL are involved in the efflux mechanism, while tetM plays a role in ribosomal protection among enterococci.Citation50 Our data have indicated that most enterococcal clinical isolates (89.3%) carried more than one tet gene conferring different mechanisms of resistance to tetracyclines (efflux and ribosomal protection). There is not enough data or reports describing the prevalence of tetracycline resistance and its determinants among enterococcal clinical isolates. Recently, Zahid et alCitation51 indicated that 57% of enterococcal isolates carried tetL, 50% carried tetM, while 33% carried both tetL and tetM.
Association of antibiotic resistance genes with mobile genetic elements increases the risk of dissemination of antibiotics resistance among enterococcal isolates. Tn916 was the first conjugative transposon, carrying the tetM gene, identified in E. faecalis.Citation52 Since then, a large number of trans-posable elements have been identified carrying resistance to different classes of antibiotics.Citation47 In the present study, the integrase (int) and the excisase (xis) genes of Tn916 were detected in 72 isolates (69.9%) of enetrococcal isolates collected from different clinical sources. A recent study has indicated that Tn916 was detected in 43.3% of enterococcal clinical isolates.Citation51
Enterococcal resistance to glycopeptides is mediated by van operons.Citation53 Most vancomycin resistant enterococcal outbreaks are attributed to vanA and vanB gene clusters.Citation43,Citation54 vanA is inducible and confers high-level resistance to both vancomycin and teicoplanin, while vanB confers a variable level of resistance to vancomycin, but not to teicoplanin.Citation53 vanC is less virulent than vanA and vanB and intrinsically present in some enterococcal species. However, the vanC1gene cluster has been recently detected in E. faecalis and E. faecium clinical isolates providing moderate level resistance to vancomycin.Citation55,Citation56 Variable rates of vancomycin resistance were detected across the world, with lower rates detected in Europe and Canada (4%–6%).Citation54,Citation57,Citation58 A recent study in Iran has indicated that 18.8% of their enterococcal clinical isolates were resistant to vancomycin, where all isolates had MIC>256% and 90% of VRE carried the vanA gene cluster.Citation43 Our data showed high prevalence of VRE in Egypt (15.5%); however, VRE carried either vanB or vanC1 gene clusters. Moreover, our results coincide with previous reports that showed a higher rate of vancomycin resistance in E. faecium than E. faecalis clinical isolates.Citation54
Linezolid, the first oxazolidinone used clinically, is one of the most promising agents against MDR G+ve pathogens, especially VRE. However, linezolid resistance has been increasingly reported among enterococcal clinical isolates.Citation59,Citation60 Klare et alCitation59 found that the rate of linezolid resistance increased in Germany from <1% in 2008 to >9% in 2014. Our results coincide with their results, where 9.7% of our isolates were linezolid resistant. Mutation in domain V of the 23S rRNA gene, and transferable plasmid mediated methytransferase (cfr) and optrA genes have been reported to mediate resistance to oxazolidinones.Citation36,Citation37 Beside oxazolidinones, the optrA gene also confers resistance to phenolics. It was first described in 2015 in enterococci recovered from human and animal origins in China.Citation37 Afterwards, the optrA gene has been detected in linezolid resistant enterococcal isolates in several places worldwide.Citation61–Citation63 In our study, the optrA gene was detected in 80% of the linezolid resistant enterococci. To our knowledge, this is the first report of the optrA gene among linezolid resistant enterococci in Egypt. The cfr gene has been previously detected among linezolid resistant enterococci;Citation36,Citation59,Citation60 however, it was not detected among linezolid resistant enterococci tested.
Enterococci have a high biofilm formation capacity, which increases the difficulty of management of enterococcal infections and hinders the penetration of antibiotics.Citation64,Citation65 In the present study, most of the enterococcal clinical isolates were biofilm producers, where 60.2% were strong/moderate biofilm producers. Several previous studies have indicated a high biofilm formation capacity among enterococcal clinical isolates.Citation64,Citation65 All linezolid-resistant strains exhibited strong/moderate biofilm formation. Moreover, vancomycin-resistant isolates were more likely to exhibit strong/moderate biofilm formation than vancomycin-sensitive isolates. A previous study has also indicated the correlation between biofilm formation capacity among enterococcal clinical isolates and resistance to linezolid.Citation65 Another study has indicated that resistance to penicillin G, ampicillin, vancomycin, ciprofloxacin, chloramphenicol, and nitrofurantoin was significantly higher among biofilm producers than biofilm non-producers.Citation66
In this study, a higher level of resistance was observed among E. faecium than E. faecalis isolates () as previously reported.Citation2,Citation43,Citation45,Citation59 Magiorakos et alCitation16 have defined MDR as non-susceptibility to at least one agent in three or more antimicrobial classes, while XDR was defined as non-susceptibility to at least one agent in all but two or fewer antimicrobial classes. According to this definition, 53 E. faecalis isolates (74.6%) were MDR, while all E. faecium (N=32) were MDR strains. Two E. faecalis isolates (2.8%) and four E. faecium (12.5%) were resistant to all tested antimicrobi-als tested and considered as XDR (Table S4). Horizontal gene transfer is held responsible for the elevated levels of resistance to different antimicrobials, since plasmids and transposable elements usually carry resistance determinants for more than one class of antimicrobial agents. The increased level of resistance to vancomycin and linezolid highlights the problem of limited options to treatment infections caused by MDR and XDR enterococcal strains.
Conclusion
Antimicrobial susceptibility testing is of utmost importance in formulating an effective antibiotic policy for treatment of enterococcal infections and reducing morbidity and mortality. Neglecting standard protocols, empirical use of antibiotics, and lack of sufficient information are the leading causes for the emergence and spread of MDR and XDR enterococci in hospitals. Hence, effective measures, standard protocols, and programs to control the spread of enterococci should be implemented.
Supplementary materials
Figure S1 Agarose gel electrophoresis for detection of antimicrobials resistance determinants among enterococcal isolates. (A). Detection of antimicrobials resistance encoding genes among enterococcal isolates by PCR. Lane M is Molecular weight marker. 1:aac(6’)-Ie-aph(2’’)-Ia (200 bp); 2: ant(6’)-Ia (597 bp); 3: tetK (370 bp); 4: tetL (715 bp); 5: tetM (170 bp); 6: ermB (639 bp) and 7: msrA/B (400 bp); 8: optrA (1395 bp); 9: int-Tn (1046 bp); and 10: xis-Tn (194 bp) genes that are used for detection antimicrobials resistance among enterococcal isolates. (B). Multiplex PCR for detection of vancomycin resistance determinants (vanA(1030 bp),vanB(536 bp),vanC1 (822 bp), and vanC2/3 (484 bp)), E. faecium-specific (658 bp), E. faecalis-specific (941 bp) and of rrs (320 bp) genes. Lane M is Molecular weight marker. 1:E. faecalis isolate; 2:E. faecium isolate; 3:E. faecium vanB isolate; 4: E. faecalis vanC1 isolate; 5: E. faecium vanC1isolate; 6:E. faecalis vanBisolate.
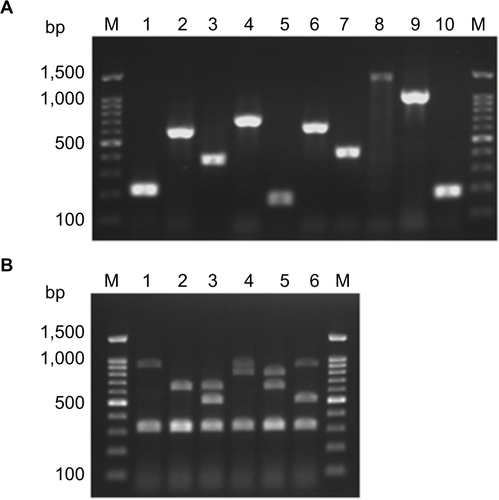
Table S1 Prevalence of antibiotic susceptibility among enterococcal species isolated from different clinical sources
Table S2 Prevalence of biofilm formation among enterococcal isolates collected from different clinical sources
Table S3 Correlation between biofilm formation capacity and antibiotic susceptibility among enterococcal clinical isolates
Table S4 Distribution of multidrug resistance (MDR) and extensive drug resistance (XDR) among enterococcal clinical isolates
Disclosure
The authors report no conflicts of interest in this work.
References
- FisherKPhillipsCThe ecology, epidemiology and virulence of EnterococcusMicrobiology2009155Pt 61749175719383684
- Van TyneDGilmoreMSFriend turned foe: evolution of enterococcal virulence and antibiotic resistanceAnnu Rev Microbiol20146833735625002090
- SimmonsBPLarsonELMultiple drug resistant organisms in healthcare: the failure of contact precautionsJ Infect Prev201516417818128989425
- DahlénGBlomqvistSAlmståhlACarlénAVirulence factors and antibiotic susceptibility in enterococci isolated from oral mucosal and deep infectionsJ Oral Microbiol20124110855
- RamsTEDegenerJEvan WinkelhoffAJPrevalence of β-lactamase-producing bacteria in human periodontitisJ Periodontal Res201348449349923173872
- RamsTEFeikDYoungVHammondBFSlotsJEnterococci in human periodontitisOral Microbiol Immunol1992742492521408361
- HammerumAMEnterococci of animal origin and their significance for public healthClin Microbiol Infect201218761962522487203
- HuyckeMMSahmDFGilmoreMSMultiple-drug resistant enterococci: the nature of the problem and an agenda for the futureEmerg Infect Dis1998422392499621194
- KayeKSKayeDMultidrug-resistant pathogens: mechanisms of resistance and epidemiologyCurr Infect Dis Rep20002539139811095883
- AriasCAMurrayBEThe rise of the Enterococcus: beyond vancomycin resistanceNat Rev Microbiol201210426627822421879
- FlokasMEKarageorgosSADetsisMAlevizakosMMylonakisEVancomycin-resistant enterococci colonisation, risk factors and risk for infection among hospitalised paediatric patients: a systematic review and meta-analysisInt J Antimicrob Agents201749556557228336313
- MoosavianMGhadriHSamliZMolecular detection of vanA and vanB genes among vancomycin-resistant enterococci in ICU-hospitalized patients in Ahvaz in southwest of IranInfect Drug Resist2018112269227530532561
- ChenMPanHLouYEpidemiological characteristics and genetic structure of linezolid-resistant Enterococcus faecalisInfect Drug Resist2018112397240930538507
- GawryszewskaIŻabickaDHryniewiczWSadowyELinezolid-resistant enterococci in Polish hospitals: species, clonality and determinants of linezolid resistanceEur J Clin Microbiol Infect Dis20173671279128628197728
- van HartenRMWillemsRJLMartinNIHendrickxAPAMultidrug-resistant enterococcal infections: new compounds, novel antimicrobial therapies?Trends Microbiol201725646747928209400
- MagiorakosAPSrinivasanACareyRBMultidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistanceClin Microbiol Infect201218326828121793988
- PaganelliFLWillemsRJLeavisHLOptimizing future treatment of enterococcal infections: attacking the biofilm?Trends Microbiol2012201404922169461
- ParkerRELautCGaddyJAZadoksRNDaviesHDManningSDAssociation between genotypic diversity and biofilm production in group B StreptococcusBMC Microbiol20161618627206613
- SandoeJAWitherdenIRCoveJHHeritageJWilcoxMHCorrelation between enterococcal biofilm formation in vitro and medical-device-related infection potential in vivoJ Med Microbiol200352Pt 754755012808074
- SenoYKariyamaRMitsuhataRMondenKKumonHClinical implications of biofilm formation by Enterococcus faecalis in the urinary tractActa Med Okayama2005593798716049560
- FacklamRRMaria da GloriaSCTeixeiraLMHistory, Taxonomy, Biochemical Characteristics, and Antibiotic Susceptibility Testing of EnterococciWashington, DCASM Press2002
- MahonCRLehmanDCManuselisGSelected proceduresTextbook of Diagnostic Microbiology4th edMahonCRLehmanDManuselisGOxfordElsevier Health Sciences201110181024
- ElsayedSHamiltonNBoydDMulveyMImproved primer design for multiplex PCR analysis of vancomycin-resistant Enterococcus sppJ Clin Microbiol20013962367236811414244
- KariyamaRMitsuhataRChowJWClewellDBKumonHSimple and reliable multiplex PCR assay for surveillance isolates of vancomycin-resistant enterococciJ Clin Microbiol20003883092309510921985
- BauerAWKirbyWMSherrisJCTurckMAntibiotic susceptibility testing by a standardized single disk methodAm J Clin Pathol19664544934965325707
- CLSIPerformance Standards for Antimicrobial Susceptibility Testing27th edCLSI document M100-S271-56238-805-32017
- MohamedJAHuangWNallapareddySRTengFMurrayBEInfluence of origin of isolates, especially endocarditis isolates, and various genes on biofilm formation by Enterococcus faecalisInfect Immun20047263658366315155680
- Toledo-AranaAValleJSolanoCThe enterococcal surface protein, esp, is involved in Enterococcus faecalis biofilm formationAppl Environ Microbiol200167104538454511571153
- EnglenMDKelleyLCA rapid DNA isolation procedure for the identification of Campylobacter jejuni by the polymerase chain reactionLett Appl Microbiol200031642142611123549
- ClarkNCOlsvikOSwensonJMSpiegelCATenoverFCDetection of a streptomycin/spectinomycin adenylyltransferase gene (aadA) in Enterococcus faecalisAntimicrob Agents Chemother19994311571609869582
- Van de KlundertJPCR detection of genes coding for aminoglycoside-modifying enzymesDiagn Mol Microbiol1993547552
- AminovRIGarrigues-JeanjeanNMackieRIMolecular ecology of tetracycline resistance: development and validation of primers for detection of tetracycline resistance genes encoding ribosomal protection proteinsAppl Environ Microbiol2001671223211133424
- CochettiITiliEVecchiMNew Tn916-related elements causing erm(B)-mediated erythromycin resistance in tetracycline-susceptible pneumococciJ Antimicrob Chemother200760112713117483548
- GeversDDanielsenMHuysGSwingsJMolecular characterization of tet (M) genes in Lactobacillus isolates from different types of fermented dry sausageAppl Environ Microbiol20036921270127512571056
- SutcliffeJGrebeTTait-KamradtAWondrackLDetection of erythromycin-resistant determinants by PCRAntimicrob Agents Chemother19964011256225668913465
- DiazLKiratisinPMendesREPanessoDSinghKVAriasCATransferable plasmid-mediated resistance to linezolid due to cfr in a human clinical isolate of Enterococcus faecalisAntimicrob Agents Chemother20125673917392222491691
- WangYLvYCaiJA novel gene, optrA, that confers transferable resistance to oxazolidinones and phenicols and its presence in Enterococcus faecalis and Enterococcus faecium of human and animal originJ Antimicrob Chemother20157082182219025977397
- Martín-PlateroAMValdiviaEMaquedaMMartínez-BuenoMCharacterization and safety evaluation of enterococci isolated from Spanish goats’ milk cheesesInt J Food Microbiol20091321243219375810
- Muñoz-AtienzaEAraújoCRdelCampoHernándezPEHerranzCCintasLMSafety assessment and molecular genetic profiling by pulsed-field gel electrophoresis (PFGE) and PCR-based techniques of Enterococcus faecium strains of food originLWT Food Sci Technol201665357362
- HerasJDomínguezCMataEGelJ-a tool for analyzing DNA fingerprint gel imagesBMC Bioinformatics201516127026307353
- SaitouNNeiMThe neighbor-joining method: a new method for reconstructing phylogenetic treesMol Biol Evol1987444064253447015
- ArshadiMDouraghiMShokoohizadehLMoosavianSMPourmandMRHigh prevalence of diverse vancomycin resistance Enterococcus faecium isolates in clinical and environmental sources in ICU wards in Southwest of IranMicrob Pathog201711121221728882784
- JahansepasAAghazadehMRezaeeMAOccurrence of Enterococcus faecalis and Enterococcus faecium in Various Clinical Infections: Detection of Their Drug Resistance and Virulence DeterminantsMicrob Drug Resist2018241768228525287
- SomilyAMAl-MohizeaMMAbsarMMMolecular epidemiology of vancomycin resistant enterococci in a tertiary care hospital in Saudi ArabiaMicrob Pathog201697798327247096
- HeidariHEmaneiniMDabiriHJabalameliFVirulence factors, antimicrobial resistance pattern and molecular analysis of enterococcal strains isolated from burn patientsMicrob Pathog201690939726620079
- SheteVGroverNKumarMAnalysis of aminoglycoside modifying enzyme genes responsible for high-level aminoglycoside resistance among enterococcal isolatesJ Pathog20172017325695229435370
- MarosevicDKaevskaMJaglicZResistance to the tetracyclines and macrolide-lincosamide-streptogramin group of antibiotics and its genetic linkage- a reviewAnn Agric Environ Med201724233834428664720
- RobertsMCSutcliffeJCourvalinPJensenLBRoodJSeppalaHNomenclature for macrolide and macrolide-lincosamide-strep-togramin B resistance determinantsAntimicrob Agents Chemother199943122823283010582867
- IwerieborBCObiLCOkohAIMacrolide, glycopeptide resistance and virulence genes in Enterococcus species isolates from dairy cattleJ Med Microbiol201665764164827166215
- RobertsMCTetracycline resistance determinants: mechanisms of action, regulation of expression, genetic mobility, and distributionFEMS Microbiol Rev19961911248916553
- ZahidSBin-AsifHHasanKARehmanMAliSAPrevalence and genetic profiling of tetracycline resistance (Tet-R) genes and transposable element (Tn916) in environmental Enterococcus speciesMicrob Pathog201711125226128888881
- FrankeAEClewellDBEvidence for a chromosome-borne resistance transposon (Tn916) in Streptococcus faecalis that is capable of “conjugal” transfer in the absence of a conjugative plasmidJ Bacteriol198114514945026257641
- AhmedMOBaptisteKEVancomycin-resistant enterococci: a review of antimicrobial resistance mechanisms and perspectives of human and animal healthMicrob Drug Resist201824559060629058560
- O’DriscollTCrankCWVancomycin-resistant enterococcal infections: epidemiology, clinical manifestations, and optimal managementInfect Drug Resist2015821723026244026
- de GarnicaMLValdezateSGonzaloCSaez-NietoJAPresence of the vanC1 gene in a vancomycin-resistant Enterococcus faecalis strain isolated from ewe bulk tank milkJ Med Microbiol201362Pt 349449523161771
- SunMWangYChenZZhuXTianLSunZThe first report of the vanC1 gene in Enterococcus faecium isolated from a human clinical specimenMem Inst Oswaldo Cruz20141096712715
- SievertDRicksPEdwardsJNational Healthcare Safety Network (NHSN) Team and Participating NHSN FacilitiesAntimicrobial-resistant pathogens associated with healthcare-associated infections: summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2009–2010Infect Control Hosp Epidemiol201334111423221186
- ZhanelGGAdamHJBaxterMRCanadian Antimicrobial Resistance Alliance Antimicrobial susceptibility of 22746 pathogens from Canadian hospitals: results of the CANWARD 2007-11 studyJ Antimicrob Chemother201368Suppl 1i7i2223587781
- KlareIFleigeCGeringerUIncreased frequency of linezolid resistance among clinical Enterococcus faecium isolates from German hospital patientsJ Glob Antimicrob Resist20153212813127873661
- LiBMaCLYuXInvestigation of mechanisms and molecular epidemiology of linezolid nonsusceptible Enterococcus faecalis isolated from a teaching hospital in ChinaJ Microbiol Immunol Infect201649459559926210761
- CaiJWangYSchwarzSHigh detection rate of the oxazolidinone resistance gene optrA in Enterococcus faecalis isolated from a Chinese anorectal surgery wardInt J Antimicrob Agents201648675775927751624
- CavacoLMBernalJFZankariEDetection of linezolid resistance due to the optrA gene in Enterococcus faecalis from poultry meat from the American continent (Colombia)J Antimicrob Chemother2016723678683
- VorobievaVRoerLJustesenUSDetection of the optrA gene in a clinical ST16 Enterococcus faecalis isolate in DenmarkJ Glob Antimicrob Resist201710121328572038
- AndersonACJonasDHuberIEnterococcus faecalis from food, clinical specimens, and oral sites: prevalence of virulence factors in association with biofilm formationFront Microbiol20156153426793174
- ZhengJXBaiBLinZWCharacterization of biofilm formation by Enterococcus faecalis isolates derived from urinary tract infections in ChinaJ Med Microbiol Epub20171117
- FallahFYousefiMPourmandMRHashemiANazari AlamAAfsharDPhenotypic and genotypic study of biofilm formation in enterococci isolated from urinary tract infectionsMicrob Pathog2017108859028483600