Abstract
Chronic rhinosinusitis (CRS) is a common disorder characterized by mucosal inflammation of the nose and paranasal sinuses with sinonasal symptoms persisting for greater than 12 weeks. The etiology of CRS is incompletely understood. Current understanding supports inflammation, rather than infection, as the dominant etiologic factor. CRS significantly impacts patients’ quality of life and health care expenditure. There is no standard management of CRS. Treatment strategies differ based on divergent etiologies of the various CRS subclasses. Both systemic and topical agents are used. These interventions differ in CRS with nasal polyposis (CRSwNP), CRS without nasal polyposis (CRSsNP) and specific situations such as allergic fungal rhinosinusitis or aspirin-exacerbated respiratory disease. Antibiotics are the most commonly prescribed medication for CRS, but their role in management is not strongly supported by high-level studies. This paper provides a succinct review of the evidence supporting or refuting common therapeutic agents in the management of CRS. Novel and emerging strategies will also be discussed.
Keywords:
Introduction
Chronic rhinosinusitis (CRS) is diagnosed when specific sinonasal symptoms lasting 12 or more weeks are confirmed by nasal endoscopy or radiographic imaging ().Citation1 CRS is best considered as a group of heterogeneous disorders from a multitude of causes that result in mild to severe symptomatic inflammation of the sinonasal mucosa ().Citation2 The management of this complex and diverse disease is therefore a challenge. Much ongoing research is being directed toward the investigation of treatment strategies, as well as developing criteria for diagnosing the various CRS subsets. The most simplified classification divides CRS into those patients who have nasal polyps (CRSwNP) and those without (CRSsNP) ().Citation3
Figure 1 Diagnosis of CRS.
Note: © 2007 Sage Publications. Reproduced with permission from Rosenfeld RM, et al. Clinical practice guideline: adult sinusitis. Otolaryngol Head Neck Surg. 2007;137(3 Suppl)S1–S31.
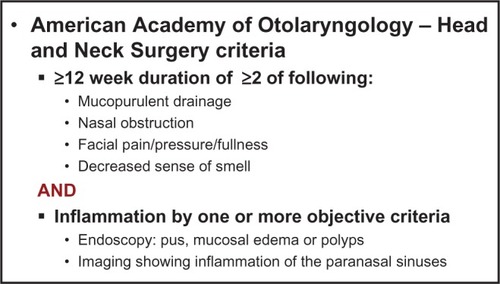
Figure 2 Factors associated with CRS.
Note: © 2003 Sage Publications. Adapted with permission from Benninger M, et al. Otolaryngol Head Neck Surg. 2003;129(3 suppl):S1–S32.
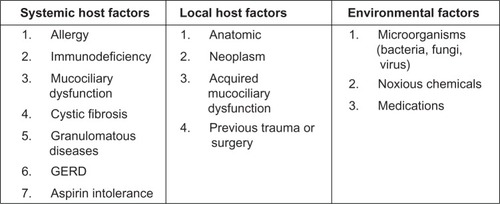
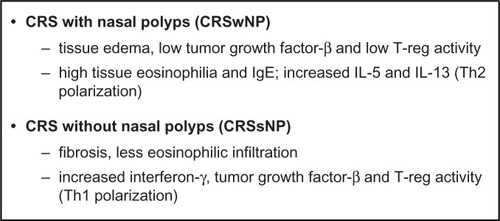
Figure 3 CRS differentiation by inflammatory mediators.
Note: Data from Van Zele T, et al. Differentiation of chronic sinus diseases by measurement of inflammatory mediators. Allergy. 2006;61:1280–1289.
Medical therapy of CRS is a key strategy, with surgery playing a vital adjunctive role. Medical therapy is directed toward treatment of the underlying etiology, as well as the resultant inflammation. A variety of systemic and topical therapeutic agents are commonly employed. These include corticosteroids, antimicrobials, and immune modulating medications. As CRS is a chronic disease, there are concerns related to the use of systemic agents over prolonged periods. Long-term use of corticosteroids and antibiotics may lead to adverse effects, drug interactions, and antimicrobial resistance. The development of topical therapy delivered directly to the sinonasal cavity has created an alternative treatment strategy to help potentiate these concerns. Many therapeutic agents can now be delivered into the sinonasal cavity by a variety of delivery methods, such as irrigations, sprays, and aerosols.
This paper will provide a succinct summary of current and emerging evidence-based strategies to treat CRS.
Epidemiology
CRS is estimated to result in over 18 million physician visits in the United States each yearCitation4 and is self-diagnosed in one in seven adults.Citation5 It is also the fifth most common diagnosis for an antibiotic prescription.Citation6 Despite its prevalence, there is a surprising paucity of accurate epidemiologic data for CRS, especially CRSsNP. Patient surveys in the United States have found a 15%–16% prevalence of CRS;Citation7,Citation8 however, a prevalence of only 2% was found using ICD-9 (International Classification of Diseases, Ninth Revision) codes as an identifier.Citation9 In studies from Canada, Korea, Scotland, Europe, and Sao Paulo, prevalence of CRS ranges from 1%–11%.Citation10–Citation14
Population-based studies of CRSwNP from Sweden, Korea, Finland, and France report the prevalence of CRSwNP to lie between 0.5% and 4.3%.Citation15–Citation18 Autopsy studies reveal a higher prevalence between 2% and 42%, with more polyps found in dissected naso-ethmoidal blocks and endoscopic sinus surgery (ESS) than with anterior rhinoscopy alone.Citation19,Citation20 Men and women are both affected by CRSwNP, with some discordance in the literature as to which sex is more frequently affected. In general, nasal polyps occur in all races and become more common with age, with the average age of onset being 42 years.Citation18
Etiology
Regarding the etiology of CRS, numerous hypotheses have been proposed with a great deal of overlap, supporting a multifactorial basis. One classification method separates potential contributing entities into host and environmental factors ().Citation2 Although comprehensive, this scheme fails to illustrate causal relationships and host–environment interactions. The heterogeneous nature of CRS is important to understand when planning treatment for this diverse group of patients whose disease may have arisen from very different underlying etiologies.
In a broad generalization, CRSwNP in the Caucasian population is associated more closely with high tissue eosinophilia and increased T helper (Th)-2 cytokine expression (interleukin [IL]-5 and IL-13) as well as nasal obstruction and smell loss. Meanwhile, CRSsNP may have more Th-1 polarization and less eosinophilic infiltration ().Citation3 However, these characterizations may not hold true for other ethnic populations. Dysfunction in the eicosanoid pathway, with increased synthesis of pro-inflammatory leukotrienes and decreased synthesis of anti-inflammatory prostaglandins, has been proposed as a mechanism for both aspirin-sensitive and aspirin-tolerant CRSwNP.Citation21 Defects in the coordinated mechanical barrier and/or the innate immune response of the sinonasal epithelium has also been proposed as a mechanism for CRS. This susceptibility may be based on host genetic factors, predisposing some individuals to mechanical barrier failure in the presence of environmental stress.Citation22 CRS is a common problem in patients with Kartagener’s syndrome, primary ciliary dyskinesia, and cystic fibrosis. Inability of the sinonasal cilia to transport viscous mucus causes ciliary malfunction leading to CRS.
Epithelial damage and/or host barrier dysfunction may result in colonization of the sinonasal mucosa with Staphylococcus aureus. Subsequent secretion of superantigenic toxins may lead to a skewed Th-2 host inflammatory response with generation of local polyclonal immunoglobulin E (IgE), promotion of eosinophil survival and mast cell degranulation with alteration of eicosanoid metabolism.Citation23 The sum of these local tissue effects may lead to polyp formation. New evidence also implicates the generation of local autoantibodies in perpetuating tissue damage in the most severe forms of CRSwNP.Citation24
The role of microbes as causative agents in CRS is not clear, but microbial infection and biofilms may contribute to the propagation of CRS. S. aureus is the most common bacterial pathogen identified in CRS patients in Western countries.Citation25 Coagulase-negative Staphylococcus and anaerobic and Gram-negative bacteria are also commonly cultured from CRS patients.Citation26 A recent prospective study of samples obtained from the middle meatus using the 16S ribosomal technique revealed a polymicrobial flora in CRS that was distinct from controls, with a preponderance of anaerobes in CRS.Citation27 In post-surgical patients, Pseudomonas, Klebsiella, Enterobacter, and Staphylococcus species predominate.Citation26 Bacterial biofilms, which are largely absent in controls, have been recovered from both CRSsNP and CRSwNP patients, with reported rates varying between 30% and 100%.Citation28–Citation30 While it is not known whether biofilms have a role in the establishment of CRS, it is widely accepted that biofilms facilitate resistance to host defenses and antibiotics, helping to foster recalcitrant disease. Although antibiotics are the most common form of therapy prescribed by physicians for the treatment of CRS,Citation31 the precise role of bacteria in CRS pathogenesis remains unclear.
The role of fungi in CRS has been the source of much debate in the last decade. The use of sensitive detection techniques has shown fungi are a ubiquitous intranasal presence in close to 100% of CRS patients and controls.Citation32 Despite this observation, there is a lack of definitive evidence demonstrating that fungal antigens are the primary targets of the mucosal T or B cell responses observed in CRS (with the exception of allergic fungal rhinosinusitis).Citation2,Citation33
Diagnosis
CRS is diagnosed based on clinical symptoms and objective evaluation. Symptoms must be present for at least 12 consecutive weeks. Nasal obstruction, facial pressure/ congestion/fullness, discolored nasal discharge, and hyposmia are the signs and symptoms used to diagnose CRS ().Citation1 Several studies have shown using symptoms alone to diagnose CRS can be nonspecific.Citation34–Citation36 Therefore, nasal endoscopy or imaging must also be used to confirm the presence of sinonasal disease to increase the specificity of diagnosis.Citation1 Endoscopic findings suggestive of CRS include mucopurulent discharge, nasal polyps or polypoid change, and/or mucosal edema obstructing the middle meatus. A recent study found the addition of endoscopic findings to symptom-based criteria significantly improved diagnostic accuracy of CRS.Citation37
Computed tomography (CT) is considered the gold standard for imaging in CRS.Citation38,Citation39 Findings consistent with CRS include isolated or diffuse mucosal thickening, bone changes, or air-fluid levels.Citation1 Magnetic resonance imaging (MRI) does not pose a radiation risk and has improved soft tissue definition over CT scan, but is more expensive. Recent evidence shows a close correlation between CT and MRI in the staging accuracy of sinonasal disease.Citation40
Patients with CRS may frequently present with associated diagnoses of asthma, allergy, dental disease, nasal polyposis, ciliary dyskinesia, cystic fibrosis, and immunodeficiency syndromes. Thus, CRS represents a spectrum of diseases with a range of appropriate treatments. Once the diagnosis of CRS has been established, workup and treatment of patients must be individualized.
Standard treatment
Although the American Academy of Otolaryngology – Head and Neck Surgery guidelines state CRS should be treated with “maximal medical therapy,”Citation1 there is no such standardized therapy for CRS. This is in part due to the heterogeneity of the disease, which includes CRSwNP, CRSsNP, allergic fungal rhinosinusitis (AFS), and CRS associated with other systemic diseases such as atopy, asthma, cystic fibrosis, and aspirin-exacerbated respiratory disease (AERD). Symptoms may be mild with little effect on quality of life, or may result in significant health problems and loss of productivity. As such, maximal medical therapy is best considered as a philosophical approach, in which CRS in a given individual is treated with a combination of medical strategies best suited for that patient. These treatment strategies include topical and systemic medications. Surgery is performed for recalcitrant disease refractory to medical therapy. This article presents a brief summary of current evidence-based management of CRS. The authors recommend referring to the “European position paper on rhinosinusitis and nasal polyps” by Fokkens et alCitation33 for a more comprehensive review.
Topical medical therapy
Topical medication delivery
The delivery of topical medications has been the subject of recent investigations. Distribution of topical solution to the unoperated sinuses is limited,Citation41 with less than 2% of the total irrigation volume attaining sinus penetration in the setting of CRS with mucosal edema.Citation42 Similar findings apply to nebulization, with less than 3% sinus penetration.Citation43 Pre-surgery nasal sprays are the least effective of all application methods.Citation41 Thus, ESS is essential to allow effective topical distribution to the sinuses.Citation41,Citation44 Singhal et alCitation45 further demonstrated this in a cadaver study which showed improved penetration of irrigant as sinus ostium dimensions increase. A critical diameter of 4.7 mm was noted to allow maximal penetration in the maxillary and sphenoid sinuses. Head position was found to effect penetration of the frontal sinus, with less penetration seen with the head in neutral position versus a forward-angled position.Citation45
Multiple studies suggest large volume devices have the best efficacy following ESS.Citation41,Citation42,Citation44 In Harvey and colleagues’Citation41 experiment using Gastroview irrigation in cadavers, distribution was significantly higher with use of a neti pot or squeeze bottle versus a pressurized spray.
Intranasal saline
Numerous studies have been performed to evaluate the efficacy of saline nasal irrigation in relieving CRS symptoms and improving clinical outcomes. Harvey et alCitation46 published a meta-analysis in 2007, which identified eight randomized controlled trials in which saline was compared with either no treatment, placebo, or as a treatment adjunct. The authors concluded that saline nasal irrigation is beneficial in relieving symptoms of CRS when used as the sole modality of treatment, as well as a treatment adjunct.Citation46 Rudmik et alCitation47 recently published an evidence-based review of topical therapies in the management of CRS including eight randomized controlled trials (RCTs) and one meta-analysis evaluating saline. They recommended sinonasal saline irrigations as an adjunct to other topical therapy strategies due to improved symptoms and health-related quality of life, an excellent safety profile, and preponderance of benefit over harm.Citation47
Intranasal saline has been shown to be beneficial in both unoperated and postoperative patients. High volume, low pressure irrigation devices have demonstrated superiority over other methods of delivery. Pynnonen et alCitation48 evaluated the efficacy of large volume, low-pressure saline irrigation versus saline spray in non-postoperative patients in an RCT. The irrigation group had improved symptoms over the spray group as measured by the Sino-Nasal Outcome Test (SNOT-20).Citation48 Liang et alCitation49 performed a randomized trial of large-volume saline irrigation in CRS patients post-ESS and found significant benefit in symptoms and endoscopy scores in patients with mild CRS. However, there was no significant difference in those with severe CRS.Citation49
Other studies evaluating the effect of intranasal saline on endoscopic appearance in CRS have been performed. A single-blinded RCT in which patients post-ESS performed unilateral nasal douching demonstrated improved discharge and edema at 3 weeks, but no difference in adhesions or crusting. There were no differences in nasal endoscopy noted at 3 months.Citation50 One criticism of this study is the low-volume saline irrigation protocol (2 mL atomized 3 times daily) used.
lists ten RCTs evaluating the impact of intranasal saline on clinical outcomes in CRS patients, with type of saline (hypertonic versus isotonic), delivery method, and outcomes noted. Both pre-surgical and post-ESS studies were included. All seven pre-surgical RCTsCitation48,Citation51–Citation55,Citation57 demonstrated improved symptoms and health-related quality of life, although the study by Heatley et alCitation53 showed no difference between reflexology as placebo and saline irrigation groups. Of the three post-ESS studies, two RCTs showed improved outcomes with intranasal saline,Citation49,Citation50 while the third showed no difference in patient symptom scores between normal saline, hypertonic saline, and no irrigation groups.Citation56 Overall, saline nasal irrigations are well tolerated. Side effects are uncommon, but include nasal discomfort, drainage, epistaxis, headache, and otalgia.Citation46 Most studies suggest symptom and health-related quality of life improvement with usage. The superiority of hypertonic versus isotonic saline remains unclear.
Table 1 Randomized controlled trials evaluating intranasal saline in CRS
Topical steroids
Glucocorticoids are a mainstay of CRS treatment. Steroids reduce eosinophil viability and activationCitation58,Citation59 and may indirectly reduce the secretion of chemotactic cytokines by nasal mucosa and polyp epithelial cells.Citation59 Topical sinonasal steroids are used to achieve these anti-inflammatory effects on a local level, thereby minimizing systemic effects. They have an excellent safety profile and are well tolerated over long periods of time.
Topical steroids can be subdivided into conventional US Food and Drug Administration (FDA)-approved formulations for nasal use, and nonconventional formulations lacking FDA approval specifically for nasal therapy. Conventional FDA-approved solutions available by metered-dose, low-volume topical sprays include fluticasone proprionate, mometasone furoate, ciclesonide, budesonide, flunisolide, fluticasone furoate, beclomethasone dipropionate monohydrate, and triamcinolone acetonide.Citation47 Nonconventional off-label use of steroid nasal irrigation is growing in popularity with rhinologists, as higher volume and higher steroid concentrations can be used. Large volume nasal irrigation with budesonide, a potent anti-inflammatory corticosteroid with a high ratio of topical-to-systemic activity, has become increasingly popular in patients with CRS and has been shown to be efficacious and well tolerated by patients.Citation60,Citation61
Fokkens et alCitation33 performed a recent systematic review of RCTs for evidence of benefit in treating CRSsNP with topical corticosteroids, which included eleven studies. Of these, data from five studies could be pooled for meta-analysis, demonstrating significant benefit in the topical steroid group when compared with placebo. When the surgical state of the patients was assessed on subgroup analysis, only patients with prior surgery for CRSsNP had symptom improvement. There was no improvement for patients without surgery.Citation33
Topical steroids are also effective in CRSwNP. Fokkens et alCitation33 performed a separate systematic review of RCTs for CRSwNP treated with topical corticosteroids, which yielded 38 studies. Meta-analysis showed intranasal steroids, when compared to placebo, improved symptoms, polyp size, polyp recurrence, and nasal airflow. In the subgroup analysis, patients with sinus surgery responded to topical steroids greater than patients without sinus surgery in polyp size reduction.Citation33
Rudmik et alCitation47 identified five meta-analyses evaluating the role of conventional FDA-approved topical nasal steroid therapy on clinical outcomes, combining CRSsNP and CRSwNP. Four of the five meta-analyses demonstrated significant improvement in symptoms, endoscopic appearance, or both.Citation62–Citation65 The meta-analysis by Kalish et alCitation66 combined the results of six RCTs to evaluate the effect of topical steroid therapy in CRSsNP, and was the only study finding insufficient evidence to demonstrate a significant benefit with treatment. However, the more recent meta-analysis of topical steroid therapy in CRSsNP by Snidvongs et alCitation65 included ten RCTs and showed improved overall symptom scores with topical steroid therapy.
There is a large body of evidence demonstrating the efficacy of conventional topical steroid therapy in both patients with CRSsNP and CRSwNP, with improved symptoms, endoscopic appearance, and reduced polyp size. Side effects are uncommon, but include epistaxis, dry nose, nasal irritation, headache, and cough.Citation33,Citation47
Limited high-quality data exists regarding off-label steroid nasal irrigation. One RCT by Rotenberg et al,Citation67 compared saline irrigation, saline plus budesonide spray (separately), and saline plus budesonide spray (combined) in patients with AERD post-ESS. All groups showed improved disease status compared with baseline, but there was no difference between groups.Citation67 Further studies are indicated to determine potential benefits and side-effects of off-label topical steroid usage.
Topical antibiotics
The goal of topical antibiotic therapy is local delivery of high drug concentrations while reducing systemic effects. However, the efficacy of topical antibiotics has not been proven. Four placebo-controlled RCTs of topical antibiotics in CRS have been performed ().Citation68–Citation71 Three RCTs show no benefit to topical antibiotics over saline; however, none of these investigations employed large volume positive pressure irrigation. The first study by Sykes et alCitation68 evaluated topical sprays with neomycin, while the others used nebulized tobramycin and bacitracin/colimycin, respectively.Citation69,Citation70 One possible reason for lack of efficacy in these studies is inadequate sinus penetration with the delivery methods used. A systematic review by Lim et alCitation72 similarly concluded that the evidence for use of topical antibacterials is limited. The highest level of evidence currently exists for studies using postsurgical patients and culture-directed therapy.Citation72
Table 2 Randomized controlled trials evaluating topical antibiotics in CRS
Jervis-Bardy et alCitation71 recently published a double-blinded, placebo-controlled RCT evaluating topical mupirocin irrigations versus saline on bacterial cultures, symptoms, and endoscopy scores in post-ESS patients with a pre-treatment S. aureus positive culture. They found 0% versus 88.9% S. aureus-negative sinonasal culture at 1 month in the saline versus mupirocin groups, respectively. Endoscopy scores at 1 month were significantly improved in the mupirocin group compared with the saline group; however, there were no significant differences in symptoms between groups.Citation71
Recent investigations of topical antibiotics in CRS have been directed toward biofilms. The topical application of mupirocin, ciprofloxacin, and vancomycin on established in-vitro biofilms of S. aureus isolated from patients with CRS was evaluated by Ha et al.Citation73 Their study showed mupirocin was capable of reducing biofilm mass by greater than 90% at safe concentrations. Ciprofloxacin and vancomycin were largely ineffective at concentrations within safe dosage ranges.Citation73 Thus, topical antibiotics have potential efficacy; however, there is currently a low level of evidence for their use.
Emerging strategies in topical therapy
The treatment of biofilms is a subject under current investigation. In addition to topical antibiotics, newer research has been directed toward surfactants, which reduce water surface tension and may help to dissolve biofilms.Citation74 Baby shampoo nasal irrigation has been studied against biofilms in symptomatic postoperative patients. One percent baby shampoo in normal saline was found to be the optimal concentration for inhibition of Pseudomonas species biofilm formation in vitro. Using this solution twice daily for 4 weeks, nearly 50% of patients experienced an overall improvement in symptoms, with 60% noting improvement of thick mucus and postnasal drainage.Citation75
Other novel nasal irrigation additives include xylitol and sodium hypochlorite. Xylitol is a naturally occurring sugar substitute commonly used in chewing gum, which has been shown to reduce dental caries.Citation76 A recent RCT evaluating xylitol in water as a nasal irrigant in CRS showed improved sinonasal symptoms over saline and was well tolerated.Citation77 Sodium hypochlorite is a bleaching and disinfecting agent effective against S. aureus and Pseudomonas aeruginosa. Nasal lavage with 0.05% sodium hypochlorite in saline twice daily for 3 months was well tolerated in patients and showed a significant improvement in symptoms and endoscopic appearance.Citation78
Systemic medical therapy
Oral steroids
Oral corticosteroids have been used in patients with CRSwNP for many years due to a positive effect on nasal polyp size, symptoms, and nasal expiratory peak flow. A recent systematic review by Poetker et alCitation79 identified five RCTs supporting the use of oral steroids in the short-term management of CRSwNP ().
Table 3 Randomized controlled trials evaluating oral steroids in CRSwNP
Hissaria et alCitation80 randomized 41 CRSwNP patients to receive 50 mg of prednisolone or placebo for 14 days. The steroid group showed a statistically significant improvement over placebo in symptoms and quality of life outcome measures, in addition to nasal endoscopy and MRI. Kirtsreesakul et alCitation83 also found statistically significant subjective and objective improvement in prednisolone-treated patients over controls. Vaidyanathan et alCitation84 again showed statistically significant subjective and objective improvement in prednisolone-treated patients over controls. Interestingly, their outcomes also included markers of adrenal suppression and bone turnover. They found overnight urinary cortisol was suppressed to 50% of baseline and adrenocorticotropic hormone-stimulated serum cortisol suppressed to 86% of baseline at the end of the treatment period (2 weeks) in the steroid arm. They also showed a transient decrease in markers of osteoblast activity at 2 weeks. Both of these effects were no longer evident at 10 and 28 weeks.Citation84 Finally, the RCT by Wright and AgrawalCitation85 demonstrated the beneficial effects of perioperative systemic steroids in patients undergoing ESS for CRSwNP. They found a higher percentage of severely inflamed sinonasal mucosa and more technically difficult surgery in patients not pretreated with systemic steroids. In addition, endoscopic assessment of patients treated postop-eratively with systemic steroids revealed clinically healthier cavities compared with controls.Citation85
There is limited evidence supporting oral steroid therapy in CRSsNP. A systematic review by Lal and HwangCitation86 revealed no RCTs of oral steroids in CRSsNP or any clinical study employing systemic corticosteroids alone. They identified two retrospectiveCitation87,Citation88 and one prospective studyCitation89 using oral steroids in combination with antibiotics and nasal steroids to treat CRSsNP. Tosca et alCitation89 prospectively studied children with allergic and nonallergic CRS and asthma, showing oral and intranasal steroids with oral antibiotics improved endoscopy and decreased inflammatory infiltrate. The retrospective study by Subramanian et alCitation87 included both CRSwNP and CRSsNP, but found the CRSsNP patients had better outcomes with a multidrug regimen including oral steroids. Lal et alCitation88 noted improved symptom resolution in CRSsNP compared with all CRS patients in a retrospective study. Due to limited low level evidence of subjective and objective improvement, oral steroids in CRSsNP remains optional.Citation79,Citation86
Rupa et alCitation90 published the only RCT evaluating post-ESS oral steroids in patients with AFS. Twenty-four patients were randomized to receive prednisolone or placebo, while patients in both arms received concurrent ranitidine, itraconazole, and fluticasone nasal spray. At 12 weeks, patients in the steroid arm had complete resolution of symptoms and polypoid disease on endoscopy, whereas only one patient in the placebo arm had full symptom and endoscopic resolution of disease.Citation90 Two prospective studies found oral steroids similarly beneficial in AFS.Citation91,Citation92
Systemic corticosteroids have a significant side effect profile, which increases with dose and duration of treatment. Patients should be counseled regarding the possible negative effects on bone mineral density, hyperglycemia, weight gain, early cataract formation, pituitary–hypothalamic axis suppression, sleep disturbance, and exacerbation of psychiatric conditions.Citation93 Given the natural history of CRS requiring ongoing treatment over long periods of time, the short-lived benefits of systemic steroids must be balanced with the long-term potential side effects. The preponderance of benefit over harm is better supported by trials in CRSwNP than in CRSsNP, where evidence is insufficient.
Oral antibiotics
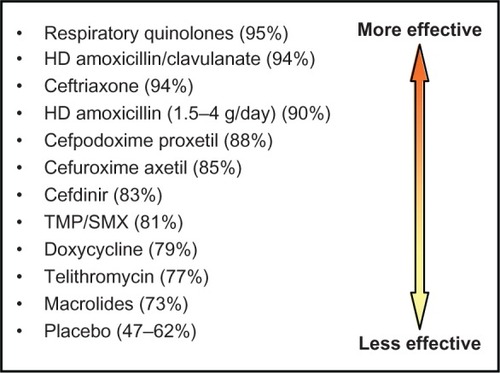
Oral antibiotics are the most commonly prescribed medication for CRSCitation31 and remain a mainstay of treatment. Despite this, there is a surprising paucity of quality data regarding efficacy. There is level 2 evidence for short-term treatment of CRSsNP in exacerbations with a positive culture based on two RCTs,Citation94,Citation95 though no placebo-controlled studies have been performed. In general, first-line antibiotics for CRS exacerbations include amoxicillin-clavulanate and second- or third-generation cephalosporins. The respiratory quinolones are helpful second-line agents for refractory cases ().Citation96
Figure 4 Efficacy of antibiotics in CRS.
Note: Data from Anon JB, et al. Otolaryngol Head Neck Surg. 2004;130(1 Suppl):1–45.
Abbreviations: HD, high dose; TMP/SMX, trimethoprim-sulfamethoxazole.
The increasing prevalence of S. aureus and antimicrobial resistance in CRS highlights the importance of using culture-directed antimicrobial therapy with the goal of minimizing future resistance patterns.Citation97 Bhattacharyya and KepnesCitation98 analyzed 701 bacterial isolates among 392 culture samples from patients with CRS, and concluded that antibiotic resistance seems to be emerging for erythromycin at a rate higher than for other antibiotics such as methicillin, clindamycin, gentamicin, tetracycline, sulfamethoxazole, and levofloxacin. As the emergence of antibiotic resistance has increased the failure rate of empiric treatment, culture-directed therapy has become the standard of care when treating CRS with antibiotics.Citation99
Based on the emerging pattern of drug-resistance, it is not surprising that macrolides have often been the antibiotic of choice in long-term therapy of CRS. Macrolides have anti-inflammatory and immune-modulatory effects similar to glucocorticoids. Knowledge of this dates back to the publication of long-term, low-dose erythromycin treatment of diffuse panbronchiolitis, which improved concomitant CRS.Citation100
Two placebo-controlled RCTs have studied the effect of a macrolide on signs, symptoms, and quality of life in CRS over a period of 12 weeks.Citation101,Citation102 While the first investigation showed clinical efficacy of roxithromycin with a response rate of 67% in the treatment group versus 22% in the placebo group,Citation101 the second study showed no significant difference between azithromycin and placebo groups.Citation102 The discrepancy in these results may be secondary to divergent CRS patient populations, as the studies had different inclusion criteria, and macrolides have been found to be more effective in certain patient populations. For example, normal IgE levels are associated with a higher response rate to macrolide treatment versus elevated IgE levels,Citation101,Citation103,Citation104 which highlights the need to individualize CRS therapy.
Doxycycline is another antibiotic with anti- inflammatory properties. In a multicenter double-blind placebo- controlled trial, both methylprednisolone and doxycycline for 20 days decreased polyp size compared with placebo in CRSwNP.Citation82
Long-term, low-dose antibacterial treatment presents the greatest concern for the emergence of resistant bacterial strains. In a placebo-controlled RCT exposing oral strepto-coccal flora of healthy volunteers to macrolides, antibiotic use was shown to be the most important driver of antibiotic resistance.Citation105 Consideration should also be given to the well known adverse effects of systemic antibiotics, including abdominal pain, diarrhea, Clostridium difficile colitis, anaphylaxis, rash, tendinitis, and tendon rupture. Some of these effects are exacerbated with concomitant oral steroid usage. Patient counseling regarding these potential effects is recommended prior to prescribing oral antibiotics.
Antifungals
Fungi have been postulated to be a potential cause of CRS,Citation32 therefore oral and topical antifungal agents have been explored in its management. Although an early RCT found topical amphotericin to be beneficial,Citation106 multiple follow-up RCTs evaluating the efficacy of topical amphotericin in CRS have not supported its use.Citation107–Citation109 A recent systematic review of the literature with meta-analysis was performed by Sacks et alCitation110 to assess the potential advantage of either topical or systemic antifungal therapy in the symptomatic treatment of CRS. This yielded five studies investigating topical and one study investigating systemic antifungals, all of which were RCTs. Pooled meta-analysis showed no statistically significant benefit of topical or systemic antifungals over placebo. Interestingly, symptoms scores statistically favored placebo and adverse event reporting was higher in the antifungal group.Citation110
Emerging strategies in systemic therapy
Leukotriene antagonists
Leukotriene antagonists, such as montelukast, zafirlukast, and zileuton, have been evaluated in numerous studies involving patients with CRSwNP and AERD. Results have been mixed. Several uncontrolled open-label studies suggest benefit of antileukotrienes on symptomatology,Citation111 nasal polyp, and CT scores.Citation112 However, data from RCTs do not consistently support the benefit of antileukotriene therapy in all CRS patients. Mostafa et alCitation113 randomized 40 CRSwNP patients to either 10 mg monteleukast or beclomethasone nasal spray daily for 1 year, finding no differences in disease relapse frequency and greater overall symptom improvement with beclomethasone. Another RCT separated 38 CRSwNP patients into two groups. The first received oral prednisolone for 14 days plus budesonide nasal spray for 8 weeks. The second received the same treatment with the addition of 10 mg oral monteleukast. The addition of monteleukast failed to show a significant effect on the overall symptom score, although reduction in headache, facial pain, and sneezing reached significance.Citation114
Anti-IgE therapy
In CRSwNP, total IgE levels in nasal secretions, nasal polyp homogenisates and blood serum have been shown to be higher than in controls.Citation115 Omalizumab is a recombinant humanized monoclonal antibody that selectively binds to human IgE and reduces levels in serum and tissue, which is approved for patients with moderate to severe or severe allergic asthma. Though anecdotal reports showed beneficial effects of omalizumab in CRSwNP, a small RCT showed no significant difference in sinus opacification or SNOT-20 scores.Citation116 This RCT, however, was underpowered. Further investigation regarding anti-IgE therapy may be warranted.
Anti-IL-5 therapy
Abundant eosinophilia is also found in the majority of patients with CRSwNP. IL-5, produced by Th-2 and mast cells, is a key player in eosinophil growth, recruitment, and activation. IL-5 has been found to be significantly increased in patients with nasal polyps compared with controls. Mepolizumab and reslizumab are humanized anti-IL-5 monoclonal antibodies currently undergoing investigation in the treatment of CRSwNP. A double-blind, placebo-controlled RCT including 30 patients with severe nasal polyposis refractory to corticosteroid therapy found two single intravenous injections of mepolizumab achieved a statistically significant reduction in nasal polyp size for at least 1 month when compared with placebo. In addition, significantly less sinus opacification was observed in the treatment arm.Citation117 Another double-blind, placebo-controlled RCT showed a single infusion of reslizumab in CRSwNP patients had no significant improvement on symptoms or nasal polyp score over controls.Citation118 Anti-IL-5 therapy is an interesting area for future research.
Aspirin desensitization
Aspirin desensitization for patients with AERD has been evaluated in several case series and prospective studies; however, no RCTs have been performed. Forer et alCitation119 found significantly improved symptoms in patients undergoing aspirin desensitization, though objective results were not significant. Stevenson et alCitation120 also noted significantly improved nasal symptoms in 25 AERD patients following aspirin desensitization. Rozsasi et alCitation121 allocated AERD patients to either take 100 mg or 300 mg aspirin daily. After 1 year of therapy, all patients in the 100 mg group had developed recurrent nasal polyps, whereas no patient in the 300 mg group had recurrent nasal polyps on endoscopy.Citation121 Risks of oral aspirin desensitization include severe hypersensitivity, anaphylaxis, and gastrointestinal side effects.
Endoscopic sinus surgery
Numerous large, well organized prospective studies have shown endoscopic sinus surgery (ESS) to be safe and effective in managing both patients with CRSsNP and CRSwNP who have failed adequate control with medical treatment.Citation122,Citation123 The goals of ESS include eradication of inflammatory tissue and osteitis, implementation of adequate drainage and ventilation pathways, restoration of mucociliary function, creation of access for topical medication, reduction of acute exacerbations and systemic medication usage, and quality of life improvement. A review of 21 studies including 2070 patients with CRS found all symptoms were improved after a mean period of 13 months following ESS, with nasal obstruction improving the most, facial pain and postnasal discharge demonstrating moderate improvements, and headache improving the least.Citation124 Improvements in generic and disease-specific quality of life with surgery have also been shown.Citation122 ESS significantly decreases antibiotic utilization in CRSwNP and CRSsNP.Citation125 In a prospective multi-institutional study comparing medical and surgical therapy for CRS, patients electing ESS experienced significantly higher levels of improvement based on two validated disease-specific quality-of-life instruments.Citation126 Approximately 15%–20% of patients require revision sinus surgery. Previous revision surgery, extensive polyps, bronchial asthma, aspirin intolerance, and cystic fibrosis are predictors of patients who may require revision surgery.Citation123
Conclusion
CRS is a complex condition with profound effects on patient quality of life and health care expenditure. Its management continues to challenge both patients and health care providers. There is now a preponderance of evidence supporting the concept that inflammation, as opposed to infection, is the dominant etiologic factor in CRS. While systemic antibiotics and steroids were a mainstay of treatment in the past, the focus is now shifting toward topical therapy, improved nasal delivery systems, and novel antiinflammatory therapies. Potential development of microbial resistance remains a salutary concern in patients treated with repeated or prolonged antimicrobial agents. Immune modulators, such as anti-IgE and anti-IL5 antibodies, are promising areas of ongoing research. Surgery continues to play an important role in management of recalcitrant disease, resulting in quality-of-life improvement and assisting in aggressive medical management. The complex and diverse nature of CRS requires an individualized approach to both medical and surgical management in a multidisciplinary setting.
Disclosure
The authors have nothing to disclose, nor any conflicts of interest.
References
- RosenfeldRMAndesDBhattacharyyaClinical practice guideline: adult sinusitisOtolaryngol Head Neck Surg2007137Suppl 3S1S3117761281
- BenningerMSFergusonBJHadleyJAAdult chronic rhinosinusitis: definitions, diagnosis, epidemiology, and pathophysiologyOtolaryngol Head Neck Surg2003129Suppl 3S1S3212958561
- Van ZeleTClaeysSGevaertPDifferentiation of chronic sinus diseases by measurement of inflammatory mediatorsAllergy20066111280128917002703
- LeeLNBhattacharyyaNRegional and specialty variations in the treatment of chronic rhinosinusitisLaryngoscope201112151092109721520129
- PleisJRLucasJ WWardB WSummary health statistics for US adults: National Health Interview Survey, 2008Vital Health Stat 102009242115720821903
- AnonJBJacobsMRPooleMDAntimicrobial treatment guidelines for acute bacterial rhinosinusitisOtolaryngol Head Neck Surg2004130Suppl 114514726904
- CollinsJGPrevalence of selected chronic conditions: United States, 1990–1992Vital Health Stat 1019971941899046223
- BlackwellDLCollinsJGColesRSummary health statistics for US adults: National Health Interview Survey, 1997Vital Health Stat 102002205110915786607
- ShashyRGMooreEJWeaverAPrevalence of the chronic sinusitis diagnosis in Olmsted County, MinnesotaArch Otolaryngol Head Neck Surg2004130332032315023840
- ChenYDalesRLinMThe epidemiology of chronic rhinosinusitis in CanadiansLaryngoscope200311371199120512838019
- GreisnerWA3rdSettipaneGAHereditary factor for nasal polypsAllergy Asthma Proc19961752832868922148
- AhsanSFJumansSNunezDAChronic rhinosinusitis: a comparative study of disease occurrence in North of Scotland and Southern Caribbean otolaryngology outpatient clinics over a two month periodScott Med J200449413013315648704
- HastanDFokkensWJBachertCChronic rhinosinusitis in Europe – an underestimated disease. A GA(2)LEN studyAllergy20116691216122321605125
- PilanRRPinnaFRBezerraTFPrevalence of chronic rhinosinusitis in Sao PauloRhinology201250212913822616073
- JohanssonLAkerlundAHolmbergKMelenIBendeMPrevalence of nasal polyps in adults: the Skovde population based studyAnn Otol Rhinol Laryngol2003112762562912903683
- MinYGJungHWKimHSParkSKYooKYPrevalence and risk factors of chronic sinusitis in Korea: results of a nationwide surveyEur Arch Otorhinolaryngol199625374354398891490
- HedmanJKaprioJPoussaTNieminenMMPrevalence of asthma, aspirin intolerance, nasal polyposis and chronic obstructive pulmonary disease in a population-based studyInt J Epidemiol199928471772210480701
- KlossekJMNeukirchFPribilCPrevalence of nasal polyposis in France: a cross-sectional, case-control studyAllergy200560223323715647046
- LarsenPLTosMOrigin of nasal polypsLaryngoscope199110133053122000020
- LarsenPLTosMSite of origin of nasal polyps. Transcranially removed nasoethmoidal blocks as a screening method for nasal polyps in autopsy materialRhinolog y1995334185188
- Roca-FerrerJGarcia-GarciaFJPeredaJReduced expression of COXs and production of prostaglandin E(2) in patients with nasal polyps with or without aspirin-intolerant asthmaJ Allergy Clin Immunol20111281667221397936
- KernRCConleyDBWalshWPerspectives on the etiology of chronic rhinosinusitis: an immune barrier hypothesisAm J Rhinol200822654955918786300
- Perez-NovoCAWaeytensAClaeysCCauwenbergeP VBachertCStaphylococcus aureus enterotoxin B regulates prostaglandin E2 synthesis, growth, and migration in nasal tissue fibroblastsJ Infect Dis200819771036104318419541
- TanBKLiQZSuhLEvidence for intranasal antinuclear autoantibodies in patients with chronic rhinosinusitis with nasal polypsJ Allergy Clin Immunol201112861198120621996343
- LarsonDAHanJKMicrobiology of sinusitis: does allergy or endoscopic sinus surgery affect the microbiologic fora?Curr Opin Otolaryngol Head Neck Surg201119319920321358332
- NadelDMLanzaDCKennedyDWEndoscopically guided cultures in chronic sinusitisAm J Rhinol19981242332419740915
- StephensonMFMfunaLDowdSEMolecular characterization of the polymicrobial fora in chronic rhinosinusitisJ Otolaryngol Head Neck Surg201039218218720211106
- RamadanHHSanclementJAThomasJGChronic rhinosinusitis and biofilmsOtolaryngol Head Neck Surg2005132341441715746854
- PsaltisAJWeitzelEKHaKRWormaldPJThe effect of bacterial bio-films on post-sinus surgical outcomesAm J Rhinol20082211618284851
- PrinceAASteigerJDKhalidANPrevalence of biofilm-forming bacteria in chronic rhinosinusitisAm J Rhinol200822323924518588755
- FairbanksDNInflammatory diseases of the sinuses: bacteriology and antibioticsOtolaryngol Clin North Am19932645495598414527
- PonikauJUSherrisDAKernEBThe diagnosis and incidence of allergic fungal sinusitisMayo Clin Proc199974987788410488788
- FokkensWJLundVJMullolJEuropean position paper on rhinosinusitis and nasal polyps 2012Rhinol Suppl2012231298
- StankiewiczJAChowJMA diagnostic dilemma for chronic rhinosinusitis: definition accuracy and validityAm J Rhinol200216419920212222944
- OrlandiRRTerrellJEAnalysis of the adult chronic rhinosinusitis working definitionAm J Rhinol200216171011895197
- HwangPHIrwinSBGriestSECaroJENesbitGMRadiologic correlates of symptom-based diagnostic criteria for chronic rhinosinusitisOtolaryngol Head Neck Surg2003128448949612707650
- BhattacharyyaNLeeLNEvaluating the diagnosis of chronic rhinosinusitis based on clinical guidelines and endoscopyOtolaryngol Head Neck Surg2010143114715120620634
- BhattacharyyaNFriedM PThe accuracy of computed tomography in the diagnosis of chronic rhinosinusitisLaryngoscope2003113112512912514395
- BhattacharyyaNJonesDTHillMShapiroNLThe diagnostic accuracy of computed tomography in pediatric chronic rhinosinusitisArch Otolaryngol Head Neck Surg200513091029103215381587
- LinH WBhattacharyyaNDiagnostic and staging accuracy of magnetic resonance imaging for the assessment of sinonasal diseaseAm J Rhinol Allergy2009231363919379610
- HarveyRJGoddardJCWiseSKSchlosserRJEffects of endoscopic sinus surgery and delivery device on cadaver sinus irrigationOtolaryngol Head Neck Surg2008139113714218585576
- SnidvongsKChaowanapanjaPAeumjaturapatSChusakulSPraweswararatPDoes nasal irrigation enter paranasal sinuses in chronic rhinosinusitis?Am J Rhinol200822548348618954507
- HyoNTakanoHHyoYParticle deposition efficiency of therapeutic aerosols in the human maxillary sinusRhinology198927117262740721
- GroblerAWeitzelEKBueleAPre- and postoperative sinus penetration of nasal irrigationLaryngoscope2008118112078208118641522
- SinghalDWeitzelEKLinEEffect of head position and surgical dissection on sinus irrigant penetration in cadaversLaryngoscope2010120122528253121058393
- HarveyRHannanSABadiaLScaddingGNasal saline irrigations for the symptoms of chronic rhinosinusitisCochrane Database Syst Rev20073CD00639417636843
- RudmikLHoyMSchlosserRJTopical therapies in the management of chronic rhinosinusitis: an evidence-based review with recommendationsInt Forum Allergy Rhinol Epub October 8, 2012
- PynnonenMAMukerjiSSKimHMAdamsMETerrellJENasal saline for chronic sinonasal symptoms: a randomized controlled trialArch Otolaryngol Head Neck Surg2007133111115112018025315
- LiangKLSuMCTsengHCJiangRSImpact of pulsatile nasal irrigation on the prognosis of functional endoscopic sinus surgeryJ Otolaryngol Head Neck Surg200837214815319128603
- FreemanS?RSivayohamESJepsonKde CarpentierJA preliminary randomized controlled trial evaluating the efficacy of saline douching following endoscopic sinus surgeryClin Otolaryngol200833546246518983380
- ShoseyovDBibiHShaiPShoseyovNShazbergGHurvitzHTreatment with hypertonic saline versus normal saline nasal wash of pediatric chronic sinusitisJ Allergy Clin Immunol199810156026059600495
- BachmannGHommelGMichelOEffect of irrigation of the nose with isotonic salt solution on adult patients with chronic paranasal sinus diseaseEur Arch Otorhinolaryngol20002571053754111195032
- HeatleyDGMcConnellKEKilleTLLeversonGENasal irrigation for the alleviation of sinonasal symptomsOtolaryngol Head Neck Surg20011251444811458213
- RabagoDZgierskaAMundtMBarrettBBobulaJMaberryREfficacy of daily hypertonic saline nasal irrigation among patients with sinusitis: a randomized controlled trialJ Fam Pract200251121049105512540331
- CordraySHarjoJBMinerLComparison of intranasal hypertonic dead sea saline spray and intranasal aqueous triamcinolone spray in seasonal allergic rhinitisEar Nose Throat J200584742643016813032
- PintoJMElwanySBaroodyFMNacierioRMEffects of saline sprays on symptoms after endoscopic sinus surgeryAm J Rhinol200620219119616686387
- HauptmanGRyanMWThe effect of saline solutions on nasal patency and mucociliary clearance in rhinosinusitis patientsOtolaryngol Head Neck Surg2007137581582117967652
- XaubetAMullolJLopezEComparison of the role of nasal polyp and normal nasal mucosal epithelial cells on in vitro eosinophil survival. Mediation by GM-CSF and inhibition by dexamethasoneClin Exp Allergy19942443073178039016
- MullolJXaubetAGayaACytokine gene expression and release from epithelial cells. A comparison study between healthy nasal mucosa and nasal polypsClin Exp Allergy19952576076158521179
- LildholdtTRundcrantzHLindqvistNEfficacy of topical corticosteroid powder for nasal polyps: a double-blind, placebo-controlled study of budesonideClin Otolaryngol Allied Sci199520126307788929
- AdappaNDWeiCCPalmerJNNasal irrigation with or without drugs: the evidenceCurr Opin Otolaryngol Head Neck Surg2012201535722143336
- JoeSAThambiRHuangJA systematic review of the use of intranasal steroids in the treatment of chronic rhinosinusitisOtolaryngol Head Neck Surg2008139334034718722209
- RudmikLSchlosserRJSmithTLSolerZMImpact of topical nasal steroid therapy on symptoms of nasal polyposis: a meta-analysisLaryngoscope201212271431143722410935
- SnidvongsKKalishLSacksRCraigJCHarveyRJTopical steroid for chronic rhinosinusitis without polypsCochrane Database Syst Rev20118CD00927421833974
- SnidvongsKKalishLSacksRSivasubramanianRCopeDHarveyRJTopical steroids for nasal polypsCochrane Database Syst Rev
- KalishLHArendtsGSacksRCraigJCTopical steroids in chronic rhinosinusitis without polyps: a systematic review and meta-analysisOtolaryngol Head Neck Surg2009141667468319932837
- RotenbergB WZhangIArraIPaytonKBPostoperative care for Samter’s triad patients undergoing endoscopic sinus surgery: a double-blinded, randomized controlled trialLaryngoscope2011121122702270521997904
- SykesDAWilsonRChanKLMackayISColePJRelative importance of antibiotic and improved clearance in topical treatment of chronic mucopurulent rhinosinusitis. A controlled studyLancet1986285033593602874366
- DesrosiersMYSalas-PratoMTreatment of chronic rhinosinusitis refractory to other treatments with topical antibiotic therapy delivered by means of a large-particle nebulizer: results of a controlled trialOtolaryngol Head Neck Surg2001125326526911555764
- VidelerWJvan DrunenCMReitsmaJBFokkensWJNebulized bacitracin/colimycin: a treatment option in recalcitrant chronic rhinosinusitis with Staphylococcus aureus? A double-blind, randomized, placebo-controlled, cross-over pilot studyRhinology2008462929818575008
- Jervis-BardyJBoaseSPsaltisAForemanAWormaldPJA randomized trial of mupirocin sinonasal rinses versus saline in surgically recalcitrant staphylococcal chronic rhinosinusitisLaryngoscope2012122102148215322865576
- LimMCitardiMJLeongJLTopical antimicrobials in the management of chronic rhinosinusitis: a systematic reviewAm J Rhinol200822438138918702902
- HaKRPsaltisAJButcherARWormaldPJTanLWIn vitro activity of mupirocin on clinical isolates of Staphylococcus aureus and its potential implications in chronic rhinosinusitisLaryngoscope2008118353554018090864
- LeTPsaltisATanLWWormaldPJThe efficacy of topical antibiofilm agents in a sheep model of rhinosinusitisAm Journal Rhinol200822656056719178792
- ChiuAGPalmerJNWoodworthBABaby shampoo nasal irrigations for the symptomatic post-functional endoscopic sinus surgery patientAm J Rhinol2008221343718284857
- LynchHMilgromPXylitol and dental caries: an overview for cliniciansJ Calif Dent Assoc200331320520912693818
- WeissmanJDFernandezFHwangPHXylitol nasal irrigation in the management of chronic rhinosinusitis: a pilot studyLaryngoscope2011121112468247221994147
- RazaTElsherifHSZulianelloLPlouin-GaudonILandisBNLacroixJSNasal lavage with sodium hypochlorite solution in Staphylococcus aureus persistent rhinosinusitisRhinology2008461152218444487
- PoetkerDMJakubowskiLALalDHwangPHWrightEDSmithTLOral corticosteroids in the management of adult chronic rhinosinusitis with and without nasal polyps: an evidence-based review with recommendationsInt Forum Allergy Rhinol Epub August 7, 2012
- HissariaPSmithWWormaldPJShort course of systemic corticosteroids in sinonasal polyposis: a double-blind, randomized, placebo-controlled trial with evaluation of outcome measuresJ Allergy Clin Immunol2006118112813316815148
- KroflicBCoerABaudoinTKalogjeraLTopical furosemide versus oral steroid in preoperative management of nasal polyposisEur Arch Otorhinolaryngol2006263876777116685542
- Van ZeleTGevaertPHoltappelsGOral steroids and doxycycline: two different approaches to treat nasal polypsJ Allergy Clin Immunol201012551069107620451040
- KirtsreesakulVWongsritrangKRuttanapholSClinical efficacy of a short course of systemic steroids in nasal polyposisRhinology201149552553222125782
- VaidyanathanSBarnesMWilliamsonPHopkinsonPDonnanPTLipworthBTreatment of chronic rhinosinusitis with nasal polyposis with oral steroids followed by topical steroids: a randomized trialAnn Intern Med2011154529330221357906
- WrightEDAgrawalSImpact of perioperative systemic steroids on surgical outcomes in patients with chronic rhinosinusitis with polyposis: evaluation with the novel Perioperative Sinus Endoscopy (POSE) scoring systemLaryngoscope200711711 Pt 2, Suppl 11512818075447
- LalDHwangPHOral corticosteroid therapy in chronic rhinosinusitis without polyposis: a systematic reviewInt Forum Allergy Rhinol20111213614322287332
- SubramanianHNSchechtmanKBHamilosDLA retrospective analysis of treatment outcomes and time to relapse after intensive medical treatment for chronic sinusitisAm J Rhinol200216630331212512904
- LalDSciannaJMStankiewiczJAEfficacy of targeted medical therapy in chronic rhinosinusitis, and predictors of failureAm J Rhinol Allergy200923439640019671254
- ToscaMACosentinoCPallestriniEMedical treatment reverses cytokine pattern in allergic and nonallergic chronic rhinosinusitis in asthmatic childrenPediatr Allergy Immunol200314323824112787306
- RupaVJacobMMathewsMSSeshadriMSA prospective, randomized, placebo-controlled trial of postoperative oral steroid in allergic fungal sinusitisEur Arch Otorhinolaryngol2010267223323819714349
- IkramMAbbasASuhailAOnaliMAAkhtarSIqbalMManagement of allergic fungal sinusitis with postoperative oral and nasal steroids: a controlled studyEar Nose Throat J2009884E8E1119358119
- LandsbergRSegevYDeRoweALandauTKhafifAFlissDMSystemic corticosteroids for allergic fungal rhinosinusitis and chronic rhinosinusitis with nasal polyposis: a comparative studyOtolaryngol Head Neck Surg2007136225225717275549
- PoetkerDMRehDDA comprehensive review of the adverse effects of systemic corticosteroidsOtolaryngol Clin North Am201043475376820599080
- LegentFBordurePBeauvillainCBerchePA double-blind comparison of ciprofloxacin and amoxycillin/clavulanic acid in the treatment of chronic sinusitisChemotherapy199440Suppl 18157805431
- NamyslowskiGMisiolekMCzeciorEComparison of the efficacy and tolerability of amoxycillin/clavulanic acid 875 mg bid with cefuroxime 500 mg bid in the treatment of chronic and acute exacerbation of chronic sinusitis in adultsJ Chemother200214550851712462431
- AnonJBJacobsMRPooleMDAntimicrobial treatment guidelines for acute bacterial rhinosinusitisOtolaryngol Head Neck Surg2004130Suppl 114514726904
- GenowayKAPhilpottCMJaverARPathogen yield and antimicrobial resistance patterns of chronic rhinosinusitis patients presenting to a tertiary rhinology centreJ Otolaryngol Head Neck Surg201140323223721518646
- BhattacharyyaNKepnesLJAssessment of trends in antimicrobial resistance in chronic rhinosinusitisAnn Otol Rhinol Laryngol2008117644845218646442
- KingdomTTSwainREJrThe microbiology and antimicrobial resistance patterns in chronic rhinosinusitisAm J Otolaryngol200425532332815334396
- NagaiHShishidoHYonedaRYamaguchiETamuraAKurashimaALong-term low-dose administration of erythromycin to patients with diffuse panbronchiolitisRespiration1991583–41451491745845
- WallworkBComanWMackay-SimAGreiffLCervinAA double-blind, randomized, placebo-controlled trial of macrolide in the treatment of chronic rhinosinusitisLaryngoscope2006116218919316467702
- VidelerWJBadiaLHarveyRJLack of efficacy of long-term, low-dose azithromycin in chronic rhinosinusitis: a randomized controlled trialAllergy201166111457146821884529
- HarunaSShimadaCOzawaMFukamiSMoriyamaHA study of poor responders for long-term, low-dose macrolide administration for chronic sinusitisRhinology2009471667119382498
- SuzukiHIkedaKHonmaRPrognostic factors of chronic rhinosinusitis under long-term low-dose macrolide therapyORL J Otorhinolaryngol Relat Spec200062312112710810255
- Malhotra-KumarSLammensCCoenenSVan HerckKGoossensHEffect of azithromycin and clarithromycin therapy on pharyngeal carriage of macrolide-resistant streptococci in healthy volunteers: a randomized, double-blind, placebo-controlled studyLancet2007369956048249017292768
- PonikauJUSherrisDAWeaverAKitaHTreatment of chronic rhinosinusitis with intranasal amphotericin B: a randomized, placebo-controlled, double-blind pilot trialJ Allergy Clin Immunol2005115112513115637558
- LiangKLSuMCShiaoJYAmphotericin B irrigation for the treatment of chronic rhinosinusitis without nasal polyps: a randomized, placebo-controlled, double-blind studyAm J Rhinol2008221525818284860
- EbbensFAScaddingGKBadiaLAmphotericin B nasal lavages: not a solution for patients with chronic rhinosinusitisJ Allergy Clin Immunol200611851149115617088142
- EbbensFAGeorgalasCLuitenSThe effect of topical amphotericin B on inflammatory markers in patients with chronic rhinosinusitis: a multicenter randomized controlled studyLaryngoscope2009119240140819160404
- SacksPL4thHarveyRJRimmerJGallagherRMSacksRAntifungal therapy in the treatment of chronic rhinosinusitis: a meta-analysisAm J Rhinol Allergy201226214114722487292
- ParnesSMChumaAVAcute effects of antileukotrienes on sinonasal polyposis and sinusitisEar Nose Throat J20007911820 24–2510665187
- NonakaMSakanushiAKusamaKOgiharaNYagiTOne-year evaluation of combined treatment with an intranasal corticosteroid and montelukast for chronic rhinosinusitis associated with asthmaJ Nippon Med Sch2010771212820154454
- MostafaBEAbdel HayHMohammedHEYamaniMRole of leukotriene inhibitors in the postoperative management of nasal polypsORL J Otorhinolaryngol Relat Spec200567314815315925911
- StewartRARamBHamiltonGWeinerJKaneKJMonteleukast as an adjunct to oral and inhaled steroid therapy in chronic nasal polyposisOtolaryngol Head Neck Surg2008139568268718984264
- WiseSKAhnCNSchlosserRJLocalized immunoglobulin E expression in allergic rhinitis and nasal polyposisCurr Opin Otolaryngol Head Neck Surg200917321622219417663
- PintoJMMehtaNDiTineoMWangJBaroodyFMNaclerioRMA randomized, double-blind, placebo-controlled trial of anti-IgE for chronic rhinosinusitisRhinology201048331832421038023
- GevaertPVan BruaeneNCattaertTMepolizumab, a humanized anti-IL-5 mAb, as a treatment option for severe nasal polyposisJ Allergy Clin Immunol2011128598999521958585
- GevaertPLang-LoidoltDLacknerANasal IL-5 levels determine the response to anti-IL-5 treatment in patients with nasal polypsJ Allergy Clin Immunol200611851133114117088140
- ForerBKivitySSadeJLandsbergRAspirin desensitization for ASA triad patients – prospective study of the rhinologist’s perspectiveRhinolog y20114919599
- StevensonDDPleskowWWSimonRAAspirin-sensitive rhinosinusitis asthma: a double-blind crossover study of treatment with aspirinJ Allergy Clin Immunol19847345005076368649
- RozsasiAPolzehlDDeutschleTLong-term treatment with aspirin desensitization: a prospective clinical trial comparing 100 and 300 mg aspirin dailyAllergy20086391228123418699939
- SmithTLBatraPSSeidenAMHannleyMEvidence supporting endoscopic sinus surgery in the management of adult chronic rhinosinusitis: a systematic reviewAm J Rhinol200519653754316402637
- HopkinsCBrowneJ PSlackRThe national comparative audit of surgery for nasal polyposis and chronic rhinosinusitisClin Otolaryngol200631539039817014448
- ChesterACAntisdelJLSindwaniRSymptom-specific outcomes of endoscopic sinus surgery: a systematic reviewOtolaryngol Head Neck Surg2009140563363919393402
- BhandarkarNDMaceJCSmithTLEndoscopic sinus surgery reduces antibiotic utilization in rhinosinusitisInt Forum Allergy Rhinol201111182221666846
- SmithTLKernRCPalmerJNMedical therapy vs surgery for chronic rhinosinusitis: a prospective, multi-institutional studyInt Forum Allergy Rhinol20111423524122287426