
Abstract
Purpose
Candida albicans (C. albicans) candidemia has been well reported in previous studies, while research on non-albicans Candida (NAC) bloodstream infections remains poorly explored. Therefore, the present study aimed to investigate the clinical characteristics and outcomes of patients with NAC candidemia.
Patients and Methods
We recruited inpatients with candidemia from January 2013 to June 2020 in a tertiary hospital for this retrospective observational study.
Results
A total of 301 patients with candidemia were recruited in the current study, including 161 (53.5%) patients with NAC candidemia. The main pathogens in NAC candidemia were Candida tropicalis (C. tropicalis) (23.9%), Candida parapsilosis (15.6%) and Candida glabrata (10.3%). Patients with NAC candidemia had more medical admissions (P=0.034), a higher percentage of hematological malignancies (P=0.007), a higher frequency of antifungal exposure (P=0.012), and more indwelling peripherally inserted central catheters (P=0.002) than those with C. albicans candidemia. In a multivariable analysis, prior antifungal exposure was independently related to NAC candidemia (adjusted odds ratio [aOR], 0.312; 95% confidence interval [CI], 0.113–0.859). Additionally, NAC was obviously resistant to azoles, especially C. tropicalis had a high cross-resistance to azoles. However, no significant differences were noted in the mortality rates at 14 days, 28 days and 60 days between these two groups.
Conclusion
NAC is dominant in candidemia, and prior antifungal exposure is an independent risk factor. Of note, although the outcomes of NAC and C. albicans candidemia are similar, drug resistance to specific azoles as well as cross-resistance frequently occurs in patients with NAC candidemia, and this drug resistance deserves attention in clinical practice and further in-depth investigation.
Introduction
With the wide usage of antibiotics, immunosuppressive agents and glucocorticoids, candidemia has become common as a bloodstream infection (BSI). It often occurs in patients receiving complex surgery, organ transplantation, intravascular catheters, and total parenteral nutrition (TPN), and in patients who have hematologic malignancies or who are in the intensive care unit (ICU).Citation1,Citation2 The prevalence of candidemia varies in different regions,Citation1,Citation3,Citation4 ranging from a relatively low occurrence of 0.32/1000 admissions in Southwest China to a high incidence of 2.49/1000 admissions in Brazil.Citation3,Citation4 Although a rapid diagnosis and timely treatment have been developed, the mortality of invasive candidemia is still relatively high, ranging from 22% to 75%.Citation2,Citation5,Citation6
The most common pathogen causing candidemia is Candida albicans (C. albicans), but epidemiological investigations in recent years have shown that the incidence of non-albicans Candida (NAC) in candidemia is increasing year by year and is mainly composed of Candida tropicalis (C. tropicalis), Candida parapsilosis (C. parapsilosis) and Candida glabrata (C. glabrata).Citation5 In addition, C. albicans is highly sensitive to commonly used clinically antifungal drugs, while the drug resistance seen in NAC is steadily increasing.Citation7,Citation8 Especially, two NAC species (spp.), C. glabrata and C. tropicalis, have demonstrated a higher drug resistance to azoles than other Candida spp.Citation7 Patients with NAC candidemia generally are more likely to have neutropenia and are more likely to have received TPN, glucocorticoids and central venous catheters (CVCs), whereas patients with C. albicans candidemia are more likely to have indwelling urethral catheters, are more likely to have candiduria and are more likely to be admitted to the ICU.Citation9–Citation11
In previous studies, some differences have been reported between C. albicans and NAC candidemia with regard to the clinical characteristics and prognostic factors.Citation7–Citation11 However, several limitations are shown as follows: (1) One study identified that the presence of a urethral catheter was an independent risk factor for C. albicans candidemia,Citation10 and glucocorticosteroids and CVC were independent risk factors for NAC candidemia in another study.Citation11 However, whether these clinical features are significantly different between these two groups remains unclear. (2) A previous study found that patients with C. albicans candidemia had a higher rate of ICU hospitalization, but there was no significant difference in the hospital mortality;Citation9 This result was completely contrary to another study (there was no difference in the ICU hospitalization rate, but there was a higher mortality rate for NAC candidemia).Citation10 Therefore, whether the clinical outcomes of NAC candidemia are better or worse than those of C. albicans candidemia remains unclear. (3) Although the distribution and antifungal resistance of Candida spp. have been well reported in a multicenter large-scale study by China CHIF-NET, more information about the demographic and clinical characteristics is still lacking, and this information is needed to draw valid conclusions.Citation8
Based on the previous results and controversies described above, we hypothesized that patients with NAC candidemia might have some specific risk factors, a more severe situation of drug resistence like azole and a worse prognosis than those with C. albicans candidemia. To address this hypothesis, we attempted to analyze the clinical features, strain distribution, antifungal resistance and prognosis of NAC candidemia compared with C. albicans candidemia in the current study.
Patients and Methods
Study Design and Patients
The present single-center retrospective study was carried out in a tertiary medical teaching hospital, the Second Affiliated Hospital, Zhejiang University School of Medicine, China. The Ethics Committee of the Second Affiliated Hospital, Zhejiang University School of Medicine approved this study protocol (No. 2020–744). Due to the retrospective analysis, the Ethics Committee decided to waive the need for informed consent of patients.
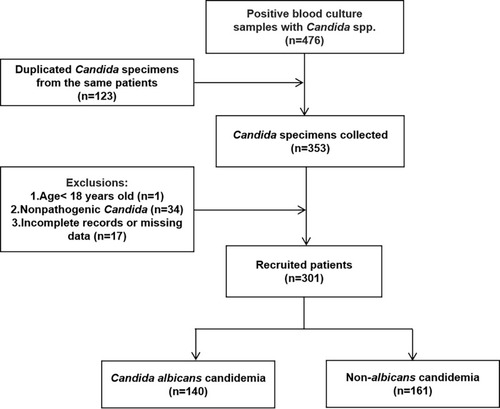
The results of 476 positive blood culture samples from the microbial laboratory between January 2013 and June 2020 were initially analyzed (). Among them, there were 123 duplicated Candida specimens, and any duplicate specimens from the same patient were excluded. Then, we excluded the following patients: 1) age < 18 years old; 2) Candida was considered as nonpathogenic; and 3) the case data were incomplete or missing. Consequently, 52 patients were excluded, including one patient less than 18 years old, 34 patients with nonpathogenic Candida and 17 patients with incomplete or missing data. Finally, 301 patients with candidemia were recruited, with 140 cases and 161 cases of C. albicans candidemia and NAC candidemia, respectively.
Figure 1 Flow diagram of patient recruitment.
Study Variables
The following patients’ medical variables were retrieved from the electronic medical record system, and the variables included basic information such as age, sex, previous medical history, and several assessments [eg, Charlson Comorbidity Index (CCI) score, acute physiology and chronic health evaluation (APACHE) II score and sequential organ failure assessment (SOFA) score within 24 hours after Candida BSI]. Other information, including a history of invasive procedures, previous exposure, previous treatment (eg, chemotherapy drugs, radiotherapy, immunosuppressive agents, surgery, mechanical ventilation), laboratory examinations (eg, blood cells, liver function, and kidney function), and the microbiological data (Candida spp., concomitant bacterial infection or not, antifungal susceptibilities and cross-resistance to azoles in vitro), were also documented. In addition, the main treatments for candidemia, such as fluid resuscitation, vasoactive drugs, renal replacement therapy (RRT) and antifungal drugs, and the outcomes, such as mortality rates at 14 days, 28 days and 60 days, were collected.
Species Identification and Microbiological Assays
Candida spp. identification and drug susceptibility testing were conducted as described in our previous study.Citation12 In brief, blood cultures were drawn under aseptic conditions, and then matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) (Bruker Daltonik GmbH, Bremen, Germany) was used to identify Candida spp. After species confirmation, all of the Candida isolates were subjected to antifungal susceptibility tests using the ATB FUNGUS 3 panel of bioMerieux company in France. Experimental assessments of drug susceptibility for Candida were based on the clinical breakpoints specified by the Clinical Laboratory Standards Institute.Citation13,Citation14
Study Definitions
Candidemia was diagnosed when there was an isolate of at least one species of Candida from the blood cultures accompanied by signs and symptoms of infection. Nonpathogenic candidemia isolates were considered contaminants and were defined as a single positive blood culture of Candida without the clinical manifestations.Citation11 The definition of catheter-related candidemia was on the basis of the Infectious Diseases Society of America and was defined as follows: 1) the isolates from a catheter tip culture was proven to be identical to the isolates in least one percutaneous peripheral blood culture; or 2) the transcatheter and peripheral blood samples cultured the same Candida spp., and met the catheter-related bloodstream infection (CRBSI) criteria.Citation15 The diagnostic criteria for septic shock was based on the definition by Sepsis-3.Citation16 When a blood bacterial culture was positive before or within 48 hours after the onset of candidemia, it was considered a concomitant bacteremia,Citation4 except for the common skin microbiota (eg, Corynebacterium spp., Streptococci, Bacillus spp., Coagulase-negative staphylococci and Lactobacillus spp.), which are possible contaminants. Unless two or more consecutive venipuncture samples cultured the above microorganisms, these isolates were considered pathogens.Citation12,Citation17 The antifungal treatment was considered adequate if: (1) the antifungal agent was administered empirically within the first 48 hours of positive culture; (2) the Candida isolates were sensitive to the selected antifungal drugs on a sensitivity test; and (3) the dosage of antifungal drugs was selected according to the clinical guidelines recommended by the Infectious Diseases Society of America.Citation18,Citation19
Statistical Analysis
All statistical analyses were performed to identify the risk factors for NAC candidemia in comparison with C. albicans candidemia by using the statistical package SPSS 23.0 (IBM Corp, Armonk, NY, USA), and a P<0.05 was considered statistically significant. First, all quantitative data were first tested for normality. If the test results conformed to a normal distribution, the mean±standard deviation was used to represent the continuous variables; otherwise the median and interquartile range (IQR) were used instead. Then, Student’s t-test or the Mann–Whitney U was used for comparison. All enumeration data were represented as N(%), and the chi-square test was used for comparisons between the two groups. In the univariate analysis, the variables with a significant P<0.05 level were considered candidate variables for establishing a stepwise logistic regression multivariate model, which was used to identify the independent risk factors associated with NAC candidemia. The 28-day survival curves of C. albicans and NAC candidemia were depicted by a Kaplan-Meier survival analysis, and the difference was evaluated by the Log rank test.
Results
Patient Characteristics
outlines the baseline characteristics of the recruited patients. The median age of these patients was 66 years (IQR, 53.0–75.5), and 64.1% (193/301) were male. A total of 66.4% (200/301) of all patients with candidemia occurred at an age of older than 60 years old. The proportion of patients over 60 years of age with NAC candidemia was lower than that with C. albicans candidemia (60.9% vs 72.9%, P<0.05). The majority of patients with candidemia were from the ICU (64.5%), followed by surgical wards (20.9%) and medical wards (14.6%), and 91.0% (274/301) of these candidemia cases were nosocomial infections. In terms of comorbidities, gastrointestinal (GI) disease (31.9%), solid tumors (23.6%), and diabetes mellitus (18.3%) were common complications. A lower proportion of diabetes mellitus (13.0% vs 24.5%, P<0.05) and GI diseases (26.1% vs 38.6%, P<0.05) were observed in patients with NAC candidemia, but more hematological malignancies (6.8% vs 0.7%, P<0.05) were observed in patients with NAC candidemia than in patients with C. albicans candidemia. There were no statistically significant differences between the two groups in terms of the CCI score, APACHE II score or SOFA score among all the patients (all P>0.05) (). The percentage of antibiotic exposure before the onset of candidemia was 86.0%, followed by TPN and surgery for more than 50% of the patients. Compared to C. albicans candidemia, patients with NAC candidemia had a lower rate of surgery (47.2% vs 67.9%, P<0.001), especially abdominal surgery (14.3% vs 34.3%, P<0.001). This result was consistent with the fact that most C. albicans candidemia cases were from surgical wards (26.4% vs 16.1%, P<0.05). In contrast, patients with NAC candidemia were more likely to be exposed to antifungal drugs (12,4% vs 4.3%, P<0.05). In addition, more than 70% of patients with candidemia had invasive procedures such as CVCs, urinary catheters, and gastric catheters. Compared with catheterization of patients with C. albicans candidemia, indwelling arterial catheters and CVCs were less common in patients with NAC candidemia (26.7% vs 39.3% and 67.1% vs 84.3%, respectively, both P<0.05), as were indwelling abdominal drainage tubes (13.7% vs 32.1%, P<0.001). However, the presence of a peripherally inserted central catheter (PICC) was more frequent in patients with NAC candidemia (24.8% vs 10.7%, P<0.05).
Table 1 Baseline Characteristics of Patients with C. albicans and NAC Candidemia
Biological Parameters
In terms of biological parameters, patients with NAC candidemia were more likely to have a white blood cell (WBC) count less than 4×109/L (16.8% vs 5.0%, P=0.001), a lower neutrophil count (NC) (median × 109/L, 7.0 vs 8.6), a lower neutrophil to lymphocyte ratio (NLR) (median, 9.2 vs 12.3), and a lower total bilirubin (TB) (median μmol/L, 15.0 vs 18.5) (all P<0.05) compared to patients with C. albicans candidemia ().
Table 2 Biological Parameters of Patients with C. albicans or NAC Candidemia
Independent Risk Factors for NAC Candidemia
Several variables with significant p values in the univariate analysis are described in . After the multivariate regression model analysis of these variables, it was noted that prior antifungal exposure was independently associated with an increased risk of NAC candidemia (adjusted odds ratio [aOR], 0.312; 95% confidence interval [CI], 0.113–0.859). Patients with diabetes mellitus had a higher risk of C. albicans candidemia than NAC candidemia (aOR, 2.267; 95% CI, 1.186–4.334).
Table 3 Multivariable Logistic Regression of Risk Factors Caused by C. albicans vs NAC Candidemia
Species Distribution
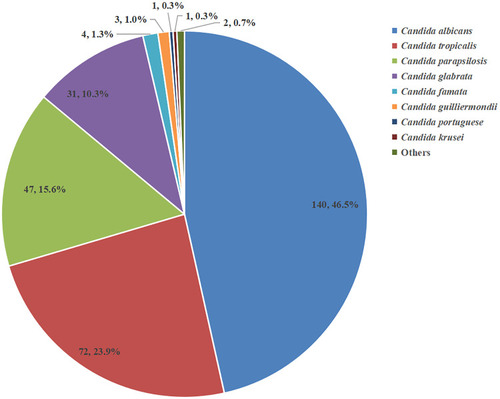
A total of 301 patients with candidemia were recruited in the current study, and C. albicans and NAC were responsible for 46.5% and 53.5% of candidemia cases, respectively. In NAC candidemia, the main species isolated were C. tropicalis, C. parapsilosis and C. glabrata, accounting for 23.9%, 15.6%, and 10.3% of the cases, respectively. In 12 hematological malignancy patients with candidemia, more than 90% of the cases (11/12) were caused by NAC, especially C. tropicalis (10/12, 83.3%). The distribution of Candida spp. is shown in and .
Table 4 Distribution of Candida spp., Cross-Resistance and Prior Antifungal Exposure of Patients with Hematological Malignancy
Figure 2 Distribution of different Candida spp. during this candidemia study period.
In vitro Susceptibilities
As shown in and , NAC isolates had a significantly higher resistance to fluconazole, voriconazole, itraconazole and clotrimazole (all P<0.05). In particularly, C. tropicalis had high resistance rates to clotrimazole (68.6%), itraconazole (45.6%), fluconazole (50.0%), and voriconazole (56.5%), whereas less than 3% of C. albicans isolates were resistant to these four drugs. Both C. albicans and NAC had a low resistance rate (less than 2.0% of isolates) to amphotericin B ().
Table 5 Comparison of Antifungal Susceptibilities of Different Candida spp. in vitro
Table 6 Clinical Features and Treatments of Patients with C. albicans or NAC at the Onset of Candidemia
In general, the resistance rate to ketoconazole (26.6%) was the highest, followed by clotrimazole (23.5%), fluconazole (14.5%), and voriconazole (13.1%) (). In terms of specific azoles, they had different resistance rates which were dependent on the different species of Candida. C. albicans was sensitive to azoles, but this was apparently not the case for NAC, as most of them were resistant to these azoles such as fluconazole, voriconazole and clotrimazole, with a high resistance rate of more than 50% (). Of note, 14.6% (44/301) of patients with candidemia exhibited cross-resistance, especially in patients with C. tropicalis among which the cross-resistance rate to azoles was as high as 50.0% (36/72). Among hematologic malignancy patients with C. tropicalis candidemia, the cross-resistance rate was up to 90% (9/10) ().
Table 7 In vitro Drug Resistance of Candida spp. to Azoles
Clinical Therapy
The details about clinical features and treatments at the onset of candidemia are shown in , which indicated significant differences in RRT, source of infection (intra-abdominal), and antifungal therapy between the two types of candidemia. A total of 10.6% of patients with NAC received RRT, which was almost three times that of patients with C. albicans (P=0.020). The main identified sources of candidemia was catheter-related candidemia (33.2%, 100/301) and intra-abdominal infections (13.0%, 39/301), whereas 42.9% (129/301) of candidemia cases were considered primary infections, as no obvious infection sources were confirmed. In further comparison, patients with NAC candidemia had fewer intraperitoneal sources for candidemia than patients with C. albicans candidemia (9.3% vs 17.1%, P=0.044). In terms of source control, the percentage of catheter removal within 48h in all patients with indwelling intravascular catheters was 73.0% (73/100), although no significant difference was found between these two groups. Regarding adequate antifungal treatment, the ratio of patients with candidemia was similar in both groups (31.7% vs 34.1%, P>0.05). In addition, pyrrole antifungal agents were more commonly used in patients with NAC, while echinocandin antifungal agents were more frequently given to patients with C. albicans ().
Outcomes
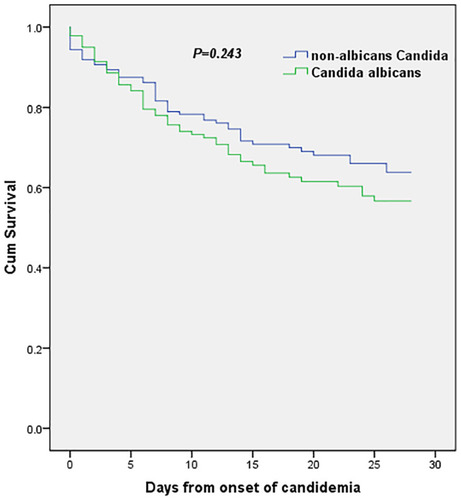
In patients with candidemia, the ICU length of stay was 14 days (IQR, 1.0–38.0), and the total length of hospitalization was 35 days (IQR, 19.3–65.0) (). Patients with NAC candidemia had a longer ICU stay and a longer total hospitalization than those with C. albicans candidemia [median days, 15.0 (0.5–46.0) vs 14.0 (2.0–33.8), P=0.406; 37.5 (20.2–70.0) vs 34.0 (19.0–60.0), P=0.303], but these values were not statistically significant. Furthermore, no significant differences were noted in the mortality rates at 14 days, 28 days and 60 days between these two groups, which was consistent with the result of survival curve ().
Table 8 Outcomes of Patients with C. albicans and NAC Candidemia
Figure 3 Kaplan-Meier estimates of survival in patients with C. albicans candidemia and NAC candidemia.
Discussion
Several findings have been revealed in our current study. First, although C. albicans was reported to be the major fungal species, NAC spp. accounted for 53.5% (161/301) of candidemia. Second, several risk factors for NAC candidemia were found, including medical admission, hematological malignancies, prior antifungal exposure, and the presence of PICC. Particularly, prior antifungal exposure constituted one of the most pivotal independent risk factors for NAC candidemia, which differed from that of diabetes mellitus for C. albicans candidemia. Moreover, C. albicans remained highly susceptible to most antifungal agents (including azoles), whereas NAC showed strikingly different responses to azoles, especially C. tropicalis, which had a high cross-resistance to azoles. Lastly, no significant differences in the clinical outcomes were observed between these two groups.
To date, numerous studies have specifically described the epidemiology of candidemia based on demographic surveys from around the world.Citation7–Citation11,Citation20–Citation22 As expected, the four major pathogens of candidemia were C. albicans, C. tropicalis, C. glabrata and C. parapsilosis, which accounted for 96.3% of all Candida spp. in this study (). NAC spp. collectively represented 53.5% of the bloodstream isolates, which exceeded the percent of C. albicans spp., and these results are consistent with the results from Northeast China, Latin America, North America and Asia-Pacific.Citation7,Citation10,Citation23 Concerning NAC candidemia, it is worth noting that C. tropicalis has become a common NAC spp. worldwide.Citation7,Citation8 In our study, C. tropicalis ranked second among all Candida spp. in candidemia, accounting for 23.9%. This rate was lower than the rate in Asia-Pacific (30.7%), but higher than that in Northeast China (10%), Latin America (17.0%), North America (8.0%) and Europe (7.5%).Citation7,Citation10,Citation23 The epidemiological difference in species for candidemia might vary with patient age, geographical area, medical practice and use of antifungal drugs.Citation1 The prevalence of NAC candidemia has significantly increased over time, which is generally associated with a reduced antifungal sensitivity resulting from the widespread use of azoles.Citation7,Citation8,Citation24,Citation25 Other possible explanations may include the increased number of immunocompromised patients, the growing use of invasive medical procedures, and the improvement of yeast isolation techniques at the species level.Citation1,Citation11,Citation22 However, the underlying mechanisms causing the epidemiological changes of NAC spp. in candidemia remain uncertain.
Common risk factors for NAC candidemia consisted of medical admissions, hematological malignancies, antifungal exposure, and the presence of PICC (). Other studies have found that hematological malignancies and prior exposure to antifungal agents were factors closely related to NAC candidemia in comparison with C. albicans candidemia,Citation26–Citation29 which echoes our study. Among hematological malignancy patients with candidemia, NAC was the main type, in which C. tropicalis accounted for 90.9% (10/11) (). Other studies also showed that C. tropicalis was the most common NAC spp. in hematological malignancy patients complicated with candidemia.Citation27,Citation30 This peculiar epidemiology might be explained by the increased invasiveness of C. tropicalis in the human gastrointestinal tract, especially in patients with hematological malignancies who are immunocompromised.Citation31 Furthermore, a high proportion of antifungal exposure before the onset of candidemia (36.4%) was observed in hematological malignancy patients with NAC candidemia, which might be partly responsible for the species’ migration to NAC. However, hematological malignancy was not independently associated with NAC candidemia after the multivariate regression analysis (), possibly due to the low proportion of these patients in our study (6.8%) (). Of note, when these risk factors were further analyzed using the multivariate regression, prior antifungal exposure was independently associated with an increased risk of NAC candidemia, while diabetes mellitus was associated with an increased risk of C. albicans candidemia (). However, it remains unknown whether patients with both risk factors, diabetes and prior antifungal exposure, are likely to develop mixed BSIs of C. albicans and NAC, which merits further investigation.
Over the past 20 years, the drug resistance of Candida to azoles has attracted worldwide attention. Although azoles show preliminary clinical benefits in C. albicans candidemia,Citation7,Citation8 the increasing prevalence of NAC spp. and their associated reduced antifungal sensitivity have become a main challenge in candidemia treatment.Citation20,Citation22,Citation25 In the current study, NAC demonstrated significantly higher resistance to fluconazole, voriconazole, itraconazole and clotrimazole (all P<0.05), especially with C. tropicalis isolates ( and ). We observed that the rate of azole resistance in C. tropicalis was over 35%, which was consistent with the high resistance rate in the CHIF-NET study;Citation8 Furthermore, 50% (36/72) of C. tropicalis isolates had cross-resistance to azoles. A striking result of this study was that the cross-resistance rate of C. tropicalis to azoles in hematological malignancy patients with candidemia was up to 90% (). Globally, the resistance to azoles in C. tropicalis mainly occurs in the Asia-Pacific region, while it is still low (less than 10%) in European and American countries.Citation7,Citation8,Citation23 Previous works have reported several variables that might contribute to high azole resistance among NAC, such as prior exposure to antifungal drugs (especially azoles) or antibiotics, the duration of prior drug exposure or inappropriate dosing.Citation30,Citation32 Moreover, Fan et alCitation33 showed that one explanation of the azole resistance in C. tropicalis isolates was the ERG11 missense mutations. Since C. tropicalis candidemia has been reported to have a higher mortality and a poor prognosis,Citation34 we should highlight the importance of monitoring antifungal drug resistance in C. tropicalis infections. Additionally, echinocandins might be used as an initial treatment for patients who have some risk factors for NAC candidemia, according to the clinical guidelines recommended by the Infectious Diseases Society of America.Citation19
In view of the high incidence of Candida and the high resistance of antifungal agents, it is important to develop new antifungal agents. In recent years, several studies have found that natural compounds have efficacy against Candida.Citation35–Citation38 Some essential oils extracted from plants have displayed inhibitory effects on the growth and activity of common Candida isolates.Citation35,Citation36,Citation38 UOST5-NPS, a novel anticandidal azole agent based on essential oils, has been developed for the newly emerged Candida auris.Citation37 In addition, amphotericin B combined with Ruta graveolens essential oil has also shown synergistic effects against C. albicans and C. tropicalis in vitro.Citation36 These results suggest that these natural compounds might provide a new promising strategy against Candida infection in the future.
Although some studies have reported worse outcomes for NAC candidemia in comparison with C. albicans candidemia,Citation10,Citation11 few significant differences were observed between these two groups in our current study. (, ). This might be partly due to the similar disease severity, similar baseline comorbidities (), and similar clinical treatments at the onset of candidemia () between the two groups.
Notably, some limitations exist in the current study. First, our results were mainly from a single-center study; therefore, they may not represent the trends in the other regions of China. Nevertheless, these data could be used as a reference. Second, although a positive blood sample culture is the gold standard in the diagnosis of candidemia, many patients do not have a positive blood culture result due to its poor sensitivity. Thus, the diagnosis of candidemia might be underestimated. Finally, echinocandins were not included in the drug sensitivity tests in this study, as we could not detect the sensitivity to echinocandins. According to the CHIF-NET study, Candida spp. were highly sensitive to echinocandins in vitro.Citation8
Conclusion
Together, we have revealed that NACs are dominant in candidemia in our current study. Several factors, including medical admissions, hematological malignancies, antifungal exposure, and the presence of PICC, are closely related to NAC candidemia, whereas prior antifungal exposure is an independent risk factor. Of note, although the outcomes of NAC and C. albicans candidemia are similar, drug resistance to specific azoles as well as cross-resistance frequently occurs in patients with NAC candidemia (especially C. tropicalis), and this deserves further evaluation in clinical practice and further in-depth investigations.
Abbreviations
C. albicans, Candida albicans; NAC, non-albicans Candida; C. parapsilosis, Candida parapsilosis; C. tropicalis, Candida tropicalis; C. glabrata, Candida glabrata; spp., species; BSI, bloodstream infection; IQR, interquartile range; ICU, intensive care unit; CCI, Charlson Comorbidity Index; APACHE, acute physiology and chronic health evaluation; SOFA, sequential organ failure assessment; CRBSI, catheter-related bloodstream infection; GI, gastrointestinal; TPN, total parenteral nutrition; CVC, central venous catheter; PICC, peripherally inserted central catheter; WBC, white blood count; NC, neutrophil count; LC, lymphocyte count; NLR, neutrophil to lymphocyte ratio; TB, total bilirubin; AST, aspartate aminotransferase; ALT, alanine aminotransferase; PCT, procalcitonin; OR, odds ratio; CI, confidence interval; S, susceptible; I, intermediate; R, resistant; RRT, renal replacement therapy.
Data Sharing Statement
All data generated and/or analyzed during the current study are included in this manuscript.
Ethics Approval and Informed Consent
This study received human research ethics approval (NO. 2020-744) from the Ethics Committee of the Second Affiliated Hospital, Zhejiang University School of Medicine. We ensure the confidentiality of patient data and comply with the Helsinki statement. Due to the retrospective nature of the study, the Ethics Committee determined that no patient consent was required.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
- PfallerMA, DiekemaDJ. Epidemiology of invasive candidiasis: a persistent public health problem. Clin Microbiol Rev. 2007;20(1):133–163. doi:10.1128/CMR.00029-0617223626
- LauschKR, SøgaardM, RosenvingeFS, et al. High incidence of candidaemia in a nationwide cohort: underlying diseases, risk factors and mortality. Int J Infect Dis. 2018;76:58–63. doi:10.1016/j.ijid.2018.08.01030176293
- ColomboAL, NucciM, ParkBJ, et al. Epidemiology of candidemia in Brazil: a nationwide sentinel surveillance of candidemia in eleven medical centers. J Clin Microbiol. 2006;44(8):2816–2823. doi:10.1128/JCM.00773-0616891497
- JiaX, LiC, CaoJ, WuX, ZhangL. Clinical characteristics and predictors of mortality in patients with candidemia: a Six-Year Retrospective Study. Eur J Clin Microbiol. 2018;37(9):1717–1724. doi:10.1007/s10096-018-3304-9
- CuervoG, Garcia-VidalC, Puig-AsensioM, et al. Usefulness of guideline recommendations for prognosis in patients with candidemia. Med Mycol. 2019;57(6):659–667. doi:10.1093/mmy/myy11830418567
- LeeRA, ZurkoJC, CaminsBC, et al. Impact of infectious disease consultation on clinical management and mortality in patients with candidemia. Clin Infect Dis. 2019;68(9):1585–1587. doi:10.1093/cid/ciy84930281081
- PfallerMA, DiekemaDJ, TurnidgeJD, CastanheiraM, JonesRN. Twenty years of the SENTRY antifungal surveillance program: results for candida species from 1997–2016. Open Forum Infect Dis. 2019;6(Suppl 1):S79–S94. doi:10.1093/ofid/ofy35830895218
- XiaoM, ChenSC, KongF, et al. Distribution and antifungal susceptibility of candida species causing candidemia in china: an update from the CHIF-NET Study. J Infect Dis. 2020;221(Suppl 2):S139–S147. doi:10.1093/infdis/jiz57332176789
- ChiH, YangY, ShangS, et al. Candida albicans versus non-albicans bloodstream infections: the comparison of risk factors and outcome. J Microbiol Immunol Infect. 2011;44(5):369–375. doi:10.1016/j.jmii.2010.08.01021524971
- ZhangW, SongX, WuH, ZhengR. Epidemiology, risk factors and outcomes of Candida albicans vs. non- albicans candidaemia in adult patients in Northeast China. Epidemiol Infect. 2019;147:e277–e277. doi:10.1017/s095026881900163831552814
- DimopoulosG, NtzioraF, RachiotisG, ArmaganidisA, FalagasME. Candida albicans versus non-albicans intensive care unit-acquired bloodstream infections: differences in risk factors and outcome. Anesth Analg. 2008;106(2):523–529. doi:10.1213/ane.0b013e318160726218227310
- ZhongL, ZhangS, TangK, et al. Clinical characteristics, risk factors and outcomes of mixed Candida albicans/bacterial bloodstream infections. Bmc Infect Dis. 2020;20(1):1–810. doi:10.1186/s12879-020-05536-z
- Clinical and Laboratory Standards Institute. M27-A3. Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeasts, Approved Standard. 3rd ed. Wayne, PA: CLSI; 2008.
- Clinical and Laboratory Standards Institute. M60. Performance Standards for Antifungal Susceptibility Testing of Yeasts. 1st ed. Wayne, PA: CLSI; 2018.
- MermelLA, AllonM, BouzaE, et al. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 update by the infectious diseases society of America. Clin Infect Dis. 2009;49(1):1–45. doi:10.1086/59937619489710
- SeymourCW, LiuVX, IwashynaTJ, et al. Assessment of clinical criteria for sepsis. JAMA. 2016;315(8):762. doi:10.1001/jama.2016.028826903335
- KimSH, YoonYK, KimMJ, SohnJW. Risk factors for and clinical implications of mixed Candida/bacterial bloodstream infections. Clin Microbiol Infect. 2013;19(1):62–68. doi:10.1111/j.1469-0691.2012.03906.x22651822
- Garnacho-MonteroJ, Diaz-MartinA, Garcia-CabreraE, Ruiz Perez de PipaonM, Hernandez-CaballeroC, Lepe-JimenezJA. Impact on hospital mortality of catheter removal and adequate antifungal therapy in Candida spp. bloodstream infections. J Antimicrob Chemother. 2012;68(1):206–213. doi:10.1093/jac/dks34722945914
- PappasPG, KauffmanCA, AndesDR, et al. Clinical practice guideline for the management of candidiasis: 2016 update by the infectious diseases society of America. Clin Infect Dis. 2016;62(4):e1–e50. doi:10.1093/cid/civ93326679628
- LamothF, LockhartSR, BerkowEL, CalandraT. Changes in the epidemiological landscape of invasive candidiasis. J Antimicrob Chemother. 2018;73(suppl 1):i4–i13. doi:10.1093/jac/dkx44429304207
- SongY, ChenX, YanY, WanZ, LiuW, LiR. Prevalence and antifungal susceptibility of pathogenic yeasts in china: a 10-Year Retrospective Study in a teaching hospital. Front Microbiol. 2020;11:1410. doi:10.3389/fmicb.2020.0140132670247
- PappasPG, LionakisMS, ArendrupMC, Ostrosky-ZeichnerL, KullbergBJ. Invasive candidiasis. Nat Rev Dis Primers. 2018;4(1):18026. doi:10.1038/nrdp.2018.2629749387
- TanTY, HsuLY, AlejandriaMM, et al. Antifungal susceptibility of invasive Candida bloodstream isolates from the Asia-Pacific region. Med Mycol. 2016;54(5):471–477. doi:10.1093/mmy/myv11426868904
- EnochDA, YangH, AliyuSH, MicallefC. The changing epidemiology of invasive fungal infections. Methods Mol Biol. 2017;1508:17–65. doi:10.1007/978-1-4939-6515-1_227837497
- PerlinDS, Rautemaa-RichardsonR, Alastruey-IzquierdoA. The global problem of antifungal resistance: prevalence, mechanisms, and management. Lancet Infect Dis. 2017;17(12):e383–e392. doi:10.1016/S1473-3099(17)30316-X28774698
- ApisarnthanarakA, NaknarongkijN, KiratisinP, MundyLM. Risk factors and outcomes of Candida albicans and non-albicans Candida species at a Thai tertiary care center. Am J Infect Control. 2009;37(9):781–782. doi:10.1016/j.ajic.2009.04.28919874981
- VigourouxS, MorinO, MoreauP, HarousseauJL, MilpiedN. Candidemia in patients with hematologic malignancies: analysis of 7 years’ experience in a single center. Haematologica. 2006;91(5):717–718.16670081
- HornDL, NeofytosD, AnaissieEJ, et al. Epidemiology and outcomes of candidemia in 2019 patients: data from the prospective antifungal therapy alliance registry. Clin Infect Dis. 2009;48(12):1695–1703. doi:10.1086/59903919441981
- ViscoliC, GirmeniaC, MarinusA, et al. Candidemia in cancer patients: a prospective, multicenter surveillance study by the Invasive Fungal Infection Group (IFIG) of the European Organization for Research and Treatment of Cancer (EORTC). Clin Infect Dis. 1999;28(5):1071–1079. doi:10.1086/51473110452637
- ChenXC, XuJ, WuDP. Clinical characteristics and outcomes of breakthrough candidemia in 71 hematologic malignancy patients and/or allogeneic hematopoietic stem cell transplant recipients: a Single-Center Retrospective Study from China, 2011–2018. Clin Infect Dis. 2020;71(Suppl4):S394–S399. doi:10.1093/cid/ciaa152333367573
- WalshTJ, MerzWG. Pathologic features in the human alimentary tract associated with invasiveness of Candida tropicalis. Am J Clin Pathol. 1986;85(4):498–502. doi:10.1093/ajcp/85.4.4983953503
- Ben-AmiR, Olshtain-PopsK, KriegerM, et al. Antibiotic exposure as a risk factor for fluconazole-resistant Candida bloodstream infection. Antimicrob Agents Chemother. 2012;56(5):2518–2523. doi:10.1128/AAC.05947-1122314534
- FanX, XiaoM, ZhangD, et al. Molecular mechanisms of azole resistance in Candida tropicalis isolates causing invasive candidiasis in China. Clin Microbiol Infect. 2019;25(7):885–891. doi:10.1016/j.cmi.2018.11.00730472420
- AndesDR, SafdarN, BaddleyJW, et al. Impact of treatment strategy on outcomes in patients with candidemia and other forms of invasive candidiasis: a patient-level quantitative review of randomized trials. Clin Infect Dis. 2012;54(8):1110–1122. doi:10.1093/cid/cis02122412055
- DonaduMG, UsaiD, MarchettiM, et al. Antifungal activity of oils macerates of North Sardinia plants against Candida species isolated from clinical patients with candidiasis. Nat Prod Res. 2020;34(22):3280–3284. doi:10.1080/14786419.2018.155717530676066
- DonaduMG, Peralta-RuizY, UsaiD, et al. Colombian essential oil of ruta graveolens against nosocomial antifungal resistant candida strains. J Fungi (Basel). 2021;7(5):383. doi:10.3390/jof705038334069001
- HamdyR, FayedB, HamodaAM, Rawas-QalajiM, HaiderM, SolimanSSM. Essential oil-based design and development of novel anti-candida azoles formulation. Molecules. 2020;25(6):1463. doi:10.3390/molecules25061463
- BonaE, CantamessaS, PavanM, et al. Sensitivity of Candida albicans to essential oils: are they an alternative to antifungal agents?J Appl Microbiol. 2016;121(6):1530–1545. doi:10.1111/jam.1328227568869