
Abstract
Purpose
The purpose of this study was to examine the prevalence of four important drug-resistance phenotypes: difficult-to-treat resistance (DTR), fluoroquinolone resistance (FQR), carbapenem resistance (CR), and extended-spectrum cephalosporin resistance (ECR).
Methods
DTR was defined as insensitivity to all the β-lactams and fluoroquinolones tested. We retrospectively analyzed the distribution characteristics of specific drug-resistant phenotypes of the main Gram-negative bacteria causing bloodstream infections (BSIs) in Tongji Hospital (Wuhan, China) between 2013 and 2021: Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa, and Acinetobacter baumannii.
Results
FQR was the main antimicrobial resistance phenotype of E. coli, accounting for 59.45% (1117/1879, 95% confidence interval, 57.21%–61.65%); the detection rates for CR and DTR were low, accounting for 1.86% (35/1879, 1.34%–2.58%), and 1.81% (34/1879, 1.30%–2.52%), respectively. However, the detection rates for CR and DTR in K. pneumoniae were 38.83% (497/1280, 36.20%–41.53%) and 35.94% (460/1280, 33.35%–38.60%), respectively. In P. aeruginosa, the detection rates of the four drug-resistant phenotypes (DTR, CR, FQR, and ECR) were all < 30%, but conversely, for A. baumannii, the detection rates were all > 80%. The changes in the data from 2013 to 2021 showed upward trends (z > 0) for CR-E. coli, DTR-E. coli, FQR-E. coli, CR-K. pneumoniae, DTR-K. pneumoniae, FQR-K. pneumoniae, and ECR-K. pneumoniae, but downward trends (z < 0) for ECR-E. coli, CR-A. baumannii, DTR-A. baumannii, FQR-A. baumannii, ECR-A. baumannii, CR-P. aeruginosa, DTR-P. aeruginosa, FQR-P. aeruginosa, and ECR-P. aeruginosa.
Conclusion
DTR warrants further attention, especially in in BSI-associated K. pneumoniae and A. baumannii, in which the detection rates were very high. Between 2013 and 2021 in this region, DTR-E. coli and CR-E. coli showed obvious upward trends, whereas DTR-P. aeruginosa and ECR-P. aeruginosa showed obvious downward trends.
Introduction
The invention of antibiotics is an important milestone in the development of modern medical science. However, the emergence of antimicrobial resistance (AMR) has seriously threatened human health. It is reported that about 23,000 and 25,000 people die each year from infections complicated by AMR in the United States and Europe, respectively.Citation1 Consequently, AMR is a very noteworthy focus of research throughout the world.
To better monitor AMR, in 2008, the European Centre for Disease Prevention and Control (ECDC) and the USA Centers for Disease Control and Prevention (CDC) jointly launched the concepts of multidrug resistance (MDR), extensive drug resistance (XDR), and pandrug resistance (PDR) to describe different drug resistance phenotypes. MDR was defined as simultaneous insensitivity to three types of antibiotics. XDR was defined as sensitivity to only one or two antibiotics. PDR was defined as nonsusceptibility to all antibiotics tested.Citation2 Although these concepts have some epidemiological value, several experts suggest that they ignore the toxicity and efficiency of antibiotics, and that their correlations with clinical outcomes are questionable.Citation3 In 2018, Kadri et al proposed a new concept with which to monitor AMR among Gram-negative bacteria, difficult-to-treat resistance (DTR), which was defined as intermediate or resistance to all first-line agents, including β-lactams and fluoroquinolones.Citation4,Citation5 However, there have been very few reports of DTR around the world outside the United States and South Korea. Therefore, we retrospectively analyzed the distribution of DTR, CR, ECR, and FQR in four common Gram-negative bacteria causing bloodstream infections (BSIs), Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa, and Acinetobacter baumannii, in our hospital between 2013 and 2021, to provide some epidemiological references for decision making about clinical treatment and infection control.
Methods
Data Source
All pathogenic microorganisms were isolated from blood-culture-positive samples at Tongji Hospital (Wuhan, China) between 2013 and 2021. In this retrospective study, the four commonest Gram-negative bacteria causing BSIs at our center, E. coli, K. pneumoniae, A. baumannii, and P. aeruginosa, were analyzed. The identification and antimicrobial sensitivity testing of the strains were performed in the microbiology laboratory of Tongji Hospital. Automated blood culture instruments, including the BD BACTECTM FX 400 (BD Co., NJ, USA) or the BacT/ALERT® 3D Microbial Detection System (bioMérieux, Lyon, France), were used in the microbiology laboratory. The strains were identified with an automatic identification system (VITEK® 2 Compact, bioMérieux) and/or MALDI Biotyper® sirius IVD System (Bruker, Antu, China). Antimicrobial susceptibility testing was performed in the final year with the disk diffusion method according to the Clinical and Laboratory Standards Institute (CLSI) guidelines. Resistance to carbapenems, including imipenem and meropenem, was screened with the disk diffusion method and confirmed with the E-test method.
Definition of Specific Antimicrobial Resistance Phenotypes
In this study, DTR was defined as resistance or intermediate resistance in vitro to all β-lactam categories, including carbapenems and fluoroquinolones.Citation4,Citation5 Carbapenem resistance (CR) was defined as resistance in vitro to imipenem and meropenem. Extended-spectrum cephalosporin resistance (ECR) was defined as resistance in vitro to ceftazidime, cefotaxime, and cefepime. Fluoroquinolone resistance (FQR) was defined as resistance in vitro to ciprofloxacin and levofloxacin.Citation6
Statistical Analysis
Data from the drug sensitivity experiments were analyzed using the WHONET 5.6 software. When multiple specimens were collected from the same patient simultaneously, only the first isolate of a given species from that patient was analyzed according to CLSI M-39.Citation7 The interpretation criteria for the antimicrobial susceptibility results were based on the CLSI 2020 guidelines.Citation8 The changing trends in the detection rates of specific drug resistance phenotypes were analyzed with the Mann–Kendall test, with the R 4.0.2 program (R Core Team). z < 0 indicated a downward trend, whereas z > 0 indicated an upward trend. P < 0.05 indicated statistical significance.
Ethics Approval and Consent to Participate
The study protocol was approved by the Tongji Hospital Ethics Committee for Research in Health. The committee also approved a waiver for informed consent to participate in this study given its retrospective design. All patient data were anonymized before analysis.
Results
Detection Rates of Specific Antimicrobial Resistance Phenotypes
For E. coli, FQR was the main drug resistance phenotype, accounting for 59.45% (1117/1879, 95% confidence interval, 57.21%–61.65%) of phenotypes detected, followed by ECR, accounting for 31.08% (584/1879, 29.03%–33.21%), whereas CR and DTR accounted for 1.86% (35/1879, 1.34%-–2.58%) and 1.81% (34/1879, 1.30%–2.52%) respectively. For K. pneumoniae, the detection rates for ECR, FQR, CR, and DTR were 50% (640/1280, 47.26%–52.74%), 48.13% (616/1280, 45.40%–50.86%), 38.83% (497/1280, 36.20%–41.53%), and 35.94% (460/1280, 33.35%–38.60%), respectively. For P. aeruginosa, the detection rates for ECR, FQR, CR and DTR were all < 30%, at 16.76% (59/352, 13.22%–21.02%), 18.18% (64/352, 14.50%–22.55%), 26.99% (95/352, 22.62%–31.86%), and 11.36% (40/352, 8.46%–15.10%), respectively. For A. baumannii, the detection rates for ECR, FQR, CR, and DTR were all > 80%, at 85.52% (384/449, 81.97%–88.48%), 83.96% (377/449, 80.28%–87.07%), 84.41% (379/449, 80.76%–87.47%), and 83.30% (374/449, 79.57%–86.46%), respectively.
Trends in Specific Drug Resistance Phenotypes
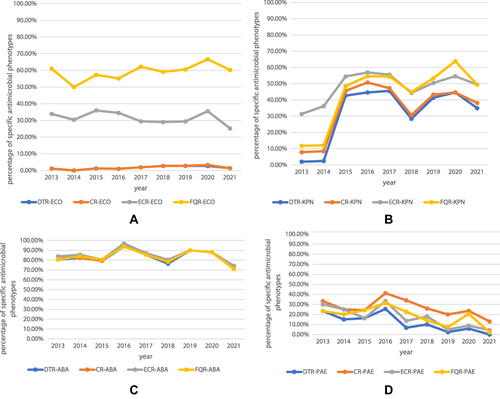
In E. coli, the detection rate of FQR ranged from 50% to 70% from 2013 to 2021; the detection rate for ECR ranged from 20% to 40%; and the detection rates for CR and DTR were < 5% (). In K. pneumoniae, DTR, CR, ECR, and FQR increased significantly after 2015. The detection rate for DTR was < 3% in 2013 and 2014, but increased from 25% to 50% between 2015 and 2021. The detection rate for CR was < 10% in 2013 and 2014, but increased from 30% to 55% after 2015. The detection rate for FQR was < 15% in 2013 and 2014, but 40%–70% after 2015 (). In A. baumannii, the detection rates for DTR, CR, ECR, and FQR were all > 70% from 2013 to 2021 (). However, the detection rates for the four drug-resistant phenotypes of P. aeruginosa were ≤40%, and showed obvious downward trends after 2019 (). Statistical analysis with the Mann–Kendall test indicated that CR-E. coli and DTR-E. coli showed significant upward trends (z > 0, P < 0.05), whereas DTR-P. aeruginosa and ECR-P. aeruginosa showed significant downward trends (z < 0, P < 0.05; ).
Table 1 Results of Statistical Analysis on the Trend of Specific Drug Resistance Phenotypes
Figure 1 Trends of special antimicrobial resistance phonotypes from 2013 to 2021. ((A), E. coli, (B), K. pneumoniae, (C), A. baumannii, (D), P. aeruginosa).
Discussion
Although MDR, XDR, and PDR are very important concepts in monitoring drug resistance, these classifications do not consider the toxicity or therapeutic efficacy of antimicrobial drugs themselves, and judging whether a strain is XDR or PDR requires that a very wide variety of antimicrobial drugs be tested. The new definition, DTR, focuses on the effect of antimicrobial resistance on treatment decisions and clinical outcomes.Citation5 DTR is a very practical value indicator, and the emergence of DTR indicates that when deciding a clinical treatment, some antibacterial drugs that are less effective and/or more toxic should be considered. DTR is also a public health threat and contributes to the international spread of plasmids, antibiotic overuse, and the need for costly infection control measures in healthcare facilities.Citation4
In this study, we found that DTR was not common in E. coli, but could not be ignored in A. baumannii and K. pneumoniae. According to the epidemic trends in 2013–2021, the specific drug resistance phenotypes of DTR and CR have increased significantly in E. coli, whereas DTR and ECR have clearly decreased in P. aeruginosa.
In our monitoring data, FQR was the most frequent phenotype in E. coli, with a prevalence rate of 59.45%, followed by ECR, with a prevalence rate of 31.08%. The drug resistance of E. coli is consistent with the monitoring data reported in the United States and South Korea, but the prevalence of FQR is significantly higher than that reported in the United States and South Korea (27.3% and 44.1% respectively).Citation4,Citation5 The prevalence rate of ECR was 31.08%, which is similar the 33.1% reported in South Korea, but significantly higher than the 6.4% reported in the United States.Citation4,Citation5 The prevalence rates of E. coli-DTR and E. coli-CR in our study are consistent with those in the United States (0.04% and 0.1%, respectively) and South Korea (1.5% and 0%, respectively).Citation4,Citation5 The resistance rates of E. coli to fluoroquinolones and cephalosporins in our region were higher than those reported in the United States and South Korea, which may be attributable to the extensive use of fluoroquinolones and cephalosporins in our region. Research at a teaching hospital in China showed that from 2010 to 2016, the outpatient prescription rate for fluoroquinolones decreased from 19.38% to 13.21%, and that for inpatients decreased from 64.34% to 34.65%.Citation9 Between 2011 and 2016, the resistance rate of E. coli to levofloxacin decreased from 61.3% to 53.9% and that to ciprofloxacin decreased from 64.3% to 58.2%.Citation9 Therefore, the reduction in E. coli resistance to fluoroquinolones correlated positively with the reduced use of antimicrobial agents. Analogously, the high resistance of E. coli to carbapenems may be related to the overuse of these antimicrobials. A study of the effects of an antimicrobial restriction system to curb the inappropriate use of carbapenem indicated that antimicrobial restriction systems can increase the appropriate prescription of carbapenem antibiotics and effectively reduce the production of carbapenem-resistant bacterial strains.Citation10
In the present study, the prevalence rates of FQR, ECR, CR, and DTR in K. pneumoniae were similar, at 48.13%, 50.00%, 38.83%, and 35.94%, respectively, but were significantly higher than those in the United States (9.7%, 8.9%, 2.1%, and 1.7%, respectively) and South Korea (19.2%, 21.2%, 2.1%, and 1.4%, respectively).Citation4,Citation5 Carbapenemases, extended-spectrum β-lactamases, and AmpC β-lactamases are the main mechanisms of K. pneumoniae resistance to a variety of antibiotics. The high prevalence of CR is mainly responsible for the high prevalence of DTR. CR is prevalent in many countries, but the resistance mechanism of CR differs in different regions. In China, blaKPC-2 is the main carbapenemase producer, whereas blaKPC-16 is most widely distributed in Japan and blaKPC-15 in Singapore.Citation11 IMP-11- and IMP-6- producing CR-K. pneumoniae are most commonly reported in Japan.Citation12 blaOX-48 is mainly distributed in Turkey, but was recently also reported in China, the United States, and several European countries (Spain, France, Germany, and Switzerland).Citation11,Citation12 In a previous study of the CR genotypes in our hospital, blakpc-2 mainly colonized the infected group of patients, accounting for 72.4% of infections, whereas blaNDM-1 mainly colonized the noninfected patient group, accounting for 42.2% of infections.Citation13 The high prevalence of CR-K. pneumoniae in our hospital may be related to the simultaneous expression of multidrug-resistance genes. The mechanism of resistance to carbapenems in K. pneumoniae in this region remains to be clarified.
In this study, the prevalence rates for FQR, ECR, CR, and DTR in A. baumannii were all > 80%, and were significantly higher than those reported in the United States (49.5%, 55.4%, 29.4%, and 18.3%, respectively) and South Korea (65.5%, 70.0%, 63.4%, and 59.4%, respectively).Citation4,Citation5 However, the drug resistance of P. aeruginosa showed a gradual downward trend. The detection rates of FQR, ECR, CR, and DTR were 18.18%, 16.76%, 26.99%, and 11.36%, respectively, whereas the corresponding data reported from the United States were 18.5%, 9.1%, 10.4%, and 2.3%, respectively, and those from South Korea were 33.0%, 28.1%, 28.1%, and 9.0%, respectively.Citation4,Citation5 The high drug resistance rates for A. baumannii may be related to the simultaneous expression of multiple drug resistance mechanisms, such as a change in the antibiotic target, the expression of an efflux pump, the production of various enzymes that hydrolyze antibiotics, and so on.Citation14 A study by Wei Feng indicated that the mutational inactivation of OprD was the main factor responsible for CR-P. aeruginosa.Citation15 The molecular mechanisms of drug resistance in A. baumannii and P. aeruginosa in this region warrant further research.
Clinical experts have been investigating new antimicrobial agents for the treatment of CR-A. baumannii infections. A study by Wasan Katip indicated that a nonloading dose of colistin methane sulfonate increased the opportunity to achieve a favorable outcome, but also increased nephrotoxicity in patients.Citation16 In another study, Wasan Katip demonstrated that the addition of meropenem to colistin reduced the 30-day mortality rate, achieved greater clinical and microbiological responses, and did not increase the nephrotoxicity compared with colistin monotherapy.Citation17 However, colistin plus vancomycin showed no significant differences in the 30-day mortality, clinical response, or microbiological response compared with colistin alone in treating infections of CR-A. baumannii.Citation18
The present study had several limitations. First, the use of a study design in which a tertiary hospital was used as the reference, rather than a geographical design that included all bacterial data from a given population, greatly limited the representativeness of the data. The fact that no information was available on the number of blood cultures taken per year during the study period, on the positivity rates of the blood cultures, or on the patient population of the hospital also limits the generalizability of our findings. Second, the mechanisms of resistance were not investigated in this study, including the resistance to cephalosporins, fluoroquinolones, and carbapenems. We look forward to examining these mechanisms of drug resistance in subsequent studies.
Conclusions
The drug resistance monitoring data from a single center from 2013 to 2021 showed that CR-E. coli, DTR-E. coli, FQR-E. coli, CR-K. pneumoniae, DTR-K. pneumoniae, ECR-K. pneumonia, and FQR-K. pneumoniae showed upward trends, whereas ECR-E. coli, CR-A. baumannii, DTR-A. baumannii, ECR-A. baumannii, FQR-A. baumannii, DTR-P. aeruginosa, CR-P. aeruginosa, ECR-P. aeruginosa, and FQR-P. aeruginosa showed downward trends. Among these trends, the upward trends in CR-E. coli and DTR-E. coli and the downward trends in DTR-P. aeruginosa and ECR-P. aeruginosa were significant.
Abbreviations
AMR, antimicrobial resistance; BSI, Bacterial bloodstream infection; MDR, Multidrug resistance; XDR, extensive drug resistance; PDR, pandrug-resistance; CDC, Center for Disease Control and Prevention; ECDC, European Centre for Disease Prevention and Control; DTR, Difficult to treat resistance; FQR, Fluoroquinolone resistance; CR, carbapenem resistance; ECR, Extended-spectrum cephalosporin resistant.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Marston HD, Dixon DM, Knisely JM, Palmore TN, Fauci AS. Antimicrobial Resistance. JAMA. 2016;316(11):1193–1204. doi:10.1001/jama.2016.11764
- Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
- Bassetti M, Vena A, Sepulcri C, Giacobbe DR, Peghin M. Treatment of Bloodstream Infections Due to Gram-Negative Bacteria with Difficult-to-Treat Resistance. Antibiotics. 2020;9(9):314. doi:10.3390/antibiotics9090632
- Kadri SS, Adjemian J, Lai YL, et al. Difficult-to-Treat Resistance in Gram-negative Bacteremia at 173 US Hospitals: retrospective Cohort Analysis of Prevalence, Predictors, and Outcome of Resistance to All First-line Agents. Clin Infect Dis. 2018;67(12):1803–1814. doi:10.1093/cid/ciy378
- Huh K, Chung DR, Ha YE, et al. Impact of Difficult-to-Treat Resistance in Gram-negative Bacteremia on Mortality: retrospective Analysis of Nationwide Surveillance Data. Clin Infect Dis. 2020;71(9):e487–e96. doi:10.1093/cid/ciaa084
- Zhang Z, Sun Z, Tian L. Antimicrobial Resistance Among Pathogens Causing Bloodstream Infections: a Multicenter Surveillance Report Over 20 Years (1998-2017). Infect Drug Resist. 2022;15:249–260. doi:10.2147/IDR.S344875
- Clinical and Laboratory Standards Institute. Analysis and Presentation of Cumulative Antimicrobial Susceptibility Test Data, M39-A4. Wayne, PA: Clin Lab Stand Institute; 2014.
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing, Thirtieth Informational Supplement, M100-S30. Wayne, PA: Clin Lab Stand Institute; 2020.
- Wang H, Wang H, Yu X, et al. Impact of antimicrobial stewardship managed by clinical pharmacists on antibiotic use and drug resistance in a Chinese hospital, 2010-2016: a retrospective observational study. BMJ Open. 2019;9(8):e026072. doi:10.1136/bmjopen-2018-026072
- Wanla W, Katip W, Supakul S, et al. Effects of an antimicrobial restriction system on appropriate carbapenem use in a hospital without infectious diseases consultation. Int J Gen Med. 2017;10:443–449. doi:10.2147/IJGM.S145133
- Li J, Huang Z, Tang M, et al. Clonal Dissemination of Multiple Carbapenemase Genes in Carbapenem-Resistant Enterobacterales Mediated by Multiple Plasmids in China. Infect Drug Resist. 2021;14:3287–3295. doi:10.2147/IDR.S327273
- Chen HY, Jean SS, Lee YL, et al. Carbapenem-Resistant Enterobacterales in Long-Term Care Facilities: a Global and Narrative Review. Front Cell Infect Microbiol. 2021;11:601968. doi:10.3389/fcimb.2021.601968
- Lin Q, Wang Y, Yu J, et al. Bacterial characteristics of carbapenem-resistant Enterobacteriaceae (CRE) colonized strains and their correlation with subsequent infection. BMC Infect Dis. 2021;21(1):638. doi:10.1186/s12879-021-06315-0
- Kyriakidis I, Vasileiou E, Pana ZD, Tragiannidis A. Acinetobacter baumannii Antibiotic Resistance Mechanisms. Pathogens. 2021;10(3):2154. doi:10.3390/pathogens10030373
- Feng W, Huang Q, Wang Y, et al. Changes in the resistance and epidemiological characteristics of Pseudomonas aeruginosa during a ten-year period. J Microbiol Immunol Infect. 2021;54(2):261–266. doi:10.1016/j.jmii.2019.08.017
- Katip W, Uitrakul S, Oberdorfer P. Clinical Efficacy and Nephrotoxicity of the Loading Dose Colistin for the Treatment of Carbapenem-Resistant Acinetobacter baumannii in Critically Ill Patients. Pharmaceutics. 2021;14(1):365. doi:10.3390/pharmaceutics14010031
- Katip W, Uitrakul S, Oberdorfer P. A Comparison of Colistin versus Colistin Plus Meropenem for the Treatment of Carbapenem-Resistant Acinetobacter baumannii in Critically Ill Patients: a Propensity Score-Matched Analysis. Antibiotics. 2020;9(10):871. doi:10.3390/antibiotics9100647
- Katip W, Oberdorfer P. Clinical Efficacy and Nephrotoxicity of Colistin Alone versus Colistin Plus Vancomycin in Critically Ill Patients Infected with Carbapenem-Resistant Acinetobacter baumannii: a Propensity Score-Matched Analysis. Pharmaceutics. 2021;13(2):87. doi:10.3390/pharmaceutics13020162