
Abstract
Background
Carbapenemase-producing Gram-negative bacteria, particularly Klebsiella pneumoniae (K. pneumoniae), are at the forefront of the list of causative agents of ventilator-associated pneumonia (VAP). The treatment options for such infections are limited, and various antimicrobial combinations have been suggested as alternatives in clinical practice. New antibiotics, such as ceftazidime/avibactam, ceftolozane/tazobactam and cefiderocol, have shown advantages in both in vitro and clinical studies.
Purpose
To evaluate the in vitro effect of meropenem–ciprofloxacin and meropenem–colistin combinations on carbapenem-resistant (CR) K. pneumoniae VAP isolates and to determine their susceptibility to new antibiotics.
Methods
Seventy-three K. pneumoniae isolates from 176 endotracheal samples from VAP cases were studied. Antibiotic susceptibility testing and phenotypic detection of extended-spectrum β lactamase (ESBL) and carbapenemase production were done. CR K. pneumoniae isolates were tested for the five predominant carbapenemase genes (blaKPC, blaOXA-48, blaNDM, blaVIM, and blaIMP). In vitro evaluation of meropenem–ciprofloxacin and meropenem–colistin combinations was done by MIC test strips. Susceptibility to new antibiotics was tested by disk diffusion method.
Results
Sixty-three (86.3%) of the isolates were ESBL producers and 52 (71.2%) were carbapenem resistant. BlaNDM was the most prevalent carbapenemase gene (50%), followed by blaOXA-48, (36.5%) then blaKPC in (11.5%). BlaVIM and blaIMP were not detected. Meropenem–ciprofloxacin combination showed indifferent effect on all isolates, while meropenem–colistin combination showed 25% synergism, 15.4% addition and 59.6% indifference. All (100%) CR K. pneumoniae isolates were resistant to ceftolozane/tazobactam and 79% were resistant to ceftazidime/avibactam, while 96% were sensitive to cefiderocol.
Conclusion
A high rate of carbapenem resistance exists among VAP K. pneumoniae isolates. Meropenem–colistin combination and cefiderocol appear to be potential treatment options for infections caused by CR K. pneumoniae. Resistance to the tested new β-lactam/β-lactamase inhibitors was high, signifying a major threat.
Introduction
Ventilator-associated pneumonia (VAP) is the most serious intensive care unit (ICU)-acquired infection of the lung parenchyma that develops after 48 hours of endotracheal intubation and mechanical ventilation.Citation1
Multidrug-resistant (MDR) bacteria, both Gram-positive and Gram-negative, have been associated with VAP but in low- and middle-income countries, it was found that the MDR Gram-negative bacilli like K. pneumoniae, Escherichia coli, Pseudomonas aeruginosa, Acinetobacter baumannii, and Enterobacter species predominate.Citation2
Carbapenems have been the last therapeutic option in the treatment of infections induced by MDR Enterobacterales.Citation3 Nevertheless, the development of different resistance mechanisms to carbapenems, as a result of their misuse, has reduced their effectiveness.Citation4
The use of antibiotic combinations has emerged as an alternative option for treatment of such infections seeking the synergism in suppressing bacterial resistance and curtailing the toxicity of the used antibiotics.Citation5
The use of broad-spectrum β-lactam and fluoroquinolone in combination has been recommended for treatment of VAP patients with risk factors for MDR Gram-negative bacilli or at high risk of death.Citation6
Colistin has been increasingly prescribed as the last treatment option for infections caused by CR bacteria, but limited efficacy of colistin monotherapy, its high toxicity and colistin hetero-resistance, have led to its use in combinations with other antibiotics.Citation7
In 2017, WHO defined CR Enterobacterales as one of the highest priority pathogens for the development of new antibiotics and some new antibiotics have been marketed or have approached late stages of development, new β-lactam/β-lactamase inhibitors such as ceftolozane/tazobactam, ceftazidime/avibactam, meropenem/vaborbactam have brought additional choices for clinicians treating these MDR organisms. With a broader spectrum of activity, the clinicians’ repertoire furtherly welcomed newer agents including cefiderocol, a catechol-substituted siderophore cephalosporin, eravacycline, a fluorocycline of the tetracycline class, and the synthetic aminoglycoside, plazomicin.Citation8
This study aimed to evaluate the in vitro effect of the frequently used combination in our ICU, meropenem–ciprofloxacin, in comparison to meropenem–colistin combination on CR K. pneumoniae isolates and to determine the susceptibility of these isolates to three new antibiotics with previously reported favorable outcomes in nosocomial pneumonia.
Materials and Methods
Study Design and Setting
This cross-sectional study was carried out during the period from January 2020 to November 2021 in the Medical Microbiology and Immunology Department and the Emergency ICU of Zagazig University Hospitals, a set of tertiary referral hospitals that serves five governorates in eastern Egypt. The Emergency ICU is a 24-bed unit that provides care for the most challenging and life-threatening acute, severely injured and critical cases.
The study was approved by the Institutional Review Board of Faculty of Medicine, Zagazig University (approval #5347-31-3-2019) and carried out in accordance with the Declaration of Helsinki. Informed written consent was obtained from patient first-degree relatives.
Patients
Mechanically ventilated patients who met the clinical and laboratory criteria of infection-related ventilator-associated complication as described by CDC’s National Health Safety Network (NHSN) in 2013 were subjected to microbiological evaluation for possible VAP.Citation9 Immunocompromised patients or those with evidence of chest infection prior to intubation were excluded.
Sample size was estimated using Epi Info 6, to be 176 VAP patients assuming that the frequency of K. pneumoniae among VAP patients is 43%Citation10 and the total number of possible VAP patients was 328 with 80% statistical power and 95% confidence interval.
Microbiological Evaluation
Specimen Collection, Culture and Bacterial Identification
Endotracheal aspirates (ETAs) were obtained under complete aseptic conditions. Microscopic examination of Gram-stained smears showing more than 25 neutrophils and less than 10 squamous epithelial cells/LPF was indicative of purulent lower respiratory secretions and possible infection.
Quantitative cultures were performed as follows: ETAs were liquefied and homogenized by vortexing for 1 minute and centrifuged at 3000 rpm for 10 minutes. They were serially diluted in sterile normal saline to 1/10, 1/100, and 1/1000, then 0.01 mL of 1/1000 dilution was inoculated on blood agar and MacConkey agar (Oxoid, UK) and incubated aerobically at 37 °C for 48 hours. Colony count was done by multiplying the number of colonies by the dilution and inoculation factor and expressed as CFU/mL. A colony count ≥105 CFU/mL was considered a diagnostic growth.Citation9,Citation11
Isolates from 176 non-duplicate VAP samples were identified by standard bacteriological methods: colonial morphology, Gram-stained films, and biochemical tests,Citation12 and K. pneumoniae species was then confirmed by API-20E (BioMérieux, USA).
Antimicrobial Susceptibility Testing
Antimicrobial susceptibility testing of K. pneumoniae isolates was done using the modified Kirby–Bauer disk diffusion method, and colistin minimum inhibitory concentration (MIC) value was detected by the colistin broth disk elution (CBDE) method according to the CLSI guidelines.Citation13 K. pneumoniae ATCC 2146 and K. pneumoniae ATCC 1705 were used as the quality control strains (Global Bioresource Center of American Type Culture Collection).
MDR strains were those showing non-susceptibility to one or more drugs in at least three antibiotic classes.Citation14
Phenotypic Determination of ESBL-Producing Isolates
K. pneumoniae isolates were first screened phenotypically for ESBL production according to the previous standard disk diffusion procedure by the four antimicrobial disks: Ceftazidime 30 μg, cefotaxime 30 μg, ceftriaxone 30 μg, and aztreonam 30 μg. ESBL production was considered if the inhibition zones were less than 22, 27, 25, and 27 mm respectively and was further confirmed by double disk synergy test (DDST).Citation13
Phenotypic Detection of Carbapenem-Resistant and Carbapenamase-Producing Strains
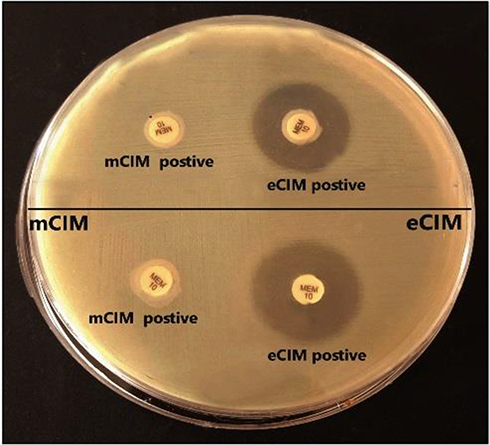
K. pneumoniae isolates that showed non-susceptibility to at least one of the four tested carbapenem antimicrobials (imipenem 10 μg, meropenem 10 μg, ertapenem 10 μg, and doripenem 10 μg) were considered carbapenem resistant and were phenotypically screened for carbapenemases production by modified carbapenem inactivation method (mCIM) and EDTA-modified carbapenem inactivation method (eCIM) as illustrated by CLSI 2021.Citation13 Briefly, one μL loopful of K. pneumoniae isolates from an overnight blood agar plate was resuspended in a 2 mL tube of tryptic soy broth (TSB) and in another 2-mL tube of TSB supplemented with EDTA at a final concentration of 5mM (20 μL of 0.5M EDTA was added to 2 mL of TSB). A meropenem disk was placed in each tube, and the tubes were incubated at 35°C for 4 h. Meropenem disks were then removed and applied to Mueller Hinton agar plates freshly plated with a 0.5 McFarland suspension of a carbapenem-susceptible E. coli ATCC25922 strain. The plates were incubated at 35°C for 16–20 h. The diameter of the inhibition zone around each meropenem disk was then measured. As for mCIM test interpretation, a tested isolate is considered carbapenemase producer if the inhibition zone diameter is 6−15 mm or presence of pinpoint colonies within a 16- to 18-mm zone while a clear zone of diameter 19 mm or more indicates a carbapenemase-negative isolate. eCIM results were interpreted only if mCIM was positive; an isolate is positive for MBL production when the eCIM zone size increases by ≥5 mm compared to the zone size observed for the mCIM, and is negative or MBL if the increase in zone size is <4 mm.
Molecular Detection of Carbapenemase Genes in CR K. pneumoniae Isolates
DNA extraction was done using GeneJET™ Genomic DNA Purification Kit (ThermoFisher Scientific, Germany). Five carbapenemase genes were sought by two multiplex PCRs; the first reaction was for genes encoding class A (blaKPC) and those encoding class D carbapenemases (blaOXA48). The other was for genes encoding class B “metallo-beta-lactamases” (MBL) (blaNDM, blaVIM and blaIMP). Amplification was performed using DreamTaq Green PCR Master Mix (ThermoFisher Scientific, Germany). Primers and conditions were as described by Poirel et alCitation15 K. pneumoniae ATCC BAA-1705 and K. pneumoniae ATCC BAA-2146 were used as the positive controls for blaKPC and blaNDM, respectively.
Antimicrobial Combination Testing
The in vitro effect of two combinations (ie, meropenem/ciprofloxacin and meropenem/colistin) was evaluated for CR K. pneumoniae isolates by “Perpendicular MIC test strip” method.Citation16
MIC values of meropenem, ciprofloxacin, and colistin were determined by MIC test strip (Liofilchem, Italy) separately and in combinations and the fractional inhibitory concentration index (Σ FIC) was calculated for each combination using the formula: Σ FIC = FIC [A]+ FIC [B].
FIC [A]= MIC of drug A in combination with drug B/ MIC of drug A alone.
FIC [B]= MIC of drug B in combination with drug A/ MIC of drug B alone.
The Σ FIC values determine the effect of the tested combination as follows: ≤0.5, synergy; >0.5 to ≤1.0, additively; >1.0 to <4.0, indifference; and ≥4, antagonism.Citation17
New Antibiotics Susceptibility Testing
The new agents obtained from (Liofilchem, Italy): ceftazidime/avibactam (CZA) (30/20 µg), ceftolozane/tazobactam (C/T) (30/10 µg) and cefiderocol (FDC) (30µg) were tested against CR K. pneumoniae isolates using the disk diffusion method. The diameters of the inhibition zones were interpreted according to CLSI 2021 guidelines.Citation13
Statistical Analysis
The data were statistically analyzed using (Statistical Package for Social Science) SPSS software version 20.0. Terms of numbers and percentages were used for representation of categorical variables. The distribution differences in categorical variables were calculated using the Chi square and Fisher exact test. A p value <0.05 was considered statistically significant and p > 0.05 was considered non-significant.
Results
Seventy-three (41.5%) K. pneumoniae isolates were recovered from 176 non duplicate endotracheal samples.
Most of the isolates were resistant to most classes of antibiotics with the highest resistance to penicillin (97.3%), cephalosporins (85%), monobactams (Aztreonam 83.6%), aminoglycoside (gentamycin 85%, and amikacin 80.8%), quinolones (ciprofloxacin and levofloxacin 85%) and carbapenems (imipenem 68.5% and meropenem 71.2%). While the least resistance was observed with doxycycline (11%) and chloramphenicol (20.5%). For colistin, 89% of the isolates were of intermediate susceptibility (MIC ≤2 μg) while 11% were resistant with (MIC ≥ 4 μg). Most of the isolates (n = 66, 90.4%) showed MDR phenotype. ().
Table 1 Antibiotic Susceptibility Pattern of K. pneumoniae Isolates by Disk Diffusion Method (n=73)
A high prevalence of ESBL production was detected among K. pneumoniae isolates reaching 86.3%.
Recent antibiotic therapy (within 1 month prior to mechanical ventilation) and previous hospitalization of 5 days or more were significant risk factors for CR K. pneumoniae in VAP cases ().
Table 2 Risk Factors Associated with VAP Caused by CR K. pneumoniae Isolates
Out of 52 CR K. pneumoniae isolates, carbapenemase production was detected in (38/52, 73.1%) using mCIM test (); of which 22 (58%) showed MBL production by eCIM test (.
Table 3 Carbapenemase Genes Detected in CR K. pneumoniae Isolates and the Corresponding mCIM and eCIM Results (n=52)
Figure 1 Results of mCIM/eCIM test of 2 CR K. pneumoniae isolates. The two isolates show positive mCIM/eCIM test results indicating MBL production.
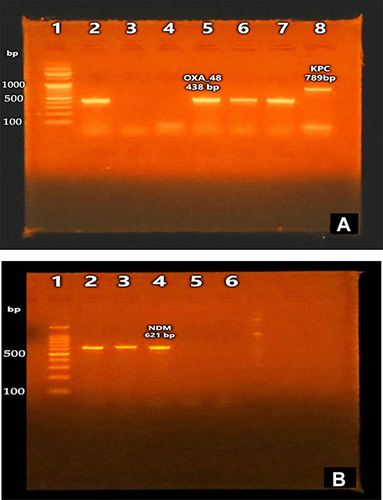
Regarding carbapenemase genes, PCR results showed that 42/52 (80.8%) of CR isolates harbored one or more of the tested carbapenemase genes. The most prevalent gene was blaNDM, it was found in 50% of the isolates (32.7% blaNDM only and 17.3% both blaNDM + blaOXA-48) , followed by blaOXA-48 in 36.5% of the isolates (19.2% blaOXA-48 only and 17.3% both blaNDM + blaOXA-48), then blaKPC in 11.5% of the isolates , while blaVIM and blaIMP were not detected. None of the studied genes were detected in (10/52, 19.2%) of the isolates. Co-existence of blaNDM and blaOXA-48 carbapenemase genes were observed in (9, 17.3%) of the isolates ().
Figure 2 PCR results for carbapenemase genes. (A) Agarose gel electrophoresis of blaKPC and blaOXA-48 amplicons. Lane (1): DNA ladder 100 bp, lanes (2, 5, 6, 7): positive for blaOXA-48 gene (438bp), lane (8): positive for blaKPC gene (789bp). (B) Agarose gel electrophoresis of blaNDM amplicons. Lane (1): DNA ladder 100 bp, lanes (2–4): positive for blaNDM gene (621bp).
Correlating the results of the phenotypic mCIM/eCIM for carbapenemases production and PCR results for carbapenemase genes showed that, only 38 out of 42 carbapenemase gene-positive isolates showed positive results by mCIM/eCIM. In addition, four of the isolates that co-harbor blaOXA-48 and blaNDM showed negative results for eCIM test ().
Meropenem MICs for the 52 CR K. pneumoniae isolates by E-test ranged from 8 to more than 32 μg/mL. All these isolates were ciprofloxacin resistant, where ciprofloxacin MIC values ranged from 8 to 64 μg/mL. Forty-four isolates (84.6%) were colistin-intermediate (MIC ≤2 μg/mL), and 8 isolates (15.4%) were resistant (MIC ≥4 μg/mL) where colistin MICs ranged from 0.125 to 16 μg/mL.
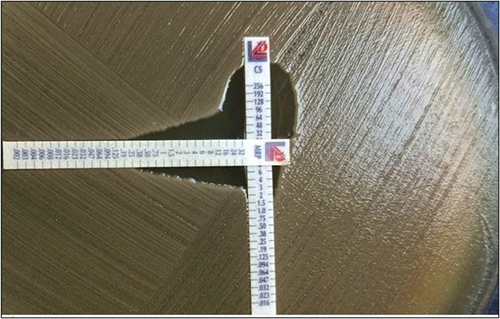
Meropenem–ciprofloxacin combination test showed indifferent effect against all CR K. pneumoniae isolates. On the other hand, meropenem–colistin combination showed 25% synergism (, 15.4% addition and 59.6% indifference. No antagonism was detected for either combination ().
Table 4 The Effect of Meropenem–Ciprofloxacin and Meropenem–Colistin Combinations on CR K. pneumoniae Isolates (n = 52)
Figure 3 Meropenem–colistin combination testing. This was a synergistic effect. Meropenem MIC was >32 μg/mL when tested alone but was 0.25 μg/mL in combination. Colistin MIC was 8 μg/mL when tested alone but was 1.5 μg/mL in combination.
Regarding susceptibility to new antibiotics (52/52) 100% of CR K. pneumoniae isolates were resistant to ceftolozane/tazobactam and (41/52) 79% were resistant to ceftazidime/avibactam; however, (50/52) 96% were sensitive to cefiderocol. All the MBL producing isolates were resistant to CZA and C/T (100% resistance), while resistance rates in serine producing strains were 62.5% and 100%, respectively ().
Table 5 Antibiotics Susceptibility Pattern of Carbapenem-Resistant K. pneumoniae Isolates to New Antibiotics According to Their Carbapenemase Genes (n=52)
Discussion
VAP accounts for one-fourth of the infections occurring in critically ill patients and is the reason for half of antibiotic prescriptions in mechanically ventilated patients.Citation1 CR K. pneumoniae is associated with high morbidity and mortality and is considered a significant public health challenge worldwide.
In the present study, K. pneumoniae was the most frequent VAP isolate with a rate of 41.5% (73/176). Similar results were obtained by a previous study on VAP in Emergency ICU in Zagazig University Hospitals where K. pneumoniae represented (43%) of VAP agents.Citation10 Lower results (29%) were reported by El-Kholy et alCitation18 The outstanding ability of K. pneumoniae to colonize skin, respiratory and gastrointestinal tracts of ICU patients as well as devices and instruments, its rapid spread between patients and its resistance to commonly used empirical antibiotics, account for the high prevalence of K. pneumoniae particularly in ICU patients with multiple risk factors including invasive mechanical ventilation.Citation19
Information about the prevalent VAP agents and their susceptibility to antimicrobials is regularly required to guide initial empirical therapy. In the present study, antibiotic resistance was high among K. pneumoniae isolates even to typically recommended antibiotics for the treatment of VAP. High resistance was detected with penicillins (97.3%) and cephalosporins (85%). Similarly, high rates of resistance were noticed for quinolones; 85% for each of ciprofloxacin and levofloxacin, and for aminoglycosides; 85% for gentamycin and 80.8% for amikacin. More or less similar high rates were reported by other studies.Citation10,Citation20–22 A high rate of carbapenem resistance was noticed where 71.2% of K. pneumoniae were carbapenem resistant, which is near to the results of a previous study in different ICUs in our facility.Citation20 The high rates of resistance are due to rapid horizontal transmission of resistance determinants between different species that is augmented by non-adherence to infection control standards.
Multidrug resistance among Gram-negative bacilli is a growing problem in hospital settings that led to the resurrection of polymyxin antibiotics as last options in life-threatening infections by these superbugs. In our study, 90.4% of K. pneumoniae isolates were MDR; this high rate was comparable to Azzab et al, who reported a similar rate of MDR K. pneumoniae causing VAP.Citation10 Colistin resistance, however, was detected in 11% of our isolates (MIC ≥ 4 μg) which goes in line with a recent study conducted on hospitalized patients at Egyptian National Cancer Institute where 8.8% of MDR K. pneumoniae isolates were colistin-resistant.Citation23
Evaluating the risk factors of VAP caused by CR K. pneumonia revealed that recent antibiotic use (1 month prior to mechanical ventilation) and previous hospitalization of 5 or more days were significant risk factors. Other studies reported similar findings as Patro et al.Citation24 Both prolonged hospitalization and the use of antibiotics enhances patients’ upper airway and endotracheal tube colonization with MDR bacteria that finally gain access to the lower airways causing pneumonia. In this perspective, routine surveillance endotracheal cultures, that detect colonizers, are proposed as predictors of invasive infection and a guide for empirical therapy in case VAP develops.
In the present study, the prevalence of ESBL-producing K. pneumoniae was extremely high among our isolates representing 86.3%. Similarly, a high rate (80%) was reported by another Egyptian study by Muhammed et al.Citation25 However, these are much higher than ESBL rates reported in many European countries that range from 2.4% to 5.1%.Citation26 The less controlled use of antibiotics in Egypt, where many drugs are still available over the counter, and the over reliance on third-generation cephalosporins, being broad spectrum and safe drugs, led to this high rate of ESBL production.
In fact, the hospital authorities and staff did not stand idly by on the issue of antibiotic resistance and since 2016, a comprehensive infection control program was started comprising bundle care to reduce hospital-acquired and device-associated infections, and thus reduce antibiotics use.Citation27 Moreover, an antibiogram was developed in 2019 to rationalize antibiotic prescription,Citation20 but unfortunately, these endeavors were hampered by the emergence of COVID-19 global pandemic and shortage of medical staff. In addition, being a tertiary hospital, the majority of the patients most probably have received medical care at some primary centers before admission where they get colonized with resistant pathogens and consequently these pathogens are continuously introduced into the hospital environment.
Carbapenem resistance is due to the production of carbapenemases or a combination of porin deficiency and other β-lactamases. As the susceptibility results of new antibiotics differ according to the type of carbapenemase, whether serine (KPC or OXA-48) or MBL, CR K. pneumoniae isolates were screened for carbapenemases production by mCIM and eCIM tests and were tested for detection of carbapenemase genes by PCR. In this study, 38 (73.1%) of the CR isolates were carbapenemase producers, of which 22 (58%) were MBL producers. Other studies reported carbapenemases as the main carbapenem-resistance mechanism;Citation28 Mohamed et al, in a previous Egyptian study, detected carbapenemase activity in 61.1% of the Klebsiella isolates; 66.2% of them were MBL producers.Citation29
PCR results for the commonly reported carbapenemase genes in Enterobacterales revealed that 80.8% of the isolates harbored carbapenemase genes, which is in concordance with another Egyptian study where carbapenemase genes were detected in 74% of the isolates.Citation30 The most prevalent gene was blaNDM (50%) followed by the blaOXA-48 (36.5%). This finding agrees with another study on Enterobacterales from Egyptian cancer patients,Citation31 but Raheel et al reported blaOXA-48 as the most common gene followed by blaNDM.Citation28 Predominance of blaNDM could be related to the fact that they are encoded on a variety of readily transmissible conjugative plasmids that are capable of horizontal inter- and intra-species transfer.Citation32 A low incidence rate of blaKPC (11.5%) was reported in our study, which is lower than Azzab et al, who reported a rate of 23.1%.Citation10 Absence of blaVIM and blaIMP genes in our study was also reported by other studiesCitation30,Citation32 suggesting that both genes are not prevalent in our geographical region. In addition, blaVIM genes are uncommon among Enterobacterales.Citation33 Co-existence of carbapenemase genes was observed where blaNDM and blaOXA48 were both detected in 17.3% of the isolates, a similar finding was reported by Raheel et al and Ahmed El-Domany et al.Citation28,Citation30 On the other hand, 10 (19.2%) of the CR isolates were negative for carbapenemase genes; these isolates may possess other mechanisms of carbapenem resistance such as ESBL production coupled with disruption in porin expression.Citation34
Four of the isolates that harbored carbapenemase genes showed negative results by mCIM. In addition, eCIM failed to detect MBL production in four isolates that co-harbor blaNDM and blaOXA-48; the co-production of a serine carbapenemase had probably masked the inhibitory effect of EDTA on the accompanying MBL. Moreover, carbapenemase genes may be not expressed or may be truncated producing nonfunctioning enzymes.Citation35 Therefore, phenotypic detection of carbapenemases production is better coupled to molecular detection of carbapenemase genes, particularly if targeted antibiotic therapy with one of the new drugs is to be considered as discussed later.
Antibiotic combination therapy and novel antibiotics are the current available strategies for treatment of infections by CR GNB. Combination therapy has long been considered as the standard for treating severe infections by CR GNB.Citation6 β-lactams and fluoroquinolones have been frequently used in our ICU for empiric treatment of VAP and in the present study, the in vitro effect of meropenem–ciprofloxacin combination was compared to meropenim–colistin combination against CR K. pneumoniae isolates. Meropenem–ciprofloxacin combination showed indifferent effect against all tested isolates. This is similar to Karki et al, who reported 100% indifferent effect of this combination when tested on XDR K. pneumoniae isolates.Citation36 On the other hand, Sueke et al reported 10% synergy, 80% addition and 10% indifference for the same combination.Citation16
Synergy testing of meropenem–colistin combination, showed 25% synergism, 15.4% addition and 59.6% indifference. No antagonism was observed for this combination. Better results with this combination were reported by a recent Indian study where the effect of meropenem–colistin combination tested by the checkerboard technique showed 56% synergism, 36% addition and indifference rate of 8%.Citation37
The favorable outcomes of the colistin-based combinations result from its ability to disrupt the outer membrane of Gram-negative bacteria by targeting lipopolysaccharides which increases the outer membrane permeability to the other drug. On the other hand, discrepant effects of antimicrobial combinations in different studies could be due to different methods of synergy testing with different interpretation methods and synergy definitions. Moreover, different genetic constitution of the tested isolates and the different antibiotic selective pressures possibly influence their response to drug combinations.
Regarding susceptibility to new antibiotics, resistance rates to ceftazidime/avibactam and ceftolozane/tazobactam were 79% and 100%, respectively. These are extremely high rates of resistance in comparison to the results of the Surveillance of Multicenter Antimicrobial Resistance in Taiwan (SMART) in 2017, which reported susceptibility rates of ceftazidime/avibactam and ceftolozane/tazobactam for K. pneumoniae isolates of 100% and 80%, respectively.Citation38 All the MBL-producing isolates were resistant to CZA and C/T (100% resistance), while resistance rates in serine-producing strains were 62.5% and 100%, respectively. These findings partially agree with previous studies, which stated that most MBL-positive strains were resistant to CZA and C/T, and the resistance rates ranged from 90.8% to 100%.Citation39
Avibactam is not effective against class B (MBL) but was found effective against serine carbapenemases by reversibly acylating themCitation40 and its reported resistance rates in serine carbapenemase-producing strains ranged from (16.7–21%) which contradicts our high rates of resistance.Citation39 Chemical modification of the target, presence of multiple (or even novel) beta-lactamases, changes in cell permeability and expression of efflux pumps are suggested causes for resistance exerted by non-MBL isolates. It is worth mentioning that avibactam, by its potent activity against class A β-lactamases (as ESBL) and AmpC-type determinants, restores the activity of aztreonam against MBL-producing Gram-negative bacteria that co-produce these β-lactamases that hydrolyze aztreonam.Citation41 Consequently, CZA plus aztreonam combination was recommended for treatment of MBL-producing Enterobacterales.Citation42
Cefiderocol had a good activity against our isolates as 96% of the isolates were sensitive, This was similar to a previous study that reported 100% sensitivity to cefiderocol.Citation43 Resistance to cefiderocol was also reported by previous studies where resistant mutants as well as cross resistance with ceftazidime/avibactam have been described.Citation44 Also, Yamano suggested that cefiderocol resistance could be attributed to simultaneous production of blaNDM and some serine-β-lactamases.Citation45
The previous findings point out to an alarming situation that might be encountered in the future, particularly with the continuous worsening of the issue of carbapenem and multidrug resistance in Egypt.
Conclusion
In this study, high resistance rates were detected among K. pneumoniae isolates to carbapenems and the tested new β-lactam/β-lactamase inhibitors. Meropenem–colistin combination appears to be a potential treatment option for infections caused by CR K. pneumoniae isolates but cefiderocol is superior for its greater in vitro activity, low resistance rates, stability to most carbapenemase classes and low toxicity, particularly if carbapenem-sparing strategies are to be implemented.
Disclosure
The authors report no conflicts of interest in relation to this work.
Acknowledgment
The authors would like to thank all the ICU staff for their assistance throughout the study.
Additional information
Funding
References
- Pozuelo-Carrascosa DP, Cobo-Cuenca AI, Carmona-Torres JM, Laredo-Aguilera JA, Santacruz-Salas E, Fernandez-Rodriguez R. Body position for preventing ventilator-associated pneumonia for critically ill patients: a systematic review and network meta-analysis. J Intensive Care. 2022;10(1):9. doi:10.1186/s40560-022-00600-z
- Erfani Y, Rasti A, Janani L. Prevalence of Gram negative bacteria in ventilator-associated pneumonia in neonatal intensive care units: a systematic review and meta-analysis protocol. BMJ Open. 2016;6(10):e012298. doi:10.1136/bmjopen-2016-012298
- Bush K. Alarming β-lactamase-mediated resistance in multidrug-resistant Enterobacteriaceae. Curr Opin Mirobiol. 2010;13(5):558–564. doi:10.1136/bmjopen-2016-012298
- El-Herte R, Kanj S, Matar G, Araj G. The threat of carbapenem resistant Enterobacteriaceae in Lebanon: an update on the regional and local epidemiology. J Infect Public Health. 2012;5(3):233–243. doi:10.1016/j.jiph.2012.02.003
- Laishram S, Pragasam AK, Bakthavatchalam YD, Veeraraghavan B. An update on technical, interpretative and clinical relevance of antimicrobial synergy testing methodologies. Indian J of Med Microbiol. 2017;35(4):445–468. doi:10.4103/ijmm.IJMM_17_189
- Barbier F, Bailly S, Schwebel C, et al. Infection-related ventilator-associated complications in ICU patients colonized with extended-spectrum beta-lactamase-producing Enterobacteriaceae. Intensive Care Med. 2018;44(5):616–626. doi:10.1007/s00134-018-5154-4
- Biswas S, Brunel JM, Dubus JC, Reynaud-Gaubert M, Rolain JM. Colistin: an update on the antibiotic of the 21st century. Expert Rev Anti Infect Ther. 2012;10(8):917–934. doi:10.1586/eri.12.78
- Doi Y. Treatment options for carbapenem-resistant gram-negative bacterial infections. Clin Infect Dis. 2019;69(Suppl 7):S565–575. doi:10.1093/cid/ciz830
- Magill SS, Klompas M, Balk R, et al. Developing a new, national approach to surveillance for ventilator-associated events: executive summary. Clin Infect Dis. 2013;57(12):1742–1746. doi:10.1093/cid/cit577
- Azzab MM, El Sokkary RH, Tawfeek MM, Gebriel MG. Multidrug-resistant bacteria among patients with ventilator-associated pneumonia in an emergency intensive care unit, Egypt. EMHJ. 2016;22(12):894–903. doi:10.26719/2016.22.12.894
- Wu CL, Yang DI, Wang NY, Kuo HT, Chen PZ. Quantitative culture of endotracheal aspirates in the diagnosis of ventilator associated pneumonia in patients with treatment failure. Chest. 2002;122:662–668. doi:10.1378/chest.122.2.662
- Cheesbrough M. District Laboratory Practice in Tropical Countries: Part 2. 1st ed. Cambridge University Press; 2006:62–70.
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing. 31st ed. CLSI supplement M100. Wayne, PA: Clinical and LaboratoryStandards Institute; 2021.
- Magiorakos A-P, Srinivasan A, Carey R, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
- Poirel L, Walsh TR, Cuvillier V, Nordmann P. Multiplex PCR for detection of acquired carbapenemase genes. Diagn Microbiol Infect Dis. 2011;70(1):119–123. doi:10.1016/j.diagmicrobio.2010.12.002
- Sueke H, Kaye SB, Neal T, Hall A, Tuft S, Parry CM. An in vitro investigation of synergy or antagonism between antimicrobial combinations against isolates from bacterial keratitis. Invest Ophthalmol Vis Sci. 2010;51(8):4151–4155. doi:10.1167/iovs.09-4839
- Pillai SK, Moellering RC, Eliopoulos GM. Antibiotics in laboratory medicine. In: Lorian V, editor. Antibiotics in Laboratory Medicine. 5th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2005:365–440.
- El-Kholy A, Saied T, Gaber M, et al. Device-associated nosocomial infection rates in intensive care units at Cairo University hospitals: the first step toward initiating surveillance programs in a resource-limited country. Am J Infect Control. 2012;40(6):e216–e220. doi:10.1016/j.ajic.2011.12.010
- Papazian L, Klompas M, Luyt CE. Ventilator-associated pneumonia in adults: a narrative review. Intensive Care Med. 2020;46(5):888–906. doi:10.1007/s00134-020-05980-0
- Negm EM, Mowafy S, Mohammed AA, et al. Antibiograms of intensive care units at an Egyptian tertiary care hospital. Egypt J Bronchol. 2021;15(1):1–5. doi:10.1186/s43168-021-00059-w
- Qadeer A, Akhtar A, Ain QU, et al. Antibiogram of medical intensive care unit at tertiary care hospital setting of Pakistan. Cureus. 2016;8(9):e809. doi:10.7759/cureus.809
- Gunjal P, Gunjal S, Kher S. A cross-sectional study to determine the profile and antibiotic resistance pattern of Gram-negative bacilli isolated from intensive care unit patients in a tertiary care hospital in Ahmednagar, Maharastra. Int J Biomed Adv Res. 2012;3(5):281–284. doi:10.7759/cureus.809
- Zafer MM, El-Mahallawy HA, Abdulhak A, Amin MA, Al-Agamy MH, Radwan HH. Emergence of colistin resistance in multidrug-resistant Klebsiella pneumoniae and Escherichia coli strains isolated from cancer patients. Ann Clin Microbiol Antimicrob. 2019;18(1):40. doi:10.1186/s12941-019-0339-4
- Patro S, Sarangi G, Das P, et al. Bacteriological profile of ventilator-associated pneumonia in a tertiary care hospital. Indian J Pathol Microbio. 2018;61(3):375–379. doi:10.4103/IJPM.IJPM_487_16
- Muhammed M, Flokas ME, Detsis M, Alevizakos M, Mylonakis E. Comparison between carbapenems and β-Lactam/β-Lactamase inhibitors in the treatment for bloodstream infections caused by extended-spectrum β-Lactamase-producing Enterobacteriaceae: a systematic review and meta-analysis. Open Forum Infect Dis. 2017;4(2):ofx099. doi:10.1093/ofid/ofx099
- Toubiana J, Timsit S, Ferroni A, et al. Community-onset extended-spectrum β-Lactamase- producing Enterobacteriaceae invasive infections in children in a university hospital in France. Medicine. 2016;95(12):e3163. doi:10.1097/MD.0000000000003163
- El-Sokkary RH, Negm EM, Othman HA, Tawfeek MM, Metwally WS. Stewardship actions for device associated infections: an intervention study in the emergency intensive care unit. J Infect Public Health. 2020;13(12):1927–1931. doi:10.1016/j.jiph.2020.10.003
- Raheel A, Azab H, Hessam W, Abbadi S, Ezzat A. Detection of carbapenemase enzymes and genes among carbapenem-resistant Enterobacteriaceae isolates in Suez Canal University Hospitals in Ismailia, Egypt. Microbes Infect Dis. 2020;1(1):24–33. doi:10.21608/mid.2020.25702.1007
- Mohamed ER, Ali MY, Waly NG, Halby HM, El-Baky RMA. The Inc FII plasmid and its contribution in the transmission of blaNDM-1 and blaKPC-2 in Klebsiella pneumoniae in Egypt. Antibiotics. 2019;8(4):266. doi:10.3390/antibiotics8040266
- Ahmed El-Domany R, El-Banna T, Sonbol F, Abu-Sayedahmed SH. Co-existence of NDM-1 and OXA-48 genes in carbapenem resistant Klebsiella pneumoniae clinical isolates in Kafrelsheikh, Egypt. Afr Health Sci. 2021;21(2):489–496. doi:10.4314/ahs.v21i2.2
- Tawfick MM, Alshareef WA, Bendary HA, Elmahalawy H, Abdulall AK. The emergence of carbapenemase blaNDM genotype among carbapenem-resistant Enterobacteriaceae isolates from Egyptian cancer patients. Eur J Clin Microbiol Infect Dis. 2020;39(7):1251–1259. doi:10.1007/s10096-020-03839-2
- Baran I, Aksu N. Phenotypic and genotypic characteristics of carbapenem-resistant Enterobacteriaceae in a tertiary-level reference hospital in Turkey. Ann Clin Microbiol Antimicrob. 2016;15:20. doi:10.1186/s12941-016-0136-2
- Codjoe FS, Donkor ES. Carbapenem resistance: a review. Med Sci. 2018;6(1):1. doi:10.3390/medsci6010001
- El-Kholy AA, Elanany MG, Sherif MM, Gad MA. High prevalence of VIM, KPC, and NDM expression among surgical site infection pathogens in patients having emergency surgery. Surg Infect (Larchmt). 2018;19(6):629–633. doi:10.1089/sur.2018.088
- Xie L, Dou Y, Zhou K, et al. Coexistence of blaOXA−48 and truncated blaNDM−1 on different plasmids in a Klebsiella pneumoniae isolate in China. Front Microbiol. 2017;8:133. doi:10.3389/fmicb.2017.00133
- Karki R, Lamichhane S, Basnet BB, Dahal A, Awal BK, Mishra SK. In vitro antimicrobial synergy testing of extensively drug-resistant clinical isolates at an organ transplant center in Nepal. Infect Drug Resist. 2021;14:1669–1677. doi:10.2147/IDR.S309531
- Dhandapani S, Sistla S, Gunalan A, Manoharan M, Sugumar M, Sastry AS. In-vitro synergistic activity of colistin and meropenem against clinical isolates of carbapenem resistant E. coli and Klebsiella pneumoniae by checkerboard method. Indian J Med Microbiol. 2021;39(1):6–10. doi:10.1016/j.ijmmb.2020.10.018
- Liao CH, Lee NY, Tang HJ, et al. Antimicrobial activities of ceftazidime-avibactam, ceftolozane-tazobactam, and other agents against Escherichia coli, Klebsiella pneumoniae, and Pseudomonas aeruginosa isolated from intensive care units in Taiwan: results from the surveillance of multicenter antimicrobial resistance in Taiwan in 2016. Infect Drug Resist. 2019;12:545–552. doi:10.2147/IDR.S193638
- de Jonge BL, Karlowsky JA, Kazmierczak KM, Biedenbach DJ, Sahm DF, Nichols WW. In vitro susceptibility to ceftazidime-avibactam of carbapenem non susceptible Enterobacteriaceae isolates collected during the INFORM Global Surveillance Study (2012 to 2014). Antimicrob Agents Chemother. 2016;60(5):3163–3169. doi:10.1128/AAC.03042-15
- Sharma R, Park TE, Moy S. Ceftazidime-avibactam: a novel cephalosporin/βlactamase inhibitor combination for the treatment of resistant Gram-negative organisms. Clin Ther. 2016;38:431–444. doi:10.1016/j.clinthera.2016.01.018
- Mauri C, Maraolo AE, Di Bella S, Luzzaro F, Principe L. The revival of aztreonam in combination with avibactam against metallo-β-Lactamase-producing gram-negatives: a systematic review of in vitro studies and clinical cases. Antibiotics. 2021;10:1012. doi:10.3390/antibiotics10081012
- Tamma PD, Aitken SL, Bonomo RA, Mathers AJ, van Duin D, Clancy CJ. Infectious Diseases Society of America guidance on the treatment of Extended-Spectrum β-lactamase Producing Enterobacterales (ESBL-E), Carbapenem-Resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with Difficult-to-Treat Resistance (DTR-P. aeruginosa). Clin Infect Dis. 2021;72(7):e169–e183. PMID: 33106864. doi:10.1093/cid/ciaa1478
- Iregui A, Khan Z, Landman D, Quale J. Activity of cefiderocol against enterobacterales, pseudomonas aeruginosa, and Acinetobacter baumannii endemic to medical centers in New York city. Microb Drug Resist. 2020;26(7):722–726. doi:10.1089/mdr.2019.0298
- Hobson CA, Cointe A, Jacquier H, et al. Cross-resistance to cefiderocol and ceftazidime–avibactam in KPC β-lactamase mutants and the inoculum effect. Clin Microbiol Infect. 2021;27(8):1172.e7–1172.e10. doi:10.1016/j.cmi.2021.04.016
- Yamano Y. In vitro activity of cefiderocol against a broad range of clinically important gram-negative bacteria. Clin Infect Dis. 2019;69(Suppl 7):S544–S551. doi:10.1093/cid/ciz827