
Abstract
Background
With the widespread use of steroids and immunosuppressants in mainland China, disseminated strongyloidiasis is becoming a severely underestimated tropical disease due to the lack of disease-specific manifestations and well-established diagnostic methods.
Case Presentation
Here, we report a 70-year-old woman who was diagnosed with Guillain-Barré syndrome due to autonomic disturbance, symmetrical bulbar palsy, and lower-motor-nerve damage in the extremities; her symptoms continued to worsen after hormone and immunoglobulin therapy. Later, parasitic larvae were found in the patient’s gastric fluid, and metagenomic Next Generation Sequencing (mNGS) detection of bronchoalveolar-lavage fluid also found a large number of Strongyloides roundworms. The patient was diagnosed with disseminated strongyloidiasis. The patient was given albendazole for anthelmintic treatment, but died two days after being transferred to the ICU due to the excessive strongyloidiasis burden.
Conclusion
This case highlights the combined application of mNGS and traditional testing in the clinical diagnosis of difficult and critical parasitic infections in immunocompromised patients. mNGS is a new, adjunct diagnostic method to rapidly screen for possible parasitic etiologies.
Introduction
Tropical and subtropical regions are highly-endemic areas of Strongyloides stercoralis, with approximately 100–370 million people worldwide affected, and yet, it is a neglected tropical disease.Citation1,Citation2 Strongyloidiasis has a high prevalence in Latin America, sub-Saharan Africa, and Southeast Asia, according to a survey. In addition, studies have shown that the main risk groups are refugees and immigrants, as their infection rate exceeds 75%.Citation3 This may indicate a high prevalence of Strongyloides infection in socioeconomically-poor and environmentally-deprived areas.
The clinical symptoms of Strongyloides stercoralis are not specific, and most cases are accompanied by eosinophilia.Citation4 Disseminated strongyloidiasis usually occurs in immunocompromised patients, such as those who are HIV-positive or who are taking long-term steroids. Strongyloides stercoralis affects various parts of the body, such as the lymph nodes, central nervous system, pancreas, kidneys, ovaries, and skeletal muscles. Mortality in such patients, if they are not treated promptly, is almost 100%.Citation5
There is no gold-standard method for diagnosing strongyloidiasis. To detect larval stages in fecal samples, there are different types of parasitological procedures available, including microscopy (direct smear, formalin-ethyl acetate, and Bellman’s method) and culture (haram and agar plates). Because low parasite loads and disturbed larval clearance may contribute to the low sensitivity of the techniques listed above, it is necessary to collect several stool samples at different times. We report a 70-year-old woman who was diagnosed with Guillain-Barré syndrome due to autonomic disturbance, symmetrical bulbar palsy, and lower-motor-nerve damage in the extremities, whose symptoms continued to worsen after hormone and immunoglobulin (Ig) therapy. Later, parasitic larvae were found in the patient’s gastric fluid, and metagenomic Next Generation Sequencing (mNGS) detection of bronchoalveolar-lavage fluid also found a large number of Strongyloides. The patient was diagnosed with disseminated strongyloidiasis and given albendazole for anthelmintic treatment, but the patient died two days after being transferred to the ICU due to the excessive strongyloidiasis burden.
Case Report
A 70-year-old rural woman went to the doctor with dyspnea, palpitations, and hoarseness that had persisted for more than twenty days. The community doctor diagnosed airway spasm and gave the patient anti-infection, anti-asthmatic, and heart-rate reduction medications, and other treatments, but the symptoms did not improve. The patient came to our hospital for treatment due to aggravation of the dyspnea and various symptoms such as anorexia, choking, difficulty in defecation, and limb weakness. The patient had coronary heart disease, hypertension, diabetes, immune thrombocytopenia, and other diseases in the past, and had a four-month history of taking glucocorticoid and immunosuppressive drugs. Physical examination showed that the patient was wheezing and was in poor spirits. The wheezing sounds were heard in both lungs, the patient’s heart rate was 128 beats/min, and ulceration scars and pigmentation were seen on the left arm and the outer side of the left thigh.
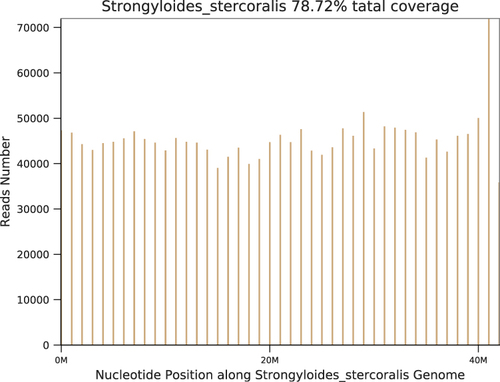
The following relevant examinations were completed after admission: blood-gas analysis indicating respiratory alkalosis combined with metabolic acidosis; blood examination indicating increases in leukocyte and eosinophil counts; liver function tests showed ALT 53 U/L and albumin 29.7g/L; tests that indicated renal function, antinuclear antibody (ANA), antiphospholipid antibody, and myocardial enzymes were all normal; and a brain MRI showed multiple ischemic foci (). Chest CT showed bronchiolitis, but did not rule out early alveolar hemorrhage (). After anti-inflammatory, anti-infective, diuretic, acid-suppressing, antiemetic, gastrointestinal motility promotion, nutritional support, and other treatments, the patient’s dyspnea symptoms were relieved, but there were still symptoms such as nausea, limb weakness, and difficulty in voluntary defecation. On the ninth day after admission, the patient developed a headache and a high fever. The blood IgE (836 IE/mL) and IgG4 (1710 mg/L) levels were significantly increased, and the complement C3 level was decreased. The neurologist recommended intravenous mannitol to reduce intracranial pressure and the headache symptoms subsequently improved. The neurologist considered the facts of the case: the patient had autonomic dysfunction; symmetrical bulbar palsy; lower-motor-nerve damage in the extremities; and the anti-sulfatide antibody blood test was positive; and gave a diagnosis of autonomic Guillain-Barré syndrome (a lumbar puncture was not performed at the patient’s request). Intravenous immune globulin combined with glucocorticoids was given for treatment. After the medication, the patient’s symptoms continued to worsen, accompanied by severe vomiting, and a larval parasite was seen in the gastric juice under the microscope (Video 1). The patient was transferred to the ICU due to lack of consciousness and dyspnea. Chest computerized tomography (CT) examination showed diffuse infectious lesions in both lungs (), and abdominal CT showed intestinal wall edema and ascites (). An endotracheal ventilator was given to assist ventilation, and blood was seen gushing out of the endotracheal tube (Video 2). Deworming treatment with albendazole was given. In order to strengthen sputum drainage and collect etiological specimens, sputum suction and bronchoalveolar lavage were performed by bronchoscopy. A large amount of bloody fluid was seen under bronchoscopy. High-throughput gene sequencing of the pathogenic microorganisms in the bronchoalveolar-lavage fluid showed that the number of strongyloides sequences identified was 1,700,865, suggesting that there were a large number of Strongyloides roundworms in the bronchoalveolar lavage fluid (). The patient died two days after being admitted to the ICU, due to the rapid progression of her condition. After discussion by hospital experts, the cause of death was determined to be disseminated strongyloidiasis.
Figure 1 Brain MRI showed multiple ischemic foci in the brain.
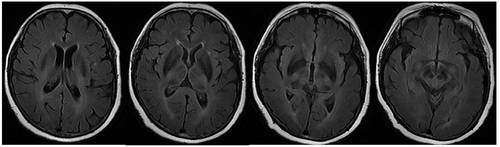
Figure 2 Chest CT showed bronchiolitis, excluding early alveolar hemorrhage.
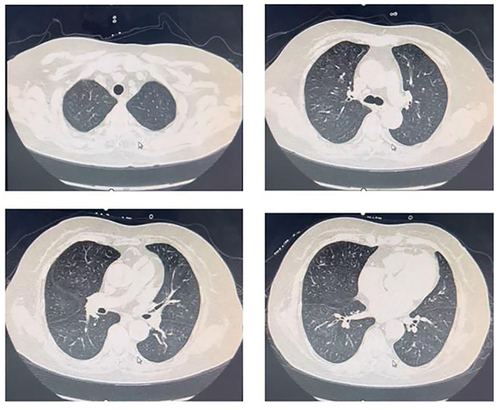
Figure 3 Diffuse infectious lesions in both lungs were seen in chest CT examination after transfer to ICU.
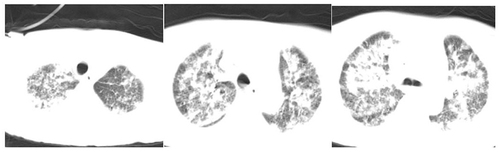
Figure 4 Abdominal CT showed intestinal wall edema and ascites.
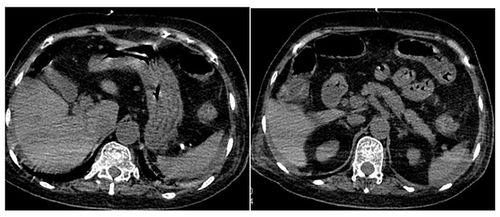
Figure 5 mNGS shows a large number of Strongyloides steroids sequences.
Discussion and Conclusions
Strongyloides stercoralis is a human parasitic nematode found in tropical and subtropical regions throughout the world. Infection rates are high in the Caribbean, West and East Africa, and especially South-East Asia.Citation6 Strongyloides stercoralis is a facultative pathogen that opportunistically alternates between free-living and parasitic life cycles. Adult worms reside in the intestinal tract during the parasitic cycle, and larvae can invade organs such as the lungs, brain, liver, and kidneys, resulting in strongyloidiasis.Citation7 In some developing countries such as China, the Philippines, and Vietnam, the incidence of strongyloidiasis is increasing year-to-year.Citation8 With the widespread use of steroids and immunosuppressants in mainland China, disseminated strongyloidiasis is becoming a severely underestimated tropical disease, due to the lack of disease-specific manifestations and well-established diagnostic methods.Citation9
According to a statistic from Boxing County, Shandong Province, 11 out of 854 residents were infected with Strongyloides stercoralis, giving an infection rate was 1.29%, and there was no significant difference in infection status related to gender or age distribution.Citation10 This patient lives in a rural area in Shandong Province, which is not an area where strongyloidiasis is endemic. The patient had a long-term history of taking glucocorticoids and immunosuppressants and was admitted to the hospital as a result of the combination of symptoms present. After admission, she was diagnosed with Guillain-Barré syndrome due to the presence of autonomic dysfunction, symmetrical bulbar palsy, and lower-motor-nerve damage in the extremities. After hormone and immunoglobulin therapy, the patient’s symptoms progressively worsened, and Strongyloides roundworms were found in the gastric juice and bronchoalveolar-lavage fluid. Although she was given deworming treatment, the patient died due to the excessive load of Strongyloides stercoralis. Many symptoms of Guillain-Barré syndrome are similar to disseminated strongyloidiasis, which was the main reason for the misdiagnosis of this case. Previous studies have found that eosinophilia and IgE increases commonly occur in asymptomatic and acute strongyloidiasis patients.Citation11 However, patients with disseminated strongyloidiasis usually do not have eosinophilia;Citation7 this case did not show eosinophilia on multiple blood tests, which made the diagnosis of strongyloidiasis more difficult.
Detection of rod-shaped or filamentous larvae in feces, sputum, gastric juice, and cerebrospinal fluid is the main diagnostic method for strongyloidiasis. Immunological techniques and RT-PCR can also be used for diagnosis.Citation12,Citation13 The adult parasite was found in the gastric juice of the patient, and a very high number of sequences of Strongyloides stercoralis were found in the bronchoalveolar-lavage fluid by mNGS. In non-endemic areas, serological methods are often not available due to constraints. The core principle of the main technology of mNGS is the sequencing-by-synthesis of bridging PCR and fluorescent, reversible terminators. First, the single-stranded DNA library to be tested is constructed to form an oligonucleotide bridge, and then PCR amplification and denaturation are carried out. The 3’-end, extension-stop group of the deoxynucleoside triphosphate (dNTP) is cut off and the bases are added for sequencing. At present, mNGS has made remarkable progress and is developing into a kind of molecular microscope, which is involved in almost every field of biomedical research.Citation14 mNGS can provide more aetiological information than RT-PCR. Therefore, mNGS could be a powerful tool for identifying unknown pathogens in clinical specimens when traditional methods are negative for all pathogens. mNGS can sensitively detect almost all kinds of microorganisms and parasites, and has an extremely important position in the diagnosis of difficult infectious diseases. mNGS has unique advantages in the detection of novel pathogens, difficult-to-cultivate mycobacteria, and parasites.Citation15,Citation16 In recent years, mNGS has been increasingly used in clinical practice, and is becoming the main means of detecting Strongyloides stercoralis in non-endemic areas.
For disseminated strongyloidiasis, the Committee to Advise on Tropical Medicine and Travel (CATMAT) recommends dual therapy with ivermectin and albendazole, based on case reportsCitation17 and the clinical experience of CATMAT members.Citation18 Ivermectin is currently the most effective treatment for strongyloidiasis,Citation19 but there is no commercial preparation of this drug in mainland China, and there is a lower success rate associated with the single-agent use of albendazole as a treatment for disseminated strongyloidiasis than there is for the recommended therapy.
Diagnosis of disseminated strongyloidiasis is difficult due to the lack of specificity in clinical manifestations and the lack of rapid and effective diagnostic methods. High-risk groups who use glucocorticoids and immunosuppressants should be aware of the threat of infection and take active prevention steps. For example, do not go barefoot when traveling in fields, and wash raw vegetables and fruit thoroughly.Citation20 Patients receiving long-term steroids should also take prophylactic medication (albendazole) every three months to prevent strongyloidiasis.Citation9
This case report has some limitations. First, the patient had a severe pulmonary infection and was transferred to the ICU, we considered that the patient might have bacterial infections in addition to parasitic ones. Therefore, the patient’s bronchoalveolar-lavage fluid was collected for mNGS (the advantage to this test is that there are more types of pathogens that can be found, and the time it takes to run is shorter). At that time, the patient’s condition was relatively urgent, and it would take a lot of time for us to contact the parasitology experts of the university, so we did not carry out the identification of parasites under the microscope. Second, our hospital does not have the PCR technology for parasite identification, which may be due to the fact that Shandong Province in China is not an endemic area for parasites. Third, ivermectin is not legally available in mainland China, so the patient did not receive the internationally-standard treatment.
Ethics Approval and Informed Consent
Written informed consent was obtained from the next of kin for publication of this case report and accompanying images. No ethical committee approval was required for this study as the data were analyzed in a retrospective manner.
Author Contributions
All authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; participated in drafting the article or revising it substantially; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to take responsibility for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
All authors thank the patient and her families for their support.
Additional information
Funding
References
- Palmeirim MS, Hürlimann E, Knopp S, et al. Efficacy and safety of co-administered ivermectin plus albendazole for treating soil-transmitted helminths: a systematic review meta-analysis and individual patient data analysis. PLoS Negl Trop Dis. 2018;12(4):e0006458. doi:10.1371/journal.pntd.0006458
- Zibaei M, Nosrati MRC, Shadnoosh F, et al. Insights into hookworm prevalence in Asia: a systematic review and meta-analysis. Trans R Soc Trop Med Hyg. 2020;114(3):141–154. doi:10.1093/trstmh/trz115
- Schär F, Trostdorf U, Giardina F, et al. Strongyloides stercoralis: global distribution and risk factors. PLoS Negl Trop Dis. 2013;7(7):e2288. doi:10.1371/journal.pntd.0002288
- Gonzalez-Ibarra F, Chevli P, Schachter L, et al. Strongyloidiasis and diffuse alveolar hemorrhage in a patient with systemic lupus erythematosus. Case Rep Med. 2014;2014:278390. doi:10.1155/2014/278390
- Beknazarova M, Whiley H, Ross K. Strongyloidiasis: a disease of socioeconomic disadvantage. Int J Environ Res Public Health. 2016;13(5):517. doi:10.3390/ijerph13050517
- Bethony J, Brooker S, Albonico M, et al. Soil-transmitted helminth infections: ascariasis, trichuriasis, and hookworm. Lancet. 2006;367(9521):1521–1532. doi:10.1016/S0140-6736(06)68653-4
- Lim S, Katz K, Krajden S, et al. Complicated and fatal Strongyloides stercoralis infection in Canadians: risk factors, diagnosis and management. CMAJ. 2004;171:479–484. doi:10.1503/cmaj.1031698
- Paula FM, Costa-Cruz JM. Epidemiological aspects of strongyloidiasis in Brazil. Parasitology. 2011;138:1331–1340. doi:10.1017/S003118201100120X
- Wang C, Xu J, Zhou X, et al. Strongyloidiasis: an emerging infectious disease in China. Am J Trop Med Hyg. 2013;88(3):420–425. doi:10.4269/ajtmh.12-0596
- Guo JD, Zhao LL. Strongyloides stercoralis investigation among population at Yellow River flood area in the lower Yellow River [in Chinese]. Chin J Parasitic Dis Contr. 2005;18:2–4.
- Lagacé-Wiens PR, Harding GKA. Canadian immigrant with coinfection of Strongyloides stercoralis and human T-lymphotropic virus 1. CMAJ. 2007;177:451–453. doi:10.1503/cmaj.070126
- Arifin N, Hanafiah KM, Ahmad H, Noordin R. Serodiagnosis and early detection of Strongyloides stercoralis infection. J Microbiol Immunol Infect. 2019;52:371–378. doi:10.1016/j.jmii.2018.10.001
- Buonfrate D, Requena-Mendez A, Angheben A, et al. Accuracy of molecular biology techniques for the diagnosis of Strongyloides stercoralis infection-A systematic review and meta-analysis. PLoS Negl Trop Dis. 2018;12:e0006229. doi:10.1371/journal.pntd.0006229
- Qian YY, Wang HY, Zhou Y, et al. Improving Pulmonary Infection Diagnosis with Metagenomic Next Generation Sequencing. Front Cell Infect Microbiol. 2021;10:567615.
- Chen P, Sun W, He Y. Comparison of metagenomic next-generation sequencing technology, culture and GeneXpert MTB/RIF assay in the diagnosis of tuberculosis. J Thorac Dis. 2020;12:4014–4024. doi:10.21037/jtd-20-1232
- Huang H, Deng J, Qin C, et al. Disseminated Coinfection by Mycobacterium fortuitum and Talaromyces marneffei in a Non-HIV Case. Infect Drug Resist. 2021;14:3619–3625. doi:10.2147/IDR.S316881
- Qu J, Zong Z. Strongyloidiasis in a patient diagnosed by metagenomic next-generation sequencing: a case report. Front Med. 2022;9:835252. doi:10.3389/fmed.2022.835252
- Boggild AK, Libman M, Greenaway C, et al. CATMAT statement on disseminated strongyloidiasis: prevention, assessment and management guidelines. Can Commun Dis Rep. 2016;42(1):12–19. doi:10.14745/ccdr.v42i01a03
- Henriquez-Camacho C, Gotuzzo E, Echevarria J, et al. Ivermectin versus albendazole or thiabendazole for Strongyloides stercoralis infection. Cochrane Database Syst Rev. 2016;1:CD007745.
- Singer R, Sarkar S. Modeling strongyloidiasis risk in the United States. Int J Infect Dis. 2020;100:366–372. doi:10.1016/j.ijid.2020.09.002