
Abstract
Introduction
The causes of femoral head necrosis mainly include trauma, corticosteroid, and alcohol, among which Brucella is highly unusual.
Patients and Methods
This paper reported three rare cases of femoral head necrosis due to Brucella, summarizing and analyzing the epidemiological history, clinical manifestations, laboratory examinations, imaging findings, individualized therapy, and biopsy results of patients with this disease. A literature review related to brucellosis and femoral head necrosis was conducted.
Results
All three patients had an epidemic history of brucellosis. They suffered from hip pain and limitation of movement for months, and femoral head necrosis was confirmed by magnetic resonance imaging (MRI). Pathological Giemsa staining or real-time polymerase chain reaction (real-time PCR) confirmed Brucella melitensis (B. melitensis) as the cause of osteonecrosis. Each patient received individualized therapy according to the degree of osteonecrosis, which was based on anti-brucellosis medications and hip puncture and irrigation decompression. They were followed up for more than two years and rehabilitated well.
Conclusion
Brucella infection should always be considered the cause of femoral head necrosis for patients with hip pain, especially for those with an epidemic history; early diagnosis and individual stepwise therapy can prevent the progression of osteonecrosis.
Introduction
Trauma, corticosteroid, alcohol, hip dysplasia, decompression sickness, homeopathy, Gaucher’s disease, and human immunodeficiency virus (HIV) are some pathogens responsible for femoral head necrosis, among which trauma, corticosteroid, and alcohol are the most common.Citation1–5 Brucella primarily infects humans’ bone and joint system, resulting in spondylitis, sacroiliitis, and so on; pyogenic hip arthritis is relatively rare, and osteonecrosis of the femoral head is even more unusual.Citation6 There have been only three cases of osteonecrosis of the femoral head caused by Brucella, mainly speculated due to the absence of a conclusive basis of bacterial culture or pathological diagnosis.Citation7–9 This paper describes three unusual cases of femoral head necrosis due to Brucella; we also discuss possible pathogenesis, the novelty of our cases, individualized stepwise therapy, and prognosis.
Patients and Methods
This study collected data on the epidemiological history, clinical manifestations, laboratory examinations, imaging findings, therapy, and pathological biopsy results of three patients with femoral head necrosis due to Brucella infection. These three patients were followed up for more than two years. We discussed the possible etiology, previous case reports, diagnosis methods, and treatment options of this type of bacterial osteonecrosis of the femoral head.
Case Presentation
Case 1
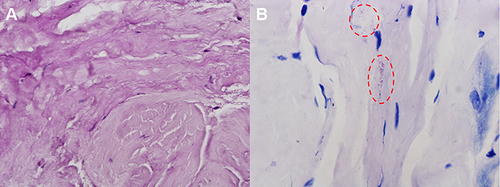
The patient is a 37-year-old Chinese male. In April 2014, he was diagnosed with brucellosis due to fever and fatigue, and his symptoms disappeared after anti-brucellosis medications for three months. In October 2014, the patient developed left hip pain, worsened by weight-bearing, and was admitted to the orthopedics department of our hospital in December 2014 due to the deterioration of symptoms. He is a sheep herdsman without any history of trauma, alcoholism, or hormone use. Physical examination revealed that the active and passive motion of the left hip was somewhat restricted due to pain. X-ray demonstrated that the left femoral head exhibited a strip-like low-density area but no evidence of stenosis (). CT scan revealed cavity necrosis in the left femoral head (). MRI revealed necrosis of the left femoral head, and effusion in the left joint cavity (). Blood test showed WBC 6.85 × 109/L with neutrophils accounted for 61.8%, CRP 3.5 mg/L, ESR 2.00 mm/h. SAT was positive at a titer of 1:320, and all tests for tuberculosis and rheumatoid arthritis were negative. Having been diagnosed with brucellar hip arthritis complicated by osteonecrosis of the left femoral head, the patient underwent puncture and irrigation of the left hip joint and core decompression and bone grafting. B. melitensis was detected in hip joint effusion and osteonecrosis of femoral head by real-time PCR. HE staining of a core biopsy of the left femoral head revealed amorphous necrotic material (); Giemsa staining can demonstrate scattered positive Brucella (). Triple anti-infective therapy was administered after the operation: rifampicin (0.6g po qd; Guangdong Hengjian Pharmaceuticals), doxycycline (0.1g po bid; Jiangsu Lianhuan Pharmaceuticals), and levofloxacin (0.2g ivgtt bid; Yangtze River Pharmaceuticals). Upon discharge from the hospital two weeks after the operation, his left hip pain was substantially relieved, and the antibiotic regimen was adjusted to rifampicin (0.6g po qd; Guangdong Hengjian Pharmaceuticals) and doxycycline (0.1g po bid; Jiangsu Lianhuan Pharmaceuticals) for six months. In follow-up, the symptoms of left hip pain and movement limitation disappeared almost half a year later, and there was no obvious abnormality in the blood test or hip X-ray (). In the telephone follow-up in April 2022, the patient’s recovery proceeded well.
Figure 1 (A and B) X-ray demonstrated that the left femoral head exhibited a strip-like low-density area (yellow arrow) but no evidence of stenosis. (C) CT revealed the left femoral head remains regular, the continuity of the upper bone cortex is poor, patchy low-density areas (red arrow) can be seen under the articular surface, edge hardening, and slightly high-density foci can be seen considering the formation of dead bone. (D and E) MRI revealed necrosis of the left femoral head, and effusion in the left joint cavity (blue arrow). (F) No obvious abnormality in Hip X-ray half a year after discharge.
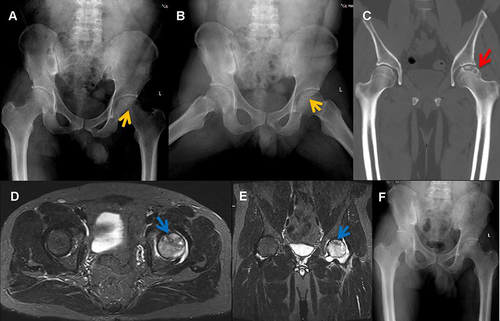
Figure 2 (A) Core biopsy of the right femoral head revealed necrotic material stained with HE. (B) Giemsa staining demonstrated scattered positive Brucella (red circle).
Case 2
The patient is a 33-year-old Chinese male. He was diagnosed with brucellosis in a local hospital in October 2017 due to right hip pain and wavy fever. Following the administration of anti-brucellosis drugs, the fever subsided, but the pain in the right hip did not. In January 2018, the patient visited the orthopedic department of our hospital due to aggravation of right hip pain and decreased hip joint mobility. History indicates that the patient’s family raised sheep for a long time, and there was no history of trauma, alcohol consumption, or hormone use. The physical examination revealed severe tenderness in the right hip region, longitudinal percussion pain in the right lower limb, and limited passive and active movement of the right hip. There was no abnormality in the chest X-ray or CT. X-ray of the hip joint showed low signal on the right femoral head, joint narrowing and even invagination of the joint space (). CT showed cavity necrosis and low-density patches of shadows in the right femoral head (). MRI of the hip joint indicates effusion of the right hip joint complicated by necrosis of the right femoral head, and the inflammatory fluid diffused with extra-articular (). Blood tests indicated WBC 4.60×109/L with neutrophils accounting for 61.1%, CRP59.3mg/L, ESR29.0mm/hr, and procalcitonin (PCT) 0.05ng/mL. T-SPOT.TB assay (T-SPOT), as well as serum anti-tuberculosis antibody tests, were negative. RBPT was positive, and SAT was positive at a titer of 1:640. The above examination eliminated tuberculosis, and a preliminary diagnosis of brucellar hip arthritis and osteonecrosis of the femoral head was made. Despite taking anti-brucellosis medications for two weeks, which included rifampicin (0.6g po qd; Guangdong Hengjian Pharmaceuticals), doxycycline (0.1g po bid; Jiangsu Lianhuan Pharmaceuticals), and levofloxacin (0.2g ivgtt bid; Yangtze River Pharmaceuticals), the right hip’s symptoms did not improve. This patient underwent puncture and irrigation of the right hip joint and core decompression with bone grafting of the femoral head. Using real-time PCR, B. melitensis was detected in joint effusions and osteonecrosis of the femoral head. HE staining in osteonecrosis of the femoral head revealed partial dead bone and inflammatory cellulose exudate (); Giemsa staining showed scattered positive Brucella (). When discharged from the hospital three weeks after surgery, the patient’s right hip pain was significantly reduced; blood tests showed a CRP level of 24.7mg/L and an ESR level of 18.00mm/hr. The antibiotic regimen was adjusted to rifampicin (0.6g po qd; Guangdong Hengjian Pharmaceuticals) and doxycycline (0.1g po bid; Jiangsu Lianhuan Pharmaceuticals) after discharge, with a total therapy duration of six months. Following a follow-up four years later, the pain in the right hip had completely disappeared, and the hip joint was no longer limited in movement; neither the blood tests nor the imaging examinations () revealed any abnormalities.
Figure 3 (A) X-ray of the Hip joint showed low signal on the right femoral head (yellow arrow), joint narrowing and even invagination of the joint space. (B) CT showed cavities necrosis and low-density patches of shadows (red arrow) in the right femoral head. (C) MRI showed effusion of the right Hip joint and necrosis of the right femoral head (blue arrow), and the inflammatory fluid diffused with extra-articular. (D–F) X-ray, CT and MRI of the osteonecrosis area four years later are better.
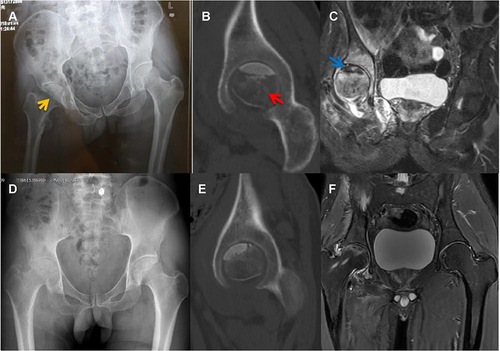
Figure 4 (A) HE staining showed partial dead bone and inflammatory cellulose exudate in osteonecrosis of the femoral head. (B) Giemsa staining revealed scattered positive Brucella (red circle).

Case 3
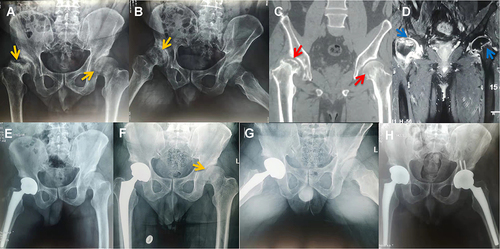
The patient is a 50-year-old Chinese male. He was admitted to the local hospital in November 2019 due to progressive right hip pain with left hip pain for five months. X-ray revealed that the right femoral head collapsed significantly, the joint space became narrow, and there were multiple areas of low density in the right femoral head; the left femoral head shape was regular, joint space was normal, and low-density area was visible in the left femoral head (). CT showed severe bilateral hip dysplasia, uneven bone density in the left femoral head, and a huge cavity in the right femoral head (). MRI of the hip joint showed bilateral effusion and bilateral osteonecrosis of the femoral head, particularly on the right side (). Blood tests revealed a WBC level of 4.70×109/L with neutrophils comprising 58.30%, CRP36.0mg/L, ESR52.00mm/hr. SAT was positive at a titer of 1:800. The patient was diagnosed with bilateral brucellar hip arthritis and bilateral osteonecrosis of the femoral head in the local hospital. Despite receiving anti-brucellosis medications for one month, his symptoms did not improve, and he was admitted to our orthopedics department for surgical treatment in December 2019. The patient had previously worked in a dairy factory for more than five years, and many of his colleagues suffered from brucellosis; he had no history of trauma, drinking, or hormone use. Physical examination revealed that both hips were tender, axial percussion was positive, active and passive hip movement was limited, especially on the right side, and a shortening deformity of the right lower limb is evident. In addition to hip joint puncture and irrigation, triple anti-infective therapy was administered after admission: rifampicin (0.6g po qd; Guangdong Hengjian Pharmaceuticals), doxycycline (0.1g po bid; Jiangsu Lianhuan Pharmaceuticals), and levofloxacin (0.2g ivgtt bid; Yangtze River Pharmaceuticals). Real-time PCR analysis of an effusion in the right hip joint revealed the presence of B. melitensis. We can confirm that Brucella is responsible for the necrosis of the right femoral head. Following three weeks of anti-brucellosis medications, inflammatory indexes returned to normal, and right total hip arthroplasty was performed (); the left femoral head was not treated since it has a regular shape. After being discharged from the hospital four weeks after the surgery, both hips were significantly less painful. The antibiotic regimen was adjusted to rifampicin (0.6g po qd; Guangdong Hengjian Pharmaceuticals) and doxycycline (0.1g po bid; Jiangsu Lianhuan Pharmaceuticals) after discharge; the total duration of the anti-brucellosis treatment is six months. This patient was hospitalized again in September 2020 due to progressive pain in the left hip, and all right hip symptoms had disappeared. Both the infection index and the SAT of the patients were standard; an X-ray of the hip joint indicated that the left femoral head collapsed and the joint space narrowed (). A left total hip arthroplasty was performed on the patient successfully. The patient’s symptoms disappeared entirely at the follow-up in January 2022; there were also no abnormalities in blood tests and X-ray of the hip (). The clinical characteristics of three patients are summarized in .
Table 1 The Clinical Characteristics of Three Patients
Figure 5 (A and B) Right femoral head collapsed significantly (yellow arrow), joint space narrowed, and multiple areas of low density were seen (yellow arrow) on X-ray; in the left femoral head, the shape and joint space were normal, and low-density areas (yellow arrow) were visible. (C) CT showed hyperplasia and sclerosis of the bilateral acetabular margins, uneven bone density in the left femoral head (red arrow), and a huge cavity in the right femoral head (red arrow). (D) MRI showed extra-articular inflammatory fluid, bilateral Hip joint effusion and bilateral osteonecrosis of the femoral head (blue arrow), especially on the right side. (E) Right total hip arthroplasty was performed when the inflammatory indexes normalized. (F and G) X-ray showed the left femoral head collapsed and joint space narrowed (yellow arrow). (H) No abnormalities in Hip X-ray at the follow-up in January 2022.
Discussion
The unique anatomical structure of the femoral head makes it more prone to ischemic necrosis than other bone tissues.Citation10 Aseptic and bacterial necroses are the two forms of osteonecrosis of the femoral head. Bacterial osteonecrosis of the femoral head is rare, requiring bacterial invasion and vascular obstruction.Citation1,Citation11 Staphylococcus aureus, Streptococcus, and Pseudomonas aeruginosa are the primary organisms responsible for orthopedic infection; bacteria like Brucella are relatively uncommon.Citation12–14. Suppurative osteomyelitis occurs when the bone becomes infected, and pus enters the Haversian canal and the bone’s perforating canal, obstructing the bone’s small nutritive arteries and disrupting the blood supply to the femoral head.Citation15,Citation16 There have only been three reports of osteonecrosis of the femoral head due to Brucella infection to date (): In the first two cases of osteonecrosis of the femoral head, Brucella was presumed as the likely cause due to a lack of diagnostic bases such as pathology and bacterial culture;Citation7,Citation8 in the third case, the diagnosis and treatment methods were outdated and the follow-up period was too short.Citation9 Our study confirmed that Brucella could cause osteonecrosis of the femoral head: Brucella was detected by Giemsa staining, and B. melitensis was identified by real-time PCR testing. This article contains more comprehensive information; the basis of bacterial osteonecrosis is more precise; we adopted individualized stepwise therapy according to the Ficat stages, the follow-up period is more extended, and the prognosis is well.
Table 2 Literature Review of Femoral Head Necrosis Due to Brucella Infection
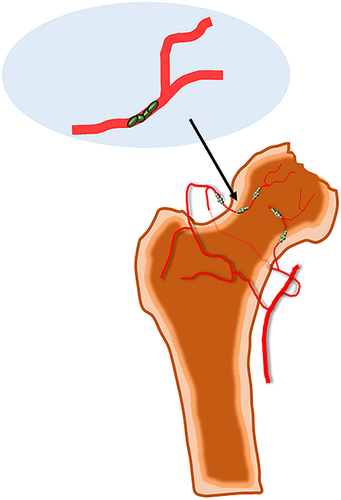
The diagnosis of femoral head necrosis was precise in these three patients based on the past epidemiological history, current medical history, physical examination, auxiliary imaging examination, and pathological results, but they were also complicated by bacterial hip arthritis. As the severity of brucellar hip arthritis in case 1 is less than that in cases 2 and 3, the joint space in case 1 is average, while the joint space in cases 2 and 3 is significantly reduced. We infer that the pathogenesis of this rare bacterial femoral head necrosis may include bacterial invasion, vascular blockage and destruction of synovial tissue (), the decrease of synovial fluid secretion and the destruction of inflammatory factors make articular cartilage lose nutrition, further soften, necrosis and exfoliate.
Figure 6 Rare bacterial avascular necrosis of the femoral head caused by Brucella infection, its pathogenesis may include bacterial invasion, vascular blockage and destruction of synovial tissue.
Brucellosis is a zoonotic disease worldwide; it is most prevalent in herders, slaughterhouse workers, and dairy farmers.Citation17–19 Internationally, there are six species of Brucella, with B. melitensis being the most common strain in China, followed by Brucella abortus (B. abortus) and Brucella suis (B. suis); B. melitensis is virulent, and the clinical symptoms of the patients are severe; the virulence of B. abortus is relatively weaker, and the clinical symptoms of the patients are mild.Citation20 Spondylitis and sacroiliitis are the most common manifestations of brucellosis when it invades the bone and joint, of which spondylitis is the most common manifestation.Citation6
There are three main types of laboratory detection of brucellosis: bacterial culture, serological detection, and molecular biological detection. Bacterial cultures are the gold standard for diagnosing brucellosis; however, the false-negative rate is high; bone marrow cultures are more sensitive than blood cultures.Citation21 Several serological tests are widely used, including RBPT, SAT, and enzyme-linked immunosorbent assay (ELISA). RBPT is mainly used for primary screening.Citation22 It is recommended by the World Health Organization (WHO) that the diagnostic criteria for SAT titer be set at 1:160, but the threshold should be set at 1:320 or higher in endemic regions; the titer of SAT is not physically related to infection, and it can remain high after the disease was cured.Citation23,Citation24 ELISA provides high sensitivity and specificity; it can monitor infection and curative effects.Citation25 Molecular biological detection entails using real-time PCR to identify strains.Citation26 It is recommended to use various detection methods to reduce the rate of missed diagnoses in patients with an epidemiological history.
For uncomplicated brucellosis, the antimicrobial regimen consisted of rifampicin and doxycycline for six weeks; treatment for brucellosis affecting the bone and joint system generally involves a triple regimen at least three months: rifampicin, doxycycline, and levofloxacin/ceftriaxone.Citation27,Citation28 These three patients were treated with antibiotics for half a year; they were followed for an extended period without recurrences or adverse effects.
Osteonecrosis of the femoral head may cause secondary osteoarthritis in the late stages due to the collapse of the femoral head and narrowing of the joint space, which inevitably leads to joint pain and loss of function.Citation29 Conservative treatment is appropriate for patients in Ficat stages I or IIa; the effect of core decompression is evident in patients with femoral head cysts and dead bone in Ficat stage IIb.Citation30,Citation31 Patients with Ficat stages III and IV are contraindicated for conservative treatment and require total hip arthroplasty in the majority of cases.Citation32 Following conservative treatment and core decompression, patients with osteonecrosis of the femoral head should undergo routine X-ray and computed tomography examinations; if the condition worsens, a total hip replacement may be necessary. In this paper, case 1 had Ficat stage IIb of the left femoral head; case 2 had Ficat stage IIb of the right femoral head; case 3 had Ficat stage IV of the right femoral head at the first admission and Ficat stage III of the left femoral head at the second admission. Brucellar hip arthritis with osteonecrosis of the femoral head is rare and does not have a standard treatment. Osteonecrosis may be exacerbated by tension within the hip joint caused by infection;Citation7–9 based on anti-infection combined with hip puncture and irrigation decompression, we provided individualized stepwise therapy for osteonecrosis of the femoral head according to the Ficat stage, and the prognosis of all three patients was well. Clinicians should be aware of the possibility of bacterial osteonecrosis of the femoral head in patients with an epidemiological history of brucellosis; osteonecrosis can result in severe complications if it is not diagnosed and treated at an early stage.
Conclusion
Brucella infection is a rare cause of femoral head necrosis. MRI and other tests should be performed in time to exclude femoral head necrosis when hip pain occurs in patients with an epidemic history of brucellosis. A timely diagnosis and individual stepwise treatment based on the Ficat stage can prevent osteonecrosis from progressing.
Patient Consent and Ethics Statement
The three patients provided informed consent for publication of this study and accompanying images. The Ethics Committee of the Beijing Ditan Hospital of Capital Medical University approved the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors have no conflicts of interest to declare in this work.
Additional information
Funding
References
- Cohen-Rosenblum A, Cui Q. Osteonecrosis of the femoral head. Orthop Clin North Am. 2019;50(2):139–149. doi:10.1016/j.ocl.2018.10.001
- Schaeffer EK, Ponton E, Sankar WN, et al.; International Hip Dysplasia (IHD) Study Group. Interobserver and intraobserver reliability in the salter classification of avascular necrosis of the femoral head in developmental dysplasia of the Hip. J Pediatr Orthop. 2022;42(1):e59–e64. doi:10.1097/BPO.0000000000001979.
- Briceño-Souza E, Méndez-Domínguez N, Cárdenas-Dajdaj R, Chin W, Huchim-Lara O. Dysbaric osteonecrosis associated with decompression sickness in a fishing diver. Undersea Hyperb Med. 2019;46:217–220.
- Katz K, Horev G, Grunebaum M, Yosipovitch Z. The natural history of osteonecrosis of the femoral head in children and adolescents who have Gaucher disease. J Bone Joint Surg Am. 1996;78(1):14–19. doi:10.2106/00004623-199601000-00003
- Munhoz lima ALL, Oliveira PR, Carvalho VC, et al. Osteonecrosis of the femoral head in people living with HIV: anatomopathological description and p24 antigen test. HIV AIDS. 2018;10:83–90. doi:10.2147/HIV.S162305
- Unuvar GK, Kilic AU, Doganay M. Current therapeutic strategy in osteoarticular brucellosis. North Clin Istanb. 2019;6(4):415–420. doi:10.14744/nci.2019.05658
- Wang P, Sun W, Shi L, Li T. Osteonecrosis of the femoral head due to brucellosis: a case report. BMC Infect Dis. 2020;20(1):202. doi:10.1186/s12879-020-4945-8
- Salarvand S, Nazer M, Shokri S, Bazhvan S, Pournia Y. Brucellosis-induced avascular necrosis of the hip in a middle-aged person. Iran J Public Health. 2012;41(12):86–88.
- Gedalia A, Howard C, Einhorn M. Brucellosis induced avascular necrosis of the femoral head in a 7 year old child. Ann Rheum Dis. 1992;51(3):404–406. doi:10.1136/ard.51.3.404
- Johnson EO, Soultanis K, Soucacos PN. Vascular anatomy and microcirculation of skeletal zones vulnerable to osteonecrosis: vascularization of the femoral head. Orthop Clin North Am. 2004;35(3):285–291. doi:10.1016/j.ocl.2004.03.002
- Wideman RF, Prisby RD. Bone circulatory disturbances in the development of spontaneous bacterial chondronecrosis with osteomyelitis: a translational model for the pathogenesis of femoral head necrosis. Front Endocrinol (Lausanne). 2013;3:183. doi:10.3389/fendo.2012.00183
- Urish KL, Cassat JE. Staphylococcus aureus osteomyelitis: bone, bugs, and surgery. Infect Immun. 2020;88(7):e00932–19. doi:10.1128/IAI.00932-19
- Griffin AT, Timbrook T, Harting J, Christensen D. Streptococcus anginosus group and osteomyelitis: a single centre clinical experience. Postgrad Med J. 2013;89(1051):262–265. doi:10.1136/postgradmedj-2012-131663
- Pliska NN. Pseudomonas aeruginosa as the main causative agent of osteomyelitis and its susceptibility to antibiotics. Drug Res. 2020;70(6):280–285. doi:10.1055/a-1150-2372
- Marx RE, Tursun R. Suppurative osteomyelitis, bisphosphonate induced osteonecrosis, osteoradionecrosis: a blinded histopathologic comparison and its implications for the mechanism of each disease. Int J Oral Maxillofac Surg. 2012;41(3):283–289. doi:10.1016/j.ijom.2011.12.016
- Sodnom-Ish B, Eo MY, Seo MH, Lee JH, Kim SM. Decompressive effects of draining tube on suppurative and sclerosing osteomyelitis in the jaw. BMC Musculoskelet Disord. 2021;22(1):469. doi:10.1186/s12891-021-04340-3
- Oyetola WD, Diallo K, Kreppel K, et al. Factors influencing the transborder transmission of brucellosis in cattle between Côte d’Ivoire and Mali: evidence from literature and current key stakeholders. Front Vet Sci. 2021;8:630580. doi:10.3389/fvets.2021.630580
- Acharya D, Hwang SD, Park JH. Seroreactivity and risk factors associated with human brucellosis among cattle slaughterhouse workers in South Korea. Int J Environ Res Public Health. 2018;15(11):2396. doi:10.3390/ijerph15112396
- Tulu D. Bovine brucellosis: epidemiology, public health implications, and status of brucellosis in Ethiopia. Vet Med. 2022;13:21–30. doi:10.2147/VMRR.S347337
- Deng Y, Liu X, Duan K, Peng Q. Research progress on brucellosis. Curr Med Chem. 2019;26(30):5598–5608. doi:10.2174/0929867325666180510125009
- Basu S, Shetty A. Laboratory diagnosis of tropical infections. Indian J Crit Care Med. 2021;25(Suppl 2):S122–S126. doi:10.5005/jp-journals-10071-23813
- Tadesse G. Brucellosis seropositivity in animals and humans in Ethiopia: a meta-analysis. PLoS Negl Trop Dis. 2016;10(10):e0005006. doi:10.1371/journal.pntd.0005006
- Hasanjani Roushan MR, Moulana Z, Mohseni Afshar Z, Ebrahimpour S. Risk factors for relapse of human Brucellosis. Glob J Health Sci. 2015;8(7):77–82. doi:10.5539/gjhs.v8n7p77
- Roushan MR, Amiri MJ, Laly A, Mostafazadeh A, Bijani A. Follow-up standard agglutination and 2-mercaptoethanol tests in 175 clinically cured cases of human brucellosis. Int J Infect Dis. 2010;14(3):e250–3. doi:10.1016/j.ijid.2009.05.008
- Xu N, Wang W, Chen F, Li W, Wang G. ELISA is superior to bacterial culture and agglutination test in the diagnosis of brucellosis in an endemic area in China. BMC Infect Dis. 2020;20(1):11. doi:10.1186/s12879-019-4729-1
- Ali Ahmadi M, Saadati D, Najimi M, Ganjali H, Shah Karami F. Comparison of PCR and conventional serological methods for detection of Brucella spp. in ovine and caprine blood serum. Arch Razi Inst. 2021;76(3):445–452. doi:10.22092/ari.2020.128449.1415
- Vollmar P, Zange S, Zöller L, Erkel J, Robert Thoma B. Brucellose [Brucellosis, an overview and current aspects]. Dtsch Med Wochenschr. 2016;141(14):1014–1018. German. doi:10.1055/s-0042-101723
- Shakir R. Brucellosis. J Neurol Sci. 2021;420:117280. doi:10.1016/j.jns.2020.117280
- Larson E, Jones LC, Goodman SB, Koo KH, Cui Q. Early-stage osteonecrosis of the femoral head: where are we and where are we going in year 2018? Int Orthop. 2018;42(7):1723–1728. doi:10.1007/s00264-018-3917-8
- Martinot P, Dartus J, Justo A, et al.; French Society of Orthopaedic Surgery and Traumatology (SoFCOT). Does augmented core decompression decrease the rate of collapse and improve survival of femoral head avascular necrosis? Case-control study comparing 184 augmented core decompressions to 79 standard core decompressions with a minimum 2 years’ follow-up. Orthop Traumatol Surg Res. 2020;106(8):1561–1568. doi:10.1016/j.otsr.2020.03.040
- Grassi M, Salari P, Massetti D, Papalia GF, Gigante A. Treatment of avascular osteonecrosis of femoral head by core decompression and platelet-rich plasma: a prospective not controlled study. Int Orthop. 2020;44(7):1287–1294. doi:10.1007/s00264-020-04628-4
- Erivan R, Caputo T, Riouach H, et al. Primary total hip replacement in Ficat-Arlet stage 3 and 4 osteonecrosis: a retrospective study at a minimum 12-year follow-up. Eur J Orthop Surg Traumatol. 2020;30(5):845–850. doi:10.1007/s00590-020-02644-z