
Abstract
Aim
Skeletal involvement of Cryptococcus neoformans is rare and normally associated with disseminated cryptococcosis or potential predisposing factors. Here, we report an atypical case of osteoarticular cryptococcosis in an immunocompetent patient.
Case Presentation
We report a case of cryptococcal osteomyelitis in a 45-year-old female who presented with swelling and pain in the left inner thigh. After a biopsy of the pubic bone and surrounding soft tissue, the pathological results and bacterial culture of the biopsy tissue confirmed Cryptococcus neoformans infection. After draining the pus by aspiration and administering oral fluconazole (400 mg/d) treatment, the patient’s symptoms disappeared.
Conclusion
Cryptococcus neoformans is a rare etiology of infection of the entire pubis, and oral fluconazole and pus aspiration could benefit some cryptococcal osteomyelitis patients with soft-tissue cryptococcal infection.
Introduction
Cryptococcus neoformans is an encapsulated yeast organism that can cause severe illness or death in immunocompromised patients.Citation1 Cases most frequently involve the central nervous system or the lungs, but multiple other sites of infection have been documented, including the skin,Citation2 kidneys,Citation3 prostate,Citation4 eyes,Citation5 sinusesCitation6 and colon.Citation7 Approximately 5% of all cryptococcal infections present with osteomyelitis.Citation8,Citation9 Predisposing factors for cryptococcal osteomyelitis include solid organ transplant, immunosuppressant medication use, diabetes mellitus and HIV.Citation8 The symptoms, signs and imaging findings of patients with cryptococcal infection are often difficult to distinguish from tumors and bacterial infections. Here, we report a case of Cryptococcus neoformans infection of the pubic bone and soft tissue without involvement of the lung and central nervous system and with normal immune function. To the best of our knowledge, this is the only case of cryptococcal osteomyelitis of the pubis reported in the past 5 years. Written informed consent of the patient was obtained for the publication of this case report and the accompanying images. Ethical approval was also acquired.
Case Report
A 45-year-old female was hospitalized due to pain and swelling in the medial left thigh for one month. The patient is a farmer, and the neighbors raise pigeons. One month prior, she had no obvious inducement for the unbearable pain and swelling of the left thigh. Cupping and acupuncture methods had no obvious effect. The size of the mass gradually increased, so she came to the hospital. A physical examination showed that the skin temperature on the surface of the mass was increased, and the tenderness was obvious. The patient had no fever, a normal heart rate and cardiac examination, and she had high blood pressure for more than 10 years.
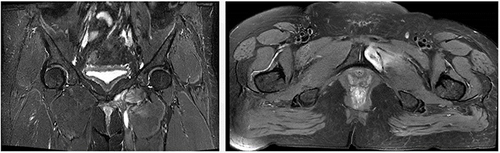
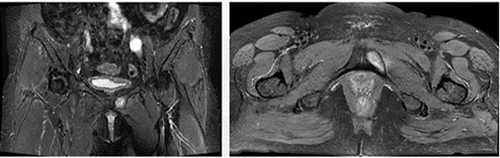
After entering the hospital, the laboratory examination revealed WBC: 10.89*109/L, RBC: 4.50*1012/L, and albumin: 33.9 g/L. The immune function of the patient was normal, and she had no history of HIV, immunosuppressive therapy or diabetes. MRI of the pelvis suggested that the soft tissue mass in the left inguinal region and the bone destruction of the left inferior pubic branch should be considered malignant tumors, and infectious lesions should not be excluded (). CT imaging of the lesion also suggested that the patient suffered from a tumor, and the lesion contained some pus. Subsequently, we carried out a soft tissue biopsy under the guidance of B-ultrasound, and a small amount of tissue and a large amount of blood-red sticky fluid were obtained in the process. We gave the patient cephalosporin antibiotics, but her symptoms did not show a significant improvement. Re-examination of the indicators of inflammatory infection revealed CRP: 36.4 mg/L, ESR: 54 mm/h, PCT: 0.06 ng/mL, and IL-6: 12.95 pg/mL. We also performed a biopsy of the pubic lesions, and Cryptococcus neoformans was found in the bacterial culture of the biopsy tissue. The drug sensitivity results showed that the lesion was sensitive to AMB, 5-FC and fluconazole. Pathology after biopsy showed a fungal infection with mild dysplasia of histiocytic cells (). After an imaging examination of the brain and lungs, no special lesions were found, so cryptococcal infection in the central nervous system and lungs was excluded. After receiving the bacterial culture results, fluconazole (400 mg/d) was taken orally for 4 weeks. During the 4-week oral fluconazole treatment, the wound was broken (), so pus aspiration was performed on the tumor on the inside of the thigh, and cephalosporins were used to control the infection. Four weeks after taking fluconazole, re-examination MRI showed that the mass on the medial side of the left thigh and the pubic lesions had decreased in size ().
Figure 1 MRI presented lesions of the pubis and surrounding soft tissue.
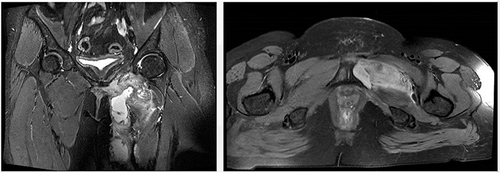
Figure 2 Pathology results showed fungal infection with mild dysplasia of histiocytic cells.
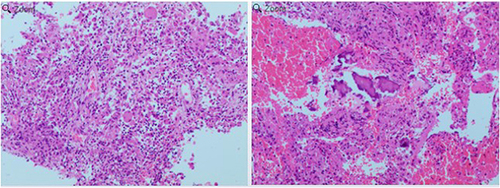
Figure 3 The appearance of the affected limb between different periods. (A) Broken biopsy wound, oozing viscous liquid. (B) After 12 weeks of treatment with oral fluconazole, the patient’s symptoms disappeared.
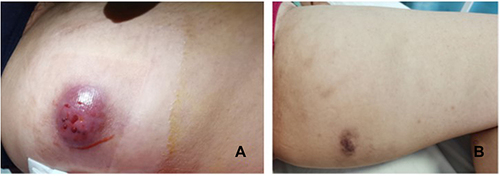
Figure 4 After 4 weeks of oral fluconazole treatment, the pubic lesions decreased in size.
The patient continued to take fluconazole (400 mg/d) orally for 12 weeks after discharge. Then, she went to the hospital for re-examination and found that the medial thigh and pubic lesions had basically disappeared (), and the swelling of the patient’s left thigh had disappeared (). At the 2-year follow-up, the patient was doing well. There were no complications or recurrences, the WBC count was normal, and the ESR and CRP were normal. After 12 weeks of oral fluconazole (400 mg/d) treatment, the pubic lesions and surrounding soft-tissue lesions disappeared.
Figure 5 After 12 weeks of oral fluconazole treatment, the pubic lesions basically disappeared.
Discussion
While the capsule produced by virulent strains of Cryptococcus neoformans under appropriate conditions is an important virulence factor, capsule material would not cause the disease on its own. There are two kinds of common pathogenic Cryptococcus, namely, Cryptococcus neoformans and Cryptococcus gattii, among which Cryptococcus neoformans infection is the most common.Citation10,Citation11 Because Cryptococcus is an opportunistic pathogen,Citation12 with the gradual increase in the population base of the so-called “vulnerable population”, Cryptococcus infection has become an important infectious disease. Cryptococcus neoformans can cause opportunistic infections in immunocompromised patients; however, 10% to 40% of infections occur in patients without known immune deficiencies.Citation13 Cryptococcus neoformans mainly lives in pigeons and weathered feces in soil, but fungi are not normal flora in soil.Citation14 Detection of Cryptococcus neoformans mainly uses etiological detection. There are three main methods: ink staining, fungal culture and identification and cryptococcal antigen detection.
Cryptococcosis is an infectious disease caused by Cryptococcus neoformans or Cryptococcus gattii. The lung and central nervous system are prone to Cryptococcus neoformans infection, while other less common body infections include skin, eyes and bones/joints.Citation14 The site of infection can be transmitted through blood, continuous transmission or direct vaccination. Apart from direct vaccination, animal-to-human or human-to-animal transmission is not known.Citation15 In the case we reported, pigeons were raised in the neighbor’s home; furthermore, the patient often had low back pain due to lumbar disc herniation, which sometimes resulted in cupping and acupuncture performed on her back and legs. We suspect that the skin barrier was damaged after cupping or acupuncture, so cryptococcus infection occurred after possible contact with soil contaminated by birds such as pigeons.
Bone invasion of cryptococcosis is usually characterized by localized osteolytic lesions of any piece of bone in the body, but the most common is the spine.Citation14,Citation16 Adjacent bones or joints and infected soft tissue can spread continuously. The clinical symptoms and radiological manifestations of skeletal cryptococcosis are nonspecific. Fungal bone infection can show a wide range of symptoms and onset times, depending on the pathogenicity of the potential organism, the site of infection and the potential health status of the patient. It has been reported that cryptococcal bone infection can lead to subperiosteal new bone formation, periosteal reaction and imaging manifestations of osteomyelitis.Citation17 However, the imaging findings of cryptococcal osteomyelitis usually have no typical features and can also show well-defined osteolytic lesions, similar to malignant tumors.Citation14,Citation16–18 Meanwhile, most patients with cryptococcal osteomyelitis show soft tissue swelling and tenderness.Citation17 Since cryptococcal infections are rare and generally subacute, the most important aspect of diagnosing these infections is to include them in differential diagnosis, especially in patients with normal immune function. It is worth noting that as many as 20% of cryptococcosis cases occur in patients with a “normal” phenotype or obvious immunity, and there are no known risk factors for infection.Citation19 Therefore, an accurate diagnosis of cryptococcosis could require various methods, such as imaging, histopathology, and microbe examination of lesion specimens. As cryptococcosis tends to occur in patients with abnormal immune function, some patients must have their immune function detected for diagnosis. The tests include an examination of autoantibodies, the complement system, and liver and kidney function.
Although Cryptococcus neoformans is distributed across most of the globe, the limited history of the treatment of Cryptococcus neoformans remains a major challenge. Apart from lung and central nervous system infections, there is no standardized treatment for cryptococcal infections in specific body parts. The combination of antifungal therapy and surgical debridement has been used to treat many patients with bone cryptococcal infections.Citation15,Citation17,Citation20,Citation21 According to the American Society for Infectious Diseases, oral fluconazole (400 mg/d for 6–12 months) is the first choice for nonmeningeal, nonpulmonary cryptococcosis patients with normal immune function.Citation16,Citation17,Citation22 Patients with disseminated diseases (involving at least two nonadjacent sites) should be given amphotericin B liposomes (3~4 mg/kg/d) plus flucytosine 100 mg/kg/d 4 times orally for at least 2 weeks. This is followed by a consolidation phase, with fluconazole 12 mg/kg taken daily for 8 weeks. Maintenance therapy includes fluconazole 200–400 mg/d for at least one year. Although the prognosis of disseminated cryptococcosis is usually poor, patients with isolated osteomyelitis with normal immune function have a good prognosis.Citation17,Citation23
It has also been reported that there is a very restricted number of antifungal drugs that are currently clinically available for the treatment of invasive fungal infections—polyenes, azoles, echinocandins, and flucytosine.Citation24 Most antifungal drugs have few side effects and complications during long-term antifungal therapy. The major drawback of amphotericin B has always been its toxicity, particularly its nephrotoxicity, which can lead to kidney failure.Citation24 Azoles are some of the most commonly used antifungal drugs for the treatment of a variety of fungal infections, but some fungal species display intrinsic (or primary) resistance to fluconazole. A major problem with flucytosine is the extremely common occurrence of the development of resistance, and because of this, it is never used in monotherapy but rather in combination with other antifungals.Citation25 In addition, hepatotoxicity and hematological toxicity are common adverse effects at target concentrations.Citation26
A literature review was performed by searching PubMed and Web of Science for articles in the last five years containing the terms ‘Cryptococcus’ and ‘osteomyelitis’. We found approximately 28 cases of cryptococcal osteomyelitis, and the clinical characteristics and treatments are listed in .
Table 1 Summary of 28 Cases of Cryptococcosis of the Bones in the Last Five Years
After our case was diagnosed as a tumor in the early stage, we performed a biopsy and found that there was a large amount of fluid in the tumor. Then, we extracted the fluid from the tumor for bacterial culture, and finally, Cryptococcus neoformans was cultured. The pathological results also confirmed that the pubic focus was fungal infection. In our case, we used oral fluconazole treatment (400 mg/d); however, the puncture wound of the patient was broken, so we emptied the pus by aspiration and did not operate on the pubic lesion. After 3 months of oral fluconazole (400 mg/d) and pus aspiration, the symptoms of the patient almost completely disappeared, and after follow-up, there were no more symptoms.
In summary, we report the first case of isolated cryptococcal osteomyelitis of the pubis with surrounding soft-tissue cryptococcal infection in an immunocompetent patient in recent years. Patients with isolated cryptococcal osteomyelitis of the pubis and surrounding soft-tissue cryptococcal infection may be cured with oral fluconazole and surgery, especially in some special cases; for example, in patients presenting only soft-tissue swelling and plentiful pus. Cryptococcosis therapy should be aimed at multiple factors, such as the size of the lesion and host immune conditions. We suggest that it is necessary to culture biopsy specimens, even in clinical cases in which a tumor is often suspected. This case can serve as a reminder of the many ways cryptococcal infection may be disguised and the usefulness of proper diagnostic procedures.
Abbreviations
NA, not available; 5-FC, 5-fluorocytosine; Flu, fluconazole; Vor, Voriconazole; LPL, lymphoplasmacytic lymphoma; TB, tuberculosis, SLE, systemic lupus erythematosus; DM, diabetes mellitus.
Data Sharing Statement
All data (image and table) used in this study are included in this published article. We do not have metadata sharing, thus, it is not applicable to this article.
Ethics Approval
The ethical approval was acquired by applying for the medical ethics committee of Zhongnan Hospital.
Consent for Publication
The patient gave written informed consent to the publication of her history and photographs.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Casadevall A, Coelho C, Cordero RJB, et al. The capsule of Cryptococcus neoformans. Virulence. 2019;10(1):822–831. doi:10.1080/21505594.2018.1431087
- Saini AG, Patil S, Agrawal T, et al. Systemic cryptococcosis in an immune-competent child. J Infect Public Health. 2018;11(3):436–438. doi:10.1016/j.jiph.2017.09.015
- Espinosa Saltaren L, Andrade Perez R. Renal Cryptococcosis. N Engl J Med. 2020;383(24):2371. doi:10.1056/NEJMicm2007464
- Epstein DJ, Thompson LDR, Saleem A, Kao CS, Epstein JI. Fungal prostatitis due to endemic mycoses and Cryptococcus: a multicenter case series. Prostate. 2020;80(12):1006–1011. doi:10.1002/pros.24034
- Alzahrani YA, Aziz HA, Shrestha NK, Biscotti CV, Singh AD. Cryptococcal iridociliary granuloma. Surv Ophthalmol. 2016;61(4):498–501. doi:10.1016/j.survophthal.2015.12.005
- Prendiville S, Bielamowicz SA, Hawrych A, Deeb ZE. Isolated cryptococcal sphenoid sinusitis with septicemia, meningitis, and subsequent skull base osteomyelitis in an immunocompetent patient. Otolaryngol Head Neck Surg. 2000;123(3):277–279. doi:10.1067/mhn.2000.104777
- Law JK, Amar JN, Kirby SD, Zetler PJ, Enns RA. Colonic cryptococcus infection. Gastrointest Endosc. 2007;65(3):525–526. doi:10.1016/j.gie.2006.08.043
- Lai KK, Rosenberg AE, Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 19-1999. A 55-year-old man with a destructive bone lesion 17 months after liver transplantation. N Engl J Med. 1999;340(25):1981–1988. doi:10.1056/NEJM199906243402508
- Shrader SK, Watts JC, Dancik JA, Band JD. Disseminated cryptococcosis presenting as cellulitis with necrotizing vasculitis. J Clin Microbiol. 1986;24(5):860–862. doi:10.1128/jcm.24.5.860-862.1986
- Zhao Y, Lin J, Fan Y, Lin X. Life Cycle of Cryptococcus neoformans. Annu Rev Microbiol. 2019;73(1):17–42. doi:10.1146/annurev-micro-020518-120210
- Knoke M, Schwesinger G. One hundred years ago: the history of cryptococcosis in Greifswald. Medical mycology in the nineteenth century. Mycoses. 1994;37(7–8):229–233. doi:10.1111/j.1439-0507.1994.tb00418.x
- Jung KW, Lee KT, So YS, Bahn YS. Genetic manipulation of cryptococcus neoformans. Curr Protoc Microbiol. 2018;50(1):e59. doi:10.1002/cpmc.59
- Bariteau JT, Waryasz GR, McDonnell M, Fischer SA, Hayda RA, Born CT. Fungal osteomyelitis and septic arthritis. J Am Acad Orthop Surg. 2014;22(6):390–401. doi:10.5435/JAAOS-22-06-390
- Maziarz EK, Perfect JR. Cryptococcosis. Infect Dis Clin North Am. 2016;30(1):179–206. doi:10.1016/j.idc.2015.10.006
- Jain D, Najjar M, Azher Q, Bachuwa G. Cryptococcal sternal osteomyelitis in a healthy woman: a review of Cryptococcus neoformans. BMJ Case Rep. 2013;2013:bcr2013009129–bcr2013009129. doi:10.1136/bcr-2013-009129
- Perfect JR, Dismukes WE, Dromer F, et al. Clinical practice guidelines for the management of cryptococcal disease: 2010 update by the infectious diseases society of America. Clin Infect Dis. 2010;50(3):291–322. doi:10.1086/649858
- Zhou HX, Lu L, Chu T, et al. Skeletal cryptococcosis from 1977 to 2013. Front Microbiol. 2014;5:740. doi:10.3389/fmicb.2014.00740
- Witte DA, Chen I, Brady J, Ramzy I, Truong LD, Ostrowski ML. Cryptococcal osteomyelitis. Report of a case with aspiration biopsy of a humeral lesion with radiologic features of malignancy. Acta Cytol. 2000;44(5):815–818. doi:10.1159/000328567
- Shourian M, Qureshi ST. Resistance and tolerance to cryptococcal infection: an intricate balance that controls the development of disease. Front Immunol. 2019;10:66. doi:10.3389/fimmu.2019.00066
- Medaris LA, Ponce B, Hyde Z, et al. Cryptococcal osteomyelitis: a report of 5 cases and a review of the recent literature. Mycoses. 2016;59(6):334–342. doi:10.1111/myc.12476
- Ramkillawan Y, Dawood H, Ferreira N. Isolated cryptococcal osteomyelitis in an immune-competent host: a case report. Int J Infect Dis. 2013;17(12):e1229–1231. doi:10.1016/j.ijid.2013.04.013
- Zhou HX, Ning GZ, Feng SQ, et al. Cryptococcosis of lumbar vertebra in a patient with rheumatoid arthritis and scleroderma: case report and literature review. BMC Infect Dis. 2013;13:128. doi:10.1186/1471-2334-13-128
- Qadir I, Ali F, Malik UZ, Umer M. Isolated cryptococcal osteomyelitis in an immunocompetent patient. J Infect Dev Ctries. 2011;5(9):669–673. doi:10.3855/jidc.1352
- Wall G, Lopez-Ribot JL. Current antimycotics, new prospects, and future approaches to antifungal therapy. Antibiotics. 2020;9(8). doi:10.3390/antibiotics9080445
- Viviani MA. Flucytosine--what is its future? J Antimicrob Chemother. 1995;35(2):241–244. doi:10.1093/jac/35.2.241
- Vermes A, Guchelaar HJ, Dankert J. Flucytosine: a review of its pharmacology, clinical indications, pharmacokinetics, toxicity and drug interactions. J Antimicrob Chemother. 2000;46(2):171–179. doi:10.1093/jac/46.2.171
- Zhang C, Wang C, Chen F, et al. Metagenomic next-generation sequencing technique helps identify cryptococcal infection in the rib: a report of 2 cases and review of the literature. JBJS Case Connect. 2019;9(4):e0367. doi:10.2106/JBJS.CC.19.00367
- Ma JL, Liao L, Wan T, Yang FC. Isolated cryptococcal osteomyelitis of the ulna in an immunocompetent patient: a case report. World J Clin Cases. 2022;10(19):6617–6625. doi:10.12998/wjcc.v10.i19.6617
- Pudipeddi AV, Liu K, Watson GF, Davis RJ, Strasser SI. Cryptococcal osteomyelitis of the skull in a liver transplant patient. Transpl Infect Dis. 2016;18(6):954–956. doi:10.1111/tid.12602
- Ghioldi ME, Dealbera ED, Chemes LN, Caballero GA, Del Vecchio JJ. Cryptococcus neoformans osteomyelitis of the calcaneus: case report and literature review. SAGE Open Med Case Rep. 2021;9:2050313X211027094. doi:10.1177/2050313X211027094
- Onishi O, Kida Y, Kiba T, et al. Cryptococcal osteomyelitis of the entire humerus: a case report. JBJS Case Connect. 2020;10(4):e2000279. doi:10.2106/JBJS.CC.20.00279
- Deus G, Gomez-Zorrilla S, Echeverria-Esnal D, et al. Osteoarticular cryptococcosis successfully treated with high-dose liposomal amphotericin B followed by oral fluconazole. Infect Drug Resist. 2021;14:719–722. doi:10.2147/IDR.S294299
- Chen WA, Emory CL, Graves BR. Disseminated Cryptococcal Osteomyelitis to the Hand in an Immunosuppressed Lymphoma Patient. J Hand Surg Am. 2018;43(3):291e291–291 e296. doi:10.1016/j.jhsa.2017.07.013
- Dumenigo A, Sen M. Cryptococcal Osteomyelitis in an Immunocompetent Patient. Cureus. 2022;14(1):e21074. doi:10.7759/cureus.21074
- Lai Q, Liu Y, Yu X, et al. Diagnosis and treatment of nonadjacent cryptococcal infections at the L1 and S1 vertebrae. Orthopade. 2017;46(1):85–89. doi:10.1007/s00132-016-3349-3
- Marino A, Caltabiano E, Zagami A, et al. Rapid emergence of cryptococcal fungemia, Mycobacterium chelonae vertebral osteomyelitis and gastro intestinal stromal tumor in a young HIV late presenter: a case report. BMC Infect Dis. 2018;18(1):693. doi:10.1186/s12879-018-3573-z
- Delat R, Laheri V. Bifocal cryptococcal osteomyelitis in an immunocompetent male. J Orthop Case Rep. 2016;6(5):17–19. doi:10.13107/jocr.2250-0685.610
- Ramesh V, Rao Polati V, Nimmala P, Anand M, Narreddy S, Saidulu G. An unusual cause for rib osteomyelitis in the tropics: cryptococcal osteomyelitis. Trop Doct. 2020;50(4):361–365. doi:10.1177/0049475520929827
- Adiwardana NS, Moras JA, Bernardo LL, Klautau GB, Queiroz W, Vidal JE. Chronic skull osteomyelitis due to Cryptococcus neoformans: first case report in an HIV-infected patient. Braz J Infect Dis. 2018;22(6):499–502. doi:10.1016/j.bjid.2018.11.004
- Sang J, Yang Y, Fan Y, et al. Isolated iliac cryptococcosis in an immunocompetent patient. PLoS Negl Trop Dis. 2018;12(3):e0006206. doi:10.1371/journal.pntd.0006206
- Matsuki T, Miyamoto S, Yamashita T. Cryptococcal osteomyelitis of the Zygomatic bone: a case report. BMC Infect Dis. 2020;20(1):399. doi:10.1186/s12879-020-05123-2
- Inoue H, Motohashi T, Ioku Y, Watanabe M, Nakajima M, Sugitatsu M. The detection of Cryptococcus in skeletal infection after tooth extraction in an acute myeloid leukemia patient. IDCases. 2020;19:e00700. doi:10.1016/j.idcr.2020.e00700
- Schrader A, Melicoff E, Munoz F, Mallory GB, Curry CV, Gazzaneo MC. Diagnosis and treatment of cryptococcal osteomyelitis in a pediatric lung transplant patient. Pediatr Transplant. 2022;26(2):e14165. doi:10.1111/petr.14165
- Li Z, Liang J, Shen J, Qiu G, Weng X. Thoracolumbar scoliosis due to cryptococcal osteomyelitis: a case report and review of the literature. Medicine. 2016;95(5):e2613. doi:10.1097/MD.0000000000002613
- Wang R, Luo H, Xin X, Qin B, Huang W. Disseminated cryptococcal infection of the lumbar Spine in an immunocompetent man. Infect Drug Resist. 2022;15:4229–4234. doi:10.2147/IDR.S359612
- Poenaru SM, Rofaiel R, Hosseini-Moghaddam SM. Cryptococcus neoformans osteomyelitis and intramuscular abscess in a liver transplant patient. BMJ Case Rep. 2017;2017. doi:10.1136/bcr-2017-221650
- Ahn JH, Park C, Lee CW, Kim YC. Cryptococcal osteomyelitis of the first metatarsal head in an immunocompetent patient. J Am Podiatr Med Assoc. 2017;107(3):248–252. doi:10.7547/16-067
- Pereira-Duarte M, Camino G, Estefan M, Kido G, Sola C, Gruenberg M. Criptococosis vertebral. Comunicación de un caso y revisión bibliográfica [Vertebral cryptococosis. Case report and literature review]. Rev Chilena Infectol. 2019;36(5):656–662. Spanish. doi:10.4067/S0716-10182019000500656