
Abstract
Intracranial infections are the most serious and common postoperative complications with significant mortality and morbidity. Myroides odoratimimus (M. odoratimimus), a Gram-negative environmental species and an opportunistic microorganism, predominantly infects immunocompromised individuals. Limited clinical experiences and documented multidrug resistance have resulted in a scarcity of data on the treatment of M. odoratimimus infections. As far as we know, this is the first reported case of an intracranial M. odoratimimus infection with external ventricular drains (EVD) that was effectively treated with a combination of intravenous and intraventricular tigecycline in an immunocompetent adult host.
Introduction
The incidence of central nervous system (CNS) infections after neurosurgical operations is about 4.6% to 25%.Citation1 Infections associated with external ventricular drains (EVD) occur at a rate of 11.4 cases per 1000 catheter days.Citation2 Gram-negative and gram-positive bacteria are the leading causative agents of intracranial infections. The Myroides genus comprises non-motile, aerobic, gram-negative bacteria, among which M. odoratimimus is an opportunistic pathogen that primarily affects immunocompromised individuals.Citation3,Citation4 While there are growing cases of clinically relevant M. odoratimimus infections in immunocompetent individuals generally affecting the skin, soft tissues, urinary tract and blood.Citation5–7 Selecting optimal antibiotic therapy for M. odoratimimus infections is challenging due to its high antimicrobial resistance.Citation8,Citation9 Here, we present a rare case of an immunocompetent patient who developed intracranial M. odoratimimus infection following EVD placement, which was successfully treated using a combination of intravenous and intraventricular tigecycline. Clinicians should be aware of the potential for infection with this pathogen, and tigecycline can be a viable option for severe M. odoratimimus infections based on antimicrobial susceptibility testing results.
Case Presentation
A 55-year-old woman weighing 52 kg with a past medical history of hypertension underwent intracranial hematoma removal for acute cerebral hemorrhage and hernia at a local hospital half a month ago. The patient was admitted to our hospital in May 2022 with severe coma and difficulty weaning from ventilation. Physical examination revealed that the patient was on mechanical ventilation without spontaneous respiration, had a Glasgow Coma Scale (GCS) score of 3 points, dilated and fixed pupils with no light reflex, and negative neuropathological reflexes including head eye reflex, corneal reflex, and Babinski sign. Brain computed tomography (CT) scan revealed severe hydrocephalus and interstitial brain edema (). Cerebrospinal fluid (CSF) was obtained via lumbar puncture showed a white blood cell count (WBC) of 60/μL (61% neutrophil granulocytes), a total protein level of 97.5 mg/dL, and a glucose level of 2.45mmol/L, while the simultaneous blood glucose level was 10.3mmol/L, and CSF cultures was negative (). It was noted that she had pneumonia and intestinal infection meanwhile, a 10-day course of piperacillin-tazobactam (Tazocin, Wyeth Lederle S.R.L.) 4.5g intravenously (IV) over 2h 4 times daily was prescribed. Endoscopic third ventriculostomy and left EVD was performed on the 13th day of hospitalization after controlling the pneumonia and intestinal infection. Empirical administration of meropenem (2g IV q8h, Beineng, Shenzhen Haibin Pharmaceutical Co. Ltd) was initiated after the surgery, and the patient was successfully weaned off the ventilator, although brain CT scan still suggested hydrocephalus and interstitial brain edema ().
Table 1 Cerebrospinal Fluid Tests and Culture During Hospitalization
Figure 1 Brain CT before and after endoscopic third ventriculostomy and left EVD. (A) Brain CT scan on admission showing severe hydrocephalus and interstitial brain edema; (B) brain CT scan after endoscopic third ventriculostomy and left EVD in our hospital; (C) brain CT about one month after endoscopic third ventriculostomy and left EVD showing improvement of interstitial cerebral edema, but hydrocephalus was still present; (D) brain CT after a new right EVD was placed due to deterioration of intracranial Myroides odoratimimus infection while hydrocephalus was significantly better than before. Red arrow: catheter of EVD.
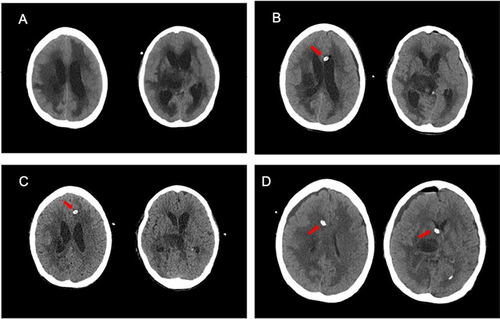
On the 24th day of hospitalization, the patient developed fever and neck stiffness. Laboratory analysis of CSF obtained via the EVD showed a WBC of 30/μL (75% neutrophil granulocytes), a total protein level of 303.2 mg/dL, and a glucose level of 2.86 mmol/L (the simultaneous blood glucose level was 7.8mmol/L), a chloride level of 114mmol/L. The CSF culture identified Klebsiella acidophilus, which was resistant to carbapenem but susceptible to amikacin. Consequently, intravenous amikacin (200 mg q12h, Amikacin Sulfate Injection, Chengyi Pharmaceutical Co. LTD) was administered in combination with intracerebral ventricular injection (ICV, 30 mg qd). However, on the 31st day of hospitalization, CSF obtained via the EVD showed a WBC of 961/μL (80% polymorphonuclear leukocytes), a total protein level of 283.6 mg/dL, and a glucose level of 1.35mmol/L (the simultaneous blood glucose level was 9.77 mmol/L), a chloride level of 111.1mmol/L, indicating a deterioration of the infection. Therefore, the antibiotics were switched to colistin IV (750,000u over 2h q12h, Colistin Sulfate for Injection, Shanghai SPH New Asia Pharmaceutical Co. LTD) in combination with ICV (100,000u qd). During the follow-up period, the patient’s fever gradually subsided, and the CSF analysis showed a decrease in leukocyte count to 65/μL (10% polymorphonuclear leukocytes), a decline in total protein level to 133.1 mg/dL, and an increase in glucose levels to 5.06 mmol/L (the simultaneous blood glucose level was 7.2mmol/L). Three consecutive CSF cultures were negative (), allowing for discontinuation of antibiotics. A brain CT scan () revealed improvement in interstitial cerebral edema, although hydrocephalus persisted, and CSF drainage from the EVD tube exceeded 200 mL per day, necessitating prolonged retention of the EVD. At that time, the patient exhibited spontaneous respiratory triggers, a Glasgow Coma Scale score of 4 points, and bilateral pupil reduction with slow light response.
Unfortunately, on the 49th day of hospitalization, the patient experienced a resurgence in body temperature (increased to 40.5°C) accompanied by sepsis, the blood WBC increased to 39.95×109/L, C-reactive protein (CRP) was 146.2mg/L and procalcitonin (PCT) was 8.07ng/mL. CSF culture showed M. odoratimimus (conventional culture and metagenomic next-generation sequencing/mNGS) which was only susceptible to tigecycline (). The blood culture showed growth of Trichosporon asahii. To treat the infections, the patient was administered a combination of meropenem (2g IV q8h), tigecycline (100mg IV q12h, Tygacil, Wyeth Lederle S.R.L.), and voriconazole (400mg IV q12h loading dose followed by 200mg IV q12h, Vfend, Pfizer Europe MA EEIG/Pharmacia & Upjohn Company LLC), and she was on ventilation again. Six days later (on the 55th day of hospitalization), the sepsis was under control, and the blood culture yielded negative results. However, body temperature was 38.2°C, the CSF obtained through EVD showed a WBC of 14,000/μL (85% polymorphonuclear leukocytes), a total protein level of 827 mg/dl, and a glucose level of 0.05mmol/L (the simultaneous blood glucose levels of 13.9mmol/L). The CSF culture remained persistently positive for M. odoratimimus (, ), and the minimum inhibitory concentration (MIC) of tigecycline against M. odoratimimus was 0.5 mg/L. Consequently, the patient received intracerebroventricular (ICV) administration of 2mg tigecycline q12h, which was diluted in saline up to a volume of 5mL and injected through the EVD catheter within two minutes after removing an equivalent volume of CSF through EVD. The EVD catheter was closed for two hours after each dose of injection, and a new right EVD was placed as well ().
Table 2 In vitro Susceptibility of the Myroides odoratimimus Isolated in Cerebrospinal Fluid
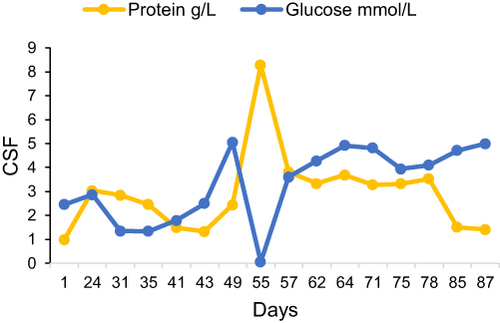
Figure 2 Protein and glucose in CSF during hospitalization.
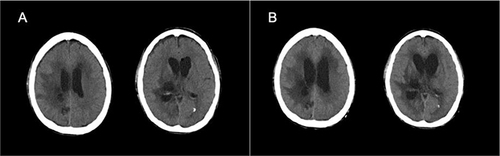
Following the adjustment of the antibiotic regimen, the patient exhibited a gradual normalization of body temperature on the next day, and the blood and CSF cultures became negative after nine days of intraventricular injection combined with fifteen days of intravenous administration of tigecycline. A CSF sample obtained through the EVD displayed a WBC count of 150/μL (30% polymorphonuclear leukocytes), a total protein level of 368.5 mg/dL, and a glucose level of 4.92 mmol/L (blood glucose level was 9.7 mmol/L). Brain magnetic resonance imaging (MRI) revealed the presence of partial blood accumulation in the right thalamus, along with mild hydrocephalus (). The patient underwent surgical excision and drainage of the blood accumulation, and the right EVD was replaced with a new left EVD on the 66th day of hospitalization. The blood accumulation and CSF sample culture were negative. After repeated negative results of CSF culture, the administration of tigecycline IV and meropenem was discontinued on the 69th day of hospitalization. The EVD was removed, and ICV tigecycline administration was stopped on the 77th day of hospitalization due to a significant improvement of CSF test results, and CSF drainage from the EVD was less than 50 mL per day. Additionally, repeated lumbar CSF sampling revealed no recurrence of intracranial infection 12 days after antibiotic discontinuation, while brain CT scanning demonstrated a deterioration of hydrocephalus (). Consequently, a ventriculoperitoneal (VP) shunt was inserted on the 92nd day of hospitalization, and the patient was weaned off the ventilator. The GCS score was 5 points with involuntary eye movement, and she was transferred to the general ward for further rehabilitation.
Figure 3 Brain MRI revealed partial blood accumulation in the right thalamus associated with mild hydrocephalus. (A) T1-weighted image; (B) T2-weighted image; (C) diffusion-weighted image (DWI); (D) flair image.
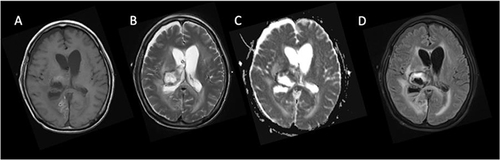
Figure 4 Brain CT on the first day and the 12th day after removal of EVD showing deterioration of hydrocephalus. (A) Brain CT on the first day after removal of EVD showing mild hydrocephalus; (B) brain CT on the 12th day after removal of EVD suggesting aggravation of hydrocephalus.
Discussion
The incidence of postoperative meningitis resulting from neurosurgical interventions ranges from 0.34% to 3.1%, causing significant morbidity and mortality.Citation10 EVD is a frequently employed neurosurgical procedure utilized to manage raised intracranial pressure, alleviate an obstructed ventricular system, or promote drainage of CSF to ameliorate intracranial infection or intraventricular hemorrhage. Aimun A Jamjoom et al reported a national rate of EVD-related infection of 9.3% in the UK and Ireland.Citation11
Several risk factors have been identified for EVD-related infections, including prolonged indwelling time, repeated CSF sampling, CSF leakage around the catheter, and bilateral ventricular drainage,Citation12–16 with the risk increasing in the first week. However, different studies have reported varying results for indwelling times longer than one week, primarily due to the inconsistent definitions of EVD-related infections.Citation12 Studies have demonstrated that CSF diversion, CSF leakage, and catheter insertion site dehiscence after brain surgery are associated with an increased risk of EVD-related infections. Nevertheless, the duration of EVD use of more than 7 days showed no significant correlation with infection risk.Citation13 Williamson et al showed that the risk of EVD-related infection increased by 8.3% for each CSF sampling from the EVD.Citation14 While the risk of intracranial infection decreased from 17% to 11% overall and definite ventricular infection from 10% to 3% once sampling frequency was once every 3 days.Citation15
Our patient was diagnosed as ventriculitis and meningitis (VM) according to the recent report of Karvouniaris et alCitation17 reviewing the current perspectives on the diagnosis and management of healthcare-associated VM. It was challenging to manage VM associated with hydrocephalus. Our patient underwent a third ventriculostomy and left EVD as a temporizing measure after the improvement of pneumonia and intestinal infection. A VP shunt was not feasible due to the patient’s CSF tests indicating intracranial infection with significantly high protein and low glucose levels, despite negative CSF cultures. The patient developed intracranial Klebsiella acidophilus infection after 11 days of continuous CSF drainage from EVD. The pathogen was controlled by colistin after the failure of amikacin IV combined with ICV injection (overall treatment period of one week) according to the guidelines issued by Infectious Diseases Society of America,Citation18 meanwhile, IV antimicrobial administration was suggested if the patient did not clinically improve on solely systemic antimicrobial treatment.Citation17 The interstitial cerebral edema improved due to successful drainage, but hydrocephalus persisted, with CSF drainage from the EVD exceeding 200 mL per day. CSF from EVD showed a high level of protein with a low level of glucose, although cultures were negative at that time. Thus, the indwelling time of EVD was prolonged for drainage of CSF as well as IV antibiotics. It was recommended that the duration of IV antibiotic treatment was 2–3 days after CSF sterility although the overall treatment may last for up to 3 weeks following culture negativity.Citation19 In our patient, the total duration of IV colistin was 21 days. The EVD catheter was not changed regularly. Hong et alCitation20 displayed that routine EVD replacement was not helpful for reducing EVD-associated infection. According to the Infectious Diseases Society of America’s Clinical Practice Guidelines, patients with intracranial infection caused by gram-negative rods should be reimplanted with VP shunt 10 days after CSF cultures are negative.Citation18 After the control of intracranial Klebsiella acidophilus infection, the implementation of VP shunt was deferred. However, during the waiting period, there was a recurrence of intracranial infection, and M. odoratimimus was identified from the CSF that was drained from the EVD. The extended retention of the EVD, frequent CSF sampling, repetitive ICV, and exposure to carbapenems constituted risk factors for EVD-associated infection in the patient.
M. odoratimimus is a non-motile, contact-positive, straight rod-shape Gram-negative bacterium with round ends and no endospore formation. It has a fruity odor and exhibits yellow pigmentation, and can grow well at 37°C. Previously classified as Flavobacteria, it was later reclassified as a member of the Myroides spp. genus and further divided into two categories, namely Myroides odoratus and M. odoratimimus in 1996.Citation21 It is widely distributed in the environment, particularly in water and soil, and is known to cause opportunistic infections in immunocompromised individuals. The main risk factors for M. odoratimimus infection are related to exposure to contaminated water sources, animal bites, and catheters, such as urinary catheters, deep venous catheters, EVD, and VP shunting. Clinical reports have demonstrated that M. odoratimimus infections are prevalent in immunocompromised individuals. Ktari et al reported that the extensive use of carbapenems in Tunisian hospitals may have led to the emergence of pan-resistant M. odoratimimus strains.Citation22
Some cases of soft tissue infection, bacteremia, urinary tract infection, have been reported in patients with immunosuppressive diseases, such as diabetes mellitus, alcoholic cirrhosis, COPD on long-term corticosteroid treatment. Cellulitis and bacteremia due to M. odoratimimus was reported by Bachmeyer et alCitation23 and LaVergne et al.Citation24 Several other serious soft tissue infections caused by this organism in immunocompromised hosts were described with favorable outcomes.Citation3,Citation25–27 Outbreak of urinary tract infections caused by M. odoratimimus in immunocompromised patients was reported in a Romanian hospitalCitation28 and Turkish.Citation29
Clinical infections in immunocompetent patients also have been described in recent years. Maraki et alCitation6 reported an immunocompetent child suffered from M. odoratimimus soft tissue infection following by a pig bite, which causing osteolytic lesions. Another occasion was a 72-year-old male with septic shock due to M. odoratimimus isolated from soft tissue and lung specimens.Citation30 Lu et alCitation5 reported a catheter related blood stream infection with septic shock caused by M. odoratimimus in an immunocompetent adult.
The opportunistic organism could cause life-threatening infections due to rapid disease progression and high levels of drug resistance. Till date, three cases were reported fatal. One case was an immunocompromised host suffered from pericardial effusion due to M. odoratimimus from India with the history of chronic kidney disease and undergoing maintenance haemodialysis.Citation31 In another case, an elderly male with urinary tract infection was found to have M. odoratimimus in urine culture. Although the patient was immunocompetent, he did not respond to antibiotics for the pan-resistant pathogen and succumbed to death.Citation7 Recently, Kurt et al described a severe case with COVID-19 pneumonia undergoing CRRT (Continuous renal replacement therapy) and ECMO (extracorporeal membrane oxygenation) ending with fatality due to the pan-resistant M. odoratimimus bacteremia.Citation32
Intracranial infections with Myroides spp. were rarely represented. A 6-week-old infant with hydrocephalus later developed Flavobacterium odoratum ventriculitis was described early in 1985.Citation33 Casalta et alCitation34 reported two cases of pneumonia and meningitis caused by a New Nonfermentative Unknown Gram-negative Bacterium resembling Flavobacterium spp. from the hot-spring area in the south of France in 1987, but the rod was not named. There was another meningitis due to Flavobacterium ceti after neurosurgery in a patient with diabetes mellitus.Citation35 Our study presents the first reported case of intracranial infection with M. odoratimimus following EVD surgery, and we document our approach to treatment utilizing a combination of IV and ICV injection of tigecycline. Our findings contribute to the existing literature on intracranial infections caused by M. odoratimimus in immunocompetent individuals.
The treatment of M. odoratimimus infection was challenging for its high antibiotic resistance. Multidrug resistance could be attributed to several factors. Most strains were resistant to β-lactams, carbapenems, monobactams, and aminoglycosides.Citation4 One strain of M. odoratimimus was found to produce Amp-C beta lactamase.Citation36 Mammeri et al and others had identified chromosomally encoded β-lactamases and other metalloenzymes to hydrolyze carbapenems and other β-lactam antibiotics.Citation37 Chromosome-encoded β-lactamases TUS-1 and MUS-1 had also been found in M. odoratimimus and Myroides odoratus.Citation37,Citation38 Shuang Yang analyzed the resistance of 22 isolates of M. odoratimimus, six of them produced MUS-1, a novel variant of blaMUS-1 encoded with MUS-3 protein was found in the remaining 16 isolates causing highly resistant to most available antibiotics.Citation39 The identified strain M. odoratimimus PR63039 was pan-resistant and the resistance genes were associated with resistance to beta-lactams (blaOXA-347, blaMUS-1, blaEBR-1), tetracyclines (tetX), sulfonamides (sul2), macrolides (ereD, ermF).Citation32
Biofilm formation was another factor of drug resistance. Arianna Pompilio studied the ability of M. odoratimimus to form biofilm through a vitro “skin-like” model. The results showed that M. odoratimimus could form biofilm biomass in a time-dependent manner, while independent of glucose concentration, the resistance genes (gyrA, acrB) increased significantly during the planktonic-to-biofilm transition.Citation40
The therapy of M. odoratimimus infection, particularly in cases of intracranial infection, is limited due to poor penetration of most antibiotics through blood-brain barrier. Literature regarding antibiotic options is primarily based on case reports. Treatment of M. odoratimimus infections has shown efficacy with various antibiotics, such as ciprofloxacin in combination with imipenem/cilastatin, tigecycline, ciprofloxacin, piperacillin/tazobactam, teicoplanin, cefoperazone/sulbactam, levofloxacin and intraventricular cefotaxime, depending on susceptibility test results.Citation5,Citation6,Citation23,Citation28,Citation30,Citation33 Pompilio et alCitation40 described that meropenem and tigecycline were obviously more active against planktonic cells than biofilm cells, while levofloxacin and tigecycline acted as a bactericidal mechanism. But the tested levofloxacin, meropenem and tigecycline were not able to completely eradicate preformed biofilms. Gunzer et alCitation36 analysed MIC results for 43 strains of M. odoratimimus about 20 important antibiotics. Only one strain was susceptible to ampicillin and two strains were susceptible to piperacillin/tazobactam, four strains were susceptible to imipenem, 74.4% of the strains were susceptible to meropenem, only one strain was susceptible to tigecycline. In our case, when the patient developed M. odoratimimus ventriculitis during the period of colistin ICV, meropenem and tigecycline was given immediately intravenously according to drug sensitivity test and the experience of these reports.
Tigecycline is a glycylcycline antibiotic which is active against a large range of multidrug-resistant Gram-positive and Gram-negative bacteria.Citation41 It was widely used in different clinical settings including pneumonia and blood stream infection. The CSF concentration of tigecycline was about 7.9% of their serum concentration due to the lack of penetration to CNS.Citation42 There have been some reports of multi-route tigecycline for the treatment of intracranial multidrug-resistant infection.Citation43–45 Lauretti et alCitation42 first reported a case of intraventricular tigecycline for multi-resistant Acinetobacter baumannii intracranial infection. In our case, tigecycline 100 mg IV over 2h q12h was initiated immediately combined with meropenem, but the intracranial infection deteriorated six days later. Study of Wilkie et alCitation46 suggested that the clearance time to CSF sterilization in intraventricular antibiotic treatment was significantly shorter than that in intravenous antibiotic therapy. The guideline recommended that if intravenous therapy failed, intraventricular antimicrobial therapy should be considered, and that the dose and intervals of intraventricular antibiotic therapy should be adjusted to 10–20 times the MIC of the pathogenic microorganism depending on the CSF concentrations of antibacterial agents, ventricular size, and daily drainage from the ventricle.Citation18 The MIC of tigecycline against M. odoratimimus was found to be 0.5 mg/L in our patient. Due to the poor penetration of tigecycline into the CNS, our patient received ICV administration of 2mg tigecycline every q12 h, and EVD catheter was changed concurrently. In our report, CSF became sterile after 20 days of intravenous tigecycline and 22 days of ICV injection. No toxicity about neurological adverse effects, such as epilepsy, muscle spasm occurred in our report. This case report contributes to the literature on clinically relevant isolation of M. odoratimimus in immunocompetent patients with intracranial infection and documents the successful antibiotic treatment of M. odoratimimus despite its resistance to most antibiotics.
The limitation of our article is that it is a case report, and more clinical cases are needed to support our results and to evaluate the safety of intraventricular tigecycline.
Conclusion
The incidence of nosocomial infections of atypical multidrug resistant organisms has gradually increased due to broad-spectrum antibiotics therapy. M. odoratimimus can cause nosocomial infections even infection outbreak and death although it is an opportunistic pathogen. Clinicians should be alert to M. odoratimimus infection especially in immunocompetent individuals. For intracranial infection of M. odoratimimus, tigecycline IV combined with ICV could be a therapeutic choice, but mainly according to the susceptibility test. We need more clinical cases to support our conclusion.
Ethics Approval and Patient Consent
Our study was approved by the Ethics Committee at Zhejiang Provincial People`s Hospital (approval number is 2022O386) in accordance with the ethical standards of Helsinki Declaration. The written and informed consent for publication of this case and any details was obtained from the patient`s husband as a legal guardian because the patient was unconscious, and the informed consent for publication of any details was also obtained if she regained consciousness in the further. We strictly abided by data protection legislation and ethical standards, patient`s personal information such as name, gender, hospitalization number won`t be appeared in terms of images, laboratory examination of our article.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Martin RM, Zimmermann LL, Huynh M, et al. Diagnostic approach to health care- and device-associated central nervous system infections. J Clin Microbiol. 2018;56(11):e00861–18. doi:10.1128/JCM.00861-18
- Ramanan M, Lipman J, Shorr A, et al. A meta-analysis of ventriculostomy-associated cerebrospinal fluid infections. BMC Infect Dis. 2015;15(1):3. doi:10.1186/s12879-014-0712-z
- Bachman KH, Sewell DL, Strausbaugh LJ. Recurrent cellulitis and bacteremia caused by Flavobacterium odoratum. Clin Infect Dis. 1996;22(6):1112–1113. doi:10.1093/clinids/22.6.1112
- Holmes B, Snell JJ, Lapage SP. Flavobacterium odoratum: a species resistant to a wide range of antimicrobial agents. J Clin Pathol. 1979;32(1):73–77. doi:10.1136/jcp.32.1.73
- Yanfei L, Xia W, Zhang X, et al. A Confirmed Catheter-Related Blood Stream Infection (CRBSI) in an immunocompetent patient due to myroides odoratimimus: case report and literature review. Infect Drug Resist. 2020;13:139–144. doi:10.2147/IDR.S234778
- Maraki S, Sarchianaki E, Barbagadakis S. Myroides odoratimimus soft tissue infection in an immunocompetent child following a pig bite: case report and literature review. Braz J Infect Dis. 2012;16(4):390–392. doi:10.1016/j.bjid.2012.06.004
- Ahamed I, Annapandian VM, Muralidhara KD. Myroides odoratimimus urinary tract infection. Saudi J Kidney Dis Transpl. 2018;29(5):1220–1222. doi:10.4103/1319-2442.243957
- Shao-hua H, Yuan S-X, Hai Q, et al. Antibiotic resistance mechanisms of Myroides sp. J Zhejiang Univ Sci B. 2016;17(3):188–199. doi:10.1631/jzus.B1500068
- Lorenzin G, Piccinelli G, Carlassara L, et al. Myroides odoratimimus urinary tract infection in an immunocompromised patient: an emerging multidrug-resistant micro-organism. Antimicrob Resist Infect Control. 2018;7:96. doi:10.1186/s13756-018-0391-4
- Dettenkofer M, Ebner W, Els T, et al. Surveillance of nosocomial infections in a neurology intensive care unit. J Neurol. 2001;248(11):959–964. doi:10.1007/s004150170048
- Jamjoom AAB, Joannides AJ, Poon MT-C, et al. Prospective, multicentre study of external ventricular drainage-related infections in the UK and Ireland. J Neurol Neurosurg Psychiatry. 2018;89(2):120–126. doi:10.1136/jnnp-2017-316415
- Korinek A-M, Reina M, Boch AL, et al. Prevention of external ventricular drain--related ventriculitis. Acta Neurochir. 2005;147(1):39–45. doi:10.1007/s00701-004-0416-z
- Walek KW, Leary QP, Sastry R, et al. Risk factors and outcomes associated with external ventricular drain infections. Infect Control Hosp Epidemiol. 2022;43:1–8.
- Williamson RA, Phillips-Bute BG, McDonagh DL, et al. Predictors of extraventricular drain-associated bacterial ventriculitis. J Crit Care. 2014;29(1):77–82. doi:10.1016/j.jcrc.2013.08.012
- Williams TA, Leslie GD, Dobb GJ, et al. Decrease in proven ventriculitis by reducing the frequency of cerebrospinal fluid sampling from extraventricular drains. J Neurosurg. 2011;115(5):1040–1046. doi:10.3171/2011.6.JNS11167
- Zheng W-J, Liang-Ming L, Zi-Hui H, et al. Bilateral external ventricular drains increase ventriculostomy-associated cerebrospinal fluid infection in low modified graeb score intraventricular hemorrhage. World Neurosurg. 2018;116:e550–e555. doi:10.1016/j.wneu.2018.05.030
- Karvouniaris M, Brotis A, Tsiakos K, et al. Current perspectives on the diagnosis and management of healthcare-associated ventriculitis and meningitis. Infect Drug Resist. 2022;15:697–721. doi:10.2147/IDR.S326456
- Tunkel AR, Hasbun R, Bhimraj A, et al. 2017 infectious diseases society of america’s clinical practice guidelines for healthcare-associated ventriculitis and meningitis. Clin Infect Dis. 2017;64(6):e34–e65. doi:10.1093/cid/ciw861
- LeBras M, Chow I, Mabasa VH, et al. Systematic review of efficacy, pharmacokinetics, and administration of intraventricular aminoglycosides in adults. Neurocrit Care. 2016;25(3):492–507. doi:10.1007/s12028-016-0269-3
- Hong B, Apedjinou A, Heissler HE, et al. Effect of a bundle approach on external ventricular drain-related infection. Acta Neurochir. 2021;163(4):1135–1142. doi:10.1007/s00701-020-04698-8
- Vancanneyt M, Segers P, Tork U, et al. Reclassification of Flavobacterium odoratum (Stutzer 1929) strains to a new genus, myroides, as Myroides odoratus comb. nov. and Myroides odoratimimus sp. nov. Int J Syst Evol Microbiol. 1996;46(4):926–932.
- Ktari S, Mnif B, Koubaa M, et al. Nosocomial outbreak of Myroides odoratimimus urinary tract infection in a Tunisian hospital. J Hosp Infect. 2012;80(1):77–81. doi:10.1016/j.jhin.2011.09.010
- Bachmeyer C, Entressengle H, Khosrotehrani K, et al. Cellulitis due to Myroides odoratimimus in a patient with alcoholic cirrhosis. Clin Exp Dermatol. 2008;33(1):97–98. doi:10.1111/j.1365-2230.2007.02590.x
- LaVergne S, Gaufin T, Richman D. Myroides injenensis bacteremia and severe cellulitis. Open Forum Infect Dis. 2019;6(7):ofz282. doi:10.1093/ofid/ofz282
- Beathard WA, Pickering A, Jacobs M. Myroides cellulitis and bacteremia: a case report. IDCases. 2021;24:e01061. doi:10.1016/j.idcr.2021.e01061
- Willems P, Muller J, Verhaegen J, et al. How to treat a fulminant erysipelas and sepsis caused by Myroides odoratimimus: case report and literature review. Acta Clin Belg. 2017;72(5):331–335. doi:10.1080/17843286.2016.1245173
- Pompilio A, Galardi G, Gherardi G, et al. Infection of recurrent calcaneal ulcer caused by a biofilm-producer Myroides odoratimimus strain. Folia Microbiol. 2018;63(2):203–207. doi:10.1007/s12223-017-0552-5
- Licker M, Sorescu T, Rus M, et al. Extensively drug-resistant Myroides odoratimimus - A case series of urinary tract infections in immunocompromised patients. Infect Drug Resist. 2018;11:743–749. doi:10.2147/IDR.S161069
- Kutlu HH, Avci M, Dal T, et al. A healthcare-associated outbreak of urinary tract infections due to Myroides odoratimimus. Jpn J Infect Dis. 2020;73(6):421–426. doi:10.7883/yoken.JJID.2019.536
- Benedetti P, Rassu M, Pavan G, et al. Septic shock, pneumonia, and soft tissue infection due to Myroides odoratimimus: report of a case and review of Myroides infections. Infection. 2011;39(2):161–165. doi:10.1007/s15010-010-0077-1
- Prateek S, Gupta P, Mittal G, et al. Fatal Case of pericardial effusion due to Myroides odoratus: a rare case report. J Clin Diagn Res. 2015;9(11):01–2.
- Kurt AF, Mete B, Houssein FM, et al. A pan-resistant Myroides odoratimimus catheter-related bacteremia in a COVID-19 patient and review of the literature. Acta Microbiol Immunol Hung. 2022. doi:10.1556/030.2022.01702
- Macfarlane DE, Baum-Thureen P, Crandon I. Flavobacterium odoratum ventriculitis treated with intraventricular cefotaxime. J Infect. 1985;11(3):233–238. doi:10.1016/S0163-4453(85)93228-1
- Casalta JP, Peloux Y, Raoult D, et al. Pneumonia and meningitis caused by a new nonfermentative unknown gram-negative bacterium. J Clin Microbiol. 1989;27(7):1446–1448. doi:10.1128/jcm.27.7.1446-1448.1989
- Park SK, Ryoo N. A Case of Flavobacterium ceti Meningitis. Ann Lab Med. 2016;36(6):614–616. doi:10.3343/alm.2016.36.6.614
- Gunzer F, Rudolph WW, Bunk B, et al. Whole-genome sequencing of a large collection of Myroides odoratimimus and Myroides odoratus isolates and antimicrobial susceptibility studies. Emerg Microbes Infect. 2018;7(1):61. doi:10.1038/s41426-018-0061-x
- Mammeri H, Bellais S, Nordmann P. Chromosome-encoded beta-lactamases TUS-1 and MUS-1 from Myroides odoratus and Myroides odoratimimus (formerly Flavobacterium odoratum), new members of the lineage of molecular subclass B1 metalloenzymes. Antimicrob Agents Chemother. 2002;46(11):3561–3567. doi:10.1128/AAC.46.11.3561-3567.2002
- Sato K, Fujii T, Okamoto R, et al. Biochemical properties of beta-lactamase produced by Flavobacterium odoratum. Antimicrob Agents Chemother. 1985;27(4):612–614. doi:10.1128/AAC.27.4.612
- Yang S, Liu Q, Shen Z, et al. Molecular epidemiology of myroides odoratimimus in nosocomial catheter-related infection at a general hospital in China. Infect Drug Resist. 2020;13:1981–1993. doi:10.2147/IDR.S251626
- Pompilio A, Galardi G, Verginelli F, et al. Myroides odoratimimus forms structurally complex and inherently antibiotic-resistant biofilm in a wound-like in vitro model. Front Microbiol. 2017;8:2591. doi:10.3389/fmicb.2017.02591
- Yaghoubi S, Zekiy AO, Krutova M, et al. Tigecycline antibacterial activity, clinical effectiveness, and mechanisms and epidemiology of resistance: narrative review. Eur J Clin Microbiol Infect Dis. 2022;41(7):1003–1022. doi:10.1007/s10096-020-04121-1
- Lauretti L, D’Alessandris QG, Fantoni M, et al. First reported case of intraventricular tigecycline for meningitis from extremely drug-resistant Acinetobacter baumannii. J Neurosurg. 2017;127(2):370–373. doi:10.3171/2016.6.JNS16352
- Perier F, Couffin S, Martin M, et al. Multidrug-resistant Acinetobacter baumannii ventriculostomy-related infection, treated by a colistin, tigecycline, and intraventricular fibrinolysis. World Neurosurg. 2019;121:111–116. doi:10.1016/j.wneu.2018.09.218
- Soto-Hernández JL, Soto-Ramírez A, Pérez-Neri I, et al. Multidrug-resistant Klebsiella oxytoca ventriculitis, successfully treated with intraventricular tigecycline: a case report. Clin Neurol Neurosurg. 2020;188:105592. doi:10.1016/j.clineuro.2019.105592
- Şahin A, Dalgic N. Intraventricular plus intravenous tigecycline for the treatment of daptomycin nonsusceptible vancomycin-resistant enterococci in an infant with ventriculoperitoneal shunt infection. World Neurosurg. 2019;130:470–473. doi:10.1016/j.wneu.2019.07.045
- Wilkie MD, Hanson MF, Statham PF, et al. Infections of cerebrospinal fluid diversion devices in adults: the role of intraventricular antimicrobial therapy. J Infect. 2013;66(3):239–246. doi:10.1016/j.jinf.2012.11.006