
Abstract
Purpose
Urinary tract infections exert a significant negative impact on an individual’s quality of life and cause significant economic and public health burdens. Therefore, this study was conducted to identify the common bacterial uropathogens associated with urinary tract infections in Wad Medani patients and their susceptibility to antibiotics.
Patients and Methods
This was a cross-sectional study. All urine samples were collected from patients at Wad Medani and investigated at the Pathology Center for Diagnosis and Research, Faculty of Medicine, University of Gezira, Sudan, from the 1st of January 2021 to the 15th of October 2023.
Results
A total of 2698 urine samples were analyzed during the three years study period, with a mean age of 45.29 ± 18.9 years. Among these patients, 1108 (41.8%) were positive for bacterial growth, and 888 (80.14%) were female. A total of 522 (47.1%) were gram positive bacteria (GPB), and 586 (52.9%) were gram negative bacteria (GNB). The most frequently isolated bacteria were S. aureus 42% (465/1108) and E. coli 38.5% (427/1108), while P. aeruginosa was less detected 3.4% (38/1108). Amikacin 91.5% was the most sensitive drug to isolated GPB, while cotrimoxazole 20.9% was the least sensitive drug. In particular, amikacin 94.1% (144/153) was the most sensitive drug to S. aureus, while cotrimoxazole 20.7% (80/386) was the least sensitive drug. Moreover, amikacin 91.5% was the most sensitive drug to the isolated GNB, while ampicillin 5.7% was the least sensitive drug. Notably, amikacin was the most sensitive drug to all the isolated GNB, and ampicillin was the least sensitive drug to all the isolated GNB.
Conclusion
This study reported a moderate uropathogen isolation rate of 41.8%. S. aureus and E. coli were the most frequently isolated bacteria, most of which were from female patients. Remarkably, amikacin was the most sensitive drug to isolated GNB and GPB.
Introduction
Urinary tract infections (UTIs) are one of the most prevalent infections caused by bacteria and can be detected in both community and healthcare settings.Citation1
UTIs exert a significant negative impact on an individual’s quality of life and cause significant economic and public health burdens.Citation2 UTIs are a major cause of morbidity in older men and women of all ages and even in infant boys. UTIs are caused by both gram-negative and gram-positive bacteria (GPB) in addition to some fungiCitation3, of these, uropathogenic Escherichia coli (E. coli) strains are the most common causative agent.Citation4,Citation5
Antimicrobial resistance (AMR) is a challenge that impacts all countries, regardless of their financial standing or developmental level.Citation1 In particular, AMR is more severe in developing countries due to irrational antibiotic use and inadequate infection prevention strategies.Citation6 The AMR Global World Health Organization (WHO) report on surveillance states that Africa and Southeast Asia are the areas without functioning AMR surveillance systems.Citation7
Recently, there has been an increase in the prevalence of uropathogen resistance to previously effective antibiotics,Citation8 given that most UTI patients start to receive empirical treatment before laboratory results are obtained from urine culture.Citation9 A previous study conducted in Sudan showed that multiple drug resistance was found in 90% of the isolated bacterial uropathogens.Citation4
Understanding local patterns of antimicrobial resistance is crucial because it can guide empirical and specific treatment recommendations.Citation10 Empirical management plans need to be updated on a regular basis to consider changing patterns of pathogen susceptibility.Citation11 However, no data have been published from the present study area. Therefore, this study was conducted to identify the common bacterial pathogens associated with UTIs in Wad Medani patients and their susceptibility to antibiotics, which might be extremely significant in establishing the most appropriate empirical antibacterial therapy.
Materials and Methods
Study Site
Wad Medani, Gezira State, Sudan.
Study Design
This was a cross-sectional study.
Sample Size and Data Collection
All urine samples were collected from patients at Wad Medani and investigated at the Pathology Center for Diagnosis and Research, Faculty of Medicine, University of Gezira, Sudan, from the 1st of January 2021 to the 15th of October 2023; these patients were included in the study.
Inclusion Criteria
All patients were aged ≥ 18 years.
Exclusion Criteria
Patients aged < 18 years.
Antibiotics were tested for less than 20% of bacteria.
Antibiotics are not included in the Clinical and Laboratory Standard Institute (CLSI) guidelines for specific bacteria.Citation12
Sample Collection and Laboratory Methods
Sample Collection
After the patients were instructed to clean their genitals, a freshly voided midstream urine sample (10–20 mL) was collected in a wide-mouthed sterile, dry, and leak-proof container.Citation13 For patients with catheters, urine was aspirated directly from the catheter using a sterile syringe and needle and then deposited in a sterile container.Citation14
Identification of the Isolated Organism
The collected urine samples were inoculated onto MacConkey agar and blood agar plates using a calibrated loop (0.001 mL).Citation13 Cultures were incubated in an aerobic atmosphere at 37°C for 24 hours. A positive urine culture was defined as a colony count of ≥105CFU/mL for midstream urine.Citation14 For all positive cultures, morphological characteristics, Gram staining, and confirmatory biochemical tests were used to identify the bacterial isolates. Gram-positive bacteria were identified by the catalase reaction, coagulase test, optochin test, bacitracin test, and hemolytic activity test on blood agar. Additionally, gram-negative bacteria (GNB) were identified by inoculation on MacConkey agar plates, followed by biochemical tests such as H2S production, indole production, utilization of citrate/carbohydrates, urease tests, and oxidase tests.Citation13
Antimicrobial Susceptibility
The antimicrobial susceptibilities of the bacterial isolates were ascertained by Mueller–Hinton agar plates (Oxoid, England) using the Kirby–Bauer disk diffusion method according to CLSI guidelines 2020.Citation12 GPB isolates were tested against the following antimicrobials: Ampicillin (10 µg), Cotrimoxazole (1.25/23.75 µg), Tetracycline (30 µg), Ciprofloxacin (5 µg), Levofloxacin (5 µg), Chloramphenicol (30 µg), Ofloxacin (5 µg), Amikacin (30 µg), Nitrofurantoin (300 µg), Norfloxacin (10 µg), and Amoxicillin/Clavulanic (20/10 µg),Citation12 while GNB isolates were tested against the antimicrobials previously mentioned as well as Ampicillin/Sulbactam (10/10 µg), Ceftriaxone (30 µg), and Cefotaxime (30 µg).Citation12 The CLSI 2020 guideline breakpoints were used to interpret zone diameters.Citation12
Quality Control
As part of the standard practice throughout the whole laboratory work process, quality control procedures were used to ensure the validity of the results. Before usage, the normal shelf life of the culture media, staining reagents, and antibiotic discs was examined.Citation15 All culture plates and antibiotic discs were prepared and autoclaved at 121 °C for 15 minutes, after which the plates were kept at the stated refrigeration temperature. The standard reference bacterial strains were examined as a positive control on agar plates with antibiotic discs and biochemical assays.Citation15 The samples were handled carefully by qualified microbiologists.
Variable Definition
Coliform: included bacteria species of genera other than E. coli and Klebsiella (Citrobacter, Enterobacter, Serratia, etc.).
Statistical Analysis
The Statistical Package for the Social Science (SPSS) version 27.0 was used to analyze the data. Qualitative data are presented as frequencies (percentages). Quantitative data are presented as the mean ± standard deviation.
Results
Sociodemographic Characteristics
A total of 2698 urine samples were analyzed during the three years study period; 1998 (73.9%) were from female patients, 700 (25.9%) were from male patients, and the mean (±standard deviation) age of the study participants was 45.29 ± 18.9 years.
Bacterial Profile
In total, our results showed that 1108 (41.8%) of the urine specimens were positive for bacterial growth, of which 522 (47.1%) were GPB, while GNB accounted for 586 (52.9%). Female patients accounted for the vast majority of positive urine culture 888 (80.14%) and male accounted for 222 (19.86)%. In addition, most of the positive culture urine samples occurred at 2022 662 (59.7%). Integrated data from three years, as well as the overall distribution of GNB and GPB incidence, are shown in ().
Table 1 Isolated Uropathogens Among the Three Years
Overall, Staphylococcus aureus (S. aureus) was the most frequently isolated bacteria 42% (465/1108), most of which was isolated from female patients aged 45–59 years 140 (15.76%), and the least incidence in male patients aged 18 −29 years 10 (4.54%), as shown in (). E. coli was the second most common bacteria isolated 38.5% (427/1108), most of which were obtained from female patients aged ≥ 60 years 100 (11.26%), and male patients aged 45–59 years were the least 6(2.73%) incidence (). Pseudomonas aeruginosa (p. aeruginosa) 3.4% (38/1108) was less detected bacteria, most of which were isolated from male patients aged ≥ 60 years 12 (5.54%) (). With respect to GPB, our data revealed that S. aureus was the most abundant bacteria, while E. coli was the most common bacteria isolated from GNB ().
Table 2 Uropathogens in Different Age Groups and Sex in the Study Population
Antimicrobial Susceptibility Profile
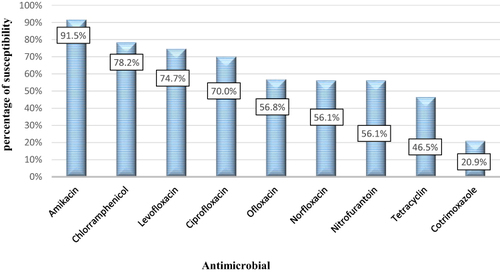
The obtained data showed that out of 15 drugs were tested. Regarding GPB, our data showed that amikacin 91.5% was the most sensitive drug to the isolated GPB, followed by chloramphenicol 78.2%, while cotrimoxazole 20.9% was the least sensitive drug to GPB (). Concerning S. aureus, amikacin 94.1% (144/153) was the most sensitive drug, followed by chloramphenicol 76% (146/192), while cotrimoxazole 20.7% (80/386) was the least sensitive drug (). On the other hand, Streptococcus species (spp) showed the highest sensitivity to chloramphenicol 92.85% (26/28), and the least sensitivity to cotrimoxazole 22% (11/50) ().
Table 3 Sensitivity of Gram Positive Bacteria to Different Antimicrobial Agents
Figure 1 Overall Gram-positive strains’ sensitivity to common antibiotics tested.
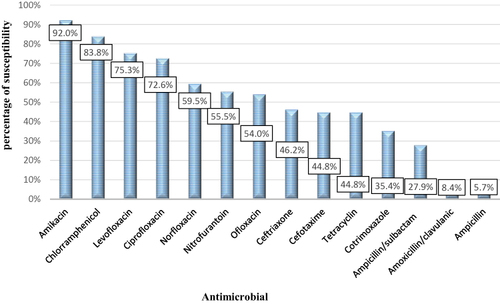
Regarding GNB, our data showed that amikacin 91.5% was the most sensitive drug to the isolated GNB, followed by chloramphenicol 83.8%, while ampicillin 5.7% was the least sensitive drug to GNB (). Notably, amikacin was the most sensitive drug to all isolated GNB. Which showed 91.2% (239/262) sensitivity to E.coli, 89.3% (25/28) to P. aeruginosa, 90.7% (39/43) to coliform, and 97.7% (43/44) to Klebsiella spp. Other remarkable results showed that ampicillin was the least sensitive drug to all isolated GNB. Which revealed 6.2% (13/210) sensitivity to E.coli, 9.5% (2/21) to coliform, and completely resistant to Klebsiella spp (0/31) as represented in ().
Table 4 Sensitivity of Gram Negative Bacteria to Different Antimicrobial Agents
Figure 2 Overall Gram-negative strains’ sensitivity to common antibiotics tested.
Discussion
Although UTIs continue to be one of the most prevalent illness patterns identified globally, treating UTIs has become more difficult as a result of the increasing development of antibiotic resistance.
Overall, the results of this investigation showed that the uropathogen isolation rate was 41.8%, which is considerably in agreement with that reported in a study conducted in Pakistan 36.1%.Citation16 However, this isolation rate was more than two studies were conducted in Addis Ababa, Ethiopia, and Yamen reported isolation rates of 9.8% and 18%, respectively.Citation17,Citation18 In addition, a study conducted in Khartoum, Sudan, revealed an isolation rate of 19.5%.Citation19 A significantly greater isolation rate of 71% was reported in a study conducted in Dhaka, Bangladesh;Citation20 this difference might be related to variations in the study population and geographical region.
The majority of isolated bacteria in this study were GNB, as has been noted in the majority of studies carried out elsewhere in the world. Our findings were in line with those of a study conducted in Pakistan, which showed that GNB were predominant;Citation16 a study performed in Irbil, Iraq, revealed that most uropathogens were GNB 82.44%.Citation21 Moreover, a study conducted in Addis Ababa, Ethiopia, reported that GNB were responsible for 84% of UTIs.Citation1
Overall, in the present study, S. aureus was the most frequently isolated bacteria, followed by E. coli. The prevalence of these bacteria among UTI patients may not be surprising, given that S. aureus is found within the skin’s normal flora; therefore, they can easily colonize the urinary tract and lead to infections, while E. coli is the most prevalent bacteria in the gastrointestinal tract and colon, from where it ascends to the urinary system and exploits its well-established virulence characteristics to colonize the urinary tract. The findings of this study were different from those of most published studies reporting that E. coli was the most predominant isolate. In two different hospital based studies conducted in Khartoum, Sudan, the most isolated bacteria were E. coli and Klebsiella pneumoniae.Citation4,Citation19 This variation might be linked to the difference in the study patients and settings, given that our study was laboratory based and encompassed outpatients and inpatients. Another study performed on outpatients at a tertiary care hospital in Pakistan revealed that E. coli 68.9% was the leading uropathogenic bacteria, followed by Klebsiella pneumoniae 8.9% and S. aureus 6.7%.Citation16 Furthermore, a study carried out in Addis Ababa, Ethiopia, showed that E. coli was the most commonly isolated 50% followed by Enterococcus spp at 12% and Enterobacter spp. at 12%.Citation1 This variation might be correlated with differences in study patients and settings.
Our study showed that female patients accounted for the vast majority of the positive urine cultures. This finding was supported by several studies worldwide; of those, a study conducted in Khartoum, Sudan, revealed that females accounted for 60% of UTI patients.Citation4 In addition, a multicenter study conducted in Eritrea showed that 64.9% of UTI patients were female.Citation22 Another study carried out in Al-Kut, Iraq, reported that 84.88% of the study population were female UTI patients.Citation23 Furthermore, a study conducted in Madinah, Saudi Arabia, showed that the percentage of female patients 52.1% was slightly higher than that of male patients 47.9%.Citation24 It is commonly recognized that women are more likely to develop UTIs because of the anatomical and physiological features of the urinary tract.Citation25
In our study, there was a progressive increase in the incidence of positive urine culture with female age during the entire study period. These findings were supported by a review study covering all aspects of UTIs, from prevalence to management, revealed that the incidence of UTIs in women increases proportionately with patient age, exceeding 10% annually for women older than 60 years.Citation26 Moreover, comprehensive observational research on UTIs in older individuals conducted in the United Kingdom revealed that in women, the incidence of UTIs increased from 11.4 to 14.3% in individuals aged 75 to 84 years and from 9 to 11% in individuals aged 65 to 74 years.Citation27 Furthermore, in a study conducted in India, the occurrence of UTIs in females increased from 9% at ages 18–30 to 24% at ages >45 years.Citation28 A study that examined why UTIs are more common in elderly women revealed that there are several risk factors, such as hormonal factors (hypoestrogenism leading to genital atrophy), anatomical alterations (uterine prolapse), and functional changes (urinary incontinence).Citation25,Citation29
In particular, the prevalence of E. coli among female patients was greater than that among men, and the highest rate was detected after 60 years of age. This result was in line with a study conducted in Brazil that reported that the prevalence of E. coli in women was 1.5 times greater than that in men.Citation30 In addition, a study conducted in Bangladesh revealed that the prevalence of E. coli was 63.6% in women and 36.4% in men.Citation31 Moreover, this result was in agreement with a study conducted in Peshawar, Pakistan, which reported that the prevalence of E. coli in female patients was 72.7%.Citation16 The high prevalence of E. coli in females might be linked to the fact that E. coli lives in the periurethral area and the shorter distance between the anal opening, the vaginal cavity and the urethra.Citation25
Regarding GPB, amikacin, chloramphenicol, and ciprofloxacin were the most sensitive drugs to isolated GPB, while the least sensitive drugs were tetracycline and cotrimoxazole. This finding was different from that of a study conducted in Bahir Dar, Northwest Ethiopia, in which the most sensitive drugs to GPB were ciprofloxacin 77.8%, penicillin 72.8%, and erythromycin 72.7%.Citation32 However, a study conducted in Addis Ababa, Ethiopia, revealed that GPB exhibited 100% total resistance to penicillin.Citation17 Furthermore, a study conducted on diabetic patients in al-Kut, Iraq, showed that gentamicin 11%, teicoplanin 6% and, vancomycin 6% were the most sensitive drugs, while oxacillin 49%, tetracycline 46%, and trimethoprim/sulfamethoxazole 45% were the least sensitive drugs.Citation23 This variation could be related to the regulation of antibiotic use and policies, in addition to the difference in the frequency of each antibiotic used among countries.
In particular, for S. aureus, amikacin was the most sensitive drug, followed by chloramphenicol, levofloxacin, and ciprofloxacin. This result contradict that reported previously in Shandi, Sudan, which showed that gentamicin was the most susceptible drug to S. aureus, followed by ceftriaxone, while the most resistant drugs were ceftazidime and cloxacillin.Citation33 In addition, a study carried out in Yemen revealed that the drugs most susceptible to S. aureus were cefepime, ampicillin, and nitrofurantoin.Citation18 Furthermore, the results of our study contradict those of a study conducted on Romanian female patients, which revealed that linezolid, levofloxacin, and nitrofurantoin were the most sensitive drugs for S. aureus.Citation34 Moreover, a study conducted in Eritrea reported that vancomycin 26.1%, rifampin 14.5%, and chloramphenicol 21.5% were the most sensitive drugs, while penicillin 95% and oxacillin 76.9% were the most resistant drugs.Citation22 However, a study conducted in Madinah, Saudi Arabia, revealed that the most sensitive drugs were vancomycin, nitroxoline, and trimethoprim/sulfamethoxazole, while the most resistant drugs were penicillin and ampicillin.Citation24 This difference might be related to the difference in study patients and geographic region, in addition to the availability of antimicrobial agents tested, given that some drugs, such as vancomycin and gentamycin, were not included in this study because they were tested in less than 20% of GPB.
Regarding GNB, our data showed that amikacin, chloramphenicol, and levofloxacin were the most sensitive drugs, and ampicillin, amoxicillin/clavulanic acid and ampicillin/sulbactam were the most resistant drugs. This result differed from that of a study conducted in Khartoum, Sudan, in which amikacin was one of the drugs that showed high resistance to GNB.Citation4 A study conducted in Bahir Dar, Northwest Ethiopia, reported that GNB had high sensitivity to ciprofloxacin, while in concordance, ampicillin was the most resistant drug against GNB.Citation32 Furthermore, a study conducted in Addis Ababa, Ethiopia, showed that GNB strains are highly sensitive to nitrofurantoin and meropenem, while in concordance, ampicillin is the most resistant drug against GNB.Citation17 However, in a study conducted on Romanian female patients, the most sensitive drugs for GNB were imipenem and meropenem, while the most resistant drugs were levofloxacin, ceftazidime, and amikacin.Citation34 This difference could be linked to the difference in study patients and settings.
In particular, for E. coli, amikacin was the most sensitive drug, followed by chloramphenicol, levofloxacin, and ciprofloxacin, while ampicillin and amoxicillin/clavulanic acid were the most resistant drugs. These findings were in line with those of a study conducted in Khartoum, Sudan, which revealed that ampicillin, cotrimoxazole, and amoxicillin-clavulanic acid were the most resistant drugs.Citation19 In addition, a study conducted in Addis Ababa, Ethiopia, showed that the most resistant drugs to E. coli were trimethoprim-sulfamethoxazole 85.7%, ampicillin 76.9%, and amoxicillin/clavulanic 71.4%.Citation1 Moreover, a study conducted in South Africa reported that the cotrimoxazole 65.1%, cefuroxime 27.3%, and amoxicillin-clavulanic acid 17.1% among the most resistance drugs.Citation35 In contrast, ampicillin and cefepime were the most sensitive drugs to E. coli in a study conducted in Yemen.Citation18 However, this result differed from that of a hospital based study conducted in Khartoum, Sudan, in which the drugs most resistant to E. coli were ampicillin, cefepime, amikacin, and ciprofloxacin.Citation4 These differences might be linked to differences in the study patients and settings, given that our study was laboratory based and encompassed outpatients and inpatients.
In particular, P. aeruginosa in this study exhibited high sensitivity to amikacin and levofloxacin, which differs from the findings of a study conducted in Khartoum, Sudan, in which amikacin exhibited a 69.3% resistance rate to P. aeruginosa.Citation4 Another study performed in Yemen revealed that the most sensitive drug for P. aeruginosa was cefepime.Citation18 However, in a study conducted in Madinah, Saudi Arabia, the most sensitive drugs were gentamicin and piperacillin/tazobactam, while the most resistant drugs were imipenem, meropenem, and levofloxacin.Citation24 This difference might be correlated with the difference in antibiotics tested.
Strengths and Limitations
As a strength of this study, we evaluated the prevalence and sensitivity patterns of uropathogens over a three-year period, which provided an accurate depiction of the prevalence and resistance patterns of uropathogens. Furthermore, the data were collected from the Pathology Center for Diagnosis and Research, Faculty of Medicine, University of Gezira. This facility works as the reference laboratory and encompasses all hospital settings at Wad Medani.
The current study has some limitations. In particular, (1) complete patient data were not available because this was a retrospective study, such as patient setting, inpatient or outpatient status, and comorbidity status. (2) Furthermore, a few bacterial isolates were not recognized at the species level, and a few antimicrobial susceptibility tests were not performed due to the acquisition of antibiotic disks. (3) In addition, some antimicrobial agents, such as vancomycin, linezolid for GPB, meropenem, and piperacillin/tazobactam for GNB, despite their useful therapeutic options, were excluded from the study because they tested for less than 20% of specific bacteria.
Conclusions
This study reported a moderate uropathogen isolation rate of 41.8%. S. aureus and E. coli were the most frequently isolated bacteria, the vast majority of which were from female patients. Remarkably, amikacin was the most sensitive drug to GNB and GPB, while the most resistant drug to GBP was cotrimoxazole, and GNB was ampicillin. Incorporating these findings allows for the planning of long- and short-term strategies as well as the use of effective empirical antibiotic choices for UTIs such as amikacin and levofloxacin.
Ethical Approval
The study protocol was approved by the Ethical Committee, Faculty of Medicine, University of Gezira (7/9/2023). Patient consent was also waived by the Ethical Committee, Faculty of Medicine, University of Gezira (7/9/2023) because this was a retrospective study in which the samples were collected for diagnostic purposes independently of the study, and the data were provided to us anonymously. This study complied with the Declaration of Helsinki.
Disclosure
The authors declare no conflicts of interest in this work.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Additional information
Funding
References
- Firissa YB, Shelton D, Azazh A, Engida H, Kifle F, Debebe F. Prevalence and antimicrobial sensitivity patterns of uropathogens, in tikur anbessa specialized hospital emergency medicine department Addis Ababa, Ethiopia. Infect Drug Resist. 2023;16(March):1649–1656. doi:10.2147/IDR.S402472
- Kostakioti M, Hultgren SJ, Hadjifrangiskou M. Molecular blueprint of uropathogenic Escherichia coli virulence provides clues toward the development of anti-virulence therapeutics. Virulence. 2012;3(7):592–594. doi:10.4161/viru.22364
- Mandracchia VJ, Hayes DW, Yoho RM, Hayes MF. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nat Rev Microbiol. 2016;13(March):34. doi:10.1038/nrmicro3432.Urinary
- Mohamed AMB. Clinical epidemiology and antibiogram of UTI patients attended different hospital in Khartoum, Sudan. Clin Microbiol. 2017;6(5):301. doi:10.4172/2327-5073.1000301
- Ibrahim Shebl R. Frequency and antimicrobial resistance pattern among bacterial clinical isolates recovered from different specimens in Egypt. Cent African J Public Heal. 2019;5(1):36. doi:10.11648/j.cajph.20190501.16
- Melkie DA, Internist T. Food, Medicine and Healthcare Administration and Control Authority of Ethiopia Standard Treatment Guidelines for General Hospital Diseases Investigations Good Prescribing & Dispensing Practices for Better Health Outcomes. Third Edi.; 2014.
- World Health Organization. Antimicrobial Resistance: global Report on Surveillance. World Health Organization; 2014.
- Okeke IN, Axminarayan RL, Bhutta ZA, et al. Antimicrobial resistance in developing countries. Lancet Infect Dis. 2005;19(5):481–493.
- Tambekar DH, Dhanorkar DV. The prevalence and antibiogram of potential bacterial pathogens in clinical specimens. In: 46th Annual Conference of Association of Microbiologist of India. Hyderabad: Department of Microbiology, Osmania University; 2005.
- El Kholy A, Baseem H, Hall GS, Procop GW, Longworth DL. Antimicrobial resistance in Cairo, Egypt 1999-2000: a survey of five hospitals. J Antimicrob Chemoth. 2003;51(3):625–630. doi:10.1093/jac/dkg101
- Holloway K, Mathai E, Gray A, Community-Based Surveillance of Antimicrobial Use and Resistance in Resource-Constrained Settings Project Group. Surveillance of community antimicrobial use in resource-constrained settings - experience from five pilot projects. Trop Med Int Heal. 2011;16(2):152–161. doi:10.1111/j.1365-3156.2010.02695.x
- Clinical and Laboratory Standards Institute, Testing AS. M100 Performance Standards for Antimicrobial. 30th Edition ed. Wayne, PA, USA: Clinical and laboratory Standards Institute; 2020.
- Cheesbrough M. District Laboratory Practice in Tropical Countries. second edition ed. Cambridge university press; 2006.
- Graham JC, Galloway A. The laboratory diagnosis of urinary tract infection. J Clin Pathol. 2001;54(12):911–919. doi:10.1136/jcp.54.12.911
- WHO Regional Office for South-East Asia. Quality Assurance in Bacteriology and Immunology. Second. ISBN. 2014. 92. 9022 2118.
- Muhammad A, Khan SN, Ali N, Rehman MU, Ali I. Prevalence and antibiotic susceptibility pattern of uropathogens in outpatients at a tertiary care hospital. New Microbes New Infect. 2020;36:100716. doi:10.1016/j.nmni.2020.100716
- Worku GY, Alamneh YB, Abegaz WE. Prevalence of bacterial urinary tract infection and antimicrobial susceptibility patterns among diabetes mellitus patients attending zewditu memorial hospital, Addis Ababa, Ethiopia. Infect Drug Resist. 2021;14:1441–1454. doi:10.1111/j.1365-3156.2010.02695.x
- Edrees WH, Alaleem A, Anbar M. Prevalence and Antibacterial Susceptibility of Bacterial Uropathogens Isolated from Pregnant Women in Sana’a, Yemen. PSM Biol Res. 2020;5(4):157–165.
- Hamdan HZ, Kubbara E, Adam AM, Hassan OS, Suliman SO, Adam I. Urinary tract infections and antimicrobial sensitivity among diabetic patients at Khartoum, Sudan. Ann Clin Microbiol Antimicrob. 2015;14(26):1–6. doi:10.1186/s12941-015-0082-4
- Islam MA, Islam MR, Khan R, et al. Prevalence, etiology and antibiotic resistance patterns of community-Acquired urinary tract infections in Dhaka, Bangladesh. PLoS One. 2022;17(9 September):1–13. doi:10.1371/journal.pone.0274423
- Al-naqshbandi AA, Chawsheen MA, Abdulqader HH. isolated from urine specimens received in rizgary hospital — erbil. J Infect Public Health. 2019;12(3):330–336. doi:10.1016/j.jiph.2018.11.005
- Garoy EY, Ghebrehiwet MA, Fessehaye N, et al. Patterns and trends of antimicrobial resistance in bacterial isolates from urine cultures in Eritrea, 2010 – 2021: a secondary dataset analysis. available at Research Square; 2024.
- Idbeis HI, Arian SR, Aidy AL. Analysis of bacterial uropathogens and antimicrobial resistance profiles among diabetic patients in Al - Kut City, Iraq. j Sci Med Life. 2024;2(4):61–70.
- Almutawif YA, Eid HMA. Prevalence and antimicrobial susceptibility pattern of bacterial uropathogens among adult patients in Madinah, Saudi Arabia. BMC Infect Dis. 2023;3:1–11.
- Foxman B. Urinary tract infection syndromes occurrence, recurrence, bacteriology, risk factors, and disease burden. Infect Dis Clin NA. 2014;28(1):1–13. doi:10.1016/j.idc.2013.09.003
- Rowe TA, Juthani-mehta M. Urinary tract infection in older adults. Aging Health. 2013;9(5):519–528.
- Ahmed H, Farewell D, Jones HM, Francis NA, Paranjothy S, Butler CC. Incidence and antibiotic prescribing for clinically diagnosed urinary tract infection in older adults in UK primary care. PLoS One. 2018;13(1):2004–2014. doi:10.1371/journal.pone.0190521
- Prabhala S, Sundaresan A, Varaiya A, Carolina N. Prevalence of bacterial isolates and change in their antibiotic susceptibility patterns in urinary tract infections- A five year retrospective study. J Comm Health Manag. 2024;10(4):157–162. doi:10.18231/j.jchm.2023.034
- Robinson D, Cardozo LD. The role of estrogens in female lower urinary tract dysfunction. Urology. 2003;62(4 SUPPL. 1):45–51. doi:10.1016/S0090-4295(03)00676-9
- Negri M, Lima BM, Batista S, et al. Prevalence and antimicrobial resistance profile of pathogens isolated from patients with urine tract infections admitted to a university hospital in a medium-sized Brazilian city Mariana. Rev Inst Med Trop São Paulo. 2024:1–11. doi:10.1590/S1678-9946202466003
- Hossain J, Azad AK, Shahjahan M, Ferdous J. Prevalence, antibiotic resistance pattern for bacteriuria from patients with urinary tract infections. Health Sci Rep. 2023;2024(October). doi:10.1002/hsr2.2039
- Belete Y, Asrat D, Woldeamanuel Y, Yihenew G, Gize A. Bacterial profile and antibiotic susceptibility pattern of urinary tract infection among children attending felege hiwot referral hospital, bahir dar, northwest Ethiopia. Infect Drug Resist. 2019;12:3575–3583. doi:10.2147/IDR.S217574
- Ahmed LM, Omer SS, Mahjaf GM, Altaher TA, Hamad MM. Determination of bacteriological profile of antimicrobial susceptibility testing among diabetic patients with urinary tract infections in. SAR J Pathol Microbiol. 2023;4(3):24–29. doi:10.36346/sarjpm.2023.v04i03.001
- Mareș C, Petca RC, Popescu RI, Petca A, Geavlete BF, Jinga VU. Antibiotic resistance evolution in a female population: a sequential multi-year comparative analysis. Antibiotics. 2023;12(6):948. doi:10.3390/antibiotics12060948
- Bhola P, Chb MB, Micro FSA, et al. Antimicrobial susceptibility patterns of uropathogens isolated from pregnant women in KwaZulu-Natal Province: 2011 - 2016. S Afr Med J. 2020;110(9):872–876. doi:10.7196/SAMJ.2020.v110i9.14468