
Abstract
Background
Adenovirus pneumonia progresses rapidly, with a high rate of progression to severe pneumonia, but the early clinical manifestations lack specificity and are not easy to be recognized.
Methods
Reviewing the relevant literatures, we studied and summarized the early recognition, clinical features and treatment outlook of severe adenovirus pneumonia Case Presentation: An 11-year-old child with community-acquired pneumonia, with influenza A antigen positive by colloidal gold, which further developed into acute respiratory distress syndrome after hospitalization. Three days later, adenovirus was detected positively by PCR of throat swab and diagnosed as severe adenovirus pneumonia. After aggressive treatment, her condition improved and was discharged from the hospital.
Conclusion
Clinically, adenovirus combined with influenza virus infection is uncommon, and adenovirus infection is even rarer in adolescent children.
Introduction
Globally, acute respiratory diseases are associated with high morbidity and mortality, with viral respiratory infections accounting for approximately 80% of the cases, primarily, including influenza and respiratory syncytial viruses, coronaviruses, adenoviruses, and rhinoviruses.Citation1 Adenovirus pneumonia accounts for approximately 3.5–11% of community-acquired pneumonia (CAP) in children.Citation2 The highest incidence of adenovirus infection is between 6 months and 2 years of age, with >80% of adenovirus pneumonia cases occurring in children <4 years of age.Citation3,Citation4 Adenoviruses are highly contagious in closed or crowded environments and universally found in a susceptible population.Citation5
The most common sites of human adenovirus (HAdV) infection include the respiratory tract, cornea, intestinal tract, and urinary tract.Citation6 Most adenoviral respiratory infections are mild to moderate and self-limiting; however, they can also be life-threatening or cause severe sequelae.Citation7 Adenoviruses can directly infect lung tissue, cause cell lysis and necrosis, and activate the body’s immune system, leading to a severe inflammatory response.Citation2,Citation8 If the infection progresses to multiple organ dysfunction syndrome, the fatality rate can increase to more than 50%.Citation9 It has been found that adenovirus infection causes a stronger immune-inflammatory response than other pathogens, with a high proportion of children having shortness of breath and respiratory distress, faster disease progression, and a tendency to develop mixed infections with other pathogens during the course of the disease.Citation10,Citation11 Therefore, it is crucial to investigate the role of early recognition and the clinical features of severe adenovirus pneumonia (SAP). Early recognition helps clinicians to detect severe cases and avoid treatment delays.
Case Report
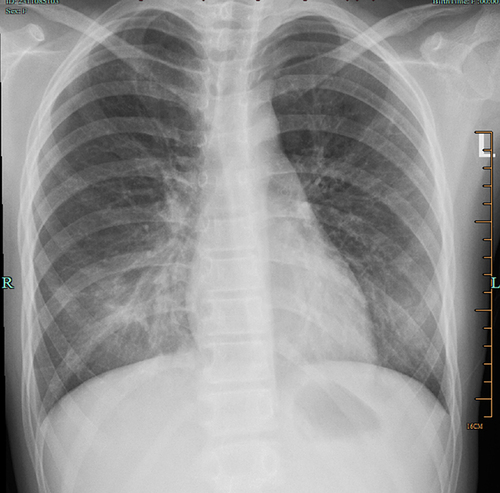
The patient was an 11-year-old girl with no known medical history and was admitted to the hospital with a history of fever and cough for 2 days. The rapid test for influenza antigen (colloidal gold method) conducted at the outpatient clinic visit during the initial stages of the disease was positive for influenza A virus. After two days of oral treatment with oseltamivir, the patient continued to have a recurrent high fever and worsening cough, with the chest computed tomography (CT) showing inflammation in both lungs (). After 2 hours of hospital admission, the patient presented with progressive dyspnea, paroxysmal chest pain, and a rapid increase in wet rales on auscultation of both lungs. Oxygen saturation (SpO2) decreased to 85%; C-reactive protein (CRP) increased from 7.3 mg/L to a maximum of 220.5 mg/L (normal range: 0–6 mg/L); D-dimer (D-D), 4.67 mg/L (normal range: 0–0.5 mg/L); activated partial thromboplastin time (APTT), 45.2 s (normal range: 23–31.3 s); procalcitonin (PCT) 15.63 ng/mL (normal range: 0–0.5 ng/mL); lactate dehydrogenase (LDH) 399 U/L (normal range: 120–250 U/L); and pulmonary exacerbations were observed on imaging (); and negative nucleic acid tests for the following respiratory pathogens: respiratory syncytial virus (RSV), adenovirus, Mycoplasma pneumoniae, influenza A virus, influenza B virus, and rhinovirus. Early on, she was provided with an oxygen mask and administered antibiotics, glucocorticoids, and gamma globulin. Three days later, the child’s condition improved, and a re-examination of the throat swab via PCR showed a positive result for Adenovirus. The administration of oxygen supply, antibiotics, and hormones was gradually reduced. After 5 days, the chest radiograph indicated obvious absorption of lung inflammation (). The levels of CRP, PCT, APTT, and LDH significantly decreased. The wet rales in both lungs disappeared, and she was discharged.
Figure 1 (A–C) Chest CT on the first day of admission: multiple flaky, cloudy lungs with increased density and blurred edges.
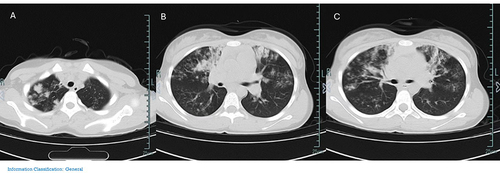
Figure 2 X-ray on the second day of admission: large patches of increased density shadow on both lungs with blurred edges.

Figure 3 X-ray on the eighth day of admission: the two pneumonia cases were significantly absorbed.
Discussion
Adenoviruses are important pathogens that cause CAP in children. In the early stages of adenovirus pneumonia, the clinical manifestations lack specificity. However, SAP rapidly progresses and can lead to respiratory failure, toxic encephalopathy, hemophagocytic lymphohistiocytosis, postinfectious occlusive bronchiolitis, and even death.Citation4,Citation12,Citation13 Adenovirus pneumonia is much more severe (47.7%)Citation13 than common pneumonia (1–2%),Citation13 and the mortality rate of severe HAdV pneumonia can be >50%.Citation13
Zheng et alCitation14 concluded that newborns with maternal immunity can resist adenovirus infection. However, as the mothers’ immune defenses wane over time and newborns have an immature immune system, children around one year of age are susceptible to adenovirus infection. Wang et alCitation15 found that levels of anti-HAdV neutralizing antibodies peaked in 6-month-old children following adenovirus infection, with a temporary trough occurring between 6 months and 3 years of age, followed by a gradual increase after 3 years of age. Zhang et alCitation3 concluded that adenovirus-specific IgG antibodies are acquired via the placenta at birth in >90% of children, and 6 months later, they are detectable in only about 14% of children. Several studies have pointed out the differences in the incidence, clinical features, and prognosis of SAP in children of different ages. This case is of an 11-year-old adolescent girl who presented with adenovirus pneumonia, which is uncommon, and the progression to SAP is even rarer. Thus, the influencing factors responsible for SAP at this age are worth exploring.
While investigating the mechanisms underlying the cytokine storm of influenza viruses, Gu et alCitation16 found that estrogen regulates the function of multiple immune cells, with low estrogen enhancing the proinflammatory cytokine response and affecting the severity of the disease. Li et alCitation17 showed that estrogen suppresses activated inflammatory and immune response biomarker genes; hence, relatively low mortality is observed in young female patients with COVID-19. Studies by Jiu et alCitation18 and Harding et alCitation19 also supported the anti-inflammatory effect of estrogen. The child in this case was menstruating when she contracted adenovirus and had low estrogen levels. Therefore, we surmise that low levels of estrogen also affect the severity of adenovirus pneumonia.
It has been found that approximately 14–60% of children with SAP have severe respiratory sequelae, such as occlusive bronchiolitis obliterans and bronchiectasis.Citation20 Thus, early identification of severely ill children and effective treatment is essential.
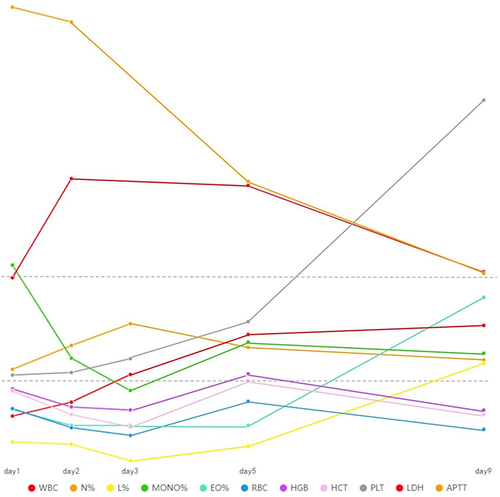
There have been many studies examining the early recognition of severe adenovirus infection. Tian et alCitation21 confirmed that the levels of N%, CRP, PCT and LDH in children with severe ADVP were significantly higher than those in the mild group. Zhang et alCitation22 found that leukocytosis, mycoplasma pneumoniae co-infection and high blood viral load may be risk factors for severe adenovirus pneumonia in children with normal immune function. Fan et alCitation23 found that the levels of MONO%, LYMPH%, EO%, RBC, HGB, HCT, PLT and PCT decreased with the increase of disease severity. Xu et alCitation24 also indicated that PCT, LDH, AST, ferritin, D-dimer and other indexes were significantly increased in severe adenovirus infection. As shown in the figure above ( and ), our study found that as the disease worsened, indexes such as N%, CRP, PCT, LDH, APTT and D-D increased, while indexes such as HCT, RBC, EO%, MONO% and L% decreased, which was similar to the results of existing studies.
Table 1 Changes in Laboratory Indicators
Figure 4 Trends of laboratory indicators over time.
During the initial assessment of adenovirus, it is difficult to distinguish whether there is a bacterial infection because adenovirus infection can cause a strong inflammatory response, resulting in a significant increase in WBC and CRP.Citation10,Citation25 More than 90% of previously reported cases have been treated with antibiotics, which have no therapeutic effect on adenoviruses.Citation26 Thus, accurate and rapid diagnosis is critical to reduce antibiotic prescription and consumption and also antibiotic resistance. Compared with traditional antigen detection and virus culture methods, polymerase chain reaction (PCR) possesses a higher detection capability of respiratory viruses,Citation27 and it can be widely used in clinical practice. However, antigen detection has the advantages of rapid achievement of results, low cost, and low maintenance, and it continues to be widely used in outpatient and emergency departments.
In this case, the rapid antigen test was positive for the influenza virus using the colloidal gold method but negative with PCR. The possible reasons are as follows: (1) False positive antigen test results due to cross-reaction of similar proteins between influenza virus and adenovirus; (2) Occurrence of RNA degradation during specimen preservation or processing, resulting in false negative nucleic acid tests; (3) False positive results due to nonstandardization of the antigen detection reagent itself or the sampling operation or the naked eye observation reaction line is fuzzy; or (4) Effective oral oseltamivir treatment leading to a significant decrease in viral load. Moreover, some studies found that positive rapid influenza diagnostic test was proportional to viral load in nasopharyngeal samples.Citation28 When a sample for PCR was collected from our patient for the first time, the lower respiratory tract infection was severe, and thus, low viral load in the oropharynx could result in false negative nucleic acid detection.
In addition, the occurrence of adenovirus along with Mycoplasma pneumoniae is common,Citation29 and blood examination revealed that the child, in this case, was positive for Mycoplasma IgM and negative for Mycoplasma nucleic acids, confirming the observation of Huang Hao et alCitation30 that false positive for Mycoplasma IgM antibody may occur in adenovirus infection. Compared with pneumonia caused by M. pneumoniae, children with adenovirus pneumonia have a longer duration of fever, a wider range of lung lesions, a higher proportion of bilateral pneumonia and severe pneumonia, and a higher incidence of hypoxemia.Citation8
Imaging can also help in early identification of adenovirus pneumonia. Adenoviruses can cause focal or lobar degeneration, with the primary imaging features similar to those typical of bacterial pneumonia, thereby misleading the diagnosis.Citation31 In this case, CT showed multiple clusters of lesions in both lungs during the initial stages of the disease, with high density, blurred edges, and centripetal distribution. This observation was similar to the chest imaging features of patients with severe adenovirus infection proposed by Uljing et alCitation32 segmental and lobular parenchymal infiltration, edge of consolidation is fuzzy, reinforcement is uniform, and most of them have centripetal distribution.
Currently, there are no specific antiviral drugs approved for the treatment of adenoviral infections. Although cidofovir administration has been successful for the treatment of severe adenovirus infections in several cases,Citation6,Citation33–35 its exact efficacy and safety have not been verified, and thus, it is not currently widely used for the treatment of HAdV.Citation34 The main treatment strategies for SAP in children are supportive therapy, immunomodulatory therapy, and respiratory support therapy, including oxygen inhalation, mechanical ventilation, and extracorporeal membrane oxygenation. The timing of transbronchoscopic alveolar lavage in children with SAP remains controversial.Citation36 Glucocorticoids possess strong anti-inflammatory and immunosuppressive effects to reduce lung inflammation in severe pneumonia and prevent respiratory failure.Citation36,Citation37 As the main immune protein of the human body, gamma globulin can inhibit the formation of antigen and antigen complexes, improving the immunity of the body. It can also block Fc receptors on cells, inhibit the production and release of cytokines, and neutralize inflammatory factors, toxins, and related antigens.Citation38 For children with SAP, early administration of gamma globulin can reduce the use of mechanical ventilation, shorten the duration of fever, reduce the incidence of bronchiectasis, and significantly reduce mortality.Citation39
Our study has some limitations. The type of adenovirus is associated with disease severity; however, adenovirus typing was not tested in this retrospective study. This study did not detect the levels of IgE, ferritin, IL-4, adenovirus antibody in blood, and viral load. During follow-up, the patient’s cough disappeared, but chest CT was not reviewed as recommended. Lung recovery is unknown and long-term prognosis cannot be assessed.
Conclusions
For children with pneumonia where the pathogen involved is unclear and a persistent fever is observed accompanied by wheezing, shortness of breath, poor spirit, ineffective antibiotic treatment, and significantly elevated levels of PCT, LDH, D-D, and other indicators, we need to be alert of the possibility of SAP. Although the virus nucleic acid test is the gold standard, in the case of a negative test result, it is still necessary to combine the corresponding clinical manifestations with the laboratory findings and imaging characteristics to provide effective treatment as early as possible. Samples can be collected repeatedly and from multiple sites for nucleic acid testing. Rapid identification of the virus would limit the unnecessary consumption of antibiotics. As the immune mechanism of adenovirus infection is complex and no specific drugs are currently available, future studies should focus on the development of new anti-adenovirus drugs through breakthroughs in the role of cytokines and hormones.
Ethics Approval
Ethical approval for the study was granted and the case details were approved to publish the case details by ShaoXing KeQiao Women And Children’s Hospital.
Consent for Publication
Written informed consent was obtained from the patient’s parents for publication of this case report and any accompanying images. A copy of the written consent is available for review.
Disclosure
The authors report no conflicts of interest in this work.
References
- Zhang N, Wang L, Deng X, et al. Recent advances in the detection of respiratory virus infection in humans. J Med Virol. 2020;92(4):408–417. doi:10.1002/jmv.25674
- Lai X, Zou Y. Progress on immunological pathogenesis of adenovirus pneumonia in children. Int J Pediatr. 2022;49(5). doi:10.3760/cma.j.issn.1673-4408.2022.05.013
- Zhang XP, Yang MY, Zhou X, et al. Clinical features of severe type 7 adenovirus pneumonia: an analysis of 45 cases. Zhongguo Dang Dai Er Ke Za Zhi. 2020;22(5):429–434. doi:10.7499/j.issn.1008-8830.1911174
- Zalcman J, Pasternak Y, Kenan D, et al. Safety of cidofovir treatment for suspected or confirmed adenovirus infection in immunocompetent Pediatric Population. Pediatr Infect Dis J. 2023;43(3):198–202. doi:10.1097/INF.0000000000004186
- Li J, Wei J, Xu Z, et al. Cytokine/chemokine expression is closely associated disease severity of human adenovirus infections in immunocompetent adults and predicts disease progression. Front Immunol. 2021;12:691879. doi:10.3389/fimmu.2021.691879
- Dodge MJ, MacNeil KM, Tessier TM, et al. Emerging antiviral therapeutics for human adenovirus infection: recent developments and novel strategies. Antiviral Res. 2021;188:105034. doi:10.1016/j.antiviral.2021.105034
- Liu MC, Xu Q, Li TT, et al. Prevalence of human infection with respiratory adenovirus in China: a systematic review and meta-analysis. PLoS Negl Trop Dis. 2023;17(2):e0011151. doi:10.1371/journal.pntd.0011151
- Zhang H, Li H, Wang L, et al. Development of a model for early differentiation of adenovirus pneumonia from Mycoplasma pneumoniae pneumonia. Transl Pediatr. 2022;11(11):1766–1775. doi:10.21037/tp-22-6
- Chowdhury F, Shahid ASMSB, Ghosh PK, et al. Viral etiology of pneumonia among severely malnourished under-five children in an urban hospital, Bangladesh. PLoS One. 2020;15(2):e0228329. doi:10.1371/journal.pone.0228329
- Liu J, Deng ZH, Luo WJ, et al. Clinical characteristics between children with adenovirus infection and children with influenza virus infection. Chin J Nosocomiol. 2023;33(1). doi:10.11816/cn.ni.2023-213584
- Mandelia Y, Procop GW, Richter SS, et al. Dynamics and predisposition of respiratory viral co-infections in children and adults. Clin Microbiol Infect. 2021;27(4):631.e1–631.e6. doi:10.1016/j.cmi.2020.05.042
- Zhong H, Dong X. Analysis of clinical characteristics and risk factors of severe adenovirus pneumonia in Children. Front Pediatr. 2021;9:566797. doi:10.3389/fped.2021.566797
- Lin J, Chen Z. Research progress on early identification of severe adenovirus pneumonia in children. Zhejiang Da Xue Xue Bao Yi Xue Ban. 2019;48(5):567–572. Chinese. doi:10.3785/j.issn.1008-9292.2019.10.16
- Zheng L, Liao W, Liang F, et al. Clinical characteristics and outcomes of severe pneumonia in children under 5 years old with and without adenovirus infection in Guangzhou. Front Pediatr. 2021;9:599500. doi:10.3389/fped.2021.599500
- Wang X, Tan X, Li Q. The difference in clinical features and prognosis of severe adenoviral pneumonia in children of different ages. J Med Virol. 2022;94(7):3303–3311. doi:10.1002/jmv.27680
- Gu Y, Zuo X, Zhang S, et al. The mechanism behind influenza virus cytokine storm. Viruses. 2021;13(7):1362. doi:10.3390/v13071362
- Li F, Boon ACM, Michelson AP, et al. Estrogen hormone is an essential sex factor inhibiting inflammation and immune response in COVID-19. Sci Rep. 2022;12(1):9462. doi:10.1038/s41598-022-13585-4
- Jiu T, Ge RL, Bai Z, Ge R-L, Bai Z. Biofunctional roles of estrogen in coronavirus disease 2019: beyond a steroid hormone. Front Pharmacol. 2022;13:1003469. doi:10.3389/fphar.2022.1003469
- Harding AT, Heaton NS. The impact of estrogens and their receptors on immunity and inflammation during infection. Cancers. 2022;14(4):909. doi:10.3390/cancers14040909
- Zhou W, Chen J, Xi Z, et al. Characteristics of Lung microbiota in children’s refractory mycoplasma pneumoniae pneumonia coinfected with human adenovirus B. Can J Infect Dis Med Microbiol. 2022;2022:7065890. doi:10.1155/2022/7065890
- Tian X, Fan Y, Wang C, et al. Seroprevalence of neutralizing antibodies against six human adenovirus types indicates the low level of herd immunity in young children from Guangzhou. China Virol Sin. 2021;36(3):373–381. doi:10.1007/s12250-020-00307-1
- Zhang R, Wang H, Tian S, et al. Adenovirus viremia may predict adenovirus pneumonia severity in immunocompetent children. BMC Infect Dis. 2021;21(1):213. doi:10.1186/s12879-021-05903-4
- Fan H, Cui Y, Xu X, et al. Validation of a classification model using complete blood count to predict severe human adenovirus lower respiratory tract infections in pediatric cases. Front Pediatr. 2022;10:896606. doi:10.3389/fped.2022.896606
- Xu N, Chen P, Wang Y. Evaluation of risk factors for exacerbations in children with adenoviral pneumonia. Biomed Res Int. 2020;2020:4878635. doi:10.1155/2020/4878635
- Lu Z, Wang H, Bao Y, et al. Retrospective study of an adenovirus pneumonia outbreak in Shenzhen in 2017. Virol Sin. 2021;36(3):555–558. doi:10.1007/s12250-021-00393-9
- Oliveira FRC, Macias KM, Rolli PA, et al. Management of acute respiratory distress syndrome in a child with adenovirus pneumonia: case report and literature review. Rev Paul Pediatr. 2020;38:e2018280. doi:10.1590/1984-0462/2020/38/2018280
- Noureddine FY, Chakkour M, El Roz A, et al. The emergence of SARS-CoV-2 variant(s) and its impact on the prevalence of COVID-19 cases in the Nabatieh Region. Lebanon. 2021;9(2):40. doi:10.3390/medsci9020040
- Huang PY, Su CP, Liu SW, et al. Correlation between negative rapid influenza diagnostic test and severe disease in hospitalized adults with laboratory-confirmed influenza virus infection. Am J Trop Med Hyg. 2020;103(4):1642–1648. doi:10.4269/ajtmh.19-0444.28
- Peng L, Zhong LL, Huang Z, et al. Clinical features of Mycoplasma pneumoniae pneumonia with adenovirus infection in children. Chin J Contemp Pediatr. 2021;23(10):1033–1037. doi:10.7499/j.issn.1008-8830.2107080
- Huang H, Chen Y, Ma L, et al. Analysis of the clinical features and the risk factors of severe adenovirus pneumonia in children. Chin J Pediatr. 2021;59(1). doi:10.3760/cma.j.cn112140-20200704-00687
- Chen X, Lv J, Qin L, et al. Severe adenovirus pneumonia requiring extracorporeal membrane oxygenation support in immunocompetent children. Front Pediatr. 2020;8:162. doi:10.3389/fped.2020.00162
- Li J, Yue X, Guo XX, et al. Clinical characteristics and CT diagnosis analysis of children patients with severe adenovirus pneumonia. Chin J CT MRI MAR. 2019;17(3):113. doi:10.3969/j.issn.1672-5131.2019.03.001
- Alcamo AM, Wolf MS, Alessi LJ, et al. Successful use of cidofovir in an immunocompetent child with severe adenoviral sepsis. Pediatrics. 2020;145(1):e20191632. doi:10.1542/peds.2019-1632
- Ko JH, Lim JU, Choi JY, et al. Early cidofovir administration might be associated with a lower probability of respiratory failure in treating human adenovirus pneumonia: a retrospective cohort study. Clin Microbiol Infect. 2020;26(5):646.e9–646.e14. doi:10.1016/j.cmi.2019.10.012
- Shi J, Zhou Y, Wang F, et al. A case series of children with adenovirus pneumonia: three-year experiences in a tertiary PICU. BMC Pediatr. 2020;20(1):375. doi:10.1186/s12887-020-02269-5
- Fan H, Lu G. Progress in early recognition and treatment of severe adenovirus pneumonia in children. Chin J Appl Clin Pediatr. 2023;38(11). doi:10.3760/cma.jcn101070-20230629-00543
- Ikuta K, Ejima A, Abe S, et al. Control of immunity and allergy by steroid hormones. Allergol Int. 2022;71(4):432–436. doi:10.1016/j.alit.2022.07.006
- Cai S, Zhu CH, Chen FG, et al. Establishment of a risk model for severe adenovirus pneumonia and prospective study of the timing of intravenous immunoglobulin therapy in children. Chin J Contemp Pediatr. 2023;25(6):619–625. doi:10.7499/j.issn.1008-8830.2211069
- Fan H, Chen C, Xu X, et al. Application strategy of intravenous immunoglobulin in children with severe adenovirus pneumonia. Chin J Appl Clin Pediatr. 2022;37(9). doi:10.3760/cma.j.Cn101070-20210402-00385