
Abstract
This is a systematic review of cases with Lemierre’s syndrome (LS) in the past 5 years. LS is characterized by sepsis often evolving after a sore throat or tonsillitis and then complicated by various septic emboli and thrombosis of the internal jugular vein. Symptoms include sepsis, pain, and/or swelling in the throat or neck, as well as respiratory symptoms. Laboratory findings show elevated infectious parameters and radiological findings show thrombosis of the internal jugular vein and emboli in the lungs or other organs. The syndrome is often associated with an infection with Fusobacterium necrophorum. We found a total of 137 cases of LS, of which 47 were infected with F. necrophorum and others with Staphylococcus and Streptococcus. Complications of this rare but severe disease included osteomyelitis, meningitis, and acute respiratory distress syndrome. Mortality was extremely high in the pre-antibiotic era but has diminished with the advent of antibiotics. This review showed a mortality rate of only 2% of which none of the cases involved fusobacteria. Duration of treatment varied; a 4–6-week course of carbapenem or piperacillin/tazobactam in combination with metronidazole was optimum. Other treatment options included anticoagulants in 46% of cases, which is unwarrantedly high, as to date, no evidence of the positive effects of anticoagulants in LS exists. Only two cases had ligation of the internal jugular vein performed. This review confirms the rare, but severe aspects of LS. Mortality from LS in this day and age appears to be low, however the syndrome is difficult to recognize, and still requires the full attention of the clinician.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Definition
Lemierre’s syndrome (LS) takes its name after the French bacteriologist André-Alfred Lemierre, who first described the syndrome in 1936.Citation1 The syndrome is defined by a pharyngeal infection, complicated by septicemia and internal jugular vein thrombosis followed by septic emboli. Due to the introduction of antibiotics, LS has aptly been referred to as “the forgotten disease”. The most commonly involved bacteria is Fusobacterium necrophorum but other bacteria such as fusobacteria, Streptococcus, Staphylococcus, and Enterococcus are commonly found in cultures.Citation2 Other bacteria, such as Klebsiella Pneumoniae have rarely been described in middle-aged persons with newly diagnosed type 2 diabetes.Citation3
Patients with LS present with a prolonged sore throat, neck pain, and often with fever.Citation4 Patients are often young (age 16–30 years) and otherwise healthy, but appear acutely ill with tachycardia, tachypnea, hypotension, and a poor saturation (often <95%).Citation2,Citation3,Citation5,Citation6 Laboratory findings showed leukocytosis with dominating neutrocytosis and elevated C-reactive protein as well as signs of organ failure, such as elevated liver enzymes. Imaging of the internal jugular vein showed thrombosis.Citation2,Citation5
Complications to this severe syndrome include a mortality rate as high as 10%,Citation3 especially when antibiotic treatment is delayed.Citation7 Other less severe complications include metastatic infections in joints, internal organs (often lungs), and/or the brain.Citation6
Fusobacterium necrophorum has a reputation for being resistant to penicillin, thus the drugs of choice have primarily been β-lactamase-resistant β-lactams, such as piperacillin–tazobactam, even though many strains are sensitive to penicillin in combination with metronidazole.Citation4,Citation7
The syndrome remains difficult to diagnose due to its low incidence and absence of pathognomonic symptoms. Thus, symptoms mimic other common diseases. Botros et alCitation8 have described this dilemma in an excellent manner.
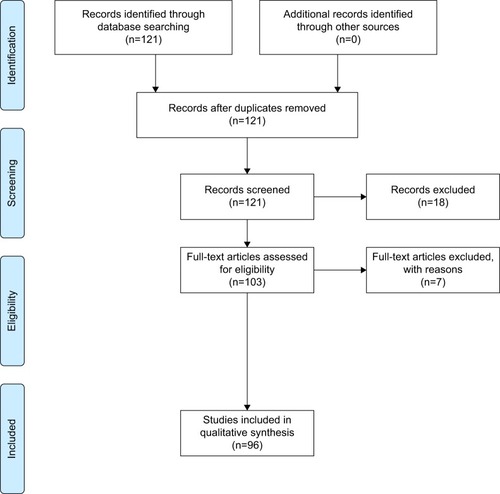
The present study is a review of the publications in the past 5 years concerning LS. A PubMed search was carried out using the MeSH terms “Lemierre Syndrome/classification”, “Lemierre Syndrome/diagnosis”, “Lemierre Syndrome/etiology”, and “Lemierre Syndrome/therapy”. Inclusion criteria were: studies published in English language, dealt with human subjects, and apublication date within the last 5 years. The search elicited 121 papers, of which the abstracts were read, and 18 papers were excluded as they did not concern LS. The full text of 103 papers was read, after which seven were excluded, since they did not include any data on patients/cases. A total of 137 cases were included for this review ().
Figure 1 Lemierre’s syndrome review: study inclusion and exclusion flow diagram.
Notes: Figure created using PRISMA 2009 flow diagram software from Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group (2009). Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6(7):e1000097 doi: 10.1371/journal.pmed.1000097. For more information, visit www.prisma-statement.org.Citation94
Diagnosis
A definite diagnosis of LS should be made based on the following findings:Citation7,Citation9
a recent pharyngeal illness,
complicated by septic emboli,
as well as either thrombosis of the internal jugular vein or findings of F. necrophorum in blood cultures.
Clinical
This review yielded at total number of 137 casesCitation2,Citation3,Citation5,Citation6,Citation8,Citation10–Citation90 including both case reports and minor reviews. The major clinical characteristics of LS are reported in . Twenty-four percent of the cases were presented with a complaint in the pharyngeal area (tonsillitis, pharyngitis, common sore throat), whereas a few came with an initial complaint of a swelling of the neck,Citation37,Citation61,Citation64–Citation66,Citation73,Citation82 due to either the thrombus itself or an abscess located in the neck region. Only eleven cases were described with initial difficulties in the dental region,Citation6,Citation16,Citation18,Citation42,Citation46 the otogenic region,Citation18,Citation19,Citation68,Citation77 or the central nervous system.Citation29,Citation45 Atypical presentations included seizuresCitation90 and blindness.Citation60,Citation63 Half the cases were presented with sepsis at their first evaluation in the hospital, and at least 17 cases were intubated (not reported in all articles), underlining the severity of LS. Interestingly, the location of the primary infection is an important prognostic factor: infection in the oropharyngeal location (compared to other sites) was associated with a higher risk of longer intensive care unit stays due to complications such as respiratory problems.Citation18 At least 37 of the cases in this review were not in the age group usually associated with LS, rather they were older than 30 years or younger than 15 years. Eleven were children younger than 15 years, who presented with a variety of symptoms, including pharyngitisCitation59 and/or pneumoniaCitation43 and also more severe symptoms such as meningitisCitation45 or febrile seizures.Citation58 None of the children in this review died. In the older age group too, common complaints such as pneumoniaCitation40 dominated, but also here more severe symptoms/illnesses were seen, such as multiple emboli.Citation38 It had previously been found that other diseases underlie LS in these older patients, such as diabetes or cancer.Citation91
Table 1 Common clinical characteristics of Lemierre’s syndrome
The overall mortality was 2%, death was reported only in two of 137 cases. This is considerably less than previously reported.Citation91 Briefly, no fusobacteria were cultured in the following two cases: 1) a diabetic patient with tonsillitis and peritonsillar abscess (K. pneumoniae positive culture)Citation3 and 2) a 79-year old with tonsillitis and multiple septic emboli in lungs, liver, heart, kidney, and joints (Streptococcus anginosus positive culture).Citation38 In a previous study, we presented morbidity and mortality in patients with positive cultures in blood, sputum, or pleural effusion with fusobacteria versus Staphylococcus aureus and showed that infections with fusobacteria were associated with a significantly lower 1-year mortality.Citation92 Only one patient in the fusobacteria group in that study had LS,Citation49 but generally mortality in the fusobacteria group was due to comorbidity and not due to severity of the infection itself. It could be speculated that publication bias plays an important role when trying to estimate the mortality in this rare syndrome. It could go both ways: fatal cases with a lesser likelihood to be published due to the simple fact that these cases could be missed and not diagnosed at all; or fatal cases could have a higher likelihood to be published due to the interest in why these cases become fatal.
Microbiological
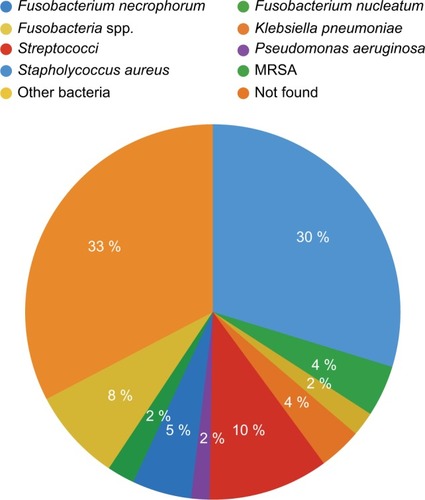
In this review, 96 cases reported a causative microbiological agent; the majority of the cases were infections with F. necrophorum (41), Fusobacterium nucleatum (6), and unspecified fusobacteria (3), others were infections with microbiological agents such as Streptococcus (17), including methicillin-resistant S. aureus, and S. aureus (six cases) (). These findings suggest that F. necrophorum is still the major microbiological agent in LS, but it could also be due to reporting bias, as clinicians and/or editors only approve “the forgotten disease” when fusobacteria is present in relevant cultures. Fusobacterium necrophorum (and other fusobacteria) is an obligate anaerobic bacterium and is notoriously difficult to culture, requiring a longer incubation period than other bacteria.Citation92 A large proportion of the cases did not report a microbiological agent (n=40). As with other bacteria, cultures can be false negative if antibiotics are administered before sample collection. Whether the cases without a positive culture of F. necrophorum (or other fusobacteria) are true cases of LS is debatable. In the review by Riordan,Citation9 it was suggested that F. necrophorum is in fact present in all patients with LS but goes undetected due to various circumstances and that the bacteria detected would be unable to cause LS on its own. However, this quite stern conclusion has not been accepted as a common rule in the clinical community, and so far a clinical diagnosis of LS is still valid if the bacteria either go undetected or turn out to be Streptococcus or some other known pathogenic bacteria.
Figure 2 Distribution of bacterial agent.
Abbreviation: MRSA, methicillin-resistant Staphylococcus aureus.
Imaging
Concerning the diagnosis of the infectious thrombosis, the optimal imaging tool is still debated. Ultrasonography is a radiation-free and easily available bedside tool, but it has the disadvantage of being less sensitive for recently formed thrombosis material, with a lesser echogenicity, as well as difficulties in the deeper tissue areas around the clavicle and mandible.Citation93 Magnetic resonance imaging (MRI) is an excellent method for visualizing all anatomic structures as well as the thrombosis and/or septic emboli. However, MRI is expensive and usually not readily available. Computed tomography (CT) scans are cheaper and available in most hospitals, but it involves radiation exposure. In this review, the vast majority of cases (95%) with thrombophlebitis of the internal jugular vein were diagnosed by CT scans. Ultrasonography was used by the remaining cases, but none used MRI.
In total, ten cases (7%) had no or unknown thrombus during their disease. The majority of cases (84%) had thrombosis of the internal jugular vein, while a few (9%) cases had thrombosis of other veins, such as the facial vein, sinus transversus, or vena ophthalmicus.Citation47,Citation60
A larger proportion of cases (71 cases) had septic emboli in the lungs, but septic emboli were also seen in other organs, such as the liver,Citation12,Citation38,Citation87 spleen,Citation81 joints,Citation38,Citation70 heart,Citation38 and the central nervous system,Citation29,Citation31 even though in smaller numbers.
Management
Antibiotics
All but a few rare cases received antibiotic treatment during their hospital stay. Multiple different regimens of the antibiotic of choice were used. Resistance to penicillin was not found at an increased frequency. However, carbapenem and piperacillin/tazobactam were commonly used, either as monotherapy or in combination with metronidazole, and 98% of the cases (mortality n=2) were treated successfully. The mean duration of antibiotic treatment was 4 weeks, but it ranged from 10 days to 8 weeks. The reason for the choice of a particular duration was not explained in any of the included papers. RiordanCitation9 highlights the features of metronidazole and also recommends it as monotherapy, which was not seen in any of the cases in this review. He especially praises metronidazole for its profound activity against all strains of Fusobacterium spp., its good penetration within the tissue, and its good oral availability. Regarding treatment duration, RiordanCitation9 and others have, similar to this review, found a wide range of treatment duration; however, it seems that there is no justified reason for prolonged intravenous treatment in cases of LS, and thus, if the patient responds well to treatment, he/she could be switched to oral treatment after the first 2 weeks of intravenous antibiotics.Citation9
Anticoagulation
Anticoagulation is still a controversial issue, with no proper studies carried out on the issue. In this review, we found that 87 cases (64%) received anticoagulation treatment, often with low-molecular-weight heparin. Treatment duration varied between 2 weeks and 6 months. A few (n=2) patients suffered from side effects (hemorrhage or disseminated intravascular coagulation) and were treated accordingly without serious adverse effects.Citation32,Citation87 In the review by Riordan and also previous reviews, the frequency of patients treated with anticoagulants was 21%–23%. The high prevalence in this study might be due to the widespread, unconfirmed hypothesis regarding the positive effects of anticoagulants, which seem to have gained a favorable position in the clinic. Also, within this review, we have not subdivided the patients receiving anticoagulation treatment regarding thrombosis solely in the jugular vein and thrombosis involving sinus cavernosus. The latter is a more severe situation and thus requires a more aggressive treatment strategy.
Other forms of treatment
A substantial number of cases (n=17) had abscesses in various anatomical locations: lungs, liver, epidura, and neck. Generally, accessible abscesses were treated by drainage. Rarely, other surgical procedures were performed: tooth extraction,Citation84 craniotomy,Citation69 and ligation of the occluded vein,Citation18,Citation65,Citation68 in order to prevent further septic emboli. Common for these cases were severe illness, and all other treatment modalities were already initiated, ligation seems to be reserved exclusively for extremely ill patients.
Conclusion
Given that we identified only 30 case reports from 2012, 27 from 2014, and ten from 2015, it does not seem that the incidence of LS is increasing. However, these are speculations, and evidently publication bias is unavoidable, and the “market” might be saturated with case reports on the subject. The syndrome still deserves the name “the forgotten disease”, and most fusobacterial infections are not LS. A fatal outcome is rare.
Diagnosing LS still requires thorough clinical examination and awareness of the association between current acute medical illness and a recent pharyngeal infection; yet, there is a need for studies on the diagnostic outcomes when LS is suspected.
Furthermore, early collection of blood samples and microbiology cultures in severely ill patients are required to establish a microbiological diagnosis. Symptoms of possible thrombosis need evaluation by an early CT scan or ultrasonography. The former has a better diagnostic capability, including intrathoracic vessels and septic emboli.
Treatment is efficacious and follows the general principles: systemic antibiotics, drainage of abscesses, and, perhaps, anticoagulation. Antibiotic treatment is crucial and should be corrected according to microbiological results on drug resistance. Penicillin, carbapenem, or piperacillin/tazobactam – often in combination with metronidazole – is efficacious. The optimal duration of treatment is not established, but 2 weeks of intravenous antibiotics with a total of 4–6 weeks seems sufficient. However, duration needs individualization according to disease severity and follow-up results, including imaging and serological inflammatory markers.
Based on the current evidence, it is still unknown whether anticoagulation therapy is mandatory. There were no apparent differences in mortality or course between the 64% cases treated with anticoagulants versus the 36% who were not. However, confounding by indication is most likely. Unfortunately, no randomized studies on this controversy are available.
Overall, LS is characterized by the absence of large-scale studies, but hopefully the future will witness a pragmatic multicenter approach to address the various controversies of this intriguing disease.
Disclosure
The authors report no conflicts of interest in this work.
References
- LemierreAOn certain septicemias due to anaerobic organismsLancet19361701703
- NohHJFreitasCASouza RdePLemierre syndrome: a rare complication of pharyngotonsillitisBraz J Otorhinolaryngol201581556857026324201
- ChuncharuneeAKhawcharoenpornTLemierre’s syndrome caused by Klebsiella pneumoniae in a diabetic patient: a case report and review of the literatureHawaii J Med Public Health201574826026626279962
- RiordanTWilsonMLemierre’s syndrome: more than a historical curiosaPostgrad Med J20048094432833415192164
- Tromop-van DalenCMekhailAMLemierre syndrome: early recognition and managementCMAJ2015187161229123126261192
- OyaMTanimotoTYamamotoTHakozakiYLemierre’s syndrome associated with periodontal injury-derived odontogenic infection that did not respond to meropenemIntern Med201554141803180826179541
- KarkosPDAsraniSKarkosCDLemierre’s syndrome: a systematic reviewLaryngoscope200911981552155919554637
- BotrosJRencicJCentorRMAnchors awayJ Gen Intern Med201429101414141824841558
- RiordanTHuman infection with Fusobacterium necrophorum (Necrobacillosis), with a focus on Lemierre’s syndromeClin Microbiol Rev200720462265917934077
- TurediSTurkmenSYadigarogluMAn unusual cause of sore throat and neck swellingEmerg Med J20153286254626195474
- WongAPDugginsMLNeilTInternal jugular vein septic thrombophlebitis (lemierre syndrome) as a complication of pharyngitisJ Am Board Fam Med201528342543025957375
- TakanoYFukudaKTakayasuHLiver abscessation and multiple septic pulmonary emboli associated with Lemierre’s syndrome: a case reportBMC Res Notes201586525889618
- CrowleyNDVercelesACReedRMSore throat. don’t forget Lemierre’s syndromeBMJ Case Rep20152015bcr2014208225
- AslanidisTMyrouAGiannakou-PeftoulidouMManagement of a young female patient with Fournier’s gangrene and Lemierre’s syndromePan Afr Med J20141827525489369
- AgrafiotisMMoularaEChlorosDLemierre syndrome and the role of modern antibiotics and therapeutic anticoagulation in its treatmentAm J Emerg Med2015335733.e3733.e425455045
- ShimadaMMorinagaYKitazakiTA severe case of Lemierre Syndrome with Streptococcus constellatus infectionJpn J Infect Dis201467648848925410567
- OlsonKRCase 36-2014: a woman with fever, pharyngitis, and double visionN Engl J Med2015372658158225651266
- SchubertADHotzMACaversaccioMDArnoldASeptic thrombosis of the internal jugular vein: lemierre’s syndrome revisitedLaryngoscope2015125486386825387698
- DavidossNHaJFAndersonJRRodriguesSLemierre’s syndrome – an unusual complication of otitis externa in a young, healthy femaleJ Laryngol Otol2015129suppl 1S60S6225292182
- LedochowskiSFreichetMWalletFLemierre’s syndrome: when a contralateral thrombosis stirs the debateIntensive Care Med201541232933025274006
- KempenDHvan DijkMHoepelmanAIOnerFCVerlaanJJExtensive thoracolumbosacral vertebral osteomyelitis after Lemierre syndromeEur Spine J201524suppl 4S502S50725245891
- TakenouchiSKuniedaTYamadaRLemierre syndrome caused by oral sexJ Formos Med Assoc20141131076276325240308
- AsnaniJJonesSCase review. Lemierre’s syndromeJ Fam Pract201463419319624905121
- Cardenas-GarciaJNarasimhanMKoenigSJA teenager with fever and sore throat. Diagnosis: lemierre syndromeChest20141454e10e1324687725
- MurthyKAThippeswamyTKiranHSThe ‘forgotten disease’ (or the never known)J Assoc Physicians India2013611075475724772738
- ShookJTriggerCLemierre’s SyndromeWest J Emerg Med201415212512624672595
- Behpour-OskooeeMKarimiASayyahfarSLemierre’s syndrome with double heterozygote status in the methylenetetrahydrofolate reductase geneWorld J Pediatr201410328128324668238
- GuptaNKralovicSMMcGrawDLemierre syndrome: not so forgotten! American journal of critical care: an official publicationAm J Crit Care201423217617924585168
- LinHYLiaoKHJeanSSLemierre syndrome with cervical spondylodiscitis and epidural abscess associated with direct injection of heroin into the jugular veinJ Microbiol Immunol Infect201548223823924388576
- AzzopardiCGrechRMizziALemierre syndrome: more than just a sore throatBMJ Case Rep20132013bcr2013201868
- RatnasinghamYKristensenLHGammelgaardLBalslevTArterial ischemic stroke as a complication to disseminated infection with Fusobacterium necrophorumNeuropediatrics201445212012224227208
- HorwitzMChaumoitreKGrimaldiCSpontaneous regression of multiple Rasmussen aneurysms in a child with Lemierre syndrome and pulmonary abscessesPediatr Infect Dis J201332111301130224141806
- HawesDLinneyMJWilkinsonRPaulSPLemierre’s syndrome: the importance of early detectionBr J Nurs201322181075107824121852
- MorelliNRotaESacchiniDLemierre syndrome: more than “the forgotten disease”Neurology201381131179118024062342
- GolanEWongKAlahmadiHEndoscopic sphenoid sinus drainage in Lemierre syndromeJ Clin Neurosci201421234634824060623
- BlessingKToepfnerNKinzerSLemierre syndrome associated with 12th cranial nerve palsy – a case report and reviewInt J Pediatr Otorhinolaryngol20137791585158823845534
- AbhishekASandeepSTarunPLemierre syndrome from a neck abscess due to methicillin-resistant Staphylococcus aureusBraz J Infect Dis201317450750923797007
- RighiniCAKarkasATourniaireRLemierre syndrome: study of 11 cases and literature reviewHead Neck20143671044105123784917
- TakedaKKenzakaTMoritaYKurokiSKajiiEA rare case of Lemierre’s syndrome caused by Porphyromonas asaccharolyticaInfection201341488989223435719
- KimBYYoonDYKimHCThrombophlebitis of the internal jugular vein (Lemierre syndrome): clinical and CT findingsActa Radiol201354662262723528567
- LitmatheJZardoPDickgreberNMayGSuckerCFischerSSevere ARDS induced by fusobacterial infections: a rare clinical presentation of Lemierre syndromeThorac Cardiovasc Surg201361875475723564539
- BoydDPatersonPDunphyLCartonAHammersleyNA case report of Lemierre’s Syndrome associated with dental sepsisScott Med J2013581e24e2723596035
- MaçãoPCancelinhaCLopesPRodriguesFAn 11-year-old boy with pharyngitis and cough: lemierre syndromeBMJ Case Rep20132013bcr2012008527
- WahabDBichardJShahAMannBJust a sore throat? Uncommon causes of significant respiratory diseaseBMJ Case Rep20132013bcr2013008739
- DeGaffeGHMurphyJRButlerIJShelburneJHeresiGPSevere narrowing of left cavernous carotid artery associated with Fusobacterium necrophorum infectionAnaerobe20132211812023664903
- GhalyBBertramANaimALemierre’s syndrome: a serious complication of a routine dental procedureAust Dent J201358224624923713647
- GutzeitARoosJEPortocarrero-FahBDifferential diagnosis of Lemierre’s syndrome in a patient with acute paresis of the abducens and oculomotor nervesKorean J Ophthalmol201327321922323730118
- McGouranDKeeneAWalklinRA complex case of bilateral Lemierre syndrome with suggestions on anticoagulation managementIntern Med J201343672873023745997
- JohannesenKBodtgerUHeltbergOLemierre’s syndrome: the forgotten diseaseJ Thromb Thrombolysis201437324624823686643
- PaulSPBeriRLinneyMJLemierre’s syndrome: a sinister sore throat every clinician should rememberTurk J Pediatr201254552853123427519
- SohTLimMHLemierre’s syndrome: an unusual cause of calf abscessAnn Acad Med Singapore2013421525423417592
- ValeskyWAgoritsasKLemierre syndrome complicated by cerebral abscessAm J Emerg Med2013312458.e1458.e323407038
- DholakiaSHashimiYDoctor, I have a sore throatBMJ Case Rep20132013bcr2012007736
- KumarMSinghRSawlaniKKKumarSAtypical presentation of Lemierre syndrome: role of imagingBMJ Case Rep20132013bcr2012007647
- JiYQWangJKongLQLemierre syndrome caused by Arcanobacterium haemolyticumChin Med J2013126239139223324298
- MurataYWadaMKawashimaAKagawaKEarly diagnosis of Lemierre’s syndrome based on a medical history and physical findingsIntern Med201352228528823318865
- RodgaardJCNiedvaraiteRAndersenGNLemierre’s syndrome in systemic lupus erythematosus: a report of two casesScand J Rheumatol201342216716823311933
- KhanAGanesanSAroraMHussainNLife threatening complication of sore throat: lemierre’s syndromeIndian J Pediatr201380121059106123275185
- DaviesOThanMLemierre’s syndrome: diagnosis in the emergency departmentEmerg Med Australas201224667367623216731
- AkiyamaKKarakiMSamukawaYMoriNBlindness caused by septic superior ophthalmic vein thrombosis in a Lemierre Syndrome variantAuris Nasus Larynx201340549349623084837
- LimALPuaKCLemierre syndromeMed J Malaysia201267334034123082433
- IizukaTNagayaKSasakiDAtypical Lemierre syndrome, thrombophlebitis of the facial veinAm J Emerg Med2013312460.e1460.e323041486
- StaufferCJosiahAFFortesMMenakerJColeJWLemierre syndrome secondary to community-acquired methicillin-resistant Staphylococcus aureus infection associated with cavernous sinus thrombosesJ Emerg Med2013442e177e18222989693
- PhanTSoTYUse of anticoagulation therapy for jugular vein thrombus in pediatric patients with Lemierre’s syndromeInt J Clin Pharm201234681882122899236
- MurrayMStevensTHerfordALemierre syndrome: two cases requiring surgical interventionJ Oral Maxillofac Surg201371231031522835986
- TsaiYJLinYCHarnndDJChiangRPWuHMA Lemierre syndrome variant caused by Klebsiella pneumoniaeJ Formos Med Assoc2012111740340522817819
- RootRWBarrettTWAbramoTJA 10-month-old with Lemierre syndrome complicated by purulent pericarditisAm J Emerg Med2013311274.e5274.e722809766
- HileLMGibbonsMDHileDCLemierre syndrome complicating otitis externa: case report and literature reviewJ Emerg Med2012424e77e8019327936
- TengHWChenCYChenHCChungWTLeeWSFusobacterium septicemia complicated by cerebral subdural and epidural empyemas: a rare case of Lemierre syndromeJ Emerg Med201243467167320566261
- ChowBJTupesisJPDisseminated Lemierre syndrome presenting as septic arthritisJ Emerg Med201242557357521035986
- KisserUGurkovRFlatzWBerghausAReichelOLemierre syndrome: a case reportAm J Otolaryngol201233115916221345516
- WingfieldTBlanchardTJAjdukiewiczKMSevere pneumonia and jaundice in a young man: an atypical presentation of an uncommon diseaseJ Med Microbiol201160pt 91391139421546562
- SinghiSMathewJJindalAVermaSClinical Pearls in pediatric infectionsIndian J Pediatr201178121536154221625832
- IkemotoTKawasakiMKatoTDangerous cervical radiculopathy by Lemierre’s syndromeJ Orthop Sci201217566366621643795
- DorfmanAShokoohiHTaheriMRLemierre’s syndrome and rapidly deteriorating respiratory failure in the emergency departmentAm J Emerg Med20123081658.e51658.e722033390
- PriceKWilsonLTsegayeMA case of craniocervical abscess with sinus thrombosis in Lemierre’s syndromeBr J Neurosurg201226342642822077587
- BababeygySRAlmarzoukiHBuffennANIsolated abducens nerve palsy secondary to Lemierre syndromeJ AAPOS201115658758922153405
- LeeWSWangFDShiehYHLemierre syndrome complicating multiple brain abscesses caused by extended-spectrum beta-lactamase-producing Klebsiella pneumoniae cured by fosfomycin and meropenem combination therapyJ Microbiol Immunol Infect2012451727422154996
- NisarMKKuttikatAVRamabhadranBLemierre’s syndrome: a rare cause of septic polyarthritisRheumatol Int201333381781822190274
- RehmanHUA woman with headache and ptosisQJM2014107975976122267575
- KieranILyttleMLeroiMSuccessful antibiotic stewardship: are we a victim of our own success? ANZ J Surg201181648848922295363
- WasilewskaEMorrisADLeeEYCase of the season: lemierre syndromeSemin Roentgenol201247210310522370188
- KleinNCPetelinACunhaBAMycoplasma pneumoniae preceding Lemierre’s syndrome due to Fusobacterium nucleatum complicated by acute Epstein-Barr virus (EBV) infectious mononucleosis in an immunocompetent hostHeart Lung2013421747622464641
- WuAYTsengHKSuJLiuCPLemierre’s syndrome in a patient with habitual toothpick usageJ Microbiol Immunol Infect201346323724022487510
- ChattopadhyayDMostafaMLCarrMAcute neck pain referred to the surgeon: lemierre’s syndrome as a differential diagnosisAnn R Coll Surg Engl2012943e132e13322507711
- KrollDSendiPLemierre’s syndrome in the liverInfection201240447747822527877
- IwasakiTYamamotoTInoueKTakakuKA case of Lemierre’s syndrome in association with liver abscess without any other metastatic lesionsIntern Med201251111419142322687854
- MolloyATowerseyGShackletonDThe changing face of an old disease: case report of nonclassical Lemierre’s syndrome caused by a Panton-Valentine leucocidin-positive methicillin-susceptible Staphylococcus aureus isolateJ Clin Microbiol20125093144314522760040
- PitsiouGKachrimanidouMPapaALemierre’s syndrome presenting to the ED: rapidly fatal sepsis caused by methicillin-susceptible Staphylococcus aureus Staphylococcus protein A type t044Am J Emerg Med2013311268.e5268.e722795989
- KrishnaKDiwanAGGuptALemierre’s syndrome – the syndrome quite forgottenJ Assoc Physicians India2012606063
- Hagelskjaer KristensenLPragJLemierre’s syndrome and other disseminated Fusobacterium necrophorum infections in Denmark: a prospective epidemiological and clinical surveyEur J Clin Microbiol Infect Dis200827977978918330604
- JohannesenKDessauRHeltbergOBodtgerUBad news itself or just the messenger? The high mortality of Fusobacterium spp. infections is related to disseminated malignancy and other comorbiditiesEur Clin Respir J201633028727171316
- UngprasertPSrivaliNDiagnosis and treatment of Lemierre syndromeAm J Emerg Med2015339131926099786
- MoherDLiberatiATetzlaffJAltmanDGPRISMA GroupPreferred reporting items for systematic reviews and meta-analyses: the PRISMA statementPLoS Med200967e1000097 Available from: www.prisma-statement.orgAccessed May 9, 201619621072