
Abstract
Hepatitis C viral infection is endemic in Egypt with the highest prevalence rate in the world. It is widely accepted that the implementation of mass population antischistosomal treatment involving administration of tartar emetic injections (from 1950s to 1980s) led to widespread infection. What is less well known, however, is that these schemes were implemented by the Egyptian Ministry of Health on the advice of the World Health Organization. There has been a spectrum of treatments to target the public health disaster represented by the hepatitis C problem in Egypt: from the use of PEGylated interferon to the recent use of direct acting antiviral drugs. Some new treatments have shown >90% efficacy. However, cost is a key barrier to access these new medicines. This is coupled with a growing population, limited resources, and a lack of infection control practices which means Egypt still faces significant disease control issues today.
Keywords:
Introduction
This article aims to put the hepatitis C viral (HCV) epidemic in Egypt into a historical and cultural context, given that it arose in part from public health measures encouraged by Egyptian health authorities and World Health Organization (WHO) officials in a period spanning over three decades in the latter half of the last century. The long natural history of the condition has meant that the country is still grappling with the effects of these policies to the present day. However, new treatments for HCV with direct-acting antiviral agents allow, for the first time, the prospect of future eradication of the condition. This article aims to highlight these prospects against the economic costs of such treatment and the steps that have been taken to obtain the widest possible treatment coverage.
HCV, and its long-term resultant consequences, is a major endemic medical health problem in Egypt. Having taken a representative sample of the country, from both urban and rural areas, an Egyptian demographic health survey conducted in 2008 concluded that 14.7% of the population have been infected, making this the highest prevalence in any population in the world.Citation1–Citation3 In the Nile Delta and Upper Egypt, infection rates can be much higher at around 26% and 28%, respectively.Citation4 With incidence rates between 2 and 6 per 1000 every year, this leads to an estimated 170,000 new cases every year to add to the 11.5 million patients suffering from the disease.Citation4
More recent epidemiological modeling studies conducted to assess the HCV disease burden have suggested a more conservative estimate of 7.3% of the population with viremic HCV in 2013.Citation5,Citation6 This is mainly due to the mortality in the older age groups who have the highest prevalence of infection.
HCV infection occurs through blood contact.Citation2 Apart from the usual modes of transmission, such as intravenous drug usage, the main risk factors for transmission in Egypt historically have included the now archaic parenteral antischistosomal therapy, shared or reused needles, poorly sterilized surgical or dental equipment, and blood transfusions.Citation7 In the past, it was primarily the use of widespread tartar emetic injections, which were used to treat schistosomiasis in Egypt in the 1950s to the early 1980s, which laid the foundation for the HCV epidemic currently seen. Since it can take up to 20–30 years for HCV infection to become clinically evident, there has been a lag phase of several decades before the problem became apparent. While currently, Egypt is still seeing a few new cases of hepatitis C-related liver disease presenting from the initial antischistosomal campaign, with some patients displaying a lag phase of 40 years before clinical presentation, in practice, poor infection control and equipment sterilization procedures used in medical and dental settings also led and continue to lead to iatrogenic HCV infections to the present day, which further stimulate the spread of the disease and continue to fuel the current epidemic.Citation2
Although around 30% of patients may clear the virus spontaneously,Citation8 the main health burden occurs from the majority of patients who develop chronic HCV. In this patient population, cirrhosis may develop within 20 years of infection.Citation8 With hepatic decompensation and hepatocellular carcinoma, these long-term consequences have put further strain on resources in an already overstretched Egyptian healthcare system.Citation4,Citation9
What is HCV?
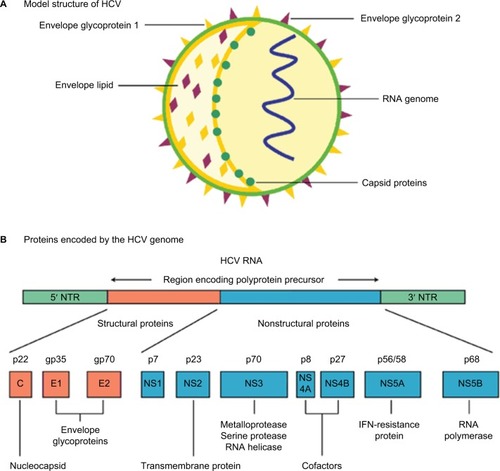
HCV is a hepatotropic RNA virus of the genus Hepacivirus in the Flaviviridae family.Citation10–Citation12 The virus exists as an enveloped, positive-stranded RNA virus which is ~50 nm in size (). The HCV RNA strand is made up of ~9600 nucleotide bases and is covered by an icosahedral nucleocapsid which is further surrounded by a lipid bilayer and glycoproteins. HCV is grouped into 6 major genotypes that exhibit at least 30% variation in nucleotide sequence from one another.Citation10–Citation12 This genetic variation within the population is a powerful selection mechanism for resistance to both medicinal drugs and evasion of the immune system.Citation10,Citation12 The most common HCV RNA genotype in Egypt is genotype 4, representing >85% of all HCV cases in Egypt.
Figure 1 HCV: model structure and genome organization.
Abbreviations: HCV, hepatitis C viral; IFN, interferon; NTR, nontranslated RNA.
History of the infection
With HCV seroprevalence at up to 40% in some areas of Egypt,Citation13–Citation16 based on blood-bank surveys, it is obvious that HCV is a huge public health issue within the country.Citation17–Citation19 A particular focus is placed on the Nile delta region which holds the greatest rates of infection and was, historically, the main focus for schistosomiasis.Citation2 The primary two schistosome species in Egypt are Schistosoma mansoni and Schistosoma haematobium.Citation20,Citation21 Until the HCV epidemic became apparent, schistosomiasis was the most important public health problem in Egypt with S. mansoni being the primary cause of liver disease within Egypt historically.Citation22
In 1918, JB Christopherson made the discovery that injections with the antimony salt, tartar emetic, could induce a cure.Citation2,Citation20 Egypt, at the time, had the greatest schistosomiasis burden in the world, and mass treatment of the parasite was introduced via primary health care services.Citation20
From the 1950s to the 1980s, community-wide mass antischistosomal therapy was introduced by the Egyptian Ministry of Health with the advice and support of the WHO.Citation22–Citation24 At the time, tartar emetic injections were the standard treatment. They were injected intravenously, unlike some other now-archaic antischistosomal drugs that were injected intramuscularly. Over 2 million injections were given annually to an average of 250,000 patients, meaning over the 18 years of treatment, 36 million injections were administered.Citation2,Citation20 Each patient was supposed to have a series of injections with the average number of injections per patient being nine in the 1960s, which then dropped to six after 1975.Citation20,Citation21
There are three main causes for the transmission of HCV, as well as other blood-borne diseases in this mass treatment scheme.Citation20 First, patients were exposed to multiple injections over the time period which increased the likelihood of pathogen transmission. Second, sterilization techniques were extremely poor, which led to high frequency of HCV transmission, a virus that was not known to medical science until the 1990s. Finally, the mass scale of the antischistosomal eradication campaign led to widespread mistakes, including reuse of equipment, which was something not considered important until the advent of the HIV epidemic in the early- to mid-1980s.Citation2
To add to the danger of the campaign, “acute clinical symptoms are not present in about 80% of HCV infections.”Citation20 This means infection spread rapidly and would go largely unnoticed. These campaigns are hypothesized to have led to the “high HCV seroprevalency rates currently observed in the Nile delta”.Citation2,Citation13,Citation16,Citation23,Citation24, This hypothesis is further supported by the clustering effect observed between HCV infections in households with patients who received parenteral treatment for schistosomiasis.Citation23
Toward the end of the campaign in the 1970s, oral drugs to treat schistosomiasis were developed, including the oral agent, praziquantel, which slowly replaced the tartar emetic injections as the gold standard of treatment.Citation20,Citation22
How HCV affects the liver
Hepatitis C viral infection is largely asymptomatic with little visible symptoms in its acute infection stage. It is only when a patient has been harboring the disease for anywhere between 20–40 years and therefore has a chronic HCV infection when noticeable symptoms or signs will occur. HCV is a significant “precursor” for fibrosis, cirrhosis, and ultimately, hepatocellular carcinoma, but it is important to understand this is only in long-term, chronic cases.Citation20,Citation25 In Egypt, up to 85% of HCV infections persist for life, leading to chronic hepatitis.Citation20,Citation27 The major cause of death is primarily associated with cirrhosis in the liver as well as other conditions including liver failure, hematemesis from esophageal varices, hepatic encephalopathy and hepatocellular carcinoma.Citation20,Citation28 HCV may complicate the course of schistosomiasis and vice versa with a perhaps synergistic effect. A long-term study showed that complications occurred at a much faster rate in those with coinfection with around 48% having cirrhosis, compared with 15% in those who had HCV alone and 0% in the group with schistosomiasis alone.Citation20
Previous and current treatments
Interferon treatment was incredibly costly especially for a largely poor patient population in Egypt, which meant that access to treatment was sporadic.Citation20,Citation28 Focus for HCV treatment has therefore switched to promoting the research and development of direct acting antiviral (DAA) drugs which present an oral, interferon-free treatment option.Citation28,Citation29 The drugs are specific to the HCV particle and aim to inhibit viral RNA replication by attacking some of the several enzymes involved in the RNA replication process, thereby inhibiting viral replication and causing viral eradication.Citation29 This represents a novel and less invasive treatment scheme which has proven revolutionary in tackling the HCV epidemic in Egypt.
Efficacy of treatment with sofosbuvir and ribavirin
In a study of the DAA combination, sofosbuvir and ribavirin, pan-genotypic clinical efficacy in HCV genotypes 1–6 was demonstrated.Citation30,Citation31 Another stage 3 clinical trial involving giving patients sofosbuvir in conjunction with ribavirin and PEGylated alpha interferon for a 12-week treatment period showed a sustained virological response in 27 out of 28 treatment-naïve patients with HCV genotype 4 (96% efficacy).Citation30 The efficacy of treatment has been profound to the extent that the European Association for the Study of the Liver and the WHO have recommended either a course of sofosbuvir, ribavirin and PEGylated alpha-interferon for a 12-week treatment period or 24 weeks of ribavirin in conjunction with sofosbuvir as an interferon-free treatment regime.Citation32–Citation34 Other direct acting antiviral treatments include simeprevir, daclatasvir, a ledipasvir–sofosbuvir combination tablet, and a paritaprevir–ombitasvir combination tablet.
Accessibility of treatment
This study highlighted that while HCV is a prevalent and difficult medical problem in Egypt, there are existing drug regimens which have a proven efficacy in tackling the disease. One of the biggest problems facing the Egyptian population, however, comes in access to these drug treatments – especially when considering that the HCV epidemic in Egypt is one of a largely socioeconomic nature.Citation1,Citation35 The condition is most prevalent within rural communities compared with urban communities (12% and 7% prevalence rates, respectively).Citation1 As well as this, HCV varies with wealth too, having a 12% prevalence in the lowest quartile compared with 7% in the upper quartile of the population.Citation1 It is therefore the case that the poorest and least educated in society suffer the problematic effects of this epidemic which poses challenges both in access and affordability of treatment but also in diagnosing the true extent of the problem due to high illiteracy rates and low HCV awareness levels.Citation36
Between 2008 and 2012, the Egyptian National Committee for the Control of Viral Hepatitis (established in 2006) aimed to develop a strategy to control viral hepatitis. This involved investing US$80 million each year with the aim of treating 20% of the HCV patients in Egypt by the end of 2012.Citation36,Citation37 The scheme would subsidize the preferred treatment at the time – which was PEGylated alpha interferon with ribavirin. By the end of 2011, around 2.8% of patients had benefited from HCV treatment with only 114,000 achieving a sustained virological response (1.67%). The reasons for this low cure rate are multifactorial, but principally include poor patient supervision and poor patient compliance with, or adherence to a 6–12 month interferon-based regimen that had significant side effects including lethargy, depression, and “flu-like” symptoms. When this scheme was a national policy, only patients with relatively higher chances of cure had access to treatment.Citation36,Citation37 At the time the Egyptian Ministry of Health, also, put too much emphasis on treatment, compared with infection control and education which with hindsight proved to be a key failure of the plan.Citation19
The Egyptian Ministry of Health has since proposed a new national strategy to control the HCV epidemic in Egypt with a greater capital fund and with support from the WHO as well as other institutes.Citation19 This scheme was entitled “The Plan of Action for the Prevention, Care and Treatment of Viral Hepatitis 2014–2018” and promoted sofosbuvir (Sovaldi™, Gilead Sciences, San Francisco, USA) as its primary treatment.Citation36 The scheme aims to treat 300,000 patients annually and the cost of treatment would be distributed between the Egyptian Ministry of Health (38%), the Egyptian Health Insurance Organization (51%), private payments (3%), and finally cash payments from patients (8%).Citation14,Citation36
Sovaldi retails for US$84,000 for a 12-week course making it a staggering US$1000 per pill.Citation36 This makes it out of reach for the Egyptian HCV patient population. Negotiations between the Egyptian government in the form of the “National Committee for the Control of Viral Hepatitis” and Gilead Sciences resulted in a reduced cost of US$300 per box of Sovaldi which would supply 1 month of treatment.Citation36 Headlines portrayed this as a 99% discount on the original price of the treatment. However, the reality is that only patients treated under the governmental treatment scheme are currently able to access this discounted price.Citation38 Gilead registered the same product on the private pharmaceutical market for EGP 14,900 per box.Citation36 This makes the private cost of treatment around six times the government price. Hence, due to the limited availability and reach of the governmental scheme, patients are still faced with unaffordable drug treatment. However, there is hope that the subsidized scheme will be extended in the future as part of Egyptian Government policy and/or Gilead corporate social responsibility. Such negotiations are ongoing at the time of writing. This would then offer the real possibility of HCV eradication in Egypt for the first time.
Conclusion/Discussion
Alternative treatments and future steps
It is clear that there is evidence of some good foundations for tackling the widespread prevalence of HCV in Egypt. At the time of writing, the development of effective DAAs has shown up to 90% efficacy against HCV genotype 4, and such treatment has been able to produce excellent SVR results in the Egyptian context. There is less ignorance and lack of awareness of the need to properly sterilize equipment and medical instruments than there has been in the past, although public awareness campaigns still need to be conducted, including to allied health care professionals. From a historical perspective, the Egyptian population has become much more aware of the threats associated with swimming and utilizing canal water which has led to a decrease in incidence rates of schistosomiasis in parallel. Effort must now be concentrated on treating the existing HCV patients, who are suffering from the failed treatments initiatives of the past.
The Egyptian Ministry of Health must take a two-pronged approach to tackling this disease. Currently, there are established DAAs that have the portent to eliminate HCV. In addition, local pharmaceutical companies should be aided in developing drug generic versions in order to make direct acting antiviral drugs more accessible for those who have not been able to gain access to treatment through governmentally subsidized schemes.
It is important to realize, however, that widespread DAA treatment will not solve all the associated problems of the HCV epidemic in Egypt. The complications of decompensated cirrhosis and hepatocellular carcinoma present a massive burden to Egyptian society and they still need to be addressed with adequate health care resource allocation.
Egypt has all the potential tools to tackle its HCV crisis. What is needed is ring-fenced governmental funding to enforce treatment policy, as well as clear medical and public health guidance in order to target treatment effectively. At the same time, the Egyptian Ministry of Health must continue to invest in research and development for the best emerging treatments to be implemented. However, it is important not to forget the essentials of education, infection control, equipment sterilization, and risk aversion to stop further growth of those who continue to become newly infected.
Acknowledgments
All authors acknowledge the support of the Wellcome Global Centre at Imperial College London for financial and logistic support and the National Institute for Health Research Biomedical Research Centre at Imperial College London for infrastructure support.
Disclosure
MMEC is supported by a Fellowship from the Sir Halley Stewart Trust (Cambridge, UK). MMEC and SDT-R hold grants from the United Kingdom Medical Research Council. AIG was supported by a doctorate grant from the Egyptian Ministry of Higher Education. The authors report no other conflicts of interest in this work.
References
- El-ZanatyFWayAEgypt Demographic and Health Survey 2008Cairo, EgyptMinistry of Health, El-Zanaty and Associates, and Macro International2009431
- FrankCMohamedMStricklandGTThe role of parenteral antischistosomal therapy in the spread of hepatitis C virus in EgyptLancet2000355920788789110752705
- ShepardCWFinelliLAlterMJGlobal epidemiology of hepatitis C virus infectionLancet Infect Dis20055955856716122679
- WanisHHCV treatment in Egypt – why cost remains a challenge?Cairo, EgyptEgyptian initiative for personal rights [serial on the Internet]201414 Available from: http://www.eipr.org/sites/default/files/pressreleases/pdf/hcv_treatment_in_egypt.pdfAccessed June 16, 2016
- WakedIDossWEl-SayedMThe current and future disease burden of chronic hepatitis C virus infection in EgyptArab J Gastroenterol2014152455225097045
- RazaviHWakedISarrazinCThe present and future disease burden of hepatitis C virus with today’s treatment paradigmJ Viral Hepat201421Suppl 1345924713005
- MohamoudYMumtazGRiomeSMillerDRaddadLThe epidemiology of Hepatitis C virus in Egypt: a systematic review and data synthesisBMC Infect Dis [serial on the Internet]201313288 Available from: https://bmcinfectdis.biomedcentral.com/articles/10.1186/1471-2334-13-288Accessed May 16, 2016
- LozanoRNaghaviMForemanKGlobal and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010Lancet201238098592095212823245604
- NHS Choices [page on the Internet]Complications of Hepatitis C2013 Available from: http://www.nhs.uk/Conditions/Hepatitis-C/Pages/Complications.aspxAccessed July 10, 2015
- KimCWChangKMHepatitis C Virus: virology and life cycleClin Mol Hepatol2013191172523593605
- ZhaoLHepatits C virus: molecular pathways and treatmentsFoster, USAOMICS Group eBooks2014313 Available from: http://www.esciencecentral.org/ebooks/hepatitis/pdf/hepatitis-c-virus-molecular-pathways-and-treatments.pdfAccessed May 16, 2016
- AsterJCAbbasAKRobbinsSLKumarVRobbins Basic Pathology9th edPhiladelphia, PAElsevier Saunders2013
- DarwishMARaoufTARushdyPConstantineNTRaoMREdelmanRRisk factors associated with a high seroprevalence of hepatitis C virus infection in Egyptian blood donorsAm J Trop Med Hyg19934944404477692754
- ArthurRRHassanNFAbdallahMYHepatitis C antibody prevalence in blood donors in different governorates in EgyptTrans R Soc Trop Med Hyg19979132712749231192
- Abdel-AzizFHabibMMohamedMHepatitis C virus (HCV) infection in a community in the Nile Delta: population description and HCV prevalenceHepatology200032111111510869297
- DarwishMFarisRClemensJRaoMEdelmanRHigh seroprevalence of hepatitis A, B, C, and E viruses in residents in an Egyptian village in the Nile Delta: a pilot studyAm J Trop Med Hyg19965465545588686770
- HibbsRCorwinAHassanNThe epidemiology of antibody to hepatitis C in EgyptJ Infect Dis199316837897908394867
- El-SayedNGomatosPRodierGSeroprevalence survey of Egyptian tourism workers for hepatitis B virus, hepatitis C virus, human immunodeficiency virus, and Treponema pallidum infections: association of hepatitis C virus infections with specific regions of EgyptAm J Trop Med Hyg19965521791848780457
- Abdel-WahabMFZakariaSKamelMHigh seroprevalence of hepatitis C infection among risk groups in EgyptAm J Trop Med Hyg19945155635677527186
- StruthersAFrom schistosomiasis to hepatitis C: the spread of HCV in EgyptMed J Ther Africa200713213221 Available from: http://mjota.org/images/SpreadofHCVEgypt.pdfAccessed February 16, 2016
- Centers for Disease Control and Prevention, National Center for Infectious Diseases, Division of Parasitic Diseases. [homepage on the Internet]Schistosomiasis public information fact sheet [updated November 7, 2012] Available from: http://www.cdc.gov/parasites/schistosomiasis/Accessed June 01, 2016
- StricklandGLiver disease in Egypt: hepatitis C superseded schistosomiasis as a result of iatrogenic and biological factorsHepatology200643591592216628669
- RaoMRNaficyABDarwishMAFurther evidence for association of hepatitis C infection with parenteral schistosomiasis treatment in EgyptBMC Infect Dis200222912464161
- FrankCMohamedMKStricklandGTThe role of parenteral antischistosomal therapy in the spread of hepatitis C virus in EgyptLancet2000355920788789110752705
- BallesterJMRiveroRAVillaescusaRHepatitis C virus antibodies and other markers of blood-transfusion-transmitted infection in multi-transfused Cuban patientsJ Clin Virol200534Suppl 2S39S4616461239
- DarwishMFarisRDarwishNHepatitis C and cirrhotic liver disease in the Nile delta of Egypt: a community-based studyAm J Trop Med Hyg2001643–414715311442209
- HoofnagleJHepatitis C: the clinical spectrum of diseaseHepatology1997263 Suppl 115S20S9305658
- RuanePAinDStrykerRSofosbuvir plus ribavirin for the treatment of chronic genotype 4 Hepatitis C virus infection in patients of Egyptian ancestryJ Hepatol20156251040104625450208
- MuirAJThe rapid evolution of treatment strategies for hepatitis CAm J Gastroenterol2014109562863524732866
- LawitzEMangiaAWylesDSofosbuvir for previously untreated chronic hepatitis C infectionN Engl J Med2013368201878188723607594
- JacobsonIGordonSKowdleyKSofosbuvir for hepatitis C genotype 2 or 3 in patients without treatment optionsN Engl J Med2013368201867187723607593
- American Association for the Study of Liver Diseases and the Infectious Diseases Society of AmericaRecommendations for testing, managing, and treating hepatitis C2014 Available from: http://www.hcvguidelines.org/Accessed June 16, 2016
- European Association for the Study of the LiverEASL clinical practice guidelines: management of hepatitis C virus infectionJ Hepatology201463pt 392420
- WHO [fact page on the Internet]Guidelines for screening, care and treatment of persons with hepatitis C infectionPublications on Viral Hepatits2014 Available from: http://www.who.int/hiv/pub/hepatitis/hepatitis-c-guidelines/en/Accessed June 12, 2016
- DossWShihaGHassanyMSofosbuvir plus ribavirin for treating Egyptian patients with hepatitis C genome 4J Hepatol2015633584585
- WanisHHusseinAEl ShibinyAHCV treatment in Egypt – why cost remains a challenge Egyptian initiative for personal rights2014618 Available from: http://www.eipr.org/sites/default/files/pressreleases/pdf/hcv_treatment_in_egypt.pdfAccessed June 16, 2016
- DossWMohammedMEsmatGEgyptian National Control Strategy for Viral Hepatitis 2008–20122008 Available from: http://www.hepnile.org/images/stories/doc/NSP_10_April_2008_final2.pdfAccessed June 16, 2016
- FickMHirschlerBGilead offers Egypt new hepatitis C drug at 99 percent discountReuters [serial on the internet]2014 Available from: http://www.reuters.com/article/2014/03/21/us-hepatitis-egypt-gilead-sciences-idUSBREA2K1VF20140321Accessed June 16, 2016
- HuiAYFriedmanSLMolecular basis of hepatic fibrosisExpert Rev Mol Med200355123