
Abstract
Acromegaly is an uncommon, chronic disease, characterized by hypersecretion of a pituitary growth hormone by somatotroph adenomas, along with increased levels of insulin-like growth factor-1. Although acromegaly presents a wide array of clinical manifestations, the salient symptoms include acral and soft tissue enlargement, joint pain, heart and respiratory failure, diabetes mellitus, and hypertension, leading to increased morbidity and mortality. Hence, early diagnosis of the disease is critical to enhance life expectancy and quality of life. New approaches are being developed for diagnosis and surveillance (both screening and follow-up), including sensitive biochemical assays and the use of MRI to visualize extremely small tumors, and are helpful in the early diagnosis of acromegaly, subsequent treatment, and disease control. This mini-review summarizes the most common and effective tools used in the diagnosis of acromegaly.
Introduction
Acromegaly is a rare, chronic, endocrine disorder, usually caused by hypersecretion of growth hormone (GH) for a prolonged period from a somatotroph adenoma.Citation1 The term “acromegaly” is derived from two Greek words: “akrom”, meaning extremity, and “megas”, meaning great; the meaning reflects one of the familiar symptoms of the disease, which is abnormal growth of hands and feet.Citation2
Epidemiology of acromegaly
The exact prevalence of acromegaly is not quite clear; however, the estimated incidence is three to four cases per million per year, with an occurrence rate of ~40–125 people per million of the population.Citation3,Citation4 Even though the mean age of occurrence of the disease is 32 years, the mean age of diagnosis is 40–45 years, primarily owing to a delay in diagnosis.Citation2,Citation3 The incidence of acromegaly does not vary with gender, race, and ethnicity, although epidemiological studies conducted in Spain reported a predominance of acromegaly among women.Citation5 A study in a highly polluted area in the Messina province of Italy revealed an increased prevalence of acromegaly, indicating the pathogenic role of environmental factors in the development of acromegaly.Citation6
Causes of acromegaly
The pea-sized pituitary gland, located at the sella turcica, is responsible for secreting a multitude of hormones, including GH or somatotropin, the action of which is controlled by a complex feedback mechanism.Citation7 The most common cause of acromegaly is the presence of a benign tumor or adenoma originating from pituitary somatotroph cells and secreting excess GH.Citation1,Citation7 This excessive secretion of GH leads to a persistent elevation of insulin-like growth factor-1 (IGF-1),Citation8 which is produced by the liver, kidney, pituitary gland, muscle, and gastrointestinal tract; with liver being the primary source.Citation9 IGF-1 facilitates the growth-promoting effects of GH.Citation9 In 95% of acromegalic cases, enhanced levels of GH and serum IGF-1 are responsible for the distinctive features of the disease and numerous comorbidities. Alternatively, increased levels of growth hormone-releasing hormone (GHRH) produced in the hypothalamus account for 0.5% of acromegaly cases.Citation10 Hence, serum IGF-1 concentration is considered as a sensitive measure of integrated GH levels in patients with acromegaly.Citation9 Furthermore, some correlation between acromegaly and familial syndromes, such as McCune–Albright syndrome, multiple neoplasia type I, Carney complex, and isolated familial acromegaly, has been detected.Citation5
Clinical manifestations and associated comorbidities of acromegaly
Acromegaly is an insidious disease, which typically takes about 10–12 years from the onset of symptoms to diagnosis.Citation2 The exact reasons for the insidious nature of acromegaly remain unclear. It is likely that the gradual, progressive course of the disease leads to alterations ignored by the patient, family members, and even physicians. In addition, some of the comorbidities resemblance common disorders. As a result, before obtaining the correct diagnosis, patients usually have to visit primary care physicians and even other specialists several times.Citation11 The clinical manifestations of acromegaly depend on several factors, including levels of GH and IGF-1, the sensitivity of different tissues and organs to increased levels of GH and IGF-1, age, and tumor size, as well as delays in diagnosis.Citation12 In general, the clinical features of acromegaly include somatic effects due to excessive GH and IGF-1 levels and local effects caused by expansion of the pituitary tumor.Citation2
Somatic effects
Somatic effects include increases in the thickness of the skin and connective tissue; uneven proliferation of cartilage, bone, and other epithelial tissues; and visceromegaly in the form of goiter, hepatomegaly, splenomegaly, and macroglossia.Citation12 Acral enlargement, such as enlargement of hands, feet, and fingers, and typically coarse facial features, are the universal clinical manifestations of acromegaly. Facial changes include enlarged lips, tongue, and nose; deep nasolabial furrows; frontal skull bossing; mandibular prognathism; and separation of maxillary teeth.Citation2 Changes in the skin and soft tissues involve thickening of the skin owing to glycosaminoglycan deposition, leading to hyperhidrosis or oily skin texture, acanthosis nigricans (dark skin patches), and skin tags.Citation2,Citation12
Local effects of tumor
In a 2015 demographic study conducted on 271 patients, 6.6% and 83% were found to have microadenoma and macroadenoma, respectively.Citation24 According to another study, the prevalence of macroadenoma was found to be higher than that of microadenoma.Citation25 The adenoma may compress local organs and even cause neurological symptoms along with visual disturbances, which include headaches, defects in the visual field, cranial nerve palsies, hypopituitarism, and hypothyroidism.Citation2 The optic chiasm is an X-shaped structure formed by crossing of the optic nerves (CN II) in the brain. Upward growth of a pituitary adenoma leads to optic chiasm compression, thereby producing visual field disturbance, which starts in the mid-periphery of the superior temporal sectors and finally leads to bitemporal hemianopsia. The cavernous sinus is an important structure in the brain which is formed by a large channel of venous blood forming a cavity surrounded by sphenoid and temporal bones. This cavity is significant because of its location and content. It contains the third (oculomotor) and fourth (trochlear) cranial nerves. It also contain parts one (the ophthalmic nerve) and two (the maxillary nerve) of the fifth cranial (trigeminal) nerve, and the sixth cranial (abducens) nerve. Cavernous sinus invasion by a pituitary adenoma is of clinical significance it makes surgery more difficult and less efficient.Citation31
Associated comorbidities
Manifestations of acromegaly include soft and acral tissue overgrowth, joint pain, hypertension, and heart and respiratory failure.Citation12 Many studies have provided diagnostic algorithms from the associated comorbidities to identify acromegaly.Citation8 A scoring system called “ACROSCORE” has been used to investigate and confirm acromegaly in the very early stages ().Citation28
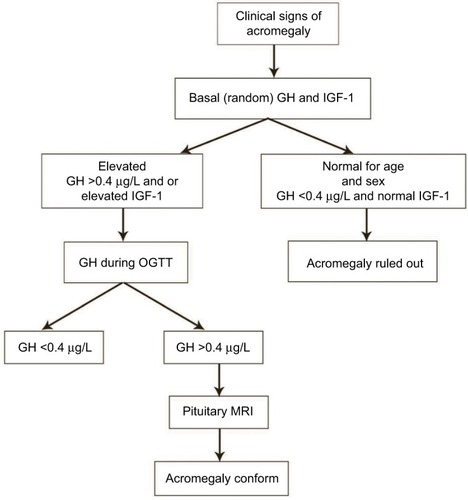
Figure 1 Diagnostic flow of acromegaly.
Abbreviations: GH, growth hormone; IGF-1, insulin-like growth factor-1; OGTT, oral glucose tolerance test; MRI, magnetic resonance imaging.
Cardiovascular complications
One of the most prevalent comorbidities related to acromegaly is cardiovascular disorder,Citation8 occurring in 60% of patients with acromegaly.Citation12 Cardiovascular disorders act as negative determinants for life expectancy in acromegaly patients. Acromegaly is associated with a typical cardiomyopathy, characterized by biventricular hypertrophy, and hypertension is one of the most common cardiovascular comorbidities in acromegaly, with an average prevalence of ~35%. In addition, congestive heart failure, cardiomyopathy, arrhythmias, coronary disease, and hypertension commonly occur.
Pulmonary and respiratory complications
Patients suffering from acromegaly have altered structures of the respiratory apparatus, which lead to severe respiratory problems.Citation2,Citation8 Respiratory complications associated with acromegaly include sleep breathing disorders, generally represented by sleep apnea, which affects up to 80% of patients, and respiratory insufficiency. The anatomical changes in respiratory structures affect lung volumes, respiratory mucosa/cartilage, lung elasticity, chest muscle structure, and respiratory muscle activities. Some patients develop a barrel chest as a result of the changes in vertebral and costal morphology. Other complications include hyperventilation, and hypertrophy of the laryngeal mucosa and cartilage, causing sleep apnea and excessive snoring.Citation8,Citation12
Gastrointestinal complications
Development of colon carcinoma, adenomatous polyps, and dolichocolon are some of the common gastrointestinal problems detected in acromegaly patients.Citation12 It is accepted that the risk of colon cancer is higher in acromegalic patients than in the general population.Citation32
Orthopedic comorbidities
Arthropathy widely occurs in patients with acromegaly, along with vertebral fractures, joint disease, and loss of weight-bearing ability. Early diagnosis of acromegaly may decrease the risk of bone and joint disease, resulting in improved quality of life.
Metabolic disorders
Increased secretion of GH and IGF-1 leads to abnormal glucose regulation, causing diabetes mellitus. A defect in lipid metabolism is also observed in some patients with acromegaly.Citation13
Cancer
The high level of IGF-1 in acromegaly is related to an increased risk of some cancers, particularly colon cancer and thyroid cancer.Citation8 An increased incidence of micronucleus (MN) and oxidative DNA damage in lymphocytes of patients with acromegaly was found by Hamurcu et al.Citation22 An increased MN frequency (chromosomal DNA damage) in peripheral blood lymphocytes is predictive of an increased risk of cancer in humans. Thus, the increase in chromosomal/oxidative DNA damage and the positive association between MN frequency and serum IGF-1 levels may predict an increased risk of malignancy in acromegalic patients.Citation23
Other complications
Women suffering from acromegaly have higher probabilities of menstrual irregularities and infertility. Hyperprolactinemia was also found to develop in 30% of patients.Citation12
Mortality
The mortality rate in patients with active acromegaly is two to four times higher than in the general population.Citation3 This is mostly due to cardiovascular disorders, pulmonary complications, and diabetes mellitus. Cardiovascular disease has historically been reported to represent the primary cause of death in these patients, contributing to nearly 50% of increased mortality. However, according to recent studies, the most common cause of mortality in acromegaly was malignancy, followed by cardiovascular diseases,Citation29,Citation30 then respiratory problems and neoplasias, accounting for ~25% and 15% of mortality, respectively.Citation14 There is a direct correlation between the mortality rate and excess GH and IGF-1 secretion. Normalization of GH and IGF-1 has been found to reduce the mortality rate and disease-related morbidity.Citation3 A positive correlation also exists between mortality in acromegaly patients and colorectal cancer.Citation12 However, with advances in the management strategies of acromegaly and its associated comorbidities, there have been marked improvements in the survival rate and quality of life of patients with acromegaly.Citation13
Diagnosis of acromegaly
Acromegaly is a chronic, debilitating disorder with slow disease onset, which impedes accurate diagnosis in the early stages.Citation15 None of the signs and symptoms is sensitive enough to be detected at the beginning of the disease. Failure to recognize appropriate symptoms causes a delay in disease diagnosis, leading to a high incidence of acromegaly.Citation4 According to a study by Reid et al, involving 324 acromegaly patients from the periods 1981–1994 and 1995–2006, the majority of patients showed many clinical symptoms and complications consistent with the disease being at an advanced stage at diagnosis, indicating that there is a high prevalence of underdiagnosed acromegaly.Citation11,Citation13 In general, primary care physicians diagnose ~40% of patients with acromegaly.Citation33 Nevertheless, patients often consult other specialists and dentists, besides primary care physicians, before obtaining the correct diagnosis, and are then treated according to the presenting symptoms, instead of being treated for acromegaly.Citation16
The phenotype of acromegaly develops gradually over several years; usually, the first clinical manifestation of the disease includes the growth of acral parts and physiognomic alterations.Citation12 Thus, comparison of new and old facial photographs was conventionally used in early detection of the disease. The main drawback in considering phenotypic alterations for the initial recognition of acromegaly is that only 50% of patients with somatotroph adenomas reveal distinct phenotypic changes, whereas the other 50% either show insignificant symptoms or are completely asymptomatic, even having elevated levels of GH and IGF-1, and even after several years of observation.Citation13 Another possible method for early diagnosis of acromegaly is to use software to depict the features that have developed as a result of acromegaly in a single photograph of the patient’s face.Citation12 However, the sensitivity and specificity of the computer modeling system in early acromegaly are not yet clear. Once there is a clinical suspicion of acromegaly, biochemical tests should be performed for every patient to confirm the diagnosis.
Biochemical tests
GH level
The biochemical diagnosis of acromegaly is traditionally based on the levels of oversecreted GH and IGF-1. However, in normal healthy individuals the levels of circulating GH secreted from the pituitary fluctuate greatly throughout the day owing to the pulsatile nature of GH production.Citation17 Maximum secretion of GH occurs at night in accordance with sleep stages. The value of GH usually ranges between 0.1–0.2 µg/L and 5–30 µg/L during the secretory bursts, and these values overlap with the values observed in acromegaly patients.Citation12 A random GH value <0.04 µg/L with a normal level of IGF-1 (matched for age and gender) excludes the diagnosis. Thus, determination of the GH level is of minimal diagnostic utility in acromegaly. Instead, a GH level <0.4 ng/mL in an oral glucose tolerance test (OGTT) is the gold standard for diagnosis.Citation13 In normal individuals, the GH nadir value during an OGTT is undetectable as secretion is suppressed, but the value is very high in acromegaly patients owing to the lack of suppression.Citation2
IGF-1 level
IGF-1, the level of which is correlated with mean GH level, has been used as a biomarker of acromegaly since the turn of the millennium.Citation5 Measurement of circulating IGF-1 is considered a vital biochemical tool because of its long half-life of 18–20 hours and stability throughout the day.Citation5 An elevated IGF-1 level along with inability to reduce GH levels <1 µg/L in an OGTT is considered an important criterion for acromegaly detection.Citation1 Although a correlation exists between the levels of serum IGF-1 and GH, some acromegaly patients show high IGF-1 levels in spite of a normal daily GH concentration, indicating a complex correlation between them, which cannot be simply explained by GH elevation.Citation13 Regardless of the substantial advantages of IGF-1 as a biochemical tool, there are certain limitations to its use. The IGF-1 level is affected by multiple physiological factors such as age, gender, and body mass index, and these should be considered during data interpretation. The IGF-1 level is raised during normal pregnancy and puberty and rarely represents a clinical problem. In contrast, malnutrition, liver and renal failure, hypothyroidism, and insulin-dependent diabetes reduce the level of IGF-1. Major technical problems of IGF-1 assay include interference caused by endogenous IGF-1-binding protein and the tendency of IGF-1 to plateau at mean GH levels.Citation5 All these factors lead to variability in IGF-1 assay performance. Therefore, technical refinements of IGF-1 biochemical assays, validation of assay performance, and assay-specific reference data are essential to detect specific clinical conditions related to acromegaly.Citation18
Immunoassays
For accurate diagnosis of acromegaly, it is imperative to have a highly sensitive GH assay, with the ability to detect GH levels <1.0 ng/mL. The development of a radioimmunoassay (RIA) to measure serum GH and IGF-1 levels presented a biochemical device to diagnose acromegaly. RIA has several limitations as a result of which more sensitive immunoassays, such as immunoluminometric and immunoradiometric assays based on the use of monoclonal antibodies, have been developed to measure plasma GH and IGF-1 levels precisely in patients with suspected acromegaly. These assays can determine GH concentrations <0.05 µg/mL;Citation19 the sensitivity of these immunoassays is up to 100 times greater than RIA.Citation20 However, one limitation of these assays is proper reproducibility. Variability of measured GH values occurs owing to the lack of universal standards, recognition of non-uniform antibodies by GH isoforms, and the presence of circulating GH-binding protein. Hence, more authentic and reliable ultrasensitive GH assays based on strong reference standards are required.Citation19
Imaging studies
MRI with contrast administration is considered to be the most effective imaging technique to locate the pituitary source of excess GH.Citation12 MRI is a sensitive and reliable technique, which enables the identification of very small tumors, even smaller than 2 mm, tumor invasiveness, proximity to the optic chiasm, and compression of surrounding structures by the tumor which previously remained undetected.Citation5 The majority of somatotroph adenomas (75%–85%) are macroadenomas (>10 mm in diameter) at the time of diagnosis, which rarely grow into the cavernous sinus.Citation12 MRI helps to identify a pituitary macroadenoma in acromegaly patients.Citation2 Advanced MRI techniques such as post-contrast, volumetric interpolated breath-hold MRI can detect acromegaly in patients with pituitary tumors, which was otherwise unidentified by traditional spin-technique T1-weighted MRI. Hence, improved MRI techniques have advantages over conventional methods for the diagnosis of acromegaly.Citation13
Rarely, acromegaly occurs as a result of ectopic tumors producing GH or GHRH. When a biochemical diagnosis has been established for acromegaly without any pituitary tumor or diffused pituitary enlargement is detected, physicians should suspect ectopic sources.Citation12 Measurement of the plasma GHRH level is beneficial in identifying ectopic sources of tumor.Citation5
Treatment of acromegaly
Improved understanding of the disease mechanism has led to the development of successful treatment modalities of acromegaly. Novel surgical techniques are used to operate on pituitary tumors.
The majority of pituitary tumor operations in patients with acromegaly are performed by transsphenoidal surgery.Citation30 Some surgeons use an image intensifier for navigation while others choose neuronavigation. A submucosal tunnel is dissected, usually followed by a medial nasal incision. The mucosal tunnel is kept open by a nasal speculum. Then the operating microscope is introduced. Sphenoidotomy is performed using the vomer as a midline orientation. A direct perinasal intervention to the sphenoid sinus is usually chosen by endoscopic transsphenoidal surgeons. The transnasal/transsphenoidal technique seems to be accurate and safe, with good surgical results. Based on the preoperative MRI, the decision is made to carry out a curative or debulking procedure. The resectioning of the adenoma depends on the size and invasive character of the tumor. For patients who are not cured by surgery, or for those whose health status prohibits surgery, medical therapy using somatostatin analogs and GH-receptor antagonists is considered to be the principal therapy.Citation1,Citation13 For those patients in whom both surgical and medical therapy fails to provide biochemical control of acromegaly, radiation therapy is the best curative technique. Sometimes, more than one treatment procedure is required. In almost all cases, long-term treatment and monitoring are essential.Citation1 With progress in disease management, the prognosis of the disease has improved, and in the majority of the cases adequate hormonal disease control is attained, resulting in life expectancy comparable to the general population.Citation21
Conclusion
Acromegaly is a rare, devastating disorder associated with multiple comorbidities, poor quality of life, and increased mortality. Timely diagnosis and subsequent therapies are vital for successful prevention of disease and premature death. To mitigate the problems related to the delay in diagnosis of acromegaly, it is essential to develop awareness about the early signs and symptoms of the disease among primary care physicians, specialists, dentists, and other health care professionals. In addition, better communication and collaboration are necessary between patients and health care providers for disease diagnosis as well as long-term care. Recently, several techniques have been developed to aid in the early identification and monitoring of acromegaly and its associated complications. These advances in disease identification have led to a rise in the number of patients diagnosed with the disease and the development of better treatment modalities. This, in turn, will result in increased cure and decreased mortality rates in acromegaly patients.
Acknowledgments
The author is thankful to www.manuscriptedit.com for providing English language editing and proofreading services for this manuscript.
Disclosure
The author reports no conflicts of interest in this work.
References
- AdelmanDTLiebertKJNachtigallLBLamersonMBakkerBAcromegaly: the disease, its impact on patients, and managing the burden of long-term treatmentInt J Gen Med20136313823359786
- BanerjeeAPatelKWrenAMAcromegaly- clinical manifestations and diagnosisPharm J200313273278
- NachtigallLDelgadoASwearingenBLeeHZeriklyRKlibanskiAExtensive clinical experience: changing patterns in diagnosis and therapy of acromegaly over two decadesJ Clin Endocrinol Metab2008932035204118381584
- SchneiderHJSieversCSallerBWittchenHUStallaGKHigh prevalence of biochemical acromegaly in primary care patients with elevated IGF-1 levelsClin Endocrinol2008693432435
- CorderoRABarkanALCurrent diagnosis of acromegalyRev Endocr Metab Disord200891131918236162
- CannavòSFerraùFRagoneseMIncreased prevalence of acromegaly in a highly polluted areaEur J Endocrinol2010163450951320621957
- MelmedSMedical progress: AcromegalyN Engl J Med2006355242558257317167139
- AbreuATovarAPCastellanosRChallenges in the diagnosis and management of acromegaly: a focus on comorbiditiesPituitary201619444845727279011
- BrabantGInsulin-like growth factor-I: marker for diagnosis of acromegaly and monitoring the efficacy of treatmentEur J Endocrinol2003148Suppl 2S15S2012670296
- IsidroMLIglesias DíazPMatías-GuiuXCordidoFAcromegaly due to a growth hormone-releasing hormone-secreting intracranial gangliocytomaJ Endocrinol Invest200528216216515887863
- ReidTJPostKDBruceJNNabi KanibirMReyes-VidalCMFredaPUFeatures at diagnosis of 324 patients with acromegaly did not change from 1981 to 2006: acromegaly remains under-recognized and under-diagnosedClin Endocrinol2010722203208
- LugoGPenaLCordidoFClinical manifestations and diagnosis of acromegalyInt J Endocrinol2012201254039822518126
- Ribeiro-OliveiraABarkanAThe changing face of acromegaly--advances in diagnosis and treatmentNat Rev Endocrinol201281060561122733271
- HoldawayIMRajasooryaRCGambleGDFactors influencing mortality in acromegalyJ Clin Endocrinol Metab200489266767414764779
- Ben-ShlomoASheppardMCStephensJMPulgarSMelmedSClinical, quality of life, and economic value of acromegaly disease controlPituitary201114328429421597975
- Kreitschmann-AndermahrISiegelSKleistBDiagnosis and management of acromegaly: the patient’s perspectivePituitary201619326827626742496
- MelarvieSJeevanandamMHoladayNJPetersenSRPulsatile nature of growth hormone levels in critically ill trauma victimsSurgery199511744024087716722
- ClemmonsDRConsensus statement on the standardization and evaluation of growth hormone and insulin-like growth factor assaysClin Chem201157455555921285256
- MelmedSAcromegaly pathogenesis and treatmentJ Clin Invest2009119113189320219884662
- CostaACRossiAMartinelliCEMachadoHRMoreiraACAssessment of disease activity in treated acromegalic patients using a sensitive GH assay: should we achieve strict normal GH levels for a biochemical cure?J Clin Endocrinol Metab20028773142314712107214
- GiustinaAChansonPBronsteinMDA consensus on criteria for cure of acromegalyJ Clin Endocrinol Metab20109573141314820410227
- HamurcuZCakirIDonmez-AltuntasHMicronucleus evaluation in mitogen-stimulated lymphocytes of patients with acromegalyMetabolism2011601620162621550080
- BayramFBitgenNDonmez-AltuntasHIncreased genome instability and oxidative DNA damage and their association with IGF-1 levels in patients with active acromegalyGrowth Horm IGF Res2014241293424382376
- DuttaPHajelaAPathakAClinical profile and outcome of patients with acromegaly according to the 2014 consensus guidelines: Impact of a multi-disciplinary teamNeurol India201563336036826053808
- DayPFLotoMGGlereanMPicassoMFLovazzanoSGiuntaDHIncidence and prevalence of clinically relevant pituitary adenomas: retrospective cohort study in a Health Management Organization in Buenos Aires, ArgentinaArch Endocrinol Metab201660655456127982201
- RosarioPWCalsolariMRLaboratory investigation of acromegaly: Is basal or random GH > 0.4 µg/L in the presence of normal serum IGF-1 an important result?Arch Endocrinol Metab2015591545825926115
- CordidoFGarcía ArnésJAMarazuela AspirozMTorres VelaEPractical guidelines for diagnosis and treatment of acromegalyEndocrinología y Nutrición2013608457.e145723660006
- PrencipeNFlorianiIGuaraldiFACROSCORE: a new and simple tool for the diagnosis of acromegaly, a rare and underdiagnosed diseaseClin Endocrinol2016843380385
- ÖbergKLambertsSWSomatostatin analogues in acromegaly and gastroenteropancreatic neuroendocrine tumours: past, present and futureEndocr Relat Cancer20162312R551R56627697899
- BuchfelderMSchlafferSSurgical treatment of pituitary tumours. Best practice & researchClin Endocrinol Metab200923677692
- CottierJPDestrieuxCBrunereauLCavernous sinus invasion by pituitary adenoma: MR imagingRadiology2000215246346910796926
- TiroshAShimonIComplications of acromegaly: thyroid and colonPituitary2017201707527631334
- ChiaghanaCOBauerfeindJMSulekCAGoldsteinJCAwoniyiCAAcromegaly discovered during a routine out-patient surgical procedure: a case reportJ Med Case Rep201711116928645320