
Abstract
Background
Disseminated avascular coagulation (DIC) is the main cause of death among patients with sepsis. In particular, low platelet count is predictive of poor outcome. However, the significance of platelet activation in patients with sepsis-related DIC is poorly understood. To determine the characteristics of platelet-related abnormality in patients with sepsis-related DIC, we assessed the expression levels of several biomarkers.
Methods
Plasma levels of biomarkers, including cytokines, chemokines, soluble selectins, platelet-derived microparticles (PDMPs), soluble vascular adhesion molecule 1, and high mobility group box protein 1 were measured by enzyme-linked immunosorbent assay at baseline and after 4, 7, 14, and 21 days of DIC treatment.
Results
Differences in platelet activation and in the elevation of activated platelet-related PDMPs and of soluble P-selectin were seen between patients suffering from sepsis and hematologic malignancy with DIC. In addition, the elevation of interleukin (IL)-6 and thrombopoietin (TPO) was significant in sepsis patients with DIC. Furthermore, IL-6 and TPO promoted platelet activation in vitro.
Conclusion
Assessment of PDMPs, sP-selectin, IL-6, and TPO may be beneficial in the primary prevention of multi-organ failure in sepsis patients with DIC.
Introduction
Disseminated intravascular coagulation (DIC) is frequently complicated by sepsis or hematologic malignancy, and shows fulminant clinical signs of hemorrhage.Citation1 In addition to deterioration attributable to the original disease, DIC development doubles a specific patient’s risk of death.Citation1,Citation2 Coagulation abnormalities and thrombocytopenia are common in DIC, and the extent of hemostatic disorders appears to correlate with disease severity.Citation3
In particular, low platelet count is predictive of poor outcome.Citation4 However, the significance of platelet activation in patients with sepsis-related DIC is poorly understood. The pathophysiology of DIC is complex and involves numerous interactions between the coagulation cascade, the host immune and inflammatory system, and the damaged vascular endothelium.Citation5 Although the diagnosis of sepsis-associated DIC is a complex clinical problem, this exaggerated response can lead to multi-organ failure, shock, and death.Citation5,Citation6 The severity of organ dysfunction has prognostic value, and in clinical practice is usually classified according to the Sequential Organ Failure Assessment (SOFA) score.Citation7 Several scoring systems for DIC have been proposed and tested, with the system proposed by the International Society of Thrombosis and Hemostasis being the most widely accepted.Citation8,Citation9
In the present study, we assessed the levels of various biomarkers in patients with sepsis-related DIC, including cytokines, chemokines, soluble selectins, platelet-derived microparticles (PDMPs),Citation10–Citation13 soluble vascular adhesion molecule 1 (sVCAM-1) protein, and high mobility group box 1 (HMGB1) protein. The purpose of the study was to clarify the characteristics of platelet-related abnormality in patients with sepsis-related DIC.
Patients and methods
Patients
The study cohort included 25 sepsis patients, 18 with and 7 without DIC, selected from those admitted to our hospital between April 2013 and August 2016. An additional group comprised 15 patients with hematological malignancy (HM; acute leukemia, malignant lymphoma, or multiple myeloma) and DIC. Three patients received angiotensin II receptor blocker in addition to statin. However, all patients not received any supplements that may effect on coagulation and inflammation, such as omega 3, vitamin E, coenzyme Q10, and vitamin K. A control group comprised 12 healthy volunteers. The study protocol was approved by our institutional review board of Kansai Medical University, and written informed consent was obtained from each patient. The 3 groups of patients and the healthy volunteers were compared in terms of age, sex, infection focus, vital signs, the Japanese Association for Acute Medicine (JAAM) DIC scoreCitation14 along with the positive rate, the SOFA scoreCitation7,Citation15 on ICU admission, and therapeutic agents. Moreover, sepsis biomarkers and coagulation/fibrinolysis markers were compared between the groups.
Data collection
Baseline data for the coagulation markers, including fibrin/fibrinogen degradation products (FDP), D-dimers, prothrombin time ratios, platelet counts, and antithrombin (AT) activity were measured before treatment. The Acute Physiology and Chronic Health Evaluation II (APACHE II) and SOFA scores were also calculated. The diagnosis of DIC was established using the JAAM and Japanese Ministry of Health and Welfare (JMHW) DIC criteria.Citation14,Citation16 Serial data for each coagulation marker, APACHE II score, SOFA score, JAAM-DIC, and JMHW-DIC criteria were also measured after the start of treatment.
Measurement of PDMPs
An ELISA kit used for PDMP measurements was obtained from JIMRO Co. Ltd. (Tokyo, Japan).Citation17 The kit used 2 monoclonal antibodies against glycoproteins CD42b and CD42a. One U/mL of PDMPs for this ELISA kit was defined as the amount of PDMPs obtained from solubilized 24,000 platelets/mL. Blood samples were collected from peripheral veins into vacutainers containing EDTA-anticoagulant citrate dextrose (NIPRO Co. Ltd., Osaka, Japan) using 21-gauge needles to minimize platelet activation. The samples were gently mixed by turning the tubes up-side down once or twice and then kept at room temperature for the maximum period of 2–3 hours. Immediately after centrifugation at 8,000 × g for 5 minutes, 200 µL was collected from the upper layer supernatant of the 2 mL samples to avoid contamination by platelets. The collected samples were stored at −40°C until analysis. The PDMP levels were measured twice and the mean values were recorded. Furthermore, some basic studies were carried out prior to this measurement using clinical specimens.
Measurement of cytokines and soluble molecules
Blood samples from patients and controls under fasting conditions were collected into tubes with or without sodium citrate and allowed to clot at room temperature for a minimum of 1 hour. Citrated plasma or serum, respectively, was isolated by centrifugation at 1,000 × g for 20 minutes at 4°C and stored at −30°C until analyzed. Plasma concentrations of interleukin (IL)-6, thrombopoietin (TPO), soluble P-selectin (sP-selectin), sE-selectin, sL-selectin, sVCAM-1, and soluble CD40 ligand (sCD40L) were measured using monoclonal antibody-based ELISA kits (Invitrogen Inc., Camarillo, CA, USA). sVCAM-1 was identified in plasma samples. A monoclonal antibody specific for human VCAM-1 has been pre-coated onto a microplate. Samples were frozen if not analyzed shortly after collection. Multiple freeze-thaw cycles of frozen samples were unavoidable in this study. Forty assays were evaluated and the minimum detectable dose of human VCAM-1 ranged from 0.17 to 1.26 ng/mL. Samples from apparently healthy volunteers were evaluated for the presence of human VCAM-1 in this assay. The range of healthy plasma was 341–897 ng/mL and SD was 132.5 ng/mL. HMGB1 was measured using an HMGB1 ELISA Kit II (Shino-test Corp., Kanagawa, Japan). The recombinant products and standard solutions provided with each kit were used as positive controls in each assay and all procedures were performed according to the manufacturers’ instructions.
Cutoff value of the marker
Receiver operating characteristic analysis was performed and the optimal cutoff value of 28-day mortality was calculated using the marker that was selected in multivariate logistic regression.
Study of platelet activation using agonists and cytokines
To study the effect of cytokines on platelet activation and the activation-related release of PDMPs, platelet activation tests were performed using agonists, adenosine diphosphate (ADP), and collagen (Funakoshi Inc., Tokyo, Japan). IL-6 and TPO were highly purified and were checked carefully for contaminants, such as endotoxin by the supplier. Platelet-rich plasma (400 µL) was incubated with cytokines (IL-6, 10 ng/mL, or TPO, 10 ng/mL; BioSourse International Inc., Camarillo, CA, USA) and then exposed to 2 µM ADP plus 1 µg/mL collagen. 4-(2-Hydroxyethyl)-1-piperazineethane-sulfonic acid-Tyrode’s buffer containing 2 mM EDTA was added, and platelet was removed by centrifugation at 1,000 × g for 15 minutes. PDMP and sCD40L levels were determined by the aforementioned ELISA methods.
Treatment
When patients met the JAAM-DIC criteria and had an AT activity level of <70%, AT concentrate (Nihon Pharmaceutical Co. Ltd., Tokyo, Japan) was administered for up to 3 consecutive days unless the patient died or treatment was stopped for any other justifiable reason.Citation18 The concomitant use of other anticoagulants was not prohibited, and recombinant thrombomodulin (rTM; Asahi Kasei Parma Corporation, Tokyo, Japan) was administered intravenously according to the drug manufacturer’s recommendation (0.06 mg/kg/day for 6 days by either intravenous bolus injection or intravenous infusion over 15 minutes via a catheter).Citation19 Standard sepsis care was performed, and platelet concentrate and fresh-frozen plasma were used for substitution therapy, if necessary.Citation18
Statistics
Data are expressed as mean ± SD. Between-group comparisons were analyzed using the Newman–Keuls and Scheffe’s tests. Correlations were assessed with Spearman’s rank correlation test. The significance of differences among variables was determined by analysis of variance. P-values <0.05 were considered statistically significant. All analyses were performed using the StatFlex program (version 6).
Results
Patient demographic and clinical characteristics are shown in . Age and sex were similar in the patients (both sepsis and HM) and the healthy controls. The APACHE II scores, DIC scores, FDP, and D-dimer levels were significantly higher in patients suffering from sepsis with DIC vs sepsis without DIC. However, antithrombin III (ATIII) was significantly lower in patients with sepsis and DIC compared with sepsis without DIC.
Table 1 Demographic and clinical characteristics of the patients and controls
The levels of PDMP, IL-6, TPO, HMGB1, sVCAM-1, sP-selectin, sE-selectin, and sL-selectin were compared in plasma from patients with sepsis and DIC vs healthy volunteers (). In addition, the levels of PDMP, IL-6, TPO, and sP-selectin were found to be significantly elevated in patients with sepsis and DIC compared with HM and DIC (PDMP, P<0.05; IL-6, P<0.01; TPO, P<0.01; sP-selectin, P<0.05). However, there were no significant differences in HMGB1, sVCAM-1, sE-selectin, or sL-selectin between these 2 groups.
Table 2 Comparison of PDMPs, cytokines, and soluble factors between the patients and controls
Correlations between the 2 platelet activation markers (PDMP and sP-selectin) and cytokines are summarized in . There were significant positive correlations of platelet activation markers with IL-6 and TPO in patients with sepsis and DIC, but not HM and DIC.
Table 3 Correlations of PDMPs and sP-selectin with cytokines in sepsis and HM patients with DIC
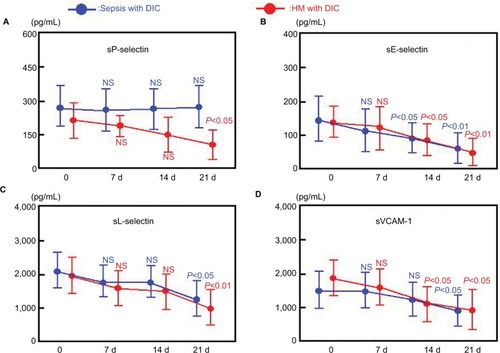
We divided DIC patients into 2 subgroups according to their fundamental disease, either sepsis or HM. After DIC treatment, the sepsis subgroup showed significant reductions in plasma concentrations of HMGB1, IL-6, sE-selectin, sL-selectin, and sVCAM-1 relative to baseline (P<0.05 or P<0.01; and ). However, there was no significant change from baseline in PDMP, TPO, or sP-selectin levels in these patients after treatment for DIC ( and ).
Figure 1 Plasma concentrations of PDMPs, HMGB1, IL-6, and TPO before and after ATIII or rTM treatment of DIC patients.
Abbreviations: ATIII, antithrombin III; DIC, disseminated intravascular coagulation; HM, hematologic malignancy; HMGB1, high mobility group box 1; IL-6, interleukin-6; NS, not significant; PDMP, platelet-derived microparticle; rTM, recombinant thrombomodulin; TPO, thrombopoietin.
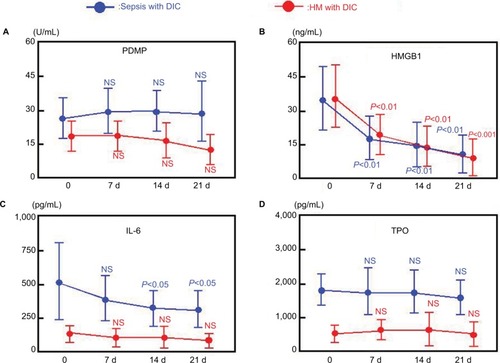
Figure 2 Plasma concentrations of sP-selectin, sE-selectin, sL-selectin, and sVCAM-1 before and after ATIII or rTM treatment of DIC patients.
Abbreviations: ATIII, antithrombin III; DIC, disseminated intravascular coagulation; HM, hematologic malignancy; NS, not significant; rTM, recombinant thrombomodulin; sP-selectin, soluble P-selectin; sE-selectin, soluble E-selectin; sL-selectin, soluble L-selectin; sVCAM-1, soluble vascular cell adhesion molecule-1.
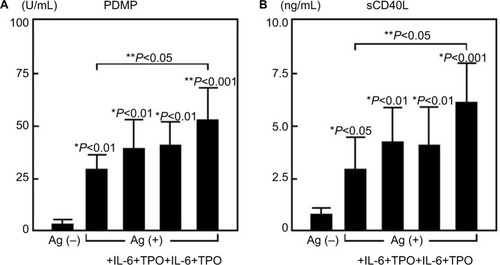
To study the effect of cytokines on platelet activation in sepsis patients, a platelet activation test was conducted using the agonists, ADP and collagen (). Both PDMP and sCD40L were significantly elevated in platelets stimulated by the agonists compared with unstimulated platelets (). Furthermore, the addition of IL-6 or TPO enhanced the elevation of PDMPs and sCD40L. The addition of both cytokines together significantly enhanced the elevation of PDMP, and sCD40L (P<0.05) ().
Figure 3 Study of platelet activation by agonists and cytokines.
Abbreviations: Ag, agonist; PDMP, platelet-derived microparticle; sCD40L, soluble CD40 ligand; IL-6, interleukin-6; TPO, thrombopoietin.
Discussion
DIC complicated by leukemia is characterized by exaggerated fibrinolysis, but the consumption of ATIII is relatively low. On the other hand, DIC complicated by infection or sepsis is coagulation-predominant, resulting in the over-consumption of ATIII. The present study confirmed these tendencies; ATIII levels in sepsis with DIC vs HM with DIC were 57.5% ± 4.7% vs 71.3 ± 4.6%. Coagulopathies are present in many sepsis patients,Citation20,Citation21 but the severity of sepsis-associated coagulopathy is variable, ranging up from subclinical abnormalities detectable only by a mild decrease in platelet count.Citation22 Therefore, a low platelet count is a well-known biomarker for sepsis disease severity.
Platelets also play a role in the pathogenesis of multi-organ failure.Citation6 Platelet interaction with immune and endothelial cells is a well-known and conserved response against infection and sepsis.Citation6 In particular, the elevation of neutrophils is remarkable in these diseases. Thus, platelets are also involved in the formation of neutrophil extracellular traps (NETs), which trap microorganisms and facilitate their clearance.Citation23 The formation of NETs by platelets can promote thrombosis and contribute to organ failure.Citation24
Platelets show complex interactions with neutrophils and the endothelium, resulting in altered glycocalyx and cytokine release.Citation25 In these interactions, there is no doubt that P-selectin is the most important molecule. P-selectin is contained in platelet α-granules and expressed on the membrane surface after activation.Citation26 Greco et alCitation6 previously reported that P-selectin-mediated adhesion is an important platelet–endothelial cell–leukocyte interaction in sepsis. In the present study, levels of sP-selectin were significantly elevated in sepsis patients, both with and without DIC, compared with patients suffering from HM with DIC. These results are consistent with previous reports. We suspect that the low platelet count in HM patients with DIC is caused by bone marrow dysfunction. Therefore, it may be difficult to detect elevated sP-selectin in these patients.
Another interesting result of the present study involves PDMPs. PDMPs were elevated in patients with both sepsis and HM, compared with healthy volunteers. However, PDMPs in sepsis patients with DIC were elevated to the greatest extent. PDMPs are small vesicles released from platelet surface, which function as storage repositories for coagulation factors and cytokines.Citation11,Citation12,Citation27 Elevated PDMP levels correlate with the severity of sepsis in clinical studies.Citation28–Citation30 Furthermore, studies investigating the effect of intravenous PDMPs in rats found that they resulted in deranged clotting, acute respiratory distress syndrome (ARDS), and a hemodynamic syndrome typical of sepsis.Citation31,Citation32 Our results and previous reports suggest that the elevation of PDMPs in sepsis patients with DIC originates platelet activation during the progression of sepsis.
Inflammatory cytokines such as IL-6 can modulate platelet activation.Citation33 Interestingly, TPO has this ability as well.Citation34–Citation36 TPO may also be involved in platelet–leukocyte interaction and the development of organ damage in sepsis.Citation6 TPO levels are increased in inflammatory states,Citation37 enhancing the response of mature platelets to several agonists, increasing platelet–leukocyte adhesion via P-selectin, increasing reactive oxygen species release, and inducing IL-8 production by neutrophils and monocytes.Citation38–Citation40 Furthermore, significantly elevated levels of TPO have been shown in both murine and human sepsis.Citation41–Citation43 In the present study, IL-6 and TPO levels were both significantly elevated in patients suffering from sepsis with DIC compared with HM with DIC. We postulated that platelet activation in sepsis patients would be consequence of their elevated IL-6 and TPO. Thus, platelet activation tests performed to measure the effect of IL-6 and TPO on platelet activation in these patients. The addition of IL-6 and TPO significantly enhanced the elevation of PDMP and sCD40L. These results suggest that IL-6 and TPO enhanced the platelet–endothelial cell–leukocyte interaction in sepsis, resulting in the elevation of sP-selectin, sE-selectin, and sL-selectin.
The significance of platelet activation in sepsis is also previously reported.Citation6,Citation44–Citation48 ARDS is one of the most severe complications of sepsis and finally causes endothelial damage and intravascular coagulation.Citation44 Katz et alCitation45 reported that post mortem biopsies of patients who died with ARDS showed excess numbers of platelets and neutrophil deposition in pulmonary vessels. In addition, enhanced platelet activation has also been demonstrated in bronchoalveolar lavage of patients with ARDS.Citation46 Acute kidney injury (AKI) is also a frequent complication of sepsis.Citation47 Tőkés-Füzesi et alCitation48 reported that the correlation between PDMPs and blood urea nitrogen in AKI was indicated in sepsis patients. Therefore, these previous reports may propose as possible targets for sepsis prevention and treatment.Citation49,Citation50
This study has 2 potential strengths. First, we clarified differences in platelet activation and the elevation of PDMPs and of sP-selectin between patients suffering from sepsis with DIC and HM with DIC. Second, we showed that elevation of IL-6 and TPO promotes the induction of PDMPs and sP-selectin in sepsis patient with DIC. However, the study also had several limitations. First, patient numbers were small. Second, changes in clinical parameters of fibrinolysis, such as soluble-fibrin or plasminogen activator inhibitor-1 were not routinely recorded. Third, we could not identify the causes of different platelet counts in the sepsis and HM groups. HM patients had poorer values for platelet counts, suggesting that bone marrow inhibition was associated with these differences. Fourth, we could not clarify the significance of HMGB1, sP-selectin, and PDMP levels after DIC treatment. Extension of these findings in larger and more specific studies would be useful. Finally, we were unable to evaluate the therapeutic effects of ATIII and rTM using DIC scores. We suggest that the assessment of DIC scores in ATIII or rTM-treated DIC patients would be beneficial.
Conclusion
Differences were found between patients suffering from sepsis with DIC and HM with DIC in platelet activation and in the elevation of activated platelet-related PDMPs and sP-selectin. In addition, IL-6 and TPO were significantly elevated in sepsis patients with DIC. IL-6 and TPO promoted platelet activation in vitro. Assessment of these biomarkers may be beneficial in the primary prevention of multi-organ failure in sepsis patients with DIC. However, larger clinical trials are required to test this hypothesis.
Acknowledgments
This study was partly supported by a grant from the Japan Foundation of Neuropsychiatry and Hematology Research, a Research Grant for Advanced Medical Care from the Ministry of Health and Welfare of Japan, and a Grant (13670760 to S.N.) from the Ministry of Education, Science and Culture of Japan. We thank Nicholas Rufaut, Phd, from Edanz Group (www.edanzediting.com/ac) for editing a draft of this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
- LeviMTen CateHDisseminated Intravascular CoagulationN Engl J Med Overseas Ed19993418586592
- SaraccoPVitalePScolfaroCPollioBPagliarinoMTimeusFThe coagulopathy in sepsis: significance and implications for treatmentPediatr Rep201134e3022355515
- TohCHDennisMDisseminated intravascular coagulation: old disease, new hopeBMJ2003327742197497714576251
- YaguchiALoboFLVincentJLPradierOPlatelet function in sepsisJ Thromb Haemost20042122096210215613012
- WalbornAHoppensteadtDSyedDMosierMFareedJBiomarker Profile of Sepsis-Associated Coagulopathy Using Biochip Assay for Inflammatory CytokinesClin Appl Thromb Hemost201824462563228514870
- GrecoELupiaEBoscoOVizioBMontrucchioGPlatelets and Multi-Organ Failure in SepsisInt J Mol Sci20171810E220029053592
- HowellMDDavisAMManagement of Sepsis and Septic ShockJAMA2017317884784828114603
- TaylorFBTohCHHootsWKWadaHLeviMScientific Subcommittee on Disseminated Intravascular Coagulation (DIC) of the International Society on Thrombosis and Haemostasis (ISTH)Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulationThromb Haemost20018651327133011816725
- WadaHThachilJdi NisioMGuidance for diagnosis and treatment of DIC from harmonization of the recommendations from three guidelinesJ Thromb Haemost201311761767
- NomuraSOzakiYIkedaYFunction and role of microparticles in various clinical settingsThromb Res2008123182318667228
- NomuraSShimizuMClinical significance of procoagulant microparticlesJ Intens Care201572
- NomuraSMicroparticle and Atherothrombotic DiseasesJ Atheroscler Thromb20162311926412494
- MiyazakiYNomuraSMiyakeTHigh shear stress can initiate both platelet aggregation and shedding of procoagulant containing microparticlesBlood1996889345634648896411
- GandoSIbaTEguchiYA multicenter, prospective validation of disseminated intravascular coagulation diagnostic criteria for critically ill patients: comparing current coagulation diagnostic criteria for critically ill patients: comparing current criteriaCrit Care Med20063462563116521260
- VincentJLde MendonçaACantraineFUse of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Working in intensive care units: results of a multicenter, prospective study. Working group on “sepsis-related problems” of the European Society of Intensive Care MedicineCrit Care Med19982611179318009824069
- KobayashiNMaekawaTTakadaMTanakaHGonmoriHCriteria for diagnosis of DIC based on the analysis of clinical and laboratory findings in 345 DIC patients collected by the Research Committee on DIC in JapanBibl Haematol19834949265275
- OsumiKOzekiYSaitoSDevelopment and assessment of enzyme immunoassay for platelet-derived microparticlesThromb Haemost200185232633011246556
- WadaHAsakuraHOkamotoKExpert consensus for the treatment of disseminated intravascular coagulation in JapanThromb Res2010125161119782389
- IkezoeTPathogenesis of disseminated intravascular coagulation in patients with acute promyelocytic leukemia, and its treatment using recombinant human soluble thrombomodulinInt J Hematol20141001273724217998
- KinasewitzGTYanSBBassonBUniversal changes in biomarkers of coagulation and inflammation occur in patients with severe sepsis, regardless of causative micro-organism [ISRCTN74215569]Crit Care200482R82R9015025782
- ZeerlederSHackCEWuilleminWADisseminated Intravascular Coagulation in SepsisChest200512842864287516236964
- KoyamaKMadoiwaSNunomiyaSCombination of thrombin-antithrombin complex, plasminogen activator inhibitor-1, and protein C activity for early identification of severe coagulopathy in initial phase of sepsis: a prospective observational studyCrit Care2014181R1324410881
- ClarkSRMaACTavenerSAPlatelet TLR4 activates neutrophil extracellular traps to ensnare bacteria in septic bloodNat Med200713446346917384648
- AndrewsRKArthurJFGardinerEENeutrophil extracellular traps (NETs) and the role of platelets in infectionThromb Haemost2014112465966525265341
- InceCMayeuxPRNguyenTTHE ENDOTHELIUM IN SEPSISShock201645325927026871664
- YeoELSheppardJAFeuersteinIARole of P-selectin and leukocyte activation in polymorphonuclear cell adhesion to surface adherent activated platelets under physiologic shear conditions (an injury vessel wall modelBlood1994839249825077513201
- BurnierLFontanaPKwakBRAngelillo-ScherrerACell-derived microparticles in haemostasis and vascular medicineThromb Haemost2009101343945119277403
- Tőkés-FüzesiMWothGErnyeyBMicroparticles and acute renal dysfunction in septic patientsJ Crit Care201328214114722951018
- WothGTőkés-FüzesiMMagyarlakiTKovácsGLVermesIMühlDActivated platelet-derived microparticle numbers are elevated in patients with severe fungal (Candida albicans) sepsisAnn Clin Biochem201249Pt 655456022933445
- OhuchiMFujinoKKishimotoTAssociation of the Plasma Platelet-Derived Microparticles to Platelet Count Ratio with Hospital Mortality and Disseminated Intravascular Coagulopathy in Critically Ill PatientsJ Atheroscler Thromb201522877378225864886
- LiHMengXLiangXGaoYCaiSAdministration of microparticles from blood of the lipopolysaccharide-treated rats serves to induce pathologic changes of acute respiratory distress syndromeExp Biol Med20152401217351741
- MortazaSMartinezMCBaron-MenguyCDetrimental hemodynamic and inflammatory effects of microparticles originating from septic ratsCrit Care Med20093762045205019384196
- OleksowiczLMrowiecZIsaacsRDutcherJPPuszkinEMorphologic and ultrastructural evidence of interleukin-6 induced platelet activationAm J Hematol199548292997531395
- OdaAMiyakawaYDrukerBJThrombopoietin primes human platelet aggregation induced by shear stress and by multiple agonistsBlood19968711466446708639835
- NomuraSNakamuraTConeJTandonNNKambayashiJCytometric analysis of high shear-induced platelet microparticles and effect of cytokines on microparticle generationCytometry200040317318110878559
- NomuraSInamiNKanazawaSIwasakaTFukuharaSElevation of platelet activation markers and chemokines during peripheral blood stem cell harvest with G-CSFStem Cells200422569670315342934
- LupiaEGoffiABoscoOMontrucchioGThrombopoietin as bio-marker and mediator of cardiovascular damage in critical diseasesMediators Inflamm2012201239089222577249
- MontrucchioGBrizziMFCalossoGMarengoSPegoraroLCamussiGEffects of recombinant human megakaryocyte growth and development factor on platelet activationBlood1996877276227688639892
- TibblesHENavaraCSHupkeMAVassilevAOUckunFMThrombopoietin induces p-selectin expression on platelets and subsequent platelet/leukocyte interactionsBiochem Biophys Res Commun2002292498799111944912
- LupiaEBoscoOBergeroneSThrombopoietin contributes to enhanced platelet activation in patients with unstable anginaJ Am Coll Cardiol200648112195220317161245
- ZakynthinosSGPapanikolaouSTheodoridisTSepsis severity is the major determinant of circulating thrombopoietin levels in septic patientsCrit Care Med20043241004101015071393
- LupiaEBoscoOMarianoFElevated thrombopoietin in plasma of burned patients without and with sepsis enhances platelet activationJ Thromb Haemost2009761000100819317837
- SegreEPigozziLLisonDMay thrombopoietin be a useful marker of sepsis severity assessment in patients with SIRS entering the emergency department?Clin Chem Lab Med201452101479148324887960
- YadavHKorDJPlatelets in the pathogenesis of acute respiratory distress syndromeAm J Physiol Lung Cell Mol Physiol20153099L915L92326320157
- KatzJNKolappaKPBeckerRCBeyond thrombosis: the versatile platelet in critical illnessChest2011139365866821362652
- CarvalhoACDemarinisSScottCFSilverLDSchmaierAHColmanRWActivation of the contact system of plasma proteolysis in the adult respiratory distress syndromeJ Lab Clin Med198811222702773397629
- SingbartlKLeyKLeukocyte recruitment and acute renal failureJ Mol Med20048229110114669001
- Tőkés-FüzesiMWothGErnyeyBMicroparticles and acute renal dysfunction in septic patientsJ Crit Care201328214114722951018
- Valerio-RojasJCJafferIJKorDJGajicOCartin-CebaROutcomes of severe sepsis and septic shock patients on chronic antiplatelet treatment: a historical cohort studyCrit Care Res Pract2013201378257323509620
- WangLLiHGuXWangZLiuSChenLEffect of Antiplatelet Therapy on Acute Respiratory Distress Syndrome and Mortality in Critically Ill Patients: A Meta-AnalysisPLoS One115e0154754