Abstract
Background:
The objectives of this review were to integrate the evidence of curative effects through aquatic exercise and assess the quality of studies based on a review of nonrandomized controlled trials (nRCTs).
Methods:
Study design was a systematic review of nonrandomized controlled trials. Trials were eligible if they were nonrandomized clinical trials. Studies included one treatment group in which aquatic exercise was applied. We searched the following databases from 2000 up to July 20, 2009: MEDLINE via PubMed, CINAHL, and Ichushi-Web.
Results:
Twenty-one trials met all inclusion criteria. Languages included were English (N = 9), Japanese (N = 11), and Korean (N = 1). Target diseases were knee and/or hip osteoarthritis, poliomyelitis, chronic kidney disease, discomforts of pregnancy, cardiovascular diseases, and rotator cuff tears. Many studies on nonspecific disease (healthy participants) were included. All studies reported significant effectiveness in at least one or more outcomes. However results of evaluations with the TREND and CLEAR-NPT checklists generally showed a remarkable lack of description in the studies. Furthermore, there was the problem of heterogeneity, and we were therefore not able to perform a meta-analysis.
Conclusion:
Because there was insufficient evidence on aquatic exercise due to poor methodological and reporting quality and heterogeneity of nRCTs, we were unable to offer any conclusions about the effects of this intervention. However, we were able to identify problems with current nRCTs of aquatic exercise, and propose a strategy of strengthening study quality, stressing the importance of study feasibility as a future research agenda objective.
Introduction
Over the years, aquatic exercise has been known as pool therapy, hydrotherapy, and sometimes in earlier literature, as balneotherapy.Citation1 Exercise in warm water, usually termed hydrotherapy or aquatic therapy, is a popular treatment with a pain relief effect for many patients with painful neurologic or musculoskeletal conditions.Citation2 The warmth and buoyancy of water may block nociception by acting on thermal receptors and mechanoreceptors, thus influencing spinal segmental mechanisms.Citation3,Citation4 In addition, the warmth may enhance blood flow, which is thought to help in dissipating algogenic chemicals, and it may facilitate muscle relaxation. The hydrostatic effect may also relieve pain by reducing peripheral edemaCitation5 and by dampening sympathetic nervous system activity.Citation6
Recent reports have demonstrated the effectiveness of comprehensive health education, including lifestyle education and exercise in combination with spa bathing, for male white-collar workers,Citation7 and middle-aged and elderly people.Citation8,Citation9
It is well known in research design that evidence grading is highest for a systematic review (SR) with meta-analysis of randomized controlled trials (RCTs). In “the recent review (summary)Citation10 of the SRs of RCTs”, it was reported that there were three SRsCitation1,Citation2,Citation11 that included meta-analyses of RCTs on aquatic exercise. Bartels et alCitation1 reported that aquatic exercise had some beneficial short-term effects for patients with hip and/or knee osteoarthritis. Hall et alCitation2 reported that aquatic exercise had a small post-treatment effect in relieving pain compared with no treatment for patients with neurologic and musculoskeletal diseases, but there were no differences in pain relieving effects between aquatic and land exercise. Pittler et alCitation11 suggested that spa exercise may be effective for treating patients with chronic low back pain. However, we did not find any SRs of RCTs in which physical (eg, cardiovascular fitness) or psychological (eg, depression) effects were the primary outcome measurements.
An RCT is initially very difficult to execute and contains etiological issues, while the design of a non-RCT (nRCT) is easy to implement compared with an RCT. Although many studies have reported the curative effects of locomotrium diseases through aquatic exercise, there have been no systematic reviews of the evidence based on nRCTs. The objective of this study was to integrate the evidence from nRCTs on the curative effects through aquatic exercise for various diseases, and to assess the quality of those trials.
Methods
Criteria for considering studies included in this study
Studies were eligible if they were nRCTs and included one treatment group in which curative aquatic exercise was applied. Any type of aquatic exercise for cure and not for sports (eg, swimming) was permitted. The use of medication, alternative therapies, or lifestyle changes was described, and had to have been comparable in the group studies. There was no restriction on language.
Search methods for identification of studies
We searched the following databases from 2000 up to July 20, 2009: MEDLINE via PubMed, CINAHL, Web of Science, and Ichushi-Web (in Japanese). The International Committee of Medical Journal Editors (ICMJE) recommended uniform requirements for manuscripts submitted to biomedical journals in 1993. We selected articles published on and after 2000 because it appeared that the ICMJE recommendation had been adopted by the relevant researchers and had strengthened the quality of reports.
All searches were performed by two specific searchers (hospital librarians) who were qualif ied in medical information handling, and who were sophisticated in clinical trial research.
Search strategies
The search strategies contained the following elements and terms for all databases:
I: Search “aquatic exercise” or “water exercise”
II: Search “water gymnastic” or “water aerobics” or “pool exercise” or “pool therapy” or “aerobic aquatics” or aquatics
III: Search “exercise therapy”[MeSH] and “water”[MeSH]
IV: Search “water-based exercise”[All Fields] or “water-based training”[All Fields] or “aquatic therapy”[All Fields] or “aquatic physical therapy”[All Fields] or “water training”[All Fields] or “water-gymnastics”[All Fields]
V: Search I or II or III or IV Limits: Publication Date from January 1, 2000 to 2009
VI: Search I or II or III or IV Limits: Publication Date from January 1, 2000 to 2009, Randomized Controlled Trial
VII: Search V not VI.
Only keywords about intervention were used for the searches. First, titles and abstracts of identified published articles were reviewed to determine the relevance of the articles. Next, references in relevant studies and identified nRCTs were screened.
2000 is the year the CONSORT Statement became available on the Internet. The CONSORT Statement was created in the mid-1990s for improving the quality of RCTs. Because of the impact of the Internet, the quality of RCTs has improved since 2000.
Reference checking, hand-searching and others
We did not check the references of included studies, perform any hand-searching, or contact any institutions, societies, or specialists known to have expertise in aquatic exercise, or authors of included studies to identify any additional published or unpublished data.
Selection of trials
To make the final selection of studies for the review, all criteria were applied independently by two authors (JK and NS) to the full text of articles that had passed the first eligibility screening (). Disagreements and uncertainties were resolved by discussion between the review authors.
Figure 1 Flowchart of trial process.
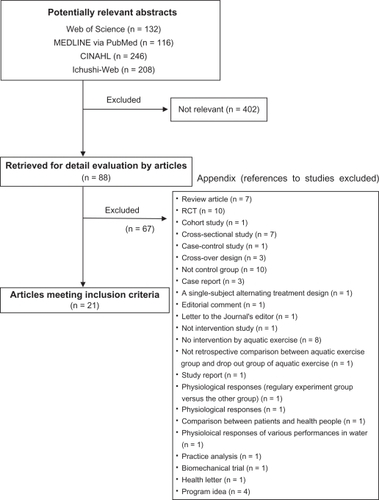
Studies were selected when 1) the design was an nRCT and 2) one of the interventions was a form of aquatic exercise. Curative effects were used as a primary outcome measure. Trials that were excluded are presented with reasons for exclusion (Appendix 1).
Quality assessment and summary of studies
To ensure that variation was not caused by systematic errors in the study design or execution, two review authors (MK and HK) independently assessed the quality of articles. A full quality appraisal of these papers was made using the TREND statement checklistCitation12 and CLEAR-NPT checklist,Citation13 developed to assess the methodological quality of nRCTs and nonpharmacological trials, respectively. Disagreements and uncertainties were resolved by discussion between the review authors.
For meta-analysis preparation, the target objects and main outcomes in each study were examined. We found that there were various kinds of target diseases in the studies reviewed: healthy young students, middle-aged or elderly people, or people with a certain disease. In addition, the studies were heterogeneous, and the main outcomes varied. Moreover, the quality of most studies was low according to the checklist results, and such low-quality studies were excluded from the analysis based on the Cochrane Review.Citation1 We could not perform a meta-analysis since no variable was eligible.
One review author (HK) selected the summary from each of the structured abstracts.
Benefit, harm, and withdrawals
The GRADE Working GroupCitation14 reported that the balance between benefit and harm, quality of evidence, applicability, and the certainty of the baseline risk were all considered in judgments about the strength of recommendations. Adverse events, withdrawals, and the cost for intervention were especially important information for researchers and users of clinical practice guidelines, and we presented this information with the description of each article.
Results
Study characteristics
The literature searches included 402 potentially relevant articles (). Abstracts from those articles were assessed and 88 papers were retrieved for further evaluation (checks for relevant literature). Sixty-seven publications were excluded because they did not meet the eligibility criteria (see Appendix 1). Twenty-one trialsCitation15–Citation35 met all inclusion criteria (). The languages of the eligible publications were English (N = 9), Japanese (N = 11), and Korean (N = 1). Target diseases were knee and/or hip osteoarthritis,Citation19,Citation24,Citation28 poliomyelitis,Citation15 chronic kidney disease,Citation21 discomforts of pregnancy,Citation30 cardiovascular diseases,Citation33 and rotator cuff tears.Citation35 Many studiesCitation16–Citation18,Citation20–Citation23,Citation25–Citation27,Citation29,Citation31,Citation32,Citation34 on nonspecific disease (healthy participants) were included (). All studies reported significant effectiveness in one or more outcomes. In particular, many studies reported that aquatic exercise had a significant effect on pain relief and outcome measurements for locomotor diseases.Citation15,Citation19,Citation24,Citation28,Citation35 These intervention periods ranged from 2 weeks to 12 months. These reflected the difficulty of maintaining long-term participation in each intervention trial. Whatever the case, the long-term effects are not clear.
Table 1 Summary of articles based on structured abstracts
Table 2 Brief summary of 21 articles
Withdrawals and adverse events
Withdrawals (dropouts) were reported in five studies,Citation24,Citation28,Citation29,Citation32,Citation34 and adverse events were reported in four studies (). There were three studiesCitation15,Citation19,Citation35 that reported ‘nothing’ on adverse events, and one studyCitation28 reported a slipping accident on the poolside (details of the injury were unclear). Other studies did not provide information on withdrawals or adverse events.
Intervention costs
A description of intervention costs was included in only one trial,Citation30 but the summary of that trial did not describe the costs ().
Quality assessment
We evaluated 21 items from the TREND checklist in more detail (). This assessment evaluated the quality of how the main findings of the study were summarized in the written report. A lack of description was noteworthy for the studies in general. The items for which the description rate was less than 30% were as follows: “information on how units were allocated to interventions (23.8%)”; “how sample size was determined and, when applicable, explanation of any interim analyses and stopping rules (23.8%)”; “method used to assign units to study conditions, including details of any restriction (19.0%)”; “inclusion of aspects employed to help minimize potential bias induced due to non-randomization (4.8%)”; “whether or not participants, those administering the interventions, and those assessing the outcomes were blinded to study condition assignment; if so, statement regarding how the blinding was accomplished and how it was assessed (14.3%)”; “if the unit of analysis differs from the unit of assignment, the analytical method used to account for this (9.5%)”; “statistical methods used for additional analyses, such as subgroup analyses and adjusted analysis (9.5%)”; “methods for imputing missing data, if used (14.3%)”; “flow of participants through each stage of the study: enrollment, assignment, allocation and intervention exposure, follow-up, analysis (19.0%)”; “dates defining the periods of recruitment and follow-up (14.3%)”; “baseline comparisons of those lost to follow-up and those retained, overall and by study condition (9.5%)”; “comparison between study population at baseline and target population of interest (4.8%)”; “indication of whether the analysis strategy was ‘intention to treat’ or, if not, description of how noncompliers were treated in the analyses (9.5%)”; “for each primary and secondary outcome, a summary of results for each study condition, and the estimated effect (9.5%)”; “inclusion of results from testing prespecified causal pathways through which the intervention was intended to operate, if any (14.3%)”; “summary of other analyses performed, including subgroup or restricted analyses, indicating which are prespecified or exploratory (4.8%)”; and “summary of all important adverse events or unintended effects in each study condition (19.0%)”.
Table 3 Evaluation of the quality of nonrandomized controlled trials by using the TREND checklist
presents an assessment of the evaluation of study quality by use of the CLEAR-NPT checklist. This tool mainly evaluated the quality of the study conduct. The description rate for the details of the intervention was high (81%), but the rate was low in other primary items. The primary items for which the executive rate was less than 30% were as follows: “Were participants adequately blinded? (4.8%)”; “Were care providers or persons adequately blinded? (4.8%)”; “Were outcome assessors adequately blinded to assess the primary outcomes? (9.5%)”; and “Were the main outcomes analyzed according to the intention-to-treat principle? (14.3%)”.
Table 4 Evaluation of the quality of nonrandomized controlled trials by using the CLEAR-NPT checklist
Discussion
Overall evidence and quality assessment
There were only 21 nRCTs about aquatic exercise published from 2000 to July 20, 2009, possibly due to the increase in studies with an RCT design. In previous SRsCitation1–Citation3 of RCTs, the authors actually collected many articles that were published in 2000. Pooling of the data from nRCTs was not performed because of the heterogeneity of the studies, multiple outcome measurements, and overall poor presentation. We used the TREND and CLEAR-NPT checklists as quality assessments. There were serious problems with the conduct and reporting of the target articles. Our summaries detected omissions of description and nonfulfillments, including detailed information on participants, sample size, assessors, care (health care) providers, blinding, and analysis methods. Furthermore, the description of adverse events and withdrawals were generally insufficient. In the Cochrane Review,Citation1 there are strict eligibility criteria for a meta-analysis, and for each article, heterogeneity and low quality of reporting must first be excluded. Because there was insufficient evidence in studies of aquatic exercise, due to poor methodological and reporting quality and heterogeneity, we are unable to offer any conclusions about the effects of aquatic exercise based on an SR.
Characteristics of articles
The relevant articles represented several studies of locomotorium diseases (N = 4), compared with few studies of respiratory, circulatory, and psychiatric diseases. This characteristic was apparent in the review articleCitation10 of SRs of RCTs. In that review, there were many articles (N = 15) that targeted the health enhancement effect instead of a specific disease, the primary and/or secondary outcome measurements and target participants varied, and a consistent trend was not detected.
We were interested in comparing not only nonintervention as the control, but also land exercise. There were five reports that defined land exercise as the control group, knee osteoarthritisCitation19,Citation28 and rotater cuff tearsCitation35 as the target disease; the remaining reportsCitation22,Citation31 were about healthy people. Two studies of knee osteoarthritis did not describe intervention effects. The recent meta-analysisCitation2 of RCTs showed no differences between aquatic exercise and land exercise for the pain-relieving effects on neurologic or musculoskeletal disease (P = 0.56; weighted standardized mean difference (SMD), 0.11; 95% confidence interval [CI]: −0.27–0.50; N = 103). Presently, we can not suggest that aquatic exercise is more effective than land exercise for pain relief in locomotorium diseases.
Future research agenda
There were no studies to clarify the effects on serum lipids, body composition, or blood pressure as the main outcome for patients with metabolic syndrome (MS). A joint scientific statementCitation36 about MS was issued recently, and many studies based on those criteria or outcomes should be started soon. Studies of aquatic exercise using prevention or cure as the outcome are also expected.
shows the future research agenda for aquatic exercise. In advanced nations and areas, it appears that there is interest in studies about mental health as well as MS. Researchers should use the respective checklists for research design and intervention method, which would lead to improvement in the quality of the study, and contribute to the accumulation of evidence. Suitable comparisons are necessary to explain why aquatic exercise is better than other types of dynamic exercise. Aquatic exercise needs a valuable resource (hot water pool), which can not be overlooked in the study feasibility. A recent studyCitation37 suggested that public health is moving toward the goal of implementing evidence-based interventions, but the feasibility of possible interventions and determining whether comprehensive and multilevel evaluations should be justified to accomplish it.
Table 5 Future research agenda on aquatic exercise intervention
Study limitations
This study was based on the PRISMA statement,Citation38 except for the meta-analysis. However, there were several limitations to the study. Some selection criteria were common to the studies, as described above; however, bias remained due to differences in eligibility for participation in each study. Publication bias was also a limitation. Since we did not limit our search to English, we found 11 articles (52%) published in Japanese. Furthermore, we did not check the references of hand-searches and did not contact institutions, societies, specialists known to have expertise in aquatic exercise, and authors of included studies to identify any additional published or unpublished data.
In terms of quality assessment, disagreements and uncertainties were resolved by discussion between two authors; discussions with a third expert and contact with authors for the purpose of clarification were not allowed.
Conclusion
Because there was insufficient evidence on aquatic exercise due to poor methodological and reporting quality, and heterogeneity of nRCTs, we were unable to offer any conclusions about the effects of this type of intervention. However, we were able to identify the problems with current nRCTs of aquatic exercise, and propose a strategy of strengthening study quality and stressing the importance of study feasibility as a future research agenda objective.
Acknowledgements
This study was supported by the Health and Labour Sciences Research Grants (Research on Health Security Control: ID No. H20-007) from the Japanese Ministry of Health, Labour and Welfare in 2009. We would like to express our appreciation to Ms Rie Higashino, Ms Mari Makishi, and Ms Yukiko Yamada for their assistance in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
- BartelsEMLundHHagenKBDagfinrudHChristensenRDanneskiold-SamsoeBAquatic exercise for the treatment of knee and hip osteoarthritisCochrane Database Syst Rev20074CD00552317943863
- HallJSwinkelsABriddonJMcCabeCSDoes aquatic exercise relieve pain in adults with neurologic or musculoskeletal disease? A systematic review and meta-analysis of randomized controlled trialsArch Phys Med Rehabil20088987388318452734
- BenderTKaraglleZBalintGPGutenbrunnerCBalintPVSukenikSHydrotherapy, balneotherapy, and spa treatment in pain managementRheumatol Int20052522022415257412
- YamazakiFEndoYToriiSSagawaSShirakiKContinuous monitoring of change in hemodilution during water immersion in humans: effect of water temperatureAviat Space Environ Med20007163263910870823
- GabrielsenAVidebaekRJohansenLBForearm vascular and neuroendocrine responses to graded water immersion in humansActa Physio Scand20001698794
- FamAGSpa treatment in arthritis: a rheumarologist’s viewJ Rheumatol199118177517771795308
- KamiokaHNakamuraYOkadaSEffectiveness of comprehensive health education combining lifestyle education and hot spa bathing for male white-collar employees: a randomized controlled trial with 1-year follow-upJ Epidemiol20091921923019687610
- KamiokaHNakamuraYYazakiTEffectiveness of comprehensive health education combining hot spa bathing and lifestyle education in middle-aged and elderly women: one-year follow-up on randomized controlled trial of three- and six-month interventionsJ Epidemiol200616354416369107
- KamiokaHOhshiroHMutohYEffect of long-term comprehensive health education on the elderly in a Japanese village: Unnan cohort studyInt J Sports Health Sci200866065
- KamiokaHTsutaniKOkuizumiHEffectiveness of aquatic exercise and balneotherapy: a summary of systematic reviews based on randomized controlled trials of water immersion therapiesJ Epidemiol20102021219881230
- PittlerMHKaragülleMZKaragülleMErnstESpa therapy and balneotherapy for treating low back pain: meta-analysis of randomized trialsRheumatol200645880884
- JarlaisDCLylesCCrepazNfor the TREND groupImproving the reporting quality of nonrandomized evaluations of behavioral and public health interventionsAm J Public Health20049436136614998794
- BoutronIMoherDTugwellPA checklist to evaluate a report of a nonpharmacological trial (CLEAR NPT) was developed using consensusJ Clin Epidemiol2005581233124016291467
- AtkinsDBestDBrissPAGrading quality of evidence and strength of recommendationsBMJ20043281490149715205295
- WillénCSunnerhagenKSGrimbyGDynamic water exercise in individuals with late poliomyelitisArch Phys Med Rehabil200182667211239288
- EbisuTKobayashiMKatsukiTYanagimotoYEffectiveness of serum lipids on spa-walking [in Japanese]Health Care200143981984
- AobaTMatsumotoTSuganoANomuraTThe effects of enforcement water exercise class on hypotensive to blood pressure at elderly subjects [in Japanese with English abstract]Ann Reports Health Phys Educ Sports Sci20012099104
- YamadaTWatanabeEOkadaATakeshimaNEffects of water-based well-rounded exercise on vital age and physical fitness in older adults [in Japanese with English abstract]Jpn Soc Phys Anthropol200278793
- MuraiETakedaYImayaTUchiyamaENakazonoKNakajimaHExercise therapy for osteoarthritis of the knee -preliminarily study of water exercise [in Japanese with English abstract]J Jpn Soc Clin Sports Med2002105460
- IgarashiYKondoTYamaokaKHealth effect of aquatic exercise therapy using a hot spring [in Japanese]Sick Body Phys2002361114
- PechterÜOtsMMesikeppSBeneficial effects of water-based exercise in patients with chronic kidney diseaseInt J Rehabil Res20032615315612799612
- DourisPSouthardVVargaCSchaussWGennaroCReissAThe effect of land and aquatic exercise on balance scores in older adulesJ Geriatr Phys Ther20032636
- LiquoriAWidenerGClarkLEffects of a 6-week prenatal water exercise program on physiological parameters and well-being in women with pregnancies in the 2nd–3rd trimesters: a pilot studyJ Section Women’s Health2003271119
- LinSY-CDaveyRCCochraneTCommunity rehabilitation for older adults with osteoarthritis of the lower limb: a controlled clinical trialClin Rehabil2004189210114763724
- AkamineTYamanakaTTaguchiNEffects of underwater exercise with hot spring bathing on middle aged people [in Japanese with English abstract]Kyushu Yamaguchi Sports Sci J200517712
- TakumiYMoriyaKOdaSAdikariMOFukuokaEParticipation in an aquatic exercise class twice a week for 12 weeks improved physical fitness for good walking, walking self-efficacy on winter roads, mental health and QOL in elderly women [in Japanese with English abstract]Jpn J Biometeor2005421727
- TakumiYMoriyaKParticipation in an aquatic walking class for 12 weeks improved physical fitness for good walking, emotion and walking self-efficacy on winter roads in middle-aged and elderly women [in Japanese with English abstract]Jpn J Biometeor200542515
- LeeHYComparison of effects among Tai-chi exercise, aquatic exercise, and a self-help program for patients with knee osteoarthritis [in Korean with English abstract]J Korean Acad Nurs200636571580
- LordSRMattersBGeorgeRSThomasMBindonJChanDK-YThe effects of water exercise on physical functioning in older peopleAustralasian J Ageing2006253641
- SmithSAMichelYA pilot study on the effects of aquatic exercises on discomforts of pregnancyJ Obstet Gynecol Neonatal Nurs200635315323
- ChishakiAMakayaMNagahiroCComparison of usefulness between water exercise and gymnastic exercise, Jikyojyutsu, in maintaining physical ability for the elderly [in Japanese with English abstract]Memoirs Dep Health Sci Sch Med Kyushu Univ200672332
- KawasakiTMurataniHOzoeNHigakiHKawasakiJThe effect of aquatic exercise on preventing falls and life-style related disease among middle-aged and elderly people [in Japanese]Jpn J Clin Exper Med200784402411
- NishikawaAUedaYWakayamaKHayashiYEffect of aquatic walking on the cardiovascular patients in our hospital and health-related QOL- in comparison with indoor exercise therapy [in Japanese]JJCR200813135138
- RotsteinAHarushMVaismanNThe effect of a water exercise program on bone density of postmenopausal womenJ Sports Med Phys Fitness20084835235918974722
- BradyBRedfernJMacdougalGWilliamsJThe addition of aquatic therapy to rehabilitation following surgical rotator cuff repair: a feasibility studyPhysiother Res Int20081315316118548557
- AlbertiKGMMEckelRHGrundySMHarmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation TaskForce on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of ObesityCirculation20091201640164519805654
- BowenDJKreuterMSpringBHow we design feasibility studiesAm J Prev Med20093645245719362699
- LiberatiAAltmanDGTetzlaffJThe PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaborationAnn Intern Med2009151W65W9419622512