
Abstract
Background
Coronary artery disease (CAD) is the most common cardiovascular disease (CVD). Coronary artery bypass graft (CABG) surgery is the most common treatment used for CAD. Patients undergoing this surgery are always anxious, which might increase complications in the postoperative period, especially prolongation of postoperative length of stay (LOS). It has been shown that perceived control (PC) moderated the relationship between anxiety and complications in a cardiac population, but its effect has not been studied in post-CABG.
Aim
The aim of this study was to check if there is a moderating effect for the PC on the relationship between anxiety and LOS post-CABG.
Patients and methods
A non-experimental, prospective, observational study was conducted with a consecutive sample of 250 patients who underwent elective CABG from four hospitals in Amman, Jordan. PC was measured by the Arabic version of the Control Attitude Scale-Revised (CAS-R), and anxiety was measured by the Arabic version of the anxiety subscale of Hospital Anxiety and Depression Scale. LOS and other needed information were obtained from patients’ medical records.
Results
Preoperative anxiety was significantly higher than postoperative anxiety (mean [SD]: 12.80 [6.70] vs 11.01 [6.74], P<0.001). Female patients were more anxious and had longer LOS compared to male patients. In stepwise regression, anxiety and PC scores were independent predictors for LOS. Every unit increase in preoperative anxiety increased LOS by 0.381 days, and every unit increase in PC decreased the postoperative LOS by 0.210 days. Moderating effect was checked by simple slope analysis for high (+1 SD) and low (−1 SD) levels of PC. Patients with high anxiety and low PC had the longest LOS, and patients with low anxiety and high PC had the shortest LOS, indicating the moderating effect of PC on the relationship between anxiety and LOS.
Conclusion
High levels of anxiety were associated with longer LOS after CABG. PC moderates this relationship. Enhancing PC in this population can improve outcomes and decrease LOS and morbidity.
Introduction
Coronary artery disease (CAD) is the most common cardiovascular disease (CVD). CAD accounts for more than half of all CVD eventsCitation1 and represents the most leading cause of mortality and morbidity in both developed and developing countries.Citation2 According to the WHO,Citation3 CAD is responsible for one-fifth of all deaths in Jordan (131 per 100,000).Citation3 Coronary artery bypass graft (CABG) is the most commonly used treatment approach for patients with CAD. It gives the benefit of reducing angina and enhances quality of life (QoL).Citation4,Citation5 Furthermore, it has been found that CABG is valuable in reducing the levels of anxiety and depression, especially in men.Citation6
Despite this, CABG surgery is a stressful and traumatic event and is known to be accompanied by negative psychological outcomes in the preoperative period which might extend postoperatively.Citation7,Citation8 Individuals may have high levels of anxiety when they are diagnosed with CAD,Citation9 especially in the pre-op period and when they are waiting for major surgery.Citation8,Citation10 Significantly higher levels of anxiety were reported before CABG, compared to levels after CABG.Citation11,Citation12 Factors that might increase anxiety in the preoperative period of CABG surgery are as follows: extreme chest pain and subsequent disability, fatigue, fear of death,Citation13 fear of outcomes of surgery because the heart is a vital organ, and expecting changes in lifestyle due to hospitalization.Citation7,Citation14 Most of these factors will decline gradually after a successful procedure, which causes a decline in the postoperative levels of anxiety. However, anxiety has its own negative consequences and manifestations on CABG patients.
Anxiety might be manifested as impaired functional status, chest pain, and shortness of breath.Citation15 Furthermore, increased anxiety is correlated with poorer QoL and worse long-term psychological outcomes.Citation16–Citation18 Persistent anxiety can adversely influence patients’ prognosis and physiologic parameters (pre- and intraoperatively or during anesthesia),Citation7,Citation14 which might prolong recovery and length of stay (LOS), and compromise QoL.Citation19–Citation21 This increased LOS can further impact patients’ psychological well-being, leading to increased levels of anxiety. Therefore, identifying high-risk populations for anxiety and diverse methods for controlling these negative effects of anxiety is necessary.
Diverse sociodemographic and clinical characteristics might affect the anxiety level, which include but are not limited to age, gender, marital status, history of hypertension, diabetes mellitus (DM), previous myocardial infarction, personality type, monthly income, social support, and perceived control (PC) level. It has been shown that female patients have higher levels of negative emotions (anxiety and depression) among cardiac populations.Citation21–Citation23 This phenomenon is consistent among cultures.Citation21–Citation23 However, there is a lack of information regarding this among patients undergoing CABG.
In the same line, PC is one of the methods that might reduce the effects of anxiety among patients scheduled for CABG surgery. PC is thought to be a personality characteristic that is defined as “an individual’s belief that he or she has the resources required to cope with negative events in a way that positively influences their adversive nature”.Citation24 In case of cardiac events such as acute myocardial infarction (AMI), adaptation, psychosocial recovery, and QoL can be determined by psychological rather than physiological factors.Citation24–Citation26
A number of researchers have demonstrated that lower levels of PC were associated with higher levels of anxiety and lower scores of QoL.Citation27–Citation29 Additionally, PC has been negatively correlated with anxiety in various clinical conditions of cardiac populations, including AMI, cardiac surgery, and heart failure.Citation29–Citation33 It also moderated the relationship between anxiety and complications after AMI,Citation33 and it was an independent predictor of anxiety in AMI, heart failure, and CAD populations.Citation24 However, the effect of PC on anxiety among CABG patients is not well studied.
To summarize, patients undergoing CABG have high levels of anxiety in the preoperative period that might lead to negative outcomes postoperatively, especially increasing the LOS in the hospital. Determining specific groups that have these high levels and interventions to decrease their effects on patients’ outcomes is necessary. There is a lack of studies that are specifically designed for such purpose. These studies are lacking nationwide and in developing countries particularly.
Therefore, the major purpose of this study was to check if there is a moderating effect of PC on the relationship between anxiety and LOS among patients undergoing CABG. In addition, the study was designed to check the following research hypotheses: 1) preoperative anxiety levels among patients undergoing CABG will be higher than the postoperative levels; 2) female patients will have higher levels of pre- and postoperative anxiety compared to male patients; 3) female patients will have longer postoperative LOS compared to male patients; 4) anxiety scores and PC scores will be independent predictors for postoperative LOS among CABG patients; and 5) PC scores will have a moderating effect on the relationship between anxiety and postoperative LOS among CABG patients.
Table 1 Clinical and sociodemographic characteristics (N=250)
Table 2 Stepwise regression analyses for predictors of postoperative hospital LOS (N=250)
Materials and methods
Design, sample, and setting
A descriptive, non-experimental, prospective, observational design was used to test research hypotheses of this study. A consecutive recruitment method was used. All patients who visited the cardiology outpatient clinics of four hospitals (one governmental, one teaching, and two private) in Amman, Jordan were screened for the following eligibility criteria: 1) age 18 years or more, 2) elective surgery, 3) free from any psychiatric disease, 4) not on anxiolytic medications, and 5) able to read and write Arabic. A total of 250 patients participated in this study ().
Figure 1 Flow diagram of the participants.
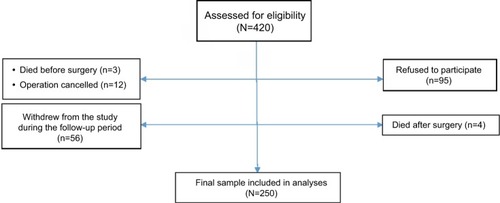
To account for multiple testing, sample size was determined based on the G*power calculator for multiple regression. The assumptions were medium effect size of 0.15, type I error of 0.01, and total number of predictors of 12. Based on these assumptions, the needed sample was 103. For this reason, the recruited patients were sufficient to account for multiple testing.
Procedure
A trained research assistant approached all participants who met the inclusion criteria at the cardiology clinic and explained the study in detail, with the benefits and risks. All participants’ queries were answered, and they were assured that participation is totally voluntary and they can withdraw at any time during the study. Participants who agreed to be enrolled signed an informed consent. Before surgery (mean ± SD: 36±14 hours), all participants who agreed to participate filled the Hospital Anxiety and Depression Scale (HADS) and a sociodemographic questionnaire on gender, age, marital status, monthly income, and working status. Participants answered HADS another time when they came for follow-up 1 month after surgery. All other needed information were collected from the medical records after discharge, including postoperative hospital LOS, history of DM, hypertension, previous myocardial infarction, previous angina, and body mass index (BMI; kg/m2).
Measurement of variables
Anxiety
Anxiety was measured by the Arabic version of the HADS-anxiety subscale at both time points. This version showed acceptable psychometric properties with a minimum Cronbach’s α of 0.78.Citation9,Citation34–Citation36 The sensitivity and specificity were 86% and 87%, respectively.Citation9,Citation34–Citation36 HADS is a self-reported questionnaire usually used in a clinical setting.Citation9,Citation21 This subscale has seven items, with a range of 0–3 for each time. The total score for the seven items ranges from 0 to 21, with higher scores indicating higher frequency and severity of symptoms. Total scores are usually classified as follows: 0–7, normal; 8–10, mild; and 11–21, moderate to severe.Citation9,Citation21
PC
The Arabic version of the Control Attitude Scale-Revised (CAS-R) was used to measure PC in this study. This instrument is valid and reliable and has been used in cardiac populations in previous studies.Citation9 The Cronbach’s α for the Arabic version was 0.75.Citation9 CAS-R consists of eight Likert scale items with five-option answers from 1 “totally disagree” to 5 “totally agree”. Total score ranges from 8 to 40, with higher scores indicating higher levels of PC.Citation9 The researchers usually use the median as the cutoff point, since there are no published mean norms.Citation9,Citation24,Citation37
LOS
The LOS was taken from the medical records after discharge and was reported in days.
Ethical consideration
The institutional review board committee at Applied Science Private University, Amman, Jordan reviewed and approved the study protocol after a detailed presentation by the principal investigator. All patients who met the inclusion criteria and agreed to participate signed an informed consent prior to data collection. All data were kept in a locked cabinet with access only by the principle investigator, and aggregate data were used for publication purposes.
Data analyses
SPSS version 21 was used to analyze the data. The value of α <0.05 was set a priori. To control for the effects of covariates, the associations between preoperative anxiety and these covariates were tested by Pearson correlation for continuous variables and independent t-test or ANOVA for categorical variables. All significant associations were controlled in the subsequent regression analysis. There were no differences between those who continued the study and those who dropped out during the study period in regard to sociodemographic and clinical characteristics.
To test the research hypothesis 1, preoperative anxiety levels among patients undergoing CABG will be higher than those of patients postoperatively, paired t-test was used. To test the research hypothesis 2, female patients will have higher levels of pre- and postoperative anxiety compared to male patients, independent t-test was used.
To test the research hypotheses 3–5 (female patients will have longer postoperative LOS compared to male patients; anxiety scores and PC scores will be independent predictors for postoperative LOS among CABG patients; and PC scores will have a moderating effect on the relationship between anxiety and postoperative LOS among CABG patients), stepwise multiple regression analyses were performed, followed by simple slope analysis. In the first step, age, gender, marital status, monthly income, history of hypertension, DM, previous myocardial infarction, previous angina, BMI, preoperative anxiety scores, and PC scores were entered as independent variables. In the second step, the interaction between centerized PC and anxiety was included. As further support for the moderating effect, we tested the combined association between LOS (dependent variable) and preoperative anxiety and PC (two independent variables) by dividing the sample using the standard HADS cutoff of ≤7 as low and ≥8 as high, and a median split of PC of 30. We used these binary variables to create four categories of participants: low anxiety/high PC, low anxiety/low PC, high anxiety/high PC, and high anxiety/low PC. Then, we compared the LOS among the four groups using ANOVA with post hoc analysis.
Results
Clinical and sociodemographic characteristics
Two hundred and fifty patients (175 males and 75 females) participated in the study. The mean age was ~70 years, and 60.4% were married. More than three-quarters of the sample were not working and had previous angina. Postoperative hospital LOS has a mean of 11.88±10.37 days. Preoperatively, more than half of the sample had moderate to severe anxiety. All other clinical and sociodemographic characteristics are presented in .
Research hypothesis 1: preoperative anxiety levels among patients undergoing CABG will be higher than the postoperative levels. Paired t-test showed that preoperative anxiety was significantly higher than postoperative anxiety (mean [wSD]: 12.80 [6.70] vs 11.01 [6.74], P<0.001). Research hypothesis 2: female patients will have higher levels of pre- and postoperative anxiety compared to male patients. Independent t-test showed pre- and postoperative anxiety levels for female patients were higher than those for male patients: preoperative (mean [SD]: 16.63 [6.25] vs 11.67 [6.42], P<0.001), postoperative (mean [SD]: 13.02 [7.25] vs 10.42 [6.48], P<0.05). Research hypotheses 3–5: female patients will have longer postoperative LOS compared to male patients; anxiety scores and PC scores will be independent predictors for postoperative LOS among CABG patients; and PC scores will have a moderating effect on the relationship between anxiety and postoperative LOS among CABG patients. The results of the regression analyses are presented in . In both models, female gender, PC, and anxiety were the independent predictors of LOS. Being a female patient increased the LOS by 0.154 days. Every one unit increase in anxiety was associated with 0.381 days increase in the LOS. Finally, every one unit increase in PC decreased the LOS by 0.210 days.
The R2 change between Model 1 and Model 2 was significant (ΔR2=0.07, P<0.01). The interaction term in Model 2 was significant, which indicated that PC was a significant moderator in the relationship between anxiety and LOS. To further investigate the nature of this moderation, a simple slope analysis was performed separately for PC at ±1 SD from the mean. Briefly, slope analysis means to check the effect of independent variable, which is anxiety in this study, on the dependent variable (LOS), when the moderator (PC) is high and low. These analyses revealed that, in those with a PC score of 1 SD below the average (low moderator), there was a significant relationship between anxiety and LOC (simple slope =0.378, t=6.65, P<0.001), indicating that anxiety increased the LOS. On the other hand, in those with a PC score of 1 SD above the average, the relationship between anxiety and LOS was not significant, indicating that higher levels of PC have a protective effect against the relationship between anxiety and LOS.
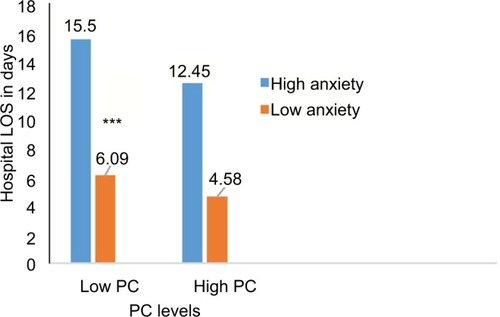
For further clarification purposes, comparisons were made among the four groups of PC and anxiety levels (low anxiety/high PC, low anxiety/low PC, high anxiety/high PC, and high anxiety/low PC). The results are demonstrated in .
Figure 2 Comparison of LOS based on anxiety and PC.
Abbreviations: LOS, length of stay; PC, perceived control.
Discussion
To our knowledge, this is the first study which was specifically designed to check the moderating effect of PC on LOS post-CABG in a developing country. Moreover, this study aimed to check if preoperative anxiety was higher than postoperative anxiety and if females undergoing CABG were more anxious than male patients. This study also checked if preoperative anxiety and PC were independent predictors of LOS.
The current study revealed that preoperative anxiety was higher than postoperative anxiety among CABG patients, indicating that when CABG surgery was completed, the anxiety levels were reduced. This finding supports the results of previous studies.Citation8,Citation38,Citation39 As reported in previous studies, most patients undergoing CABG surgery experienced increased anxiety before the surgery. The patients who had higher anxiety scores in the preoperative period were often expected to remain anxious throughout their hospital stay and recovery. Therefore, it is necessary to do interventions and conduct assessment of anxiety level of the patients undergoing CABG surgery.Citation8,Citation39 A previous study conducted at Flinders Medical Center in South Australia reported that preoperative anxiety is a predictor and reason for increased duration of anxiety postoperatively, in addition to adverse outcomes.Citation8 This result is consistent with our study which showed that anxiety was an independent predictor for longer LOS among CABG patients.
In our study, pre- and postoperative anxiety levels of female patients were higher than those of male patients. In previous studies about anxiety in different cardiac populations including CABG, CAD, and AMI, female patients demonstrated higher levels of anxiety compared to male patients.Citation21–Citation23,Citation39–Citation41 Females usually try to express their anxiety and feeling more often than males, particularly in cultures such as of Jordan and Arabic countries, because they try to help patients, specifically women.Citation21 Moreover, this was consistent with published studiesCitation39–Citation41 which found that women were more vulnerable to anxiety than men and justified that the load of home responsibilities may increase the anxiety levels among them. On the contrary, a study conducted in Ethiopia stated that there was no difference between the anxiety level based on gender among CABG patients.Citation42 Further studies exploring the reasons why women representing different cultures are at a higher risk for anxiety before and after CABG than men are still recommended.
The findings of this study showed that the postoperative LOS for female patients was higher than that for male patients, which can be justified by our previous finding which revealed that pre- and postoperative levels of anxiety were higher among female than male patients. A previous studyCitation43 related the increased LOS among CABG female patients to many factors such as differing autonomic responses to acute coronary occlusion, age, having chronic disease, weight, BMI, biases in health care providing ways, biologic differences, women’s opioid sensitivity that induced respiratory depression after cardiopulmonary bypass, and women being likely to experience more emboli during CABG or more brain edema after CABG surgery or become more susceptible to postoperative complications. To the authors’ knowledge, limited studies have investigated the link between anxiety level, gender, and LOS, which appeal the importance of the current study findings.
Our findings show that anxiety scores and PC scores are independent predictors for postoperative LOS. Moreover, PC moderated the relationship between anxiety and LOS. Among patients with cardiac disease, PC plays a vital role in determining adaptation. Level of PC is independently predictive of psychosocial recovery and plays a more prominent role than physical predictors in determining psychosocial recovery.Citation25 Higher levels of PC were associated with lower levels of anxiety and depression in a variety of cardiac populations and their families.Citation29,Citation30,Citation32 PC moderated the negative impact of anxiety on in-hospital complications such as recurrent ischemia, re-infarction, and malignant dysrhythmias after AMI.Citation9,Citation33 To the authors’ knowledge, limited studies have investigated the direct link among anxiety level, PC, and LOS, which increases the necessity of conducting further studies about this topic.
Conclusion and implications for practice
Assessing the anxiety level for patients undergoing CABG and evaluating their PC are important for nurses because this will help them to prioritize and develop appropriate and effective nursing interventions and care plan. Based on our findings, enhancing PC before CABG might decrease the anxiety levels before and after surgery and consequently decrease LOS. Routine assessment of patients’ anxiety levels before surgery is recommended to determine which patients are at risk for increased anxiety after surgery. Routine assessment also means that resources can be focused on specific groups of patients who experience high levels of anxiety, considering the vulnerable groups (ie, females).
Future research
Future research should focus on interventions that target anxious patients undergoing CABG surgery. Further randomized control trials about patients’ PC, anxiety level, and their influence on LOS indicator are recommended.
Disclosure
The authors report no conflicts of interest in this work.
References
- BenjaminEJBlahaMJChiuveSEAmerican Heart Association Statistics Committee and Stroke Statistics SubcommitteeHeart disease and stroke statistics-2017 update: a report from the American Heart AssociationCirculation201713510e146e60328122885
- SekhriTKanwarRSWilfredRPrevalence of risk factors for coronary artery disease in an urban Indian populationBMJ Open2014412e005346
- Country Statistics and Global Health Estimates by WHO and UN Partner: WHO Statistical Profile2015 Available from:https://www.who.int/gho/countries/npl.pdfAccessed March 01, 2018
- McKenzieLHSimpsonJStewartMA systematic review of preoperative predictors of post-operative depression and anxiety in individuals who have undergone coronary artery bypass graft surgeryPsychol Health Med2010151749320391226
- SerruysPWMoriceMCKappeteinAPSYNTAX InvestigatorsPer-cutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery diseaseN Engl J Med20093601096197219228612
- NematiMHAstanehBThe impact of coronary artery bypass graft surgery on depression and anxietyJ Cardiovasc Med (Hagerstown)201112640140421200327
- YilmazMSezerHGürlerHBekarMPredictors of preoperative anxiety in surgical inpatientsJ Clin Nurs2012217–895696421812848
- TullyPJBakerRADepression, anxiety, and cardiac morbidity outcomes after coronary artery bypass surgery: a contemporary and practical reviewJ Geriatr Cardiol20129219720822916068
- AbuRuzMEPerceived control moderates the relationship between anxiety and in-hospital complications after ST segment elevation myocardial infarctionJ Multidiscip Healthc20181135936530100731
- NemeroffCPrevalence of depression and anxiety in CABG patientsJ Watch Psychiatry2003181219
- AmouzeshiAHosseiniSJavadiADepression and associated factors in patients undergoing coronary artery bypass grafting in Imam Reza hospital of Mashhad in 2013J Surg Trauma201533–45156
- GuoPEastLArthurAA preoperative education intervention to reduce anxiety and improve recovery among Chinese cardiac patients: a randomized controlled trialInt J Nurs Stud201249212913721943828
- Bagheri-NesamiMShorofiSAZargarNSohrabiMGholipour-BaradariAKhalilianAThe effects of foot reflexology massage on anxiety in patients following coronary artery bypass graft surgery: a randomized controlled trialComplement Ther Clin Pract2014201424724439644
- GoebelSKaupLMehdornHMMeasuring preoperative anxiety in patients with intracranial tumors: the Amsterdam preoperative anxiety and information scaleJ Neurosurg Anesthesiol201123429730321691216
- LozanoRNaghaviMForemanKGlobal and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010Lancet201238098592095212823245604
- SutherlandGAndersenMBMorrisTRelaxation and health-related quality of life in multiple sclerosis: the example of autogenic trainingJ Behav Med200528324925616015459
- BoudrezHDe BackerGPsychological status and the role of coping style after coronary artery bypass graft surgery: results of a prospective studyQual Life Res2001101374711508474
- GallagherRMcKinleySDracupKEffects of a telephone counseling intervention on psychosocial adjustment in women following a cardiac eventHeart Lung2003322798712734530
- MiddelBEl BazNPedersenSSvan DijkJPWyniaKReijneveldSADecline in health-related quality of life 6 months after coronary artery bypass graft surgery: the influence of anxiety, depression, and personality traitsJ Cardiovasc Nurs201429654455424165701
- Abu RuzMELennieTAMoserDKEffects of β-blockers and anxiety on complication rates after acute myocardial infarctionAm J Crit Care20112016773 quiz 7420107234
- AbuRuzMEMasa’DehRGender differences in anxiety and complications early after acute myocardial infarctionJ Cardiovasc Nurs201732653854328591003
- De JongMJChungMLRoserLPA five-country comparison of anxiety early after acute myocardial infarctionEur J Cardiovasc Nurs20043212913415234317
- SerpytisPNavickasPLukaviciuteLGender-based differences in anxiety and depression following acute myocardial infarctionArq Bras Cardiol2018111567668330156607
- MoserDKRiegelBMcKinleySThe Control Attitudes Scale-Revised: psychometric evaluation in three groups of patients with cardiac illnessNurs Res2009581425119092554
- MoserDKDracupKPsychosocial recovery from a cardiac event: the influence of perceived controlHeart Lung19952442732807591794
- HeoSMoserDKRiegelBHallLAChristmanNTesting a published model of health-related quality of life in heart failureJ Card Fail200511537237915948088
- BallashNGPembleMKUsuiWMBuckleyAFWoodruff-BordenJFamily functioning, perceived control, and anxiety: a mediational modelJ Anxiety Disord200620448649716005603
- DonovanHSHartenbachEMMethodMWPatient–provider communication and perceived control for women experiencing multiple symptoms associated with ovarian cancerGynecol Oncol200599240441116112174
- EvangelistaLSMoserDDracupKDoeringLKobashigawaJFunctional status and perceived control influence quality of life in female heart transplant recipientsJ Heart Lung Transplant200423336036715019646
- DracupKWestlakeCEricksonVSMoserDKCaldwellMLHamiltonMAPerceived control reduces emotional stress in patients with heart failureJ Heart Lung Transplant2003221909312531418
- MoserDKDracupKImpact of cardiopulmonary resuscitation training on perceived control in spouses of recovering cardiac patientsRes Nurs Health200023427027810940952
- MoserDKDracupKRole of spousal anxiety and depression in patients’ psychosocial recovery after a cardiac eventPsychosom Med200466452753215272098
- MoserDKRiegelBMcKinleySDoeringLVAnKSheahanSImpact of anxiety and perceived control on in-hospital complications after acute myocardial infarctionPsychosom Med2007691101617244843
- el-RufaieOEAbsoodGValidity study of the hospital anxiety and depression scale among a group of Saudi patientsBr J Psychiatry1987151056876883446314
- el-RufaieOEAlbarAAAl-DabalBKIdentifying anxiety and depressive disorders among primary care patients: a pilot studyActa Psychiatr Scand19887732802823394530
- el-RufaieOEAbsoodGHRetesting the validity of the Arabic version of the Hospital Anxiety and Depression (HAD) scale in primary health careSoc Psychiatry Psychiatr Epidemiol199530126317892615
- McKinleySFienMRiegelBComplications after acute coronary syndrome are reduced by perceived control of cardiac illnessJ Adv Nurs201268102320233022235775
- DuitsAADuivenvoordenHJBoekeSThe course of anxiety and depression in patients undergoing coronary artery bypass graft surgeryJ Psychosom Res19984521271389753385
- GallagherRMcKinleySStressors and anxiety in patients undergoing coronary artery bypass surgeryAm J Crit Care200716324825717460316
- KingKBEmotional and functional outcomes in women with coronary heart diseaseJ Cardiovasc Nurs2001153547012968771
- RameshCNayakBSPaiVBGeorgeAGeorgeLSDeviESPreoperative anxiety in patients undergoing coronary artery bypass graft surgery – a cross-sectional studyInt J Afr Nurs Sci201773136
- NigussieSBelachewTWolanchoWPredictors of preoperative anxiety among surgical patients in Jimma University specialized teaching hospital, south western EthiopiaBMC Surg20141416725189274
- ButterworthJJamesRPrielippRCereseJLivingstonJBurnettDFemale gender associates with increased duration of intubation and length of stay after coronary artery surgery. CABG clinical benchmarking database participantsAnesthesiology200092241442410691228