Abstract
Background:
Platelet-derived microparticles (PDMP), selectins, and adiponectin play an important role in the development of atherosclerosis in diabetes. Miglitol has been shown to have a beneficial effect on postprandial hyperglycemia in diabetic patients. However, its influence on platelet activation markers (PDMP and soluble CD40 ligand [sCD40L]), selectins, and adiponectin in these patients is poorly understood.
Aim:
We investigated the effect of miglitol on circulating levels of PDMP, sCD40L, selectins, and adiponectin in patients with type 2 diabetes.
Methods:
Miglitol (150 mg/day) was administered for 4 months. Levels of PDMP, sCD40L, soluble P-selectin (sP-selectin), soluble E-selectin (sE-selectin), soluble L-selectin (sL-selectin), and adiponectin were measured by enzyme-linked immunosorbent assay at baseline, and after 1 and 4 months of treatment.
Results:
The levels of PDMP, sCD40L, sP-selectin, sE-selectin, and sL-selectin were higher in diabetic patients than in hypertensive patients, while there were no significant differences between hypertensive and hyperlipidemic patients. Before miglitol treatment, the adiponectin level of diabetic patients was lower than that of hypertensive patients. Miglitol therapy significantly decreased the plasma PDMP and sCD40L levels relative to baseline. Miglitol also caused a significant decrease of sP-selectin, sE-selectin, and sL-selectin. On the other hand, miglitol therapy led to a significant increase in adiponectin after 4 months of administration compared with baseline. Furthermore, the reduction of platelet activation markers and selectins during miglitol therapy was significantly greater in the responder (adiponectin-improved) group than the nonresponder group of diabetic patients.
Conclusion:
Miglitol has an adiponectin-dependent anti-atherothrombotic effect that may be beneficial for primary prevention of atherothrombosis in patients with type 2 diabetes.
Introduction
Diabetic patients develop hypercoagulability and platelet hyperaggregability,Citation1,Citation2 along with increased levels of platelet activation markers such as platelet-derived microparticles (PDMP).Citation3 Expression of cell adhesion molecules is also increased in diabetes,Citation4 and these molecules have been suggested to have a role in the microvascular complication of this disease. P-selectin is an adhesion molecule that is involved in adhesion of platelets to leukocytes or the endothelium.Citation5 Serum levels of soluble P-selectin (sP-selectin) are elevated in patients with diabetes.Citation6,Citation7 The first step in the process of leukocyte migration into the subendothelial space is the adhesion of circulating leukocytes to the endothelium, which may involve adhesion molecules like L-selectin and can eventually lead to vascular complications.
A large volume of epidemiological data indicates that persons with postprandial hyperglycemia have an increased risk of cardiovascular disease.Citation8,Citation9 Patients with postprandial hyperglycemia often have accompanying postprandial hyperinsulinemia. However, the postprandial rise in blood glucose itself is now considered to be a risk factor for the progression of atherosclerosis.Citation10,Citation11 α-Glucosidase inhibitors (α-GI) such as acarbose have shown long-term beneficial and protective effects against atherosclerosis. The Study to Prevent Non-Insulin-Dependent Diabetes Mellitus (STOP-NIDDM) trial demonstrated that treatment with acarbose reduces the onset of diabetes and the incidence of cardiovascular disease and new hypertension in patients with impaired glucose tolerance.Citation12–Citation14 A meta-analysis of seven long-term studies has also shown that acarbose prevents myocardial infarction and cardiovascular disease in patients with type 2 diabetes.Citation15 These findings suggest that inhibition of postprandial hyperglycemia by α-GI may be a promising therapeutic strategy for the prevention of cardiovascular disease in patients with impaired glucose tolerance and/or diabetes.
Miglitol, another α-GI, has unique pharmacokinetics.Citation16 After oral administration, it is rapidly and completely absorbed, even at a high dose, from the small intestines,Citation16 even though other α-GIs are scarcely absorbed there. These pharmacokinetics enable early-phase suppression of postprandial glucose elevation with a decrease in the severity of gastrointestinal complications, even at high doses, because absorption of carbohydrates is very low in the lower small intestine where miglitol is concentrated. However, the effects of miglitol on platelet activation markers, selectins, and adiponectin in patients with type 2 diabetes are poorly understood. Therefore, this study was performed to investigate the effects of miglitol on platelet activation markers, selectins, and adiponectin in type 2 diabetic patients.
Methods
Patients
The subjects included 72 nondiabetic (37 patients with hypertension and 35 patients with hyperlipidemia) and 38 diabetic patients (). Between April 2007 and November 2009, patients were selected from among those admitted to our hospital for the treatment of hypertension, hyperlipidemia, and diabetes. The study protocol was approved by our Institutional Review Board, and written informed consent was obtained from each patient prior to starting the trial. A history (within 3 months prior to enrolment) of inflammatory disease, coronary artery disease, or cerebrovascular disease was not permitted. Clinically detectable renal dysfunction (serum creatinine ≥2.0 mg/dL), hepatic dysfunction (elevated transaminases), infection (fever or elevated white blood cell count), or malignancy (detected by ultrasound or computed tomography) were also not permitted. Ten patients were taking aspirin because of old cerebral infarction or angina pectoris, while 39 patients were using angiotensin II receptor blockers (ARBs), and 24 patients were taking Ca antagonists for hypertension (). There were also 27 patients taking statins for hyperlipidemia. The doses of prior drugs such as aspirin, statins, ARBs, and Ca-antagonists were not adjusted during the present study.
Table 1 Baseline characteristics of the study population
Study design
Miglitol (150 mg/day) was administered for 4 months to randomly selected patients. There were no other changes to drug therapy during the treatment. Clinical and biochemical data were obtained before and after starting acarbose administration.
Measurement of platelet-derived microparticles
An enzyme-linked immunosorbent assay (ELISA) kit for the detection of PDMPsCitation17–Citation19 was obtained from Jimro Co, Ltd (Tokyo, Japan). Briefly, a blood sample was collected from a peripheral vein into a vacutainer containing EDTA-ACD (ethylenediaminetetraacetic acid–acid citrate dextrose solution) (Nipro Co Ltd, Japan) with a 21-gauge needle to minimize platelet activation. The sample was gently mixed by inverting the tube once or twice and then left at room temperature for 2–3 hours, followed by centrifugation at 8000 g for 5 minutes at room temperature. Immediately after centrifugation, we collected 200 μL of the upper layer of supernatant from a 2-mL sample to avoid contamination and stored each sample at −40°C until analysis. The results of the ELISA performed under the current experimental conditions were reproducible. PDMPs were measured twice, and the mean value was calculated. The kit employed two monoclonal antibodies directed against platelet glycoproteins CD42b and CD42a (glycoprotein Ib and IX). One U/mL of PDMP was defined as 24,000 solubilized platelets/mL in this ELISA.
Measurement of adiponectin, soluble CD40 ligand (sCD40L), sP-selectin, soluble E-selectin (sE-selectin), and soluble L-selectin (sL-selectin)
Blood samples from patients and controls were collected into tubes containing sodium citrate or tubes without anticoagulant and were allowed to clot at room temperature for a minimum of 1 hour. Serum or citrated plasma was then isolated by centrifugation for 20 minutes at 1000 g (4°C) and stored at −30°C until analysis with an adiponectin ELISA kit (Otsuka Pharmaceuticals Co Ltd, Tokyo, Japan). sCD40L, sP-selectin, sE-selectin, and sL-selectin were measured with a monoclonal antibody-based ELISA kit from BioSource International Inc (Camarillo, CA). The recombinant products and standard solutions provided with the kits were used as positive controls in each assay, and procedures were done according to the manufacturers’ instructions.
Statistics
Data are expressed as the mean ± standard deviation and were analyzed by two-factor analysis of variance (ANOVA) for repeated measures, as it was appropriate. Between-group comparisons were made with the Bonferroni test, and within-group differences were assessed with Student’s paired t-test. The level of significance was P < 0.05.
Results
When baseline values before treatment were compared among the three patient groups, no significant differences were noted for any of the parameters ().
The levels of PDMP, sCD40L, sE-selectin, sP-selectin, and sL-selectin were higher in diabetic patients than in hypertensive patients (). However, there were no significant differences between the hypertensive and hyperlipidemic patients. Before miglitol treatment, adiponectin levels were lower in the diabetic patients than the hypertensive patients (). There were no significant differences between the hypertensive and hyperlipidemic patients with respect to PDMP, sCD40L, sP-selectin, sE-selectin, and sL-selectin, although they showed a slight difference for adiponectin ().
Table 2 Levels of PDMP, sCD40 L, adiponectin, and selectins in patients with hypertension, hyperlipidemia, or type 2 diabetes
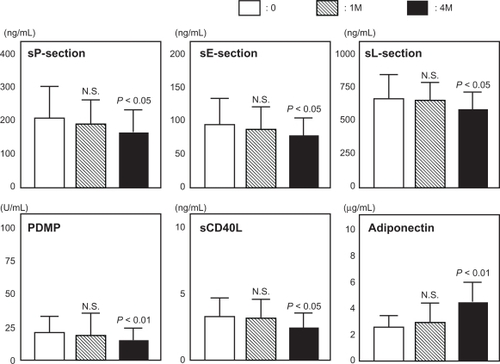
Miglitol therapy significantly decreased the plasma PDMP level relative to baseline (before vs 1 month vs 4 months; 21.2 ± 7.6 vs 18.2 ± 8.5 vs 15.4 ± 6.5 U/mL; 1 month, not significant [NS]; 4 months, P < 0.01) (). Miglitol also caused a significant decrease in sCD40L (before vs 1 month vs 4 months; 3.1 ± 1.2 vs 2.8 ± 1.1 vs 2.3 ± 0.9 ng/mL; 1 month, NS; 4 months, P < 0.05), sP-selectin (before vs 1 month vs 4 months; 213 ± 98 vs 194 ± 73 vs 162 ± 81 ng/mL; 1 month, NS, 4 months; P < 0.05), sE-selectin (before vs 1 month vs 4 months; 696 ± 141 vs 688 ± 235 vs 579 ± 128 ng/mL; 1 month, NS; 4 months, P < 0.05), and sL-selectin (before vs 1 month vs 4 months; 631 ± 195 vs 620 ± 139 vs 562 ± 124 ng/mL; 1 month, NS; 4 months, P < 0.05) (). On the other hand, miglitol therapy led to a significant increase in adiponectin levels after 4 months compared with baseline (before vs 1 month vs 4 months; 2.41 ± 1.22 vs 2.82 ± 1.34 vs 4.63 ± 1.85 μg/mL; 1 month, NS; 4 months, P < 0.01) ().
Figure 1 Changes in PDMP, sCD40L, sP-selectin, sE-selectin, sL-selectin, and adiponectin following administration of miglitol to patients with type 2 diabetes. Bars show the mean ± standard deviation. P-values are for comparison with each baseline parameter (before vs 1 month or 4 months). 0 denotes before; M denotes month (after).
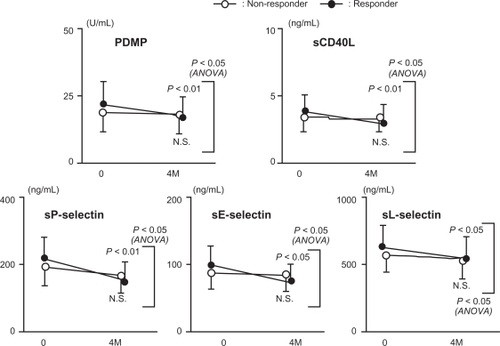
We divided the patients of the diabetes group into two subgroups (responders and nonresponders) according to their adiponectin response to miglitol treatment. Responders were defined as those patients in whom the plasma adiponectin levels increased by one and a half times or more after miglitol treatment as compared with pretreatment levels. The plasma values of PDMP and sCD40L in the two groups are shown in . Significant decreases in the plasma PDMP and sCD40L levels were observed in the responder group after miglitol treatment (PDMP before treatment vs after treatment: responder group 22.3 ± 6.4 vs 16.8 ± 6.6 U/mL, P < 0.01; nonresponder group 19.4 ± 5.9 vs 18.6 ± 6.3 U/mL, NS, ANOVA; responder group vs nonresponder group P < 0.05. sCD40L before treatment vs after treatment: responder group 3.4 ± 1.3 vs 2.5 ± 1.2 ng/mL, P < 0.05; nonresponder group 3.0 ± 1.6 vs 2.7 ± 1.7 ng/mL, NS, ANOVA; responder vs nonresponder, P < 0.05). The plasma values of selectins in the two groups are also shown in . Significant decreases in plasma sP-selectin, sE-selectin, and sL-selectin were observed after miglitol treatment in the responder group (sP-selectin before treatment vs after treatment: responder group 229 ± 88 vs 176 ± 75 ng/mL, P < 0.01; nonresponder group: 203 ± 85 vs 188 ± 87 ng/mL, NS, ANOVA; responder group vs non-responder group P < 0.05. sE-selectin before treatment vs after treatment: responder group 102 ± 44 vs 81 ± 39 ng/mL, P < 0.05; nonresponder group 93 ± 38 vs 88 ± 40 ng/mL, NS, ANOVA; responder group vs nonresponder group, P < 0.05. sL-selectin before treatment vs after treatment: responder group 649 ± 188 vs 576 ± 175 ng/mL, P < 0.05; nonresponder group 613 ± 156 vs 592 ± 163 ng/mL, NS, ANOVA; responder group vs nonresponder group P < 0.05).
Figure 2 Changes in PDMP, sCD40L, sP-selectin, sE-selectin, and sL-selectin during administration of miglitol to type 2 diabetic patients with or without a significant improvement in adiponectin. Responder: with a significant improvement of adiponectin. Nonresponder: without a significant improvement of adiponectin. Bars show the mean ± standard deviation. 0 denotes before; M denotes month (after). P-values are for comparison with each baseline parameter (before vs 4 months).
Discussion
PDMPs play an important role in the clotting process, so an increase in PDMPs is likely to cause hypercoagulability.Citation20 We previously reported that PDMP levels were significantly increased in diabetic patients.Citation21 Because PDMPs promote the expression of adhesion molecules by monocytes and endothelial cells,Citation22 it seems possible that these microparticles may participate in the development or progression of atherosclerosis in diabetics. Strong antiplatelet drugs such as cilostazol or ticlopidine can inhibit the elevation of PDMP,Citation23–Citation25 but the use of these agents for primary prevention of atherothrombosis is problematic. Thus, a new strategy is needed for diabetic patients who are highly susceptible to atherothrombosis. In the present study, miglitol therapy significantly decreased plasma PDMP levels. Although no direct changes in platelet function were shown, miglitol therapy also improved another platelet activation marker (sCD40L) in our patients with diabetes. Postprandial hyperglycemia may be related to the activation of platelets in diabetic patients. Postprandial hyperglycemia induces oxidative stress via various biochemical pathways, and generation of superoxide occurs, which reacts with nitric oxide (NO) to form peroxynitrite.Citation26 The resulting decrease in NO levels and activity could accelerate vascular inflammation and platelet activation by enhancing the expression of various cytokines and growth factors.Citation27 Thus, our results indicate that postprandial hyperglycemia causes platelet activation and endothelial dysfunction. Treatment with miglitol significantly reduces body mass index and waist circumference.Citation28,Citation29 It has also been reported that miglitol prevents nephropathic complication in type 2 diabetic patients.Citation29 Our results could explain one of the mechanisms involved.
The plasma level of adiponectin is decreased in obese individualsCitation30 and is closely related to whole-body insulin sensitivity.Citation31 A significant decrease in plasma adiponectin is also found in patients with type 2 diabetes.Citation31 Adiponectin has been reported to suppress the attachment of monocytes to endothelial cellsCitation27 and plays a role in the protection against vascular injury, so hypoadiponectinemia is associated with endothelial dysfunction.Citation32 Hypoadiponectinemia also seems to cause platelet activation. The level of NO, which regulates platelet activation, is decreased by hypoadiponectinemia because adiponectin stimulates NO production by vascular endothelial cells.Citation33–Citation35 Thus, platelet activation occurs due to low NO concentrations in persons with hypoadiponectemia. Therefore, the increase in adiponectin by miglitol may have an antiplatelet effect via the promotion of NO production. Recently, it has been shown that various posttranslational modifications, including glycosylation of lysine residues, are necessary for the multimerization of adiponectin to occur.Citation36 Such intracellular post-translational processes may be affected by hyperglycemia, leading to functional impairment at the organ level in diabetic patients.Citation37–Citation39 Therefore, the improvement in postprandial hyperglycemia by miglitol could alter the post-translational modification of adiponectin.
In the present study, we found that miglitol caused the reduction of sP-selectin, sE-selectin, and sL-selectin. When the patients in the diabetes group were divided into two subgroups according to the adiponectin response to miglitol treatment, a significant decrease in plasma levels of selectins were found after miglitol treatment in the adiponectin responder group. In addition, similar results were also found for plasma PDMP and sCD40L. These results suggest that miglitol causes adiponectin-dependent improvement in the plasma levels of selectins, PDMP, and sCD40L in diabetic patients.
The exact mechanism by which miglitol treatment leads to an increase in circulating adiponectin levels remains unclear. We postulate the participation of the gut-derived incretin hormone, glucagon-like peptide 1 (GLP-1), for the mechanism underlying adiponectin elevation by miglitol treatment. Recently, the glucose-lowering and anti-obesity effects of GLP-1-based therapies for type 2 diabetes have been extensively evaluated.Citation40 One of the antidiabetic effects of miglitol depends on GLP-1, because miglitol can enhance active GLP-1 secretion.Citation28 In addition, some studies show that GLP-1 could promote adiponectin secretion.Citation41,Citation42 We believe that the effect of miglitol on selectins and platelet activation marker activity depends on adiponectin. Therefore, miglitol could inhibit the progression of atherothrombosis by promoting adiponectin-dependent improvement of the plasma selectins, PDMP, and sCD40L. However, further studies are necessary to elucidate the effects of miglitol itself on adiponectin production.
In conclusion, miglitol increased circulating adiponectin levels in patients with type 2 diabetes. In addition, miglitol treatment led to a decrease in platelet activation markers and selectins. Miglitol may be beneficial for primary prevention of atherothrombosis in patients with type 2 diabetes. However, a large clinical trial to test this hypothesis is required.
Acknowledgements
This study was partly supported by a grant from the Japan Foundation of Neuropsychiatry and Hematology Research, a Research Grant for Advanced Medical Care from the Ministry of Health and Welfare of Japan, and a Grant (13670760 to SN) from the Ministry of Education, Science and Culture of Japan.
Disclosure
The authors report no conflicts of interest in this work.
References
- SchaferAIThe hypercoagulable statesAnn Intern Med19851028148183158262
- FradeLJGde la CalleHAlavaIDiabetes as a hypercoagulable state: its relationship with fibrin fragments and vascular damageThromb Res1987475335403118498
- NomuraSOzakiYIkedaYFunction and role of microparticles in various clinical settingsThromb Res200812382318667228
- CominaciniLPasiniAFGarbinUElevated levels of soluble E-selectin in patients with IDDM and NIDDM: relation to metabolic controlDiabetologia199538112211248591829
- LimYCSnappKKansasGSImportant contributions of P-selectin glycoprotein ligand-1-mediated secondary capture to human monocyte adhesion to P-selectin, E-selectin, and TNF-α-activated endothelium under flow in vitroJ Immunol1998161250125089725249
- TschopeDEsserJSchwippertBLarge platelets circulate in an activated state in diabetesSemin Thromb Haemost199117433439
- NomuraSShouzuAOmotoSSignificance of chemokines and activated platelets in patients with diabetesClin Exp Immunol200012143744310971508
- RodriguezBLLauNBurchfielCMGlucose intolerance and 23-year risk of coronary heart disease and total mortality: the Honolulu Heart ProgramDiabetes Care1999221262126510480768
- CoutinhoMGersteinHCWangYThe relationship between glucose and incident cardiovascular events. A metaregression analysis of published data from 20 studies of 95,783 individuals followed for 12.4 yearsDiabetes Care19992223324010333939
- The DECODE study group on behalf of the Europearn Diabetes Epidemiology GroupGlucose tolerance and mortality: comparison of WHO and American Diabetic Association diagnostic criteria. Diabetes Epidemiology: collaborative analysis of diagnostic criteria in EuropeLancet199935461762110466661
- NakagamiTHyperglycaemia and mortality from all cause and from cardiovascular disease in five populations of Asian originDiabetologia20044738539414985967
- ChiassonJLJosseRGGomisRAcarbose for prevention of type 2 diabetes mellitus: the STOP-NIDDM randomized trialLancet20023592072207712086760
- ChiassonJLJosseRGGomisRAcarbose treatment and the risk of cardiovascular disease and hypertension in patients with impaired glucose tolerance: the STOP-NIDDM trialJAMA200329048649412876091
- HanefieldMChiassonJLKoehlerCAcarbose slows progression of intima-media thickness of the carotid arteries in subjects with impaired glucose toleranceStroke2004351073107815073402
- HanefeldMCagatayMPetrowitschTAcarbose reduces the risk for myocardial infarction in type 2 diabetic patients: meta-analysis of seven long-term studiesEur Heart J200425101614683737
- AhrHJBobergMBrendelEKrauseHPSteinkeWPharmacokinetics of miglitol. Absorption, distribution, metabolism, and excretion following administration to rats, dogs, and manArzneimittelforschung1997477347459239452
- OsumiKOzekiYSaitoSDevelopment and assessment of enzyme immunoassay for platelet-derived microparticlesThromb Haemost20018532633011246556
- NomuraSUehataSSaitoSEnzyme immunoassay detection of platelet-derived microparticles and RANTES in acute coronary syndromeThromb Haemost20038950651212624635
- NomuraSShouzuATaomotoKAssessment of an ELISA kit for platelet-derived microparticles by joint research at many institutes I JapanJ Atheroscler Thromb20091687888720032575
- SimsPJFaioniEMWiedmerTComplement proteins C5b-9 cause release of membrane vesicles from the platelet surface that are enriched in the membrane receptor for coagulation factor Va and express prothrombinase activityJ Biol Chem198826318205182122848029
- NomuraSSuzukiMKatsuraKPlatelet-derived microparticles may influence the development of atherosclerosis in diabetes mellitusAtherosclerosis19951162352407575778
- NomuraSTandonNNNakamuraTHigh-shear-stress- induced activation of platelets and microparticles enhances expression of cell adhesion molecules in THP-1 and endothelial cellsAtherosclerosis200115827728711583705
- NomuraSShouzuAOmotoSEffect of cilostazol on soluble adhesion molecules and platelet-derived microparticles in patients with diabetesThromb Haemost1998803883929759615
- NomuraSInamiNIwasakaTPlatelet activation markers, microparticles and soluble adhesion molecules are elevated in patients with arteriosclerosis obliterans: therapeutic effects by cilostazol and potentiation by dipyridamolePlatelets20041516717215203718
- NomuraSTakahashiNInamiNProbucol and ticlopidine: effect on platelet and monocyte activation markers in hyperlipidemic patients with and without type 2 diabetesAtherosclerosis200417432933515136063
- KurowskaEMNitric oxide therapies in vascular diseasesCurr Pharm Des2002815516611812265
- OuchiNKiharaSAritaYNovel modulator for endothelial adhesion molecules: adipocyte-derived plasma protein, adiponectinCirculation19991002473247610604883
- ArakawaMEbatoCMitaTMiglitol suppresses the post-prandial increase in interleukin 6 and enhances active glucagons-like peptide secretion in viscerally obese subjectsMetabolism Clin Exp20085712991306
- YokoyamaHKannoSIshimuraINodeKMiglitol increases adiponectin level and decreases urinary albumin excretion in patients with type 2 diabetes mellitusMetabolism Clin Exp20085614581463
- OuchiNKiharaSAritaYAdiponectin, an adipocyte-derived plasma protein, inhibits endothelial NF-kappa B signaling through a cAMP-dependent pathwayCirculation20001021296130110982546
- HottaKFunahashiTAritaYPlasma concentrations of a novel, adipose-specific protein, adiponectin, in type 2 diabetes patientsArtherioscler Thromb Vasc Biol20002015951599
- ShimabukuroMHigaNAsahiTHypoadiponectinemia is closely linked to endothelial dysfunction in manJ Clin Endocrinol Metab2003883236324012843170
- ChenHMontagnaniMFunahashiTAdiponectin stimulates production of nitric oxide in vascular endothelial cellsJ Biol Chem2003278450214502612944390
- HattoriYSuzukiMHattoriSGlobular adiponectin upregulates nitric oxide production in vascular endothelial cellsDiabetologia2003461543154914551684
- NomuraSShouzuAOmotoSCorrelation between adiponectin and reduction of cell adhesion molecules after pitavastatin treatment in hyperlipidemic patients with type 2 diabetes mellitusThromb Res2008122394517920663
- WangYLamKSChanLPost-translational modifications of the four conserved lysine residues within the collagenous domain of adiponectin are required for the formation of its high molecular weight oligomeric complexJ Biol Chem2006281163911640016621799
- FülöpNMarchaseRBChathamJCRole of protein O-linked N-acetyl-glucosamine in mediating cell function and survival in the cardiovascular systemCardiovasc Res20077328829716970929
- FülöpNMasonMMDuttaKImpact of Type 2 diabetes and aging on cardiomyocyte function and O-linked N-acetylglucosamine levels in the heartAm J Physiol Cell Physiol2007292C1370C137817135297
- OchiaiHOokaHShidaCAcarbose treatment increases serum total adiponectin levels in patients with type 2 diabetesEndocr J20085554955618480556
- KnopFKVilsbollTLarsenSMadsbadSHolstJJKrarupTNo hypoglycemia after subcutaneous administration of glucagons-like peptide-1 in lean type 2 diabetic patients and in patients with diabetes secondary to chronic pancreatitisDiabetes Care2003262581258712941722
- PocaiACarringtonPEAdamsJRGlucagon-like peptide 1/glucagons receptor dual agonism reverses obesity in miceDiabetes2009582258226619602537
- KimVhung leTHosakaTYoshidaMExendin-4, a GLP-1 receptor agonist, directly induces adiponectin expression through protein kinase A pathway and prevents inflammatory adipokine expressionBiochem Biophys Res Commun200939061361819850014