Abstract
The natural course of heart failure with decreased and preserved systolic function is almost identical. The current concept of heart failure where decreased cardiac output plays the major role does not explain this similarity. We suggest a revised concept of heart failure where congestion plays the leading role. While congestion is almost invariably present in heart failure with normal and with reduced systolic function, the low output syndrome is only present in heart failure with reduced systolic function. The small difference in morbidity and mortality in favor of heart failure with preserved systolic function reflects the contribution of low output syndrome to the natural course of the disease. Congestion can result from low output or from multiple other conditions, but severity of congestion is the major determinant of progression of heart failure.
Keywords:
Background
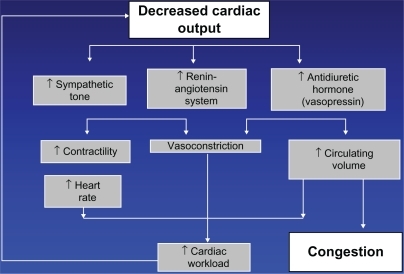
Heart failure is a final common pathway of practically all cardiac diseases, including coronary artery disease, hypertension, congenital cardiac defects, nonischemic cardiomyopathy, valvular defects of multiple etiologies, and infiltrative diseases. Surprisingly, the very term “heart failure” is not well defined. Multiple definitions circulating in the literature are inconsistent, and such inconsistency reflects the lack of uniform understanding of the essence of this condition. presents the classic chart of pathogenesis of heart failure. Decreased cardiac output triggers a cascade of neurohormonal activation that occupies center stage, with congestion being a modest byproduct of the chain of events. If this chart reflects the true picture, and decreased myocardial contractility plays the leading role, the mainstay of heart failure treatment should be inotropes. However, inotropes have a very limited place in management of heart failure. Besides, the chart does not apply to approximately one half of those patients with heart failure who have heart failure with preserved systolic function. These patients do not benefit from neurohormonal blockade, inotropes, ventricular assist devices, or cardiac transplantation. Most importantly, the natural course and prognosis in heart failure with preserved and with reduced systolic function is nearly identical. In other words, whether the pathogenetic mechanism in applies or not, the outcome is the same. There can be only one explanation, ie, decreased cardiac output does not play a key role in heart failure, and our current concept should be revised.
Figure 1 Current concept of heart failure.
Guidelines on definition of heart failure
The European Congress of Cardiology (2008) defines heart failure as a “syndrome in which the patients should have the following features: symptoms of HF, typically shortness of breath at rest or during exertion, and/or fatigue; signs of fluid retention such as pulmonary congestion or ankle swelling”.Citation1
The American College of Cardiology and the American Heart Association (2009) guidelines define heart failure as a “complex clinical syndrome … . The cardinal manifestations of HF are dyspnea and fatigue, which may limit exercise tolerance, and fluid retention, which may lead to pulmonary congestion and peripheral edema”.Citation2
The Heart Failure Society of America (2010) defines heart failure as “a syndrome caused by cardiac dysfunction … whether the dysfunction is primarily systolic or diastolic or mixed, it leads to neurohormonal and circulatory abnormalities, usually resulting in characteristic symptoms such as fluid retention, shortness of breath, and fatigue, especially on exertion”.Citation3
In summary, all definitions agree that heart failure is a syndrome that clinically manifests itself as congestion. This part of all the above texts is strong and clear and obviously does not cause any controversies. The second part of all the definitions is vague and controversial.
According to the American College of Cardiology and the American Heart Association definition, the syndrome of congestion “... can result from any structural or functional cardiac disorder that impairs the ability of the ventricle to fill with or eject blood”.Citation2 The ability of the ventricle to fill with blood reflects its diastolic function. The ability of the ventricle to eject blood reflects its systolic function.
Systolic function is measured by left ventricular ejection fraction using echocardiography or other imaging modalities, or by cardiac output using a Swan-Ganz catheter. There is plenty of evidence that 40%–50% of patients with heart failure have normal systolic function. It was once believed that although left ventricular ejection fraction is preserved, “effective blood flow” can be impaired.Citation4 However, several studies have demonstrated that blood flow is normal or increased in a substantial number of patients with heart failure with preserved systolic function.Citation5,Citation6
Diastolic function, or left ventricular filling pressure, is evaluated by echocardiography or by Swan-Ganz catheter. There is very little evidence that diastolic function is normal in any substantial proportion of the heart failure population. In heart failure patients with both reduced and with preserved left ventricular ejection fraction, diastolic dysfunction by echocardiography was present in more than 90% of cases.Citation7 None of the heart failure patients with ejection fraction less than 35% had normal diastolic function.Citation8 In the Olmstead County heart failure cohort, only 10% of patients with preserved ejection fraction and 5% of patients with reduced ejection fraction had normal diastolic function.Citation9 In another cohort, only one in 45 participants with heart failure had normal diastolic function.
Diastolic dysfunction, unlike systolic dysfunction, reflects severity of congestion. One of the parameters of diastolic function, namely the E/e′ ratio, correlates closely with intracardiac filling pressures.Citation10–Citation17 Simple volume overload with intravenous saline creates gradual progression of diastolic filling pattern from normal to restrictive.Citation18
While systolic dysfunction may or may not be present in heart failure, diastolic dysfunction is mandatory. Diastolic dysfunction is the equivalent of congestion. Diastolic dysfunction is the common denominator of heart failure. There is no heart failure without congestion. There is no heart failure without diastolic dysfunction. Diastolic function may improve and become normal as a result of treatment or natural evolution of the disease, but if there is no congestion, no diastolic dysfunction, and no elevated left ventricular end diastolic pressure at any time, there is no basis for a diagnosis of heart failure. Therefore, it is incorrect to state that heart failure results from either/or the inability of the ventricle to fill with or eject blood. It always results from the inability of the ventricle to fill with blood, while the function of ejection may be normal or impaired. Inability of the left ventricle to eject blood is important to the degree of the severity of congestion resulting from it.
According to the Heart Failure Society of America definition, the syndrome of congestion is “caused by cardiac dysfunction, generally resulting from myocardial muscle dysfunction or loss and characterized by either LV dilation or hypertrophy or both. Whether the dysfunction is primarily systolic or diastolic or mixed, it leads to neurohormonal and circulatory abnormalities …”.Citation3
The issue with primarily systolic or diastolic dysfunction or mixed is analyzed above. Neurohormonal abnormalities are well documented in heart failure with systolic dysfunction but not with preserved systolic function. All attempts to treat heart failure with preserved systolic function using medications targeting neurohormonal changes have failed. The CHARM-Preserved (Candesartan in Heart Failure Assessment of Reduction in Mortality and Morbidity) trial randomized 3023 patients between candesartan and placeboCitation19 and failed to demonstrate a significant effect on cardiovascular death, but fewer heart failure hospitalizations in the candesartan-treated patients were observed. These results are difficult to interpret because the cutoff of left ventricular ejection fraction in the CHARM trial was 40%, which creates a mix of heart failure with normal systolic function and with mild systolic dysfunction. The PEP-CHF (Perindopril in Elderly People with Chronic Heart Failure) study showed no effect of perindopril on mortality and heart failure hospitalizations.Citation20 The I-PRESERVE (Irbesartan in HF with preserved ejection fraction) trial did not demonstrate any mortality or morbidity benefit from irbesartan.Citation21 A recent meta-analysisCitation22 combined these studies to increase their statistical power and also failed to demonstrate a significant effect of inhibition of the renin-angiotensin-aldosterone system on mortality in preserved systolic function.
The statement of left ventricular dilatation or hypertrophy is also soft. The left ventricle may be dilated, but it may be normal in size. It can be hypertrophied but may also have perfectly normal wall thickness.
To summarize, heart failure is a clinical syndrome of congestion. It may be caused by decreased systolic function or other conditions causing volume overload. Therefore, evidence of congestion should be mandatory for the diagnosis of heart failure.
Guidelines on evidence of congestion
According to ADHERE (the Acute Decompensated Heart Failure National Registry), which included patients with and without left ventricular systolic dysfunction, most patients admitted for heart failure are “wet” or congested, with dyspnea, rales, edema, radiological signs of fluid overload, or combination of the above.Citation23 However, making the diagnosis of heart failure with preserved systolic function by only clinical criteria and normal ejection fraction could result in over-diagnosis of this condition. In a study by Caruana et al,Citation24 most patients with normal ejection fraction who were diagnosed as having heart failure in fact suffered from other diseases, such as coronary artery disease, obesity, chronic obstructive pulmonary disease, or other conditions explaining their symptoms, and only seven of 109 had heart failure.
To diagnose heart failure with preserved systolic function accurately, one has to demonstrate evidence of increased intracardiac pressures. Vasan and Levy proposed standardized clinical criteria where the diagnosis of “definite” heart failure requires clinical heart failure and ejection fraction ≥50% assessed within 72 hours after diagnosis and confirmed elevated filling pressures.Citation25 The timing requirement was later found to be unnecessary, because it was shown that ejection fraction does not change during decompensation and remains relatively stable.Citation26 The Working Group on Myocardial Function of the European Society of CardiologyCitation27 required evidence of diastolic dysfunction (pulmonary capillary wedge pressure >12 mmHg or left ventricular end diastolic pressures >16 mmHg) provided by cardiac catheterization or by Doppler velocities on echocardiography.
According to the European Society of Cardiology, three obligatory conditions are needed for the diagnosis of heart failure with normal systolic function. They include the presence of signs or symptoms of congestive heart failure, ejection fraction >50%, and evidence of left ventricular diastolic dysfunction.Citation28
Unfortunately, the majority of studies enrolling patients with heart failure and normal systolic function did not have documentation of either intracardiac pressure or left ventricular diastolic dysfunction. More importantly, not all current guidelines require rigorous assessment of diastolic dysfunction to establish a diagnosis of heart failure. Meanwhile, because congestion is the essence of heart failure, whether with preserved or reduced systolic function, evidence of congestion should be a mandatory part of the assessment of patients who may have heart failure based on symptoms. Addressing the requirements for initial assessment of patients with heart failure, American College of Cardiology and the American Heart Association guidelines recommend echocardiography for assessment of “... left ventricular ejection fraction, left ventricular size, wall thickness, and valve function ...” but do not even mention diastolic dysfunction.Citation2
The easiest way to estimate intracardiac pressures is to measure the level of brain natriuretic peptide, but in the American College of Cardiology and the American Heart Association guidelines it is recommended only as a supplemental tool “to improve diagnostic accuracy”.Citation2 Amazingly, recommended initial laboratory evaluation of patients presenting with heart failure includes complete blood count, urinalysis, serum electrolytes (including calcium and magnesium), blood urea nitrogen, serum creatinine, fasting blood glucose, lipid profile, liver function tests, and thyroid-stimulating hormone, but not brain natriuretic peptide.Citation2 In fact, brain natriuretic peptide is far more important for establishing the diagnosis of heart failure than the lipid profile, thyroid hormones, or any other listed parameters. On the contrary, the Heart Failure Society of America guidelines recommend measurement of brain natriuretic peptide in every patient with suspected heart failure.Citation3 Similarly, European guidelines include brain natriuretic peptide as a mandatory step in establishing the diagnosis of heart failure.Citation1
In summary, if all guidelines agree that heart failure is a syndrome of congestion, then evidence of congestion and assessment of its severity should be a cornerstone of the diagnosis and ongoing patient evaluation on follow-up. This applies similarly to heart failure with normal and reduced systolic function.
Low output syndrome
It is impossible to deny that not only congestion but also low output plays an important role in the natural history of heart failure, but only in heart failure with reduced systolic function. Multiple studies have reported decreased left ventricular ejection fraction as a poor predictive sign.Citation29,Citation30 In order to quantify its role and to compare it with the role of congestion, we have to compare the course of heart failure with normal and decreased systolic function.
Patients with preserved heart failure are usually older, more frequently women, have less coronary disease and myocardial infarction, and have more atrial fibrillation and other comorbidities. They have higher systolic blood pressures and pulse pressures,Citation29 as well as a higher prevalence of left ventricular hypertrophy, aortic valve disease, and anemia.Citation30
Despite these dissimilarities, the reported mortality is either similarCitation30–Citation34 or somewhat better in preserved systolic function.Citation35,Citation36 Earlier studies published in the 1980s and early 1990s reported a better prognosis in preserved ejection fraction, but more recent studies have identified no differences in mortality.Citation37
Patients with heart failure with both reduced and normal systolic function have congestion, but only patients with reduced systolic function have low output. Therefore, the difference in morbidity and mortality between heart failure with preserved and reduced left ventricular ejection fraction reflects the contribution of low output syndrome to the natural course of heart failure. Similarities in the natural course of heart failure with reduced and with preserved systolic function are likely explained by the syndrome of congestion shared by both groups. Using therapies unique for heart failure with the component of low output, or left ventricular remodeling, or reduced left ventricular systolic dysfunction (beta-blockers, angiotensin-converting enzyme inhibitors, cardiac resynchronization therapy, implantable cardioverter-defibrillator devices, ventricular assist devices, and cardiac transplantation) we are closing the small gap between morbidity and mortality in heart failure with normal and decreased systolic function. To treat the syndrome of congestion, which determines the course of heart failure to a much greater degree than the syndrome of low output, we use diuretics. The role of diuretics in the treatment of heart failure is discussed elsewhere.Citation38,Citation39 It typically takes fewer than 100 patients and several weeks of follow-up to realize that patients with heart failure cannot live without them,Citation40–Citation43 while it took thousands of patients and years of follow-up to demonstrate the survival benefit of angiotensin-converting enzyme inhibitors or beta-blockers.Citation44,Citation45
It is difficult to imagine a patient with heart failure who has never experienced congestion. However, there are clearly symptomatic patients with heart failure who are not congested. They are a small subset of very sick patients with low output and low systolic blood pressure. In full agreement with the pathogenetic chart (), they benefit from inotropes, an intra-aortic balloon pump, any means of mechanical circulation, and cardiac transplantation.
Inotropes were not proven to be beneficial in any of the randomized controlled trials, but everybody uses them empirically. Even if such patients are congested, they can rarely be diuresed without inotropes. The OPTIME-HF (Outcomes of Prospective Trial of Intravenous Milrinone for Acute Exacerbation of Chronic Heart Failure) trial unfortunately was not very informative because patients requiring inotropic support were not included.Citation46
Revised concept of heart failure
In the pathogenetic scheme reflecting the true relationship of two major syndromes in heart failure, ie, congestion, which is mandatory, and low output, which is optional, congestion occupies central place ().
Figure 2 Suggested concept of heart failure.
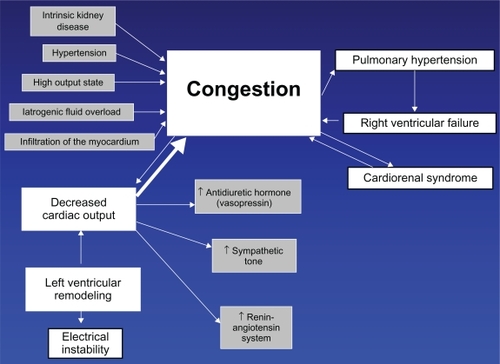
Congestion not only causes symptoms of volume overload, but it also determines the prognosis.Citation47 Congestion causes cardiorenal syndrome,Citation48,Citation49 pulmonary hypertension, and right ventricular failure. All of these symptoms exacerbate the problem, causing further congestion. Because congestion plays the central role, diuretics are the only group of medications equally effective in heart failure with preserved or reduced systolic function. In inpatient or outpatient settings, in systolic or diastolic heart failure, diuretics invariably remain the top prescribed drugs.Citation23
In about 50% of patients with heart failure, congestion is caused by left ventricular systolic dysfunction. It has been shown that heart failure with preserved and reduced systolic function is typically not different stages of the same disease but rather separate entities. The left ventricular ejection fraction has a bimodal distribution.Citation50
However, the relationship between intracardiac pressure and ejection fraction may be more complex. Evidence suggests that persistence of congestion or high intracardiac pressures results in decreased contractility, and decongestion improves contractility. In animal experiments, myocardial edema results in an immediate decrease in contractility.Citation51 Aggressive diuresis resulted not only in decreased pulmonary capillary wedge pressure but also in an increase in left ventricular ejection fraction from 35.7% to 39.5% in a matter of six days.Citation52
Even electrical instability, which is usually a feature of left ventricular remodeling, may be precipitated by congestion. Studies of tracings from implantable devices with OptiVol® indicate there is a weak but significant association between decreased intrathoracic impedance and malignant ventricular arrhythmias.Citation53,Citation54
The other 50% of patients with heart failure who have normal systolic function have congestion resulting from other causes, including renal dysfunction, infiltrative diseases of the myocardium, iatrogenic fluid overload, ischemia, hypertension with left ventricular hypertrophy, or any other conditions increasing intravascular volume, or altering myocardial relaxation. They demonstrate less electrical instability, are less prone to sudden cardiac death, and benefit little from inhibition of renin-angiotensin or beta-blockade.
Conclusion
Heart failure is a syndrome of congestion resulting from decreased left ventricular systolic function or any other condition causing fluid retention or altering relaxation of the myocardium. Evidence of congestion, increased intracardiac pressures, or diastolic dysfunction is a mandatory step in the initial diagnosis of heart failure, and evaluation of severity of congestion is a mandatory step in all subsequent evaluation of patients with heart failure. Congestion is the main factor that determines the natural course of heart failure. The role of low output syndrome, or decreased systolic function, can be defined as the difference between morbidity and mortality in heart failure with reduced and with preserved systolic function. Guidelines that currently define the strategy of diagnosis and management of heart failure could benefit from revisions consistent with this concept.
Disclosure
The author reports no conflicts of interest in this work.
References
- DicksteinKCohen-SolalAFilippatosGESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM)Eur Heart J200829192388244218799522
- HuntSAAbrahamWTChinMH2009 Focused update incorporated into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults. A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines Developed in Collaboration With the International Society for Heart and Lung TransplantationJ Am Coll Cardiol20095315e1e9019358937
- LindenfeldJAlbertNMBoehmerJPHFSA 2010 Comprehensive Heart Failure Practice GuidelineJ Card Fail2010166e1e19420610207
- AndrewPDiastolic heart failure demystifiedChest2003124274475312907569
- MaurerMSKingDLEl-Khoury RumbargerLPackerMBurkhoffDLeft heart failure with a normal ejection fraction: Identification of different pathophysiologic mechanismsJ Card Fail200511317718715812744
- MaurerMSBurkhoffDFriedLPGottdienerJKingDLKitzmanDWVentricular structure and function in hypertensive participants with heart failure and a normal ejection fraction: The Cardiovascular Health StudyJ Am Coll Cardiol200749997298117336721
- BrucksSLittleWCChaoTContribution of left ventricular diastolic dysfunction to heart failure regardless of ejection fractionAm J Cardiol200595560360615721099
- SamadBAOlsonJMAlamMCharacteristics of left ventricular diastolic function in patients with systolic heart failure: A Doppler tissue imaging studyJ Am Soc Echocardiogr200518989690016153510
- BursiFWestonSARedfieldMMSystolic and diastolic heart failure in the communityJAMA2006296182209221617090767
- OmmenSRNishimuraRAAppletonCPClinical utility of Doppler echocardiography and tissue Doppler imaging in the estimation of left ventricular filling pressures: A comparative simultaneous Doppler-catheterization studyCirculation2000102151788179411023933
- LesterSJTajikAJNishimuraRAOhJKKhandheriaBKSewardJBUnlocking the mysteries of diastolic function: Deciphering the Rosetta Stone 10 years laterJ Am Coll Cardiol200851767968918279730
- LiangHYCauduroSAPellikkaPAComparison of usefulness of echocardiographic Doppler variables to left ventricular end-diastolic pressure in predicting future heart failure eventsAm J Cardiol200697686687116516591
- MaurerMSPackerMBurkhoffDDiastolic heart failureN Engl J Med2004351111143114515356314
- MaurerMSSpevackDBurkhoffDKronzonIDiastolic dysfunction: Can it be diagnosed by Doppler echocardiography?J Am Coll Cardiol20044481543154915489083
- NishimuraRAAbelMDHatleLKSignificance of Doppler indices of diastolic filling of the left ventricle: Comparison with invasive hemodynamics in a canine modelAm Heart J19891186124812582686379
- NishimuraRAAppletonCPRedfieldMMIlstrupDMHolmesDRJrTajikAJNoninvasive Doppler echocardiographic evaluation of left ventricular filling pressures in patients with cardiomyopathies: A simultaneous Doppler echocardiographic and cardiac catheterization studyJ Am Coll Cardiol1996285122612338890820
- NishimuraRATajikAJEvaluation of diastolic filling of left ventricle in health and disease: Doppler echocardiography is the clinician’s Rosetta StoneJ Am Coll Cardiol19973018189207615
- MasutaniSLittleWCHasegawaHChengHJChengCPRestrictive left ventricular filling pattern does not result from increased left atrial pressure aloneCirculation2008117121550155418332265
- YusufSPfefferMASwedbergKEffects of candesartan in patients with chronic heart failure and preserved left-ventricular ejection fraction: The CHARM-Preserved TrialLancet2003362938677778113678871
- ClelandJGTenderaMAdamusJFreemantleNPolonskiLTaylorJThe perindopril in elderly people with chronic heart failure (PEP-CHF) studyEur Heart J200627192338234516963472
- MassieBMCarsonPEMcMurrayJJIrbesartan in patients with heart failure and preserved ejection fractionN Engl J Med2008359232456246719001508
- ShahRVDesaiASGivertzMMThe effect of renin-angiotensin system inhibitors on mortality and heart failure hospitalization in patients with heart failure and preserved ejection fraction: A systematic review and meta-analysisJ Card Fail201016326026720206902
- YancyCWFonarowGCCommitteeASAQuality of care and outcomes in acute decompensated heart failure: The ADHERE registryCurr Heart Fail Rep20041312112816036035
- CaruanaLPetrieMCDavieAPMcMurrayJJDo patients with suspected heart failure and preserved left ventricular systolic function suffer from “diastolic heart failure” or from misdiagnosis? A prospective descriptive studyBMJ2000321725521521810903655
- VasanRSLevyDDefining diastolic heart failure: A call for standardized diagnostic criteriaCirculation2000101172118212110790356
- GandhiSKPowersJCNomeirAMThe pathogenesis of acute pulmonary edema associated with hypertensionN Engl J Med20013441172211136955
- [No authors listed]How to diagnose diastolic heart failure. European Study Group on Diastolic Heart FailureEur Heart J199819799010039717033
- PaulusWJTschopeCSandersonJEHow to diagnose diastolic heart failure: A consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the Heart Failure and Echocardiography Associations of the European Society of CardiologyEur Heart J200728202539255017428822
- AnsariMAlexanderMTutarAMassieBMIncident cases of heart failure in a community cohort: Importance and outcomes of patients with preserved systolic functionAm Heart J2003146111512012851618
- BerryCHoggKNorrieJStevensonKBrettMMcMurrayJHeart failure with preserved left ventricular systolic function: A hospital cohort studyHeart200591790791315958359
- BhatiaRSTuJVLeeDSOutcome of heart failure with preserved ejection fraction in a population-based studyN Engl J Med2006355326026916855266
- Varela-RomanAGonzalez-JuanateyJRBasantePClinical characteristics and prognosis of hospitalised inpatients with heart failure and preserved or reduced left ventricular ejection fractionHeart200288324925412181216
- Varela-RomanAGrigorianLBargeEBassantePde la PenaMGGonzalez-JuanateyJRHeart failure in patients with preserved and deteriorated left ventricular ejection fractionHeart200591448949415772209
- FonarowGCStoughWGAbrahamWTCharacteristics, treatments, and outcomes of patients with preserved systolic function hospitalized for heart failure: A report from the OPTIMIZE-HF RegistryJ Am Coll Cardiol200750876877717707182
- VasanRSLarsonMGBenjaminEJEvansJCReissCKLevyDCongestive heart failure in subjects with normal versus reduced left ventricular ejection fraction: Prevalence and mortality in a population-based cohortJ Am Coll Cardiol19993371948195510362198
- SweitzerNKLopatinMYancyCWMillsRMStevensonLWComparison of clinical features and outcomes of patients hospitalized with heart failure and normal ejection fraction (≥55%) versus those with mildly reduced (40% to 55%) and moderately to severely reduced (<40%) fractionsAm J Cardiol200810181151115618394450
- SenniMRedfieldMMHeart failure with preserved systolic function. A different natural history?J Am Coll Cardiol20013851277128211691495
- GuglinMDiuretics as pathogenetic treatment for heart failureInt J Gen Med20114919821403798
- GuglinMReappraisal of the role of diuretics in heart failureCardiol Rev2009172565919367146
- RichardsonABaylissJScrivenAJParameshwarJPoole-WilsonPASuttonGCDouble-blind comparison of captopril alone against frusemide plus amiloride in mild heart failureLancet1987285617097112888942
- CowleyAJStainerKWynneRDRowleyJMHamptonJRSymptomatic assessment of patients with heart failure: Double-blind comparison of increasing doses of diuretics and captopril in moderate heart failureLancet1986285107707722876233
- van KraaijDJJansenRWBruijnsEGribnauFWHoefnagelsWHDiuretic usage and withdrawal patterns in a Dutch geriatric patient populationJ Am Geriatr Soc19974589189229256841
- MathurPNPugsleySOPowlesACMcEwanMPCampbellEJEffect of diuretics on cardiopulmonary performance in severe chronic airflow obstruction. A controlled clinical trialArch Intern Med198414411215421576388521
- [No authors listed]Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. The SOLVD InvestigatorsN Engl J Med199132552933022057034
- HjalmarsonAGoldsteinSFagerbergBEffects of controlled-release metoprolol on total mortality, hospitalizations, and well-being in patients with heart failure: The Metoprolol CR/XL Randomized Intervention Trial in congestive heart failure (MERIT-HF). MERIT-HF Study GroupJAMA2000283101295130210714728
- CuffeMSCaliffRMAdamsKFJrShort-term intravenous milrinone for acute exacerbation of chronic heart failure: A randomized controlled trialJAMA2002287121541154711911756
- LeeDAPStukelTAlterDChongAParkerJTuJ“Dose-dependent” impact of recurrent cardiac events on mortality in patients with heart failureAm J Med2009122162.e161e16219100960
- GuglinMRiveroAMatarFGarciaMRenal dysfunction in heart failure is due to congestion but not low outputClin Cardiol201134211311621298655
- MullensWAbrahamsZFrancisGSImportance of venous congestion for worsening of renal function in advanced decompensated heart failureJ Am Coll Cardiol200953758959619215833
- OwanTEHodgeDOHergesRMJacobsenSJRogerVLRedfieldMMTrends in prevalence and outcome of heart failure with preserved ejection fractionN Engl J Med2006355325125916855265
- RubboliASobotkaPAEulerDEEffect of acute edema on left ventricular function and coronary vascular resistance in the isolated rat heartAm J Physiol19942673 Pt 2H1054H10618092270
- ParrinelloGPaternaSDi PasqualePChanges in estimating echocardiography pulmonary capillary wedge pressure after hypersaline plus furosemide versus furosemide alone in decompensated heart failureJ Card Fail201117433133921440872
- IpJECheungJWParkDTemporal associations between thoracic volume overload and malignant ventricular arrhythmias: A study of intrathoracic impedanceJ Cardiovasc Electrophysiol201122329329920946226
- MooreHJPetersMNFranzMRKarasikPESinghSNFletcherRDIntrathoracic impedance preceding ventricular tachyarrhythmia episodesPacing Clin Electrophysiol201033896096620370851