Abstract
Purpose
The aim of this study was to investigate the interobserver agreement of the Lenke and King classifications for adolescent idiopathic scoliosis, and to compare the results of surgery performed based on classification of the scoliosis according to each of these classification systems.
Methods
The study was conducted in Shohada Hospital in Tabriz, Iran, between 2009 and 2010. First, a reliability assessment was undertaken to assess interobserver agreement of the Lenke and King classifications for adolescent idiopathic scoliosis. Second, postoperative efficacy and safety of surgery performed based on the Lenke and King classifications were compared. Kappa coefficients of agreement were calculated to assess the agreement. Outcomes were compared using bivariate tests and repeated measures analysis of variance.
Results
A low to moderate interobserver agreement was observed for the King classification; the Lenke classification yielded mostly high agreement coefficients. The outcome of surgery was not found to be substantially different between the two systems.
Conclusion
Based on the results, the Lenke classification method seems advantageous. This takes into consideration the Lenke classification’s priority in providing details of curvatures in different anatomical surfaces to explain precise intensity of scoliosis, that it has higher interobserver agreement scores, and also that it leads to noninferior postoperative results compared with the King classification method.
Introduction
Idiopathic scoliosis is the most common type of spinal deformity seen in orthopedic clinics. It has a rather insidious onset and shows poor progression and results.Citation1 Adolescent idiopathic scoliosis is a lateral curving of the spine occurring in children aged 10 years and older. It has been shown that 2%–3% of children under 16 years of age suffer from greater than 10° of lateral deviation of the spine; however, deviations greater than 40° have a prevalence rate lower than 0.1%.Citation2 Scoliosis causes trunk asymmetry and leads to disorders of the spinal canal, neurologic disorders, cardiovascular disorders, and osteoarthritis.Citation2,Citation3
Proper recognition and treatment of idiopathic scoliosis helps to optimize patient outcomes. Nearly 10% of scoliosis patients undergo surgical treatment. Idiopathic scoliosis needs to be well recognized and classified to ensure optimal treatment. Patient selection for surgery is based on assessment of the intensity of the disease. Several classification systems have been developed to determine the intensity of adolescent idiopathic scoliosis; these include the Lenke and King classification systems, both of which are well known to orthopedic surgeons. However, because of the existing variability worldwide in setting, patient, and observer or operating surgeon, the available evidence on reproducibility and comparability of these classification systems in making decisions on surgery indications is not adequate, especially for low- and middle-income countries. The aim of this study was to investigate the interobserver agreement of Lenke and King classifications for adolescent idiopathic scoliosis, and to compare the results of surgery performed based on classification of the scoliosis according to each of these classification systems.
Methods
The study was conducted in Shohada Hospital in Tabriz, Iran, between 2009 and 2010. It comprised two parts: first, a reliability assessment was conducted to assess interobserver agreement of the Lenke and King classifications for adolescent idiopathic scoliosis; second, postoperative efficacy and safety of surgery performed based on the Lenke and King classifications were compared.
Forty sets of preoperative radiographs of patients subject to corrective surgery for idiopathic scoliosis in the orthopedic ward of Shohada Hospital were selected for the study. For the first part of the study, three observers, all spine surgeons, classified each of these radiographs independently and according to both the Lenke and the King classifications. The radiograph sets were presented to the observers in a randomized sequence and without personal identifiers. Care was taken to guarantee blind assessment through the erasing of names and identifiers, which were replaced by a code that was added by the research assistant. During the assessment sessions, full description references to both the King and the Lenke classification systems were provided to all three observers. To remove tool variability, the observers used the same type and brand of measurement and marker tools.
For the second part of the study, which was a diagnostic clinical trial, 20 patients who were classified using the Lenke classification method and 20 patients who were classified using the King classification method were followed after surgery. Both groups of patients were treated with Cotrel-Dubousset instrumentation. The technique used was based on that of Dubousset and Cotrel.Citation4 The patients were followed after surgery to assess treatment efficacy and complications.
Data were analyzed using SPSS software (SPSS Inc, Chicago, IL). The agreement among the observers was assessed using kappa coefficients of agreement. Postoperative results were compared using bivariate tests for continuous and dichotomous outcomes as well as repeated measures analysis of variance. A P value less than 0.05 was considered statistically significant.
The regional committee of ethics of the Tabriz University of Medical Sciences approved the study. AA defended the study as the thesis work for a degree of specialty in orthopedics.
Results
Background and interobserver reliability
Of the 40 patients whose radiographs were studied, 16 (40%) were male. The mean age of the participants was 15.3 years (standard deviation [SD] = 2.1). The youngest subject was 12 years of age; the oldest was 21 years of age.
A low to moderate interobserver agreement was observed for the King classification. Kappa coefficients of agreement were 0.16, 0.24, and 0.56 respectively for 1st–2nd, 2nd–3rd, and 1st–3rd observer comparisons (P < 0.05). Regarding the Lenke classification, kappa coefficients of agreement on curve assessment were 0.96, 0.96, and 1 for the three possible paired comparisons of observers (P < 0.05). Kappa coefficients of agreement on kyphosis assessment were complete for 1st–2nd, 2nd–3rd, and 1st–3rd observer comparisons, and kappa coefficients of agreement on coronal curve assessment were similarly above 0.92 for all three paired comparisons of observers (P < 0.05).
Postoperative comparisons
Twenty patients were in the Lenke classification group, and half of these were females. Twenty patients were in the King classification group, and 70% of these were female. The mean age of patients classified through the Lenke classification method was 14.3 years (SD = 1.7), and the mean age of those classified through the King classification method was 16.1 years (SD = 3.1). Detailed classification figures, compared between males and females, are given in .
Table 1 Results of classification systems compared between genders
Surgical complications were encountered in two patients in the Lenke classification group and in three patients in the King classification group. The infectious complications were only surgical wound infections. There were no cases of mortality among the patients classified by the Lenke classification method, compared with two mortal cases in the King classification group. One person in each group needed to undergo another operation. No statistically significant difference was observed in the comparisons mentioned.
shows the comparison of Cobb angle, curve deviation at flexion, and apical rotation between the Lenke and King classifications prior to surgery. Trend of correction in curve deviation and apical rotation over time is given in . Both the difference in measures for gender and their trend over time in both groups were found to be different statistically significant.
Figure 1 Comparison of Cobb angle, curve deviation at flexion, and apical rotation between the Lenke and the King classification systems prior to surgery.
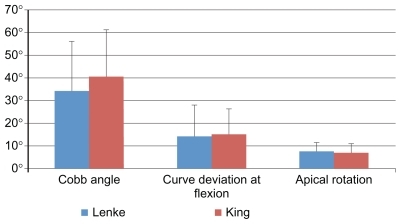
Table 2 Trend of correction in curve deviation and apical rotation (degrees) over time
Cobb angle (as mean plus or minus SD) decreased from 29.6° ± 7.4° to 24.1° ± 6° among male patients (P < 0.001). It decreased from 19.5° ± 4.1° to 13.1° ± 2.7° among female patients (P < 0.001).
Discussion
The present study did not find the surgery outcomes to be different between the two systems. In a study on 44 patients, Lenke et alCitation5 concluded that the Lenke classification method was advantageous. However, in the present study, in case of surgical outcome comparisons, the Lenke classification method was not found to be preferable to the King classification method. Schwab et alCitation6 studied 111 patients for at least 1 year and found that classification modifiers had significant variation (higher rates) in surgical care as the grade of the modifier increased. The present study did not show a statistically significant difference in Cobb angle correction between the two groups; however, both groups showed a reduction of approximately 51% in Cobb angle postoperatively. Using the Lenke classification method, Han et alCitation7 reported a reduction in Cobb angle of 68%, which was a greater improvement than that found in the present study. The infectious complications in the present study were only surgical wound infections, while Xu et alCitation8 reported pleural effusion, mesenteric artery ischemia, wound infection, and loosening of implants. Using the Lenke classification method, Xu et alCitation8 also reported the average postoperative Cobb angle to be approximately 18.5°.Citation8 In the present study, the were no cases of mortality among patients classified by the Lenke classification method, compared with two mortal cases in the King classification group. Although this was not statistically different between groups, the authors consider two cases are too few to provide enough statistical power to defend the similarity. However, this does raise some concern in the use of the King classification method and this should be addressed carefully in future studies.
Other than the role of these classification systems on predicting the surgery outcome, some studies have compared the interobserver reliability of the Lenke classification with that of the King classification. Although postoperative results were not much different, the findings of the present study indicated that the Lenke classification method provided more reliable classifications than the King classification method. compares related studies and shows some controversies in the various reliability assessment results.
Table 3 Conclusions made by studies assessing reproducibility of the King or the Lenke classification method in adolescent idiopathic scoliosis
The present study had some limitations. Although enough statistical power was reached for the first part of the study (reliability), some postoperative outcomes, such as mortality, that were not found to be statistically different between the Lenke and King classification systems in the second part of the study might have suffered lower statistical power. This should be considered when interpreting the results of the second part of the study.
Conclusion
Based on the results, the Lenke classification method seems advantageous. This takes into consideration the Lenke classification method’s priority in providing details of curvatures in different anatomical surfaces to explain precise intensity of scoliosis, that it has higher interobserver agreement scores, and also that it leads to noninferior postoperative results compared with the King classification method.
Disclosure
The authors report no conflicts of interest in this work.
References
- LonsteinJIdiopathic scoliosisLonsteinJBradfordDWinterROgilvieJMoe’s Textbook of Scoliosis and Other Spinal Deformities3rd edPhiladelphiaWB Saunders Co1995219256
- CanaleSCampbell’s Operative Orthopaedics9th edPhiladelphiaMosby1998
- RaggioCLSexual dimorphism in adolescent idiopathic scoliosisOrthop Clin North Am200637455555817141012
- DuboussetJCotrelYApplication technique of Cotrel-Dubousset instrumentation for scoliosis deformitiesClin Orthop Relat Res19912641031101997225
- LenkeLGEdwardsCC2ndBridwellKHThe Lenke classification of adolescent idiopathic scoliosis: how it organizes curve patterns as a template to perform selective fusions of the spineSpine (Phila Pa 1976)20032820S199S20714560193
- SchwabFLafageVFarcyJPSurgical rates and operative outcome analysis in thoracolumbar and lumbar major adult scoliosis: application of the new adult deformity classificationSpine (Phila Pa 1976)200732242723273018007252
- HanIHChinDKKimKSShort segment anterior correction of adolescent idiopathic scoliosisJ Korean Neurosurg Soc2008441525619096658
- XuRMSunSHMaWHAnalysis of complications in scoliosis surgeryZhongguo Gu Shang2008214245248 Chinese19102176
- BehenskyHGiesingerKOgonMMultisurgeon assessment of coronal pattern classification systems for adolescent idiopathic scoliosis: reliability and error analysisSpine (Phila Pa 1976)200227776276711923671
- CummingsRJLovelessEACampbellJSamelsonSMazurJMInterobserver reliability and intraobserver reproducibility of the system of King et al. for the classification of adolescent idiopathic scoliosisJ Bone Joint Surg Am1998808110711119730119
- ShengWBZhengXFGuoHLIntraobserver and interobserver reliability of the King, Lenke, and PUMC classification systems for idiopathic scoliosisZhonghua Yi Xue Za Zhi2009891510471052 Chinese19595255
- LenkeLGBetzRRBridwellKHIntraobserver and interobserver reliability of the classification of thoracic adolescent idiopathic scoliosisJ Bone Joint Surg Am1998808109711069730118
- OgonMGiesingerKBehenskyHInterobserver and intraobserver reliability of Lenke’s new scoliosis classification systemSpine (Phila Pa 1976)200227885886211935109
- QuiGLiQWangYComparison of reliability between the PUMC and Lenke classification systems for classifying adolescent idiopathic scoliosisSpine (Phila Pa 1976)20083322E836E84218923307
- RichardsBSSucatoDJKonigsbergDEOuelletJAComparison of reliability between the Lenke and King classification systems for adolescent idiopathic scoliosis using radiographs that were not premeasuredSpine (Phila Pa 1976)200328111148115612782983