Abstract
Background
The aim of this study was to determine possible correlates of premature ovarian failure (POF) in an Iranian population.
Methods
In a case-control study, 80 patients with POF were compared with 80 controls enrolled from the same setting during 2007–2008. A food diary was used to assess food consumption habits.
Results
Mean age of starting ovarian failure symptoms was 19.3 ± 5.7 years and mean age of menopause was 22.6 ± 6.3 years. Familial coincidence was observed in 16 POF patients versus no one in the control group (P < 0.05). POF patients had lower frequency of both eating red meat and fish when compared with controls (P < 0.001). POF and control subjects consumed similar amounts of dairy products, being 5.3 ± 3.2 times per week in POF and 5.6 ± 2.1 times in the control groups.
Conclusion
In this study, an association between POF and lower red meat or fish consumption was found.
Introduction
Premature ovarian failure (POF) is the occurrence of amenorrhea in conjunction with raised serum follicle stimulating hormone (FSH > 40 IU/L) before the age of 40 years.Citation1 Terminology is inconsistent. Some other terms have been used such as, premature menopause, premature ovarian dysfunction, and primary ovarian insufficiency. It is reported to occur in 0.9%–3.0% of the general female population.Citation2 For every decade before the age of 40, the prevalence of POF is estimated to decrease by a factor of 10. POF is the etiology in 10%–28% of the cases with primary amenorrhea and in 4%–18% of those with secondary amenorrhea.Citation3 POF, other than affecting different aspects of quality of life, may lead to infertility, osteoporosis, and cardiovascular disorders, which puts it on high priority of reproductive and health research.Citation4 Turner syndrome and gonadal dysgenesis are the best known causes of early POF. Nevertheless, in normal 46XX karyotype females presenting with early POF, the etiology is most often unknown.Citation3 There are ethnic differences in prevalence of POF in different populations. Citation5 The ethnic prevalence variations pose possible etiologic differences also due to environmental, genetic, and nutritional factors. Conduction of etiologic studies in different settings or populations can help in improving the knowledge regarding etiology and predictors of POF. The aim of this study was to determine possible correlates of POF in an Iranian population.
Methods
In a case-control study, 80 patients with POF were compared with 80 controls enrolled during 2007–2008. Study setting was Alzahra University Hospital and Tabriz Subspecialty Clinic for Infertility. Cases were menopause women under the age of 40, referred to the study centers. All the cases had referred due to amenorrhea and infertility and were assessed two times for serum FSH; they were assessed for POF if FSH was found to be above 30 U/L. Eighty patients lacking the outcome of interest were also enrolled as controls.
Food consumption variables were measured using a food diary assessment tool, measuring average frequency of consumed food. Controls were selected from other clinics of Alzahra University Hospital. They were matched with cases for age using a frequency matching technique.
Data were entered into the computer and analyzed using bivariate statistical tests as well as multivariate regression analysis. All the test results were interpreted as two-tailed results, and a P value < 0.05 was considered as statistically significant.
The study protocol was approved by the regional committee of ethics in Tabriz University of Medical Sciences.
Results
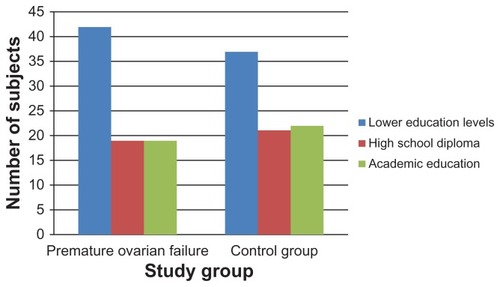
Mean (and standard deviation) of the age of the patients were 30.3 (5.9) and 30 (5.6) years, respectively, for the POF and control groups (P = 0.3). Eighty-five percent of POF and 76% of control group subjects had urban residence (P = 0.2). Education level distribution compared between groups was not statistically significant ().
Figure 1 Distribution of education level compared between primary ovarian failure group and control group subjects.
Mean age of starting ovarian failure symptoms was 19.3 ± 5.7 years, and mean age of menopause was 22.6 ± 6.3 years. In 26 patients in this group, menstruations continued dependent on drug treatment. Maternal menopausal age, if reached, was 45.0 ± 3.8 years in the POF group versus 46.6 ± 3.3 years in the control group (P < 0.05). Mean age of menarche was 13.9 ± 2.0 years for the POF group and 13.6 ± 1.2 years in the control group. The difference was not statistically significant. A history of lifelong irregular menstruation was reported in 76.3% of participants in the POF group, while no one reported an irregular menstruation history in the control group (P < 0.001). Seven patients in the POF group had a history of ovarian surgery. The surgery type was cystectomies in five patients and cauterization in two cases. Mumps history was reported in 16 POF versus 25 control participants. The difference was not statistically significant. Familial coincidence was observed in 16 POF patients versus no one in the control group (P < 0.05). Familial marriage of the parents was the case in 23 and 30 subjects in POF and controls, respectively. The difference was not found to be statistically significant. None of the patients in either group had a history of radiotherapy or chemotherapy. Only four patients in the POF group reported history of renal disease (P = 0.1). Diabetes, thyroidal disease, lupus erythematous, and rheumatoid arthritis didn’t exist in any of the participants of the study groups.
POF patients had lower frequency of consuming both red meat and fish compared with controls (P < 0.001). POF patients had a mean 2.8 times of red meat consumption and 0.23 times of fish consumption per week. Controls had a mean 4.6 times of red meat consumption and 1.37 times of fish consumption per week. Vegetable consumption as reported by the POF patients had a mean of 3.1 ± 2.2 times per week. Mean weekly consumption of vegetables was recorded to be 3.5 ± 3.3 times per week among controls. The difference was not statistically different. POF patients consumed mean 0.4 times of fast foods per week. The figure was 0.5 times per week for controls (P = 0.3). POF and control subjects consumed similar amounts of dairy products, being 5.3 ± 3.2 times per week in the POF group and 5.6 ± 2.1 times in the control group (P = 0.5). Also, living close to high voltage power posts, living close to industrial centers, and using mobile phones were not found to be associated with POF (P values were 0.210, 0.444, and 0.200, respectively). None of the participants were smokers.
Using multivariate regression analysis, the amount of weekly consumption of red meat and fish appeared as independent predictors of POF.
Discussion
Some of the possible predictors of POF were not found significant. This is possibly due to lower incidence and compared variability between groups. For example, contrary to many foreign studies, smoking is rare among women in this context and there were no smokers in either group, so the study could not investigate an association between smoking and POF. No doubt, in cases where there is a lack of variation as in the present study, the factors will be classed as insignificant. Nevertheless, smoking is repeatedly reported to be associated with POF.Citation6–Citation10 In the present study, a history of irregular menstruation was found to be strongly associated with POF. This was in line with a large Italian study reporting that the risk of POF and of early menopause was higher among women reporting lifelong irregular menstrual cycles.Citation11 The present study was a case-control study, and the Italian study was cross-sectional study; however, due to lack of clear-cut temporality assessment, in both cases, caution needs to be taken in interpreting the results. Considering this point and also lack of a reasonable biological plausibility to explain a direct causality association, it cannot be clarified with certainty whether irregular menstrual cycles can be considered as a risk factor, a predisposing factor, or even an early symptom of POF.Citation12 Nevertheless, some studies have also supported lack of an association between irregular menstrual cycles and ovarian failure.Citation13 Due to such an uncertainty, the authors of the present paper preferred to assess and discuss the association just through a bivariate analysis rather than including it in multivariate analysis.
There was no association found between age at menarche and POF that was consistent with the results of the Italian study, but controversial results can also be retrieved from literature.Citation11,Citation14,Citation15 As in the present study, insufficient or no cases of ovarian surgery, chemotherapy, or radiotherapy existed to investigate existence of association between these factors and POF. However, such an association seems quite plausible and is also reported in previous studies.Citation16–Citation18 Although the present study was not supported to do genetic assessments, family clustering of disease was a significant finding. Although preferential recall of family history by women with early menopause could contribute to the association between family history and early menopause observed in this study, a genetic factor is also plausible, including partial deletions of the X chromosome, compatible with the deficiency of male siblings in cases with family history of early menopause.Citation19 A hereditary or genetic link to POF is well discussed and substantially supported in previous POF literature.Citation20–Citation24
Interestingly, in the present study there was an association between POF and lower red meat or fish consumption. If we consider this to be a possible causal effect, the mechanism may be sought in dietary amino acid balance, minerals such as zinc in all of kinds of meat, omega fatty acids in fish, and other potential mechanisms. However, a major confounder in this regard is the economic level,Citation25,Citation26 which is very difficult to measure and control for in developing countries and is recommended to be considered in future research.
Disclosure
The authors report no conflicts of interest in this work.
References
- CoulamCBAdamsonSCAnnegersJFIncidence of premature ovarian failureObstet Gynecol19866746046063960433
- FalsettiLScalchiSVillaniMTBugariGPremature ovarian failureGynecol Endocrinol199913318919510451811
- KokcuAPremature ovarian failure from current perspectiveGynecol Endocrinol201026855556220500113
- AnastiJNPremature ovarian failure: an updateFertil Steril19987011159660412
- NippitaTABaberRJPremature ovarian failure: a reviewClimacteric2007101112217364600
- LuotoRKaprioJUutelaAAge at natural menopause and sociodemographic status in FinlandAm J Epidemiol1994139164768296776
- CramerDWHarlowBLXuHFraerCBarbieriRCross-sectional and case-controlled analyses of the association between smoking and early menopauseMaturitas199522279878538488
- NilssonPMollerLKosterAHollnagelHSocial and biological predictors of early menopause: a model for premature agingJ Intern Med199724242993059366808
- HarlowBLSignorelloLBFactors associated with early menopauseMaturitas20003513910802394
- CooperGSSandlerDPBohligMActive and passive smoking and the occurrence of natural menopauseEpidemiology199910677177310535795
- Premature ovarian failure: frequency and risk factors among women attending a network of menopause clinics in ItalyBJOG20031101596312504937
- ChangSHKimCSLeeKSPremenopausal factors influencing premature ovarian failure and early menopauseMaturitas2007581193017531410
- TestaGChiaffarinoFVegettiWCase-control study on risk factors for premature ovarian failureGynecol Obstet Invest2001511404311150874
- ParazziniFNegriELaVCReproductive and general lifestyle determinants of age at menopauseMaturitas19921521411491470046
- BrombergerJTMatthewsKAKullerLHWingRRMeilahnENPlantingaPProspective study of the determinants of age at menopauseAm J Epidemiol199714521241339006309
- WeinsteinLSLiuJSakamotoAXieTChenMMinireview: GNAS: normal and abnormal functionsEndocrinology2004145125459546415331575
- HoekASchoemakerJDrexhageHAPremature ovarian failure and ovarian autoimmunityEndocr Rev19971811071349034788
- SantoroNResearch on the mechanisms of premature ovarian failureJ Soc Gynecol Investig200181 SupplS10S12
- CramerDWXuHHarlowBLFamily history as a predictor of early menopauseFertil Steril19956447407457672145
- RizzolioFBioneSSalaCChromosomal rearrangements in Xq and premature ovarian failure: mapping of 25 new cases and review of the literatureHum Reprod20062161477148316497693
- PrueittRLRossJLZinnARPhysical mapping of nine Xq translocation breakpoints and identification of XPNPEP2 as a premature ovarian failure candidate geneCytogenet Cell Genet2000891–2445010894934
- DavisonRMFoxMConwayGSMapping of the POF1 locus and identification of putative genes for premature ovarian failureMol Hum Reprod20006431431810729312
- GoswamiDConwayGSPremature ovarian failureHorm Res200768419620217495481
- CordtsEBChristofoliniDMDos SantosAABiancoBBarbosaCPGenetic aspects of premature ovarian failure: a literature reviewArch Gynecol Obstet2011283363564321188402
- TorgersonDJAvenellARussellITReidDMFactors associated with onset of menopause in women aged 45–49Maturitas199419283927968648
- van NoordPADubasJSDorlandMBoersmaHte VeldeEAge at natural menopause in a population-based screening cohort: the role of menarche, fecundity, and lifestyle factorsFertil Steril1997681951029207591