
Abstract
Objective
The present study aims to discuss the clinical characteristics, factors, and treatment methods affecting the prognosis in patients with severe radiation pneumonia (RP).
Methods
The radiotherapy status, clinical features, imaging characteristics, laboratory examination results, treatment methods, and prognoses of 34 patients with severe RP treated in our department between January 2011 and July 2017 were retrospectively analyzed. The severe RP grading was based on the Common Terminology Criteria for Adverse Events version 4.0; patients who scored Grade ≥3 were considered to have a severe case of RP.
Results
The results of the present study showed that 22 patients had lung cancer, 6 had esophageal cancer, 5 had breast cancer, and 1 had colon cancer with lung metastasis. The total radiation dose was 37.5–66 Gy, and the overall average dose was 53 Gy; the average dose in the patients who died was 52.9 Gy. A total of 28 patients presented with a cough and sputum as the initial symptom, and 24 presented with wheezing as an accompanying symptom; of the 24 patients, 8 experienced fever, 2 experienced wheezing as the only symptom, 1 had chest pain, and 1 had chest tightness. In 26 patients, the changes were in the radiation field, and in 8 cases, the changes appeared both inside and outside the radiation field. After the use of glucocorticoid methylprednisolone, respiratory support, and anti-infection treatment, 18 patients were cured, 8 showed a condition improvement, and 8 died.
Conclusion
The prognosis of severe RP was not significantly correlated with the administered radiation dose; however, lung cancer, a high Acute Physiology and Chronic Health Evaluation score, and delayed diagnosis were risk factors for patient death. However, a combination of antibiotic therapy, ventilator-assisted respiration, and steroid therapy could improve patient prognosis.
Keywords:
Introduction
Radiotherapy is an important treatment method for lung cancer and other thoracic tumors. Radiation pneumonia (RP) is a common complication of this treatment, with an incidence rate of 5–15% in China.Citation1 Patients with mild cases of RP who undergo timely treatment have a good prognosis; however, 5–11.7% of patients who develop RP have severe cases of the diseaseCitation1–Citation3 (ie, the patients have a high mortality and are prone to developing pulmonary fibrosis,Citation4 which affects radiotherapy implementation and can seriously threaten their safety). Radiotherapy, administered either alone or in combination with chemotherapy, helps control tumor growth and prolong patient survival. However, the use of radiotherapy in the treatment of lung cancer and lung metastases can cause injury to healthy lung tissue while killing the tumor.
The majority of RP cases are mild and have a good prognosis. Atsuya Takeda reported a 95% incidence of Grade ≤2 RP, with only a 5% incidence of severe RP.Citation3 However, the mortality of patients with severe RP can reach as high as 50% within two months.Citation4 Hideomi Yamashita reported a 77.8% mortality rate among 9 cases with Grade ≥4 RP (7/9 patients died).Citation5 Other studies on radiotherapy-induced RP have been conducted; however, the relevant medical records mainly focus on patients with mild RP. Only a few studies have been conducted on patients with severe RP. Several well-established pneumonia and sepsis biomarkers, including the monocyte distribution width and the respective presepsin and mid-regional proadrenomedullin levels, have been studied.Citation6–Citation9 There is also a lack of reported studies including a comparison of patients with lung cancer and patients without lung cancer. A total of 34 patients with severe RP admitted to our hospital department between January 2011 and July 2017 were included in the present study.
Materials and Methods
General Information
A total of 34 (24 male and 10 female) consecutive patients with severe RP treated in our department between January 2011 and July 2017 were enrolled in the present retrospective study. The patients were aged 43–81, with an average age of 62.9 ± 10.6 years. Of the patients, 22 had lung cancer, 6 had esophageal cancer, 5 had breast cancer, and 1 had colon cancer with lung metastasis. All patients had complete clinical hospitalization data, and the tumor diagnosis was pathologically confirmed in each patient. The patients attended follow-ups after discharge; the follow-up duration was 1–42 months.
Inclusion criteria: All patients diagnosed with RP based on the diagnostic criteria of the Expert Consensus on the Diagnosis and Treatment of Radiation Lung Injury.Citation5 Patients diagnosed with Grade ≥3 RP were considered to be severe cases. The patient grading was based on whether or not the patients had Grade ≥3 RP at the time of admission to our department or subsequent progression to Grade ≥3.
Exclusion criteria: patients who gave up treatment after diagnosis.
Diagnostic Criteria
The diagnosis of RP was based on the Expert Consensus on the Diagnosis and Treatment of Radiation Lung Injury diagnostic criteria;Citation5 the RP was then graded in accordance with the Common Terminology Criteria for Adverse Events (CTCAE) 4.0.Citation6 (1) Grade 0: no significant differences in symptoms and signs compared with before treatment; (2) Grade 1: a slight cough and shortness of breath at exertion; (3) Grade 2: persistent cough with the need for narcotic cough suppressant, accompanied by dyspnea at slight exertion (disappears at rest); (4) Grade 3: severe cough unresponsive to narcotic cough suppressants, accompanied by shortness of breath at rest and clinical or radiographical confirmation of acute pneumonia, with the possible need for intermittent oxygen inhalation or corticosteroids; and (5) Grade 4: severe respiratory insufficiency with the need for continuous oxygen inhalation or assisted ventilation. All patient diagnoses were consistent with RP. Patients diagnosed with Grade ≥3 RP were considered to be severe cases.Citation4,Citation7 The patient grading was based on whether or not the patients had Grade ≥3 RP at the time of admission to our department or subsequent progression to Grade ≥3.
Evaluation of Therapeutic Effects
The therapeutic effect on RP was evaluated in accordance with the Criteria For Cure And Improvement Of Clinical Disease Diagnostic Basis (second edition).Citation8 A cured patient was defined as having experienced the disappearance of symptoms and signs, along with the dissipation of chest lesions (chest X-ray). Criteria improvement was defined as reductions in coughing and shortness of breath as well as the gain of basic control over secondary respiratory infections. The patient death criteria were (1) condition deterioration; and (2) death.
Clinical Data Collection
General characteristics before and after radiotherapy: (1) whether or not chemotherapy was conducted; (2) whether or not there existed a fundamental disease; and (3) the total radiation dose. General patient characteristics at the severe RP diagnosis time: (1) severe RP onset time; (2) symptoms after radiotherapy and their time of occurrence; (3); the relevant examinations and their results (4) changes in chest imaging as well as ultrasensitive C-reactive protein, blood leukocyte, procalcitonin, and lactate dehydrogenase levels, fungal G test and fungal GM test results, and other infection indicators; (5) sputum and alveolar lavage fluid culture results; and (6) the respective oxygen inhalation and oxygen partial pressure concentrations. Treatment conditions: (1) respiratory support; and (2) antibiotic and methylprednisolone doses. Patient survival follow-up: each patient was followed up with until either October 2017 or the time of death.
Statistical Methods
The Statistical Package for Social Sciences 22.0 was adopted for data analysis, and the dependent sample t-test was used for the measurement data evaluation (expressed as x ± s [mean ± SD]). The countable data were expressed in percentage, and a p value of <0.05 was considered statistically significant.
Results
Clinical Characteristics
As stated previously, 34 patients were enrolled in the present study, which had an average follow-up duration of 6 months (1–42 months). The patients’ general conditions are shown in . Among the patients, there were 24 males and 10 females. The age ranged between 43 and 81, with an average age of 62.9 ± 10.6. There were 22 cases with lung cancer (5 with adenocarcinoma, 8 with squamous cell carcinoma, 7 with small cell carcinoma, and 2 with adenosquamous carcinoma), 6 cases with esophageal cancer, 5 cases with breast cancer, and 1 case with colon cancer with lung metastasis. Moreover, 3 patients had chronic obstructive pulmonary disease, 1 patient had chronic bronchitis, 2 patients had emphysema and pulmonary bullae, 1 patient had bronchiectasis, 10 patients had cardiovascular disease, and 6 patients had type 2 diabetes mellitus. The total radiation dose was between 37.5 and 66 Gy, and the overall average dose was 53 Gy; the average dose for the dead patients was 52.9 Gy. Here, 2 patients underwent radiotherapy and chemotherapy simultaneously, 22 patients had chemotherapy before radiotherapy, and 10 patients did not have chemotherapy. The chemotherapeutic agents used included pemetrexed, cisplatin, etoposide, cyclophosphamide, docetaxel, paclitaxel, nedaplatin, irinotecan, cetuximab, eflornithine, and epirubicin. There were 20 cases with Grade 3 and 14 cases with Grade 4 according to CTCAE 4.0. Additionally, as the initial symptom, 28 patients had cough and sputum, 2 patients had wheezing, and 2 had fever. Finally, 24 patients had wheezing as the accompanying symptom with the initial symptom, and 8 had fever, 1 had chest pain, 1 had chest tightness, and 2 had wheezing as the only symptom.
Table 1 General Conditions of Patients with Severe Radiation Pneumonia
Laboratory Examinations
Klebsiella pneumoniae, Streptococcus pneumoniae, Pseudomonas aeruginosa, Stenotrophomonas maltophilia, Acinetobacter baumannii, Enterobacter cloacae, Staphylococcus haemolyticus, Staphylococcus epidermidis, Enterococcus faecium, Candida albicans, Candida glabrata, Candida tropicalis, Candida guilliermondii, and Aspergillus flavus were detected in the patients’ sputum. A total of 20 patients underwent bronchoscopy, with little secretion under microscopy. Pseudomonas aeruginosa, Klebsiella pneumoniae, Stenotrophomonas maltophilia, Enterobacter cloacae, Achromobacter xylosoxidans, Candida albicans, Candida glabrata, and Aspergillus versicolor were cultured in the alveolar lavage fluid, in which the neutrophil percentage was between 50% and 95% and the lymphocyte percentage between 5% and 35%. The sputum culture and alveolar lavage fluid culture results are illustrated in .
Table 2 Sputum and Alveolar Lavage Fluid Culture Results of Severe Radiation Pneumonia
Image Examinations
All 34 cases had lesions in the radiation field, while 8 also had lesions outside the radiation field. There were 15 cases with ground-glass opacity and 19 cases with consolidation opacity in the images. Four cases had pleural effusion, and one case developed pneumothorax (–).
Figure 1 (A) The bronchial mucosa of the left lung’s upper lobe was red and moist, with no obvious secretion, congestion, or edema. (B) The bronchial mucosa of the right lung’s lower lobe was red and moist, with no obvious secretion, congestion, or edema.
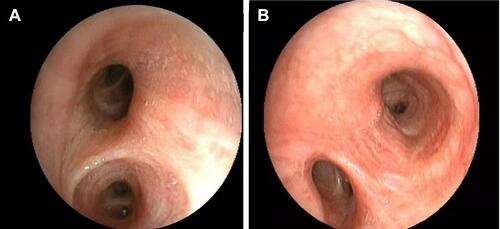
Figure 2 (A) The lower left lung consolidation using an air bronchogram. (B) Ground-glass opacity and mesh opacity of the right lung and the left lung. (C) Ground-glass bilateral lung opacity, with left pleural effusion. (D) Ground-glass opacity, mesh opacity, and pleural effusion of the right lung.
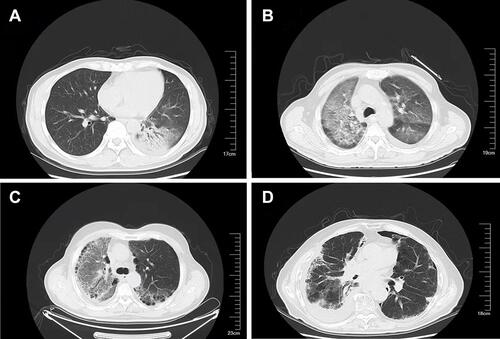
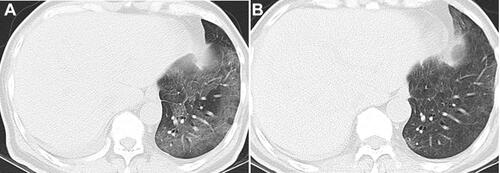
Figure 3 (A) The daily administration of 40 mg methylprednisolone was ineffective. (B) After changing to a daily dose of 80 mg methylprednisolone, the patient’s oxygenation level improved, and the inflammation was absorbed. Upon decreasing the dose to 40 mg methylprednisolone again, the inflammation recurred.
Treatment and Prognosis
Oxygen inhalation was conducted in 20 cases, and 10 cases had non-invasive ventilator assistance. Four cases experienced no improvement in symptoms after both treatments and were given tracheal intubation and ventilator-assisted respiration. Steroid therapy was conducted in all patients, with a dose between 40 and 80 mg per day. Methylprednisolone therapy was conducted in all patients as well. Among the patients, 18 cases were cured, 8 cases improved, and 8 cases died, of which 7 had lung cancer and 1 had esophageal cancer. A comparison of the results of the survival group and the death group is demonstrated in . Eight of 21 culture-negative patients died, while six of 24 culture-negative patients died.
Table 3 Comparison of the Survival and Dead Groups
Discussion
Our hospital is a general hospital specializing in oncology. Among others, it has an independent lung cancer department, breast cancer department, lymphoma department, and gastrointestinal tract tumor department. Every year, many patients with tumors need to undergo radiotherapy, resulting in a high number of patients with RP. Patients with mild RP are mostly managed by the radiotherapy department, while patients with severe RP often require ventilator-assisted respiration and visit our department.
Generally, RP appears in the radiation field; however, in certain patients, it can also appear outside the radiation field. In the present study, 8/34 patients had an RP appearance both inside and outside the radiation field, which was much higher than the ordinary RP appearance rate. The simultaneous appearance of lesions in the bilateral lungs might also be a cause of severe RP. The present study included a case of radiotherapy-induced RP following the treatment of wandering-form lung cancer. During the methylprednisolone reduction, the patient developed new exudative opacity in the lung. The exudative lesion in the lung was reabsorbed again upon restoration of the original methylprednisolone dose; this has not been previously reported in relevant literature. On the one hand, it is possible that this was correlated with radiation leakage; on the other hand, it might have been due to inflammatory signal diffusion.Citation10
Although RP is an aseptic inflammatory disease, patients with severe RP are prone to lung co-infection. A review of relevant literature failed to find a reports pathogenic RP bacteria. In the present study, sputum and/or alveolar lavage fluid were obtained from all patients for culturing. The results showed 25 microorganism cases as well as 9/21 cases of microorganisms with tracheoscopy among the 34 sputum specimens.
However, the tracheoscopy findings show that patient secretion was minimal, and the ultrasensitive C-reactive protein, calcitoninogen, and leukocyte levels were primarily within the normal range. Thus, the presence of infection or colonization was unclear. The main pathogens were Gram-negative bacteria and fungi. In particular, the alveolar lavage fluid results suggested that the pathogens were all Gram-negative bacteria and fungal infections. Moreover, none of the alveolar lavage fluid cultures showed a presence of Gram-positive bacteria, suggesting that Gram-negative and fungi pathogens should be covered in the initial treatment of patients with severe RP.
As 24 of the patients were treated with synchronous chemotherapy before and during radiotherapy and 10 were not treated with chemotherapy, it is possible that synchronous chemotherapy aggravates RP occurrence. Arrieta et alCitation11 found that radiotherapy with a simultaneous administration of gemcitabine and carboplatin increases RP incidence in patients with locally advanced non-small-cell lung cancer.
Patients with lowered lung function or emphysema were previously considered to be more likely to develop RP;Citation2 however, recent studies have shown that there is not an increased RP incidence among patients with low lung function. This is possibly due to the lower oxidative stress caused by the poor oxygenation in such patients. Additionally, 32% of patients with interstitial pulmonary disease had Grade ≥3 RP, as opposed to patients with non-interstitial pulmonary disease, of whom only 2% had Grade ≥3 RP. Moreover, with the development of RP, patients with interstitial pulmonary disease had a 21% mortality rate.Citation12
In their study, Wang et alCitation4 reported that 31 patients with non-small-cell lung cancer had a mortality of 50% after two months of severe RP. Moreover, 4 patients with Grade 3 RP as reported by Xu et alCitation13 died on days 2, 28, 48, and 62 after the diagnosis. In our department, the mortality rate was 31% among patients with small-cell lung cancer presenting with severe RP and 57.1% in patients with Grade 4. All 3 patients with lung cancer requiring tracheal intubation died. The patient mortality rate in our department was lower than the mortality rate reported in relevant literature; this is possibly correlated with the widespread use of mechanical ventilation, especially non-invasive ventilation, which may help patients survive respiratory failure and gain time for steroid therapy and anti-infection treatment.
The steroid therapy dose and duration are unclear; the usual recommended dose is 40 mg of prednisone daily;Citation14–Citation20 no distinction is made between patients with mild RP and patients with severe RP. In the present study, one patient with lung cancer and severe RP who was administered a daily dose of 40 mg methylprednisolone gradually deteriorated; however, his/her condition improved significantly with the daily administration of 80 mg methylprednisolone. When the dose was reduced to 40 mg/day, his/her condition was aggravated again. Treatment experience is usually gained from treating patients with mild disease cases; however according to our experience, the initial methylprednisolone dose should be 80 mg/day in the presence of severe RP in order to achieve a higher success rate.
Generally, cases of RP in China are reported by radiologists; there have been few cases reported by respiratory physicians. Even fewer of these cases have been severe. The mortality rate of the patients with severe RP admitted to our department was lower than the rate reported in relevant literature; this may be correlated with patient ventilator treatment in the respiratory critical care unit.
The use of methylprednisolone is an effective in-patient treatment. Based on the results of the present study, aggressive antibiotic therapy and mechanical ventilation in addition to methylprednisolone administration could reduce patient mortality. According to previous related literature and expert consensuses, there is no recommendation for anti-infection treatment for infections accompanying RP. Based on the sputum culture and bronchoscopy results, it is suggested that Gram-negative bacteria and fungi should be covered and if necessary, Gram-positive organisms targeted in the treatment of severe RP.
The limitations of the present study: (1) the dependent sample t-test was used for the evaluation of dependent data, while the potential risk factors were investigated through the comparison of the survival patient group and the dead patient group; these results were not compared between patients with lung cancer and patients without lung cancer; and (2) the case number is too limited to show significant findings. Microbiological findings need to be made in future studies in order to gain useful information.
In summary, the prognosis of severe RP is not significantly correlated with the administered radiation dose. Patients with lung cancer have a high mortality rate, while patients with other diseases who also present with severe RP have a good prognosis. Delayed diagnosis and a high Acute Physiology and Chronic Health Evaluation score increase patient mortality. Patients with severe RP are prone to co-infection or colonization with Gram-negative bacteria and fungi. A combination of antibiotic therapy, ventilator-assisted respiration, and steroid therapy could improve the prognosis. Due to the currently poor therapeutic effect on severe RP in patients with lung cancer, preventing RP occurrence is particularly important. Patients undergoing radiotherapy should be selected, and in the case of severe RP, promptly transferred to experienced departments for further treatment in order to avoid pneumonia aggravation or even the occurrence of life-threatening conditions.
Ethics Statement
This study was conducted with the approval of the Strategic Support Force Medical Center ethics committee and in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Disclosure
The authors report no conflicts of interest in this work.
References
- Robnett TJ, Machtay M, Vines EF, McKenna MG, Algazy KM, McKenna WG. Factors predicting severe radiation pneumonitis in patients receiving definitive chemoradiation for lung cancer. Int J Radiat Oncol Biol Phys. 2000;48(1):89–94. doi:10.1016/S0360-3016(00)00648-9
- Shi A, Zhu G, Wu H, Yu R, Li F, Xu B. Analysis of clinical and dosimetric factors associated with severe acute radiation pneumonitis in patients with locally advanced non-small cell lung cancer treated with concurrent chemotherapy and intensity-modulated radiotherapy. Radiat Oncol. 2010;5:35.
- Takeda A, Ohashi T, Kunieda E, et al. Early graphical appearance of radiation pneumonitis correlates with the severity of radiation pneumonitis after stereotactic body radiotherapy (SBRT) in patients with lung tumors. Int J Radiat Oncol Biol Phys. 2010;77(3):685–690. doi:10.1016/j.ijrobp.2009.06.001
- Wang JY, Chen KY, Wang JT, et al. Outcome and prognostic factors for patients with non-small-cell lung cancer and severe radiation pneumonitis. Int J Radiat Oncol Biol Phys. 2002;54(3):735–741. doi:10.1016/S0360-3016(02)02994-2
- Wang LH, Fu XL, Chen M, et al. Diagnosis and treatment of radioactive lung injury. Chin J Radiat Oncol. 2015;24:4–9.
- Ciaccio M, Fugardi G, Titone L, et al. Procalcitonin levels in plasma in oncohaematologic patients with and without bacterial infections. Clin Chim Acta. 2004;340(1–2):149–152. doi:10.1016/j.cccn.2003.10.014
- Agnello L, Bivona G, Parisi E, et al. Presepsin and midregional proadrenomedullin in pediatric oncologic patients with febrile neutropenia. Lab Med. 2020;51(6):585–591. doi:10.1093/labmed/lmaa011
- Bellia C, Agnello L, Lo Sasso B, et al. Mid-regional pro-adrenomedullin predicts poor outcome in non-selected patients admitted to an intensive care unit. Clin Chem Lab Med. 2019;57(4):549–555. doi:10.1515/cclm-2018-0645
- Agnello L, Lo Sasso B, Vidali M, et al. Validation of monocyte distribution width decisional cutoff for sepsis detection in the acute setting. Int J Lab Hematol. 2021. doi:10.1111/ijlh.13496
- Oh YT. Radiation induced lung damage: mechanisms and clinical implications. J Lung Cancer. 2008;9(7).
- Arrieta O, Gallardo-Rincón D, Villarreal-Garza C, et al. High frequency of radiation pneumonitis in patients with locally advanced non-small cell lung cancer treated with concurrent radiotherapy and gemcitabine after induction with gemcitabine and carboplatin. J Thorac Oncol. 2009;4(7):845–852. doi:10.1097/JTO.0b013e3181a97e17
- Wang J, Cao J, Yuan S, et al. Poor baseline pulmonary function may not increase the risk of radiation-induced lung toxicity. Int J Radiat Oncol Biol Phys. 2013;85(3):798–804. doi:10.1016/j.ijrobp.2012.06.040
- Xu HM, Cao JZ, Wang JB, et al. Management and outcome of symptomatic radiation induced lung injury in non-small cell lung cancer. Chin J Radiat Oncol. 2013;22:201–204.
- Sekine I, Sumi M, Ito Y, et al. Retrospective analysis of steroid therapy for radiation-induced lung injury in lung cancer patients. Radiother Oncol. 2006;80(1):93–97. doi:10.1016/j.radonc.2006.06.007
- Hanania AN, Mainwaring W, Ghebre YT, Hanania NA, Ludwig M. Radiation-induced lung injury: assessment and management. Chest. 2019;156(1):150–162. doi:10.1016/j.chest.2019.03.033
- Bledsoe TJ, Nath SK, Decker RH. Radiation pneumonitis. Clin Chest Med. 2017;38(2):201–208. doi:10.1016/j.ccm.2016.12.004
- Iovine E, Nenna R, Bloise S, et al. Lung ultrasound: its findings and new applications in neonatology and pediatric diseases. Diagnostics (Basel). 2021;11(4):652. doi:10.3390/diagnostics11040652
- Mummudi N, Jiwnani S, Niyogi D, et al. Salvage radiotherapy for postoperative locoregional failure in esophageal cancer: a systematic review and meta-analysis. Dis Esophagus. 2021;doab020. doi:10.1093/dote/doab020
- Xue N, Zhou R, Deng M, et al. High serum superoxide dismutase activity improves radiation-related quality of life in patients with esophageal squamous cell carcinoma. Clinics (Sao Paulo). 2021;76:e2226. doi:10.6061/clinics/2021/e2226
- Tzilas V, Poletti V, Bouros D. Reversed halo sign in radiation induced organizing pneumonia: natural course of the underlying pathophysiology. Pulmonology. 2021. S2531-0437(21)00008-8. doi:10.1016/j.pulmoe.2020.12.015