
Abstract
Purpose
Observational studies have examined the association between antipsychotics and ischemic heart disease (IHD) in general populations, but results did not take into account other comorbid diseases, such as Parkinson’s disease (PD). This study investigates the one-year risk of IHD, all cardiovascular events, and all-cause mortality among newly diagnosed PD patients who used antipsychotics compared to non-users.
Materials and Methods
This study included individuals aged 40 years or older with a first definitive PD diagnosis Read Code in the Secure Anonymised Information Linkage (SAIL) databank who had been initiated on any PD medication between 2000 and 2016. Antipsychotic users were matched 1:1 with non-users by a propensity score model to control the confounding effects of patients’ demographics, social deprivation status, comorbidities, and medication history. Cox regression was performed to calculate the hazard ratios (HR) and 95% CIs for the association between antipsychotics and study outcomes.
Results
A total of 1837 participants were included in the analysis. Users of first-generation antipsychotics (FGA) were significantly more likely to develop IHD compared to non-users, with an HR of 2.60 (95% CI 1.103–6.167). Among the FGAs, haloperidol had the highest likelihood of IHD developing, with an HR of 3.01 (95% CI 1.038–8.729). Any use of antipsychotics, regardless of whether they were FGA or second-generation antipsychotics (SGA), was linked to all-cause mortality, with an HR of 4.201 (95% CI 3.272–5.394). When subdividing antipsychotics into FGAs and SGAs, mortality was more likely in FGA users, with an HR of 7.557 (95% CI 5.633–10.139). Mortality also occurred in SGA users, but with a lower HR of 3.278 (95% CI 2.509–4.282).
Conclusion
FGAs were associated with an increased risk of IHD and all-cause mortality in newly diagnosed PD patients with psychosis. This finding emphasizes the need to use antipsychotics with caution in PD patients with psychosis.
Introduction
Studies have suggested that Parkinson’s disease (PD) patients are more likely to develop cardiovascular disease compared to patients without PD.Citation1 Ischemic heart disease (IHD), in particular, is more common in PD patients compared to non-PD patients, especially in the presence of other cardiac risk factors, such as a high lipid profile, smoking, and hypertension.Citation2–Citation4 Although a recent systematic review found no association between IHD and PD, the review concluded that other cardiovascular events, such as stroke, have such an association.Citation1 However, this should not exclude IHD and other cardiovascular risks in PD patients, given that other factors can impact this association, such as the cardiac side effects of some PD medications (eg, dopamine agonists),Citation5,Citation6 and the use of antidepressants and antipsychotics in PD patients.Citation7,Citation8
It is estimated that the prevalence of psychotic episodes in PD patients could reach 40%Citation9 and antipsychotics are frequently used to treat these episodes. A Canadian study found that the cumulative incidence of antipsychotics used in PD patients was 35% at 7 years,Citation10 while in a Taiwanese study the cumulative incidence was 51% at 6 years.Citation11 However, the high consumption of antipsychotics is not without risk. In 2005, the US Food and Drug Administration (FDA) released a letter linking the use of SGAs to the risk of death in dementia patients.Citation12 In 2008, the FDA letter was extended and linked the use of FGAs to higher mortality rates in dementia patients.Citation13 Recently, the use of antipsychotics has been linked to higher mortality and morbidity rates in PD patients.Citation14–Citation16
Antipsychotics are well known for their significant psychological, autonomic, metabolic, and cardiovascular side effect profile.Citation17 IHD is one of the side effects found to be linked to the use of antipsychotics in the general population.Citation18,Citation19 In vivo and in vitro pharmacological studies suggested that the link between antipsychotics and cardiovascular side events is possibly due to the metabolic side effects of antipsychotics,Citation20 blockade of dopamine type 3 receptors,Citation21 defect in cardiovascular and immunological factors such as brain derived neurotrophic factor (BDNF) and platelet derived growth factor receptor (PDGFR)-beta,Citation22 altered cardiac mitochondrial oxygen consumption,Citation23 or immunosuppression and leukocyte accumulation in the arterial wall.Citation24 However, this link has not been epidemiologically confirmed. Two meta-analyses showed contradictory results regarding the link between IHD and antipsychotics. Papola et al examined nine observational studies and concluded that antipsychotics were associated with IHD,Citation19 whereas Rotella et al found there was no significant association.Citation8 Schizophrenia in the general population was the main focus of most studies included in these meta-analyses, with no stratification based on other concurrent comorbidities.Citation8 However, there is evidence that antipsychotics are linked to cardiovascular events in diseases that might be related to PD patients, such as dementia,Citation25,Citation26 but no study examined such a link directly in PD patients.
Therefore, this study aimed to examine the one-year risk of IHD, all-cardiovascular events, and all-cause mortality among users of antipsychotics compared with non-users in newly diagnosed PD patients, using a large population database.
Materials and Methods
Design and Data Source
This observational retrospective study utilized data from the Secure Anonymised Information Linkage (SAIL) databank. The SAIL databank contains prescribing and diagnostic data from General Practice (GP) surgeries of approximately 80% of the Welsh population.Citation27 The GP diagnostic and prescribing data in SAIL was linked to other health and social Welsh databases (ie, Welsh Demographic Service, Patient Episode Database for Wales [hospital events], Annual District Death Extract [mortality data], and social deprivation status [ie, Welsh Index of Multiple Deprivation (WIMD) scores]).Citation27 Information regarding PD diagnoses and medications was extracted from GP data. Hospital data were used to extract information regarding comorbidities associated with PD patients and the first event of cardiovascular hospitalization. Mortality data were used to extract death date and cause, to examine cardiovascular and all-cause mortality.
This study obtained Information Governance Review Panel (IGRP) approval with a reference number of (0507). The data used in this study were anonymized and any cell less than 5 patients was excluded from the analysis, following the SAIL confidentiality policy.
Identifying Newly Diagnosed PD Patients and Antipsychotic Codes
Individuals with a first definitive PD diagnosis Read Code in the GP data who had been initiated on any PD medication between 1 January 2000 and 30 September 2016 were the subjects of this study (Appendix 1). The Read Code system is a coding system used in the UK and encompasses clinical data, such as patient diagnoses and prescribed medications.Citation28 The codes used to identify definitive PD diagnoses were validated in a previous study.Citation29 The exclusion criteria included: patients aged less than 40 years; PD medications having been prescribed before PD diagnosis; no PD medications prescribed after PD diagnosis; first PD diagnosis within 6 months of SAIL registration date; and patients with a Read Code of psychosis, bipolar disorder, antipsychotics, secondary parkinsonism, or diffuse Lewy body diseases (DLB) within the year preceding the first PD diagnosis.Citation30 Patients younger than 40 years were excluded because PD is uncommon in this group of patients and the risk of having other type of parkinsonism-like symptoms that have been misdiagnosed as PD is high.Citation31,Citation32 Patient with a history of psychosis and bipolar disorder were excluded due to their possible association with developing PD.Citation33 Patients with secondary parkinsonism or DLB were excluded to avoid the risk of PD misdiagnosis.
To be considered an antipsychotic user, a PD patient must have had a psychosis diagnosis that followed the date of the first diagnosis of PD, followed by a prescription of antipsychotics within a year of PD diagnosis (see Appendix 1 for Read Codes). Patients who initiated more than one antipsychotic at the same time were excluded. Furthermore, patients who were prescribed antipsychotics without a diagnosis of psychosis were excluded. The types and classes of antipsychotics used in this study are shown in Appendix 2.
Study Models and Censoring
The index date was the date of the first antipsychotic prescription after psychosis diagnosis in the newly diagnosed PD patients. Patients were followed until the first IHD event (model 1); the first cardiovascular event, specifically arrhythmia, heart failure, IHD, stroke, or cardiovascular death (model 2); or all-cause mortality (model 3). Cumulative survival was measured in days. Details of these three models, including the time of data censoring, can be seen in . Given that PD progression data were not available in the SAIL databank, the follow-up period was set to one year to minimize the confounding effects of PD progression.Citation34
Table 1 Index Date and Censoring Data for the Study Models
Covariates
The following covariates were extracted from SAIL and incorporated in the analysis: age, gender, geographical location of the health board, status of social deprivation, year of PD diagnosis, previous cardiovascular events, comorbidities, PD medication(s) used before first antipsychotic use, and previous use of medications that might trigger cardiovascular events. Age was classified into three categories: young, 40–60 years; mid, 61–80 years; and older, >80 years. The Welsh health boards were classified into the following seven boards: Abertawe Bro Morgannwg, Aneurin Bevan, Betsi Cadwaladr, Cardiff and Vale, Cwm Taf, Hywel Dda, and Powys. The status of social deprivation was measured using the Welsh Index of Multiple Deprivation (WIMD) 2011 scale, where quintile 1 refers to the most deprived areas and quintile 5 refers to the least deprived areas. The previous cardiovascular events were any occurrences of arrhythmia, heart failure, IHD, or stroke recorded in the GP data before the first prescription of antipsychotics. Comorbidities were identified using those listed in the Charlson Comorbidity Index and were extracted using the hospital admission data from up to 2 years before the first use of antipsychotics. The Charlson Comorbidity Index is comprised of 16 comorbidities and each comorbidity was treated in the analysis as a binary variable. The comorbidities included: acute myocardial infarction, congestive heart failure, diabetes, diabetes complications, cerebral vascular accident, pulmonary disease, dementia, renal disease, cancer, peripheral vascular disease, connective tissue disorder, paraplegia, peptic ulcer, metastatic cancer, liver disease, and severe liver disease. The PD medications were the first medications used by the patients to treat PD before the use of antipsychotics. Finally, previous medications used by the PD patients that might have had an association with IHD risk were considered for their confounding effects. These medications included diuretics, alpha blockers, beta blockers, calcium channel blockers, angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARB), lipid-lowering agents, anti-arrhythmia agents, anti-diabetics,Citation35 antiplatelets, anticoagulants,Citation36 tricyclic antidepressants, selective serotonin reuptake inhibitors (SSRIs), other types of antidepressants,Citation37 nonsteroidal anti-inflammatory drugs (NSAIDs) and COX-2 inhibitors.Citation38
Statistical Methods
Patients’ demographics data were tabulated and summarized. Continuous variables were presented as mean and standard deviation (SD), while categorical variables were presented as counts and percentages. Cause-specific hazard functions were evaluated using Cox regression (proportional hazards regression) to assess the association between the use of antipsychotics and the outcome of interest while controlling for the competing risk of death ().Citation39 To build the regression model, the covariates to be included in the model needed to be determined. The Wald test was used to determine the significance of each covariate in the model. A particular covariate was included in the final model if the p-value of the Wald test was ≤ 0.20.
To reduce the bias that may result from inherited differences in baseline characteristics among PD patients who were antipsychotic users and non-users, the confounding covariates were adjusted using propensity score matching.Citation34 The propensity score was the probability of being prescribed antipsychotics at the index date. This score was determined using the non-parsimonious multiple logistic regression model based on covariates that, upon bivariate regression, resulted in a p-value of the Wald test ≤0.20. Subsequently, the calculated propensity scores were used to match the groups at a 1:1 ratio between antipsychotic users and non-users based on a caliper matching of 0.2 of the pooled SD of the propensity scores’ logit.Citation34
After matching and avoiding violation of the 10 events per predictor variable (EPV) rule, a new propensity score estimate was calculated for each model.Citation40 The propensity score in this case was the probability of developing the outcome of interest in each model based on covariates which, upon conducting a single Cox regression model, resulted in a p-value ≤ 0.20.Citation40 The main explanatory covariates, which were the use of antipsychotics or type of antipsychotics, were also added to the model. To avoid the possibility of violating the linearity assumption of propensity scores, they were categorized into five quintiles: 0–0.2, 0.21–0.4, 0.41–0.6, 0.61–0.8, and 0.81–1. The proportional hazard (PH) assumption was ensured using the Schoenfeld test and revealed no violations. Hence, the covariates were independent of time and the Cox regression model was conducted for all three models. Kaplan-Meier graphs were used to show the proportion of antipsychotic users who developed the outcomes at different points in time.
Sensitivity Analysis
To assess the robustness of the study outcomes, multiple sensitivity analyses were conducted. The first sensitivity analysis reexamined the three models excluding patients with a history of myocardial infarction, congestive heart failure, cancer and active malignancy, severe liver disease, and history of ergot dopamine agonists usage. These patients were not included in the sensitivity analysis as these factors can cause cardiovascular events; hence, their inclusion might undermine the effect of antipsychotics on cardiac events.
In the second sensitivity analysis, two separate propensity score-matching processes were conducted; the first matched FGA users 1:1 with non-users, while the second matched SGA users 1:1 with non-users. Then, the statistical tests discussed previously in all three models were reconducted. This was done because the original propensity score matching was based on the demographic and clinical data of antipsychotics users vs non-users without specifying the category of antipsychotics (FGA vs SGA). However, in the regression analysis, antipsychotics users were divided into FGA and SGA and compared to non-users, which might have produced an inaccurate estimate. Finally, a third sensitivity analysis was conducted in which FGA were directly compared to SGA while excluding all non-users from the analysis. The purpose of this analysis was to obtain estimates that directly compared FGA to SGA. Then, these estimates were compared to the estimates in the original models (ie those comparing FGA and SGA users to non-users) in developing IHD, cardiac events, and all-cause mortality.
Results
Patient Characteristics
The baseline characteristics of participants and the total number of outcomes are shown in . In total, the propensity score matching process resulted in 1837 (out of 8253) participants in both treatment and control groups. Among these participants, the mean age was 76.1 years (SD=8.1). Just over half the sample (58.4%) was male and levodopa was the most commonly initiated PD medication (86.7%). As the matching process was based on the ratio of 1:1 between the treatment and control groups, about 50% of the participants received antipsychotics, with SGAs constituting the majority of prescribed antipsychotics. Quetiapine, in particular, compromised almost half of all antipsychotics prescribed (51.8%), followed by risperidone (9.9%) and olanzapine (7.9%) (Appendix 3). Within one year of the first antipsychotic prescription, 2.3% (n=42) of patients developed IHD, 4.1% (n=75) of patients developed at least one cardiovascular event, and 19.1% (n=350) of patients had died ().
Table 2 Patient Demographics
Ischemic Heart Disease Model
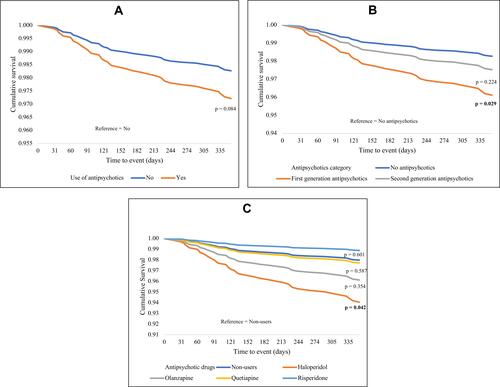
The detailed results of univariate and multivariate Cox regression are shown in Appendix 4. shows the propensity score adjusted model used to calculate the hazard ratio (HR) of developing IHD in PD patients who were antipsychotics users. The propensity score adjusted model shows that FGA users were significantly more likely to develop IHD compared to non-users, with an HR of 2.60 (95% CI 1.103–6.167). Among the FGAs, haloperidol had the highest likelihood of IHD developing, with an HR of 3.01 (95% CI 1.038–8.729). Other individual antipsychotics did not show a significant link to IHD (). presents the Cox regression curves comparing IHD hospitalization over time (365 days) for PD patients who were antipsychotic users vs PD patients who were antipsychotic non-users.
Table 3 The Propensity Score and Multivariable Adjusted Models Examining the Factors That Affecting the Study Outcomes (Matched Cohort)
Figure 1 Kaplan–Meier estimates of ischemic heart disease according to the status of antipsychotic use in PD patients. P-values indicate the differences in survival compared to the reference group in the Cox regression equation. (A) Ischemic heart disease model (propensity score adjusted), (B) Ischemic heart disease model (propensity score adjusted), (C) Ischemic heart disease model (propensity score adjusted).
All Cardiovascular Events Model
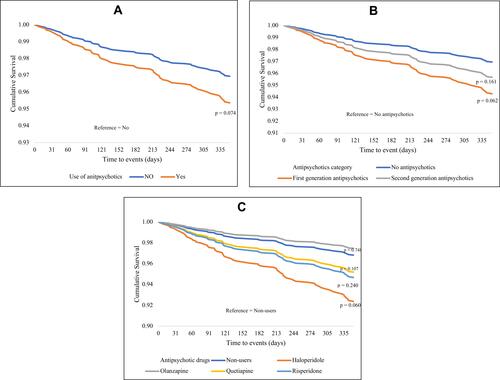
Appendix 4 shows the detailed results of univariate and multivariate Cox regression, examining the association between antipsychotic use and all cardiovascular events. The propensity score adjusted model shows there was no significant difference between antipsychotics users and non-users in developing all cardiovascular events, specifically arrhythmia, heart failure, IHD, stroke, or cardiovascular death (). However, the multivariate adjusted model shows that FGA users were significantly more likely to develop all cardiovascular events compared to non-users, with an HR of 2.018 (95% CI 1.041–3.91). Additionally, and similarly to the IHD model, the multivariate adjusted model revealed that haloperidol users were more likely to develop all cardiovascular events, with an HR of 2.715 (95% CI 1.109–6.649) (). presents the Cox regression curves comparing all cardiovascular events over time (365 days) for PD patients who were antipsychotic users vs PD patients who were antipsychotic non-users.
Figure 2 Kaplan–Meier estimates of cardiovascular events according to the status of antipsychotic use in PD patients. P-values indicate the differences in survival compared to the reference group in the Cox regression equation. (A) cardiovascular events model (propensity score adjusted), (B) cardiovascular events model (propensity score adjusted), (C) cardiovascular events model (propensity score adjusted).
All-Cause Mortality Model
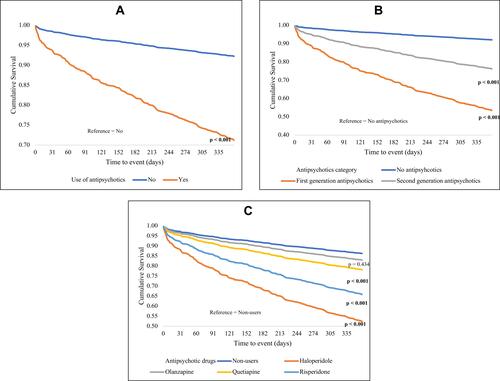
The propensity score adjusted model shows that the use of any antipsychotic, regardless of FGA or SGA, was linked to all-cause mortality, with an HR of 4.201 (95% CI 3.272–5.394) (). When subdividing antipsychotics into FGA and SGA, FGA users were more likely to die, with an HR of 7.557 (95% CI 5.633–10.139). SGA users were also likely to die, but with a lower HR of 3.278 (95% CI 2.509–4.282). Similar to the previous two models, among the individual antipsychotics, haloperidol had the highest HR of 4.372 (95% CI 2.995–6.382) in all-cause mortality, followed by risperidone (HR=2.825, 95% CI 1.962–4.068) and quetiapine (HR=1.668, 95% CI 1.3–2.141). shows the Cox regression curves comparing all-cause mortality over time (365 days) for PD patients who were antipsychotic users vs PD patients who were antipsychotic non-users.
Figure 3 Kaplan–Meier estimates of all-cause mortality according to the status of antipsychotic use in PD patients. P-values indicate the differences in survival compared to the reference group in the Cox regression equation. (A) all-cause mortality model (Propensity score adjusted), (B) all-cause mortality model (Propensity score adjusted), (C) all-cause mortality model (Propensity score adjusted).
In all three models, the outcomes of the first sensitivity analysis were consistent after excluding patients with a history of myocardial infarction, congestive heart failure, cancer and active malignancy, severe liver disease, and history of ergot dopamine agonists usage (see Appendix 5). Additionally, the second sensitivity analysis that separately matched FGA users with non-users, and SGA users with non-users, revealed consistent results that did not significantly differ from the original results (Appendix 6). Finally, the third sensitivity analysis showed that SGA users compared to FGA users were more likely to develop IHD and all-cause mortality (see ), which is consistent with the original estimates presented in .
Table 4 The Propensity Score and Multivariable Adjusted Models Examining the Factors That Affecting the Study Outcomes (Sub Cohort Analysis That Compared Second-Generation Antipsychotics to First-Generation Antipsychotics Directly)
Discussion
The growing body of literature has shown that PD patients can develop cardiovascular diseases and, in particular, IHD.Citation2 Several risk factors increase the risk of developing IHD in PD patients, such as genetic predisposition, smoking, and diabetes.Citation2 Additionally, given that PD is more prevalent in elderly patients, high cardiovascular morbidity profiles and increased prevalence of polypharmacy are expected in PD patients.Citation41 The average number of medications taken by a PD patient is ≥ 5, which increases with advanced age and deterioration of PD motor and non-motor symptoms.Citation42 Some of these medications are associated with an increased risk of cardiovascular events, such as nonsteroidal anti-inflammatory drugs (NSAIDs), COX-2 inhibitorsCitation38 and antidepressants.Citation37 Other medications, such as antipsychotics, have been linked pharmacologically to IHD in the general population and in dementia patients,Citation8,Citation26 but these medications have been understudied in PD patients.
This study has used data from a large population database in Wales, covering almost 80% of the Welsh population for a period of 17 years. The study found that IHD was 2.6 times more likely among FGA users compared to non-users in newly diagnosed PD patients. Of the FGAs, haloperidol showed the highest likelihood of IHD developing. Previous research findings into the association between antipsychotics and IHD in the general population have been contradictory.Citation8,Citation19 However, no study has examined this association in PD patients, where the use of antipsychotics is profoundly highCitation43 and the cardiovascular risks are paramount.Citation1 The current study confirmed such an association between FGAs and IHD, after controlling for other comorbidities and confounders in newly diagnosed PD patients who started antipsychotics after their PD diagnosis. Given that haloperidol was the most commonly used FGA in this cohort, this result may indicate that the FGAs that cause the greatest IHD risk in PD patients are the FGAs with the most potent dopamine receptor blockade activity or those which have a high ratio of dopamine to serotonin receptor blockade.Citation44
In general, FGAs are not recommended in the treatment of psychosis in PD patients.Citation9 Psychotic episodes can be triggered by PD itself or by medications that treat motor symptoms of PD, such as dopamine agonists (DA), therefore it is advised before initiating antipsychotics to decrease the DA dose to a level that does not worsen motor symptoms.Citation9 If psychotic episodes are not relieved using the previous strategy then SGAs, particularly quetiapine, can be used.Citation9 Although quetiapine efficacy has not been illustrated in randomized clinical trials, various experts have suggested off-label use of quetiapine as the first-line therapy in PD psychosis.Citation45
This study also found that all antipsychotics increased all-cause mortality risk in PD patients. FGA users showed the most significant association, with a seven-fold increase in mortality compared to non-users of FGAs. The association between high mortality rate and antipsychotics was previously observed in dementia patientsCitation13 and advanced PD patients,Citation15 and the current study extends this association to include recently diagnosed PD patients. Previous literature shows that the increased mortality rate is common in PD patients, with risk factors having been identified as advanced age, male sex, and psychotic episodes.Citation46 The current study accounted for these risk factors by applying the propensity score matched model to control for statistical effects such as age, sex, and concurrent comorbidities. However, factors such as psychotic episodes could not be controlled for since all antipsychotic users in the current study had a psychosis diagnosis, making it challenging to attribute the high mortality rate to the antipsychotics alone. Nevertheless, the link between antipsychotics and a higher mortality rate can by strengthened by the consistent differential risk between FGAs and SGAs in the current study (ie, FGAs had a higher hazard ratio than SGAs), which replicated the results of previous studies.Citation15,Citation47
Although the findings of this study showed that quetiapine was not associated with IHD and cardiovascular events in PD patients, quetiapine was found to be associated with all-cause mortality, requiring caution before and during its use. Quetiapine is used as the first line of treatment in psychosis in PD patients according to the UK National Institute for Health and Care Excellence (NICE) guidelinesCitation45 because it has less impact on PD motor symptoms compared to other SGAs, such as olanzapine.Citation48 However, its association with all-cause mortality, as suggested by the current study, is a matter of concern that needs further investigation.
A key strength of the present study was that it is the first study to evaluate the association between antipsychotic use and cardiovascular events (IHD in particular) in newly diagnosed PD patients. Other strengths of this study include the large sample size and use of a large population database. Additionally, the propensity score matched model applied in the analysis increased the statistical validity of the results and decreased the potential bias inherited in this type of study.Citation34
A number of limitations need to be noted regarding the present study. Firstly, medical record codes alone were used to identify PD patients and other diagnoses, with no verification from a movement disorders specialist. Secondly, the results were possibly confounded by indication. For example, PD patients who used antipsychotics may have also suffered from more severe PD, making a higher mortality rate more likely. However, since this study focused on newly diagnosed PD patients, this type of confounding was minimized. Additionally, due to data access difficulties and quality issues, IHD and cardiac events were only extracted from the hospital data rather than being combined with the GP data, which may increase the risk of misclassification; therefore, caution should be exercised when interpreting the related results. Finally, the relatively short follow-up period in this study (ie, 365 days) could be a limitation, however, this could be justified by the study aim, which was to examine the immediate effects of antipsychotics. A further study could assess the long-term effects and examine the association between newer SGAs, such as pimavanserin, and cardiovascular events and mortality.Citation49
Conclusion
The role of antipsychotic treatment for neuropsychiatric symptoms in PD patients is pivotal, however, the use of antipsychotics is not without risk.Citation50 The current study revealed a high risk of IHD and all-cause mortality associated with the use of some antipsychotics in newly diagnosed PD patients. These findings highlight that antipsychotics (both FGAs and SGAs) should be used with caution in PD psychosis, for the shortest time and at the lowest dose. PD patients with a history of cardiovascular disease and other comorbidities should be advised of the risks associated with antipsychotics prior to treatment being initiated. The current study also found different levels of risk associated with individual antipsychotics and found differences between FGAs and SGAs in relation to IHD risk. The results of this study warrant further investigation with a larger sample size and a longer duration of follow-up. In the interim, the antipsychotic benefit in PD psychosis must be measured against the risk of potential safety concerns.
Acknowledgment
I acknowledge the help provided by the SAIL team in all stages of the study.
Disclosure
The author reports no conflicts of interest in this work.
Additional information
Funding
References
- Alves M, Caldeira D, Ferro JM, Ferreira JJ. Does Parkinson’s disease increase the risk of cardiovascular events? A systematic review and meta-analysis. Eur J Neurol. 2020;27(2):288–296. doi:10.1111/ene.14076
- Scorza FA, Fiorini AC, Scorza CA, Finsterer J. Cardiac abnormalities in Parkinson’s disease and Parkinsonism. J Clin Neurosci. 2018;53:1–5. doi:10.1016/j.jocn.2018.04.031
- McLean G, Hindle JV, Guthrie B, Mercer SW. Co-morbidity and polypharmacy in Parkinson’s disease: insights from a large Scottish primary care database. BMC Neurol. 2017;17(1):126. doi:10.1186/s12883-017-0904-4
- Yang YW, Hsieh TF, Li CI, et al. Increased risk of Parkinson disease with diabetes mellitus in a population-based study. Medicine (Baltimore). 2017;96(3):e5921. doi:10.1097/MD.0000000000005921
- Schade R, Andersohn F, Suissa S, Haverkamp W, Garbe E. Dopamine agonists and the risk of cardiac-valve regurgitation. N Engl J Med. 2007;356(1):29–38. doi:10.1056/NEJMoa062222
- Crispo JAG, Willis AW, Thibault DP, et al. Associations between cardiovascular events and nonergot dopamine agonists in parkinson’s disease movement disorders clinical practice. Movement Disorders Clin Practice. 2016;3(3):257–267. doi:10.1002/mdc3.12286
- Waring WS. Clinical use of antidepressant therapy and associated cardiovascular risk. Drug Healthc Patient Saf. 2012;4:93. doi:10.2147/DHPS.S28804
- Rotella F, Cassioli E, Calderani E, et al. Long-term metabolic and cardiovascular effects of antipsychotic drugs. A meta-analysis of randomized controlled trials. Eur Neuropsychopharmacol. 2020;32:56–65. doi:10.1016/j.euroneuro.2019.12.118
- Schapira AHV, Chaudhuri KR, Jenner P. Non-motor features of Parkinson disease. Nat Rev Neurosci. 2017. doi:10.1038/nrn.2017.62
- Marras C, Kopp A, Qiu F, et al. Antipsychotic use in older adults with Parkinson’s disease. Mov Disord. 2007;22(3):319–323. doi:10.1002/mds.21192
- Wang MT, Lian PW, Yeh CB, Yen CH, Ma KH, Chan AL. Incidence, prescription patterns, and determinants of antipsychotic use in patients with Parkinson’s disease. Mov Disord. 2011;26(9):1663–1669. doi:10.1002/mds.23719
- Food and Drug Administration (FDA) Public Health Advisory. Deaths with antipsychotics in elderly patients with behavioral disturbances. Department of Health and Human Services, U.S. Government; 2005. Available from: www.fda.gov/drugs/drugsafety/postmarketdrugsafetyinformationforpatientsandproviders/ucm053171.htm. Accessed June 2.
- Food and Drug Administration (FDA). Information for Healthcare Professionals—antipsychotics. Department of Health and Human Services, U.S. Government; 2008. Available from: www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm124830.htm. Accessed June 2.
- Weintraub D, Chiang C, Kim HM, et al. Antipsychotic use and physical morbidity in parkinson disease. Am j Geriatric Psychiatry. 2017;25(7):697–705. doi:10.1016/j.jagp.2017.01.076
- Weintraub D, Chiang C, Kim HM, et al. Association of antipsychotic use with mortality risk in patients with parkinson disease. JAMA Neurol. 2016;73(5):535–541. doi:10.1001/jamaneurol.2016.0031
- Ballard C, Isaacson S, Mills R, et al. Impact of current antipsychotic medications on comparative mortality and adverse events in people with parkinson disease psychosis. J Am Med Dir Assoc. 2015;16(10):898e1–7. doi:10.1016/j.jamda.2015.06.021
- Hirsch L, Yang J, Bresee L, Jette N, Patten S, Pringsheim T. Second-generation antipsychotics and metabolic side effects: a systematic review of population-based studies. Drug Safety. 2017;40(9):771–781. doi:10.1007/s40264-017-0543-0
- Barbui C, Gastaldon C, Papola D, Ostuzzi G. Antipsychotic drug exposure and risk of myocardial infarction. Epidemiol Psychiatr Sci. 2017;26(1):18–21. doi:10.1017/S204579601600086X
- Papola D, Ostuzzi G, Gastaldon C, et al. Antipsychotic use and risk of life-threatening medical events: umbrella review of observational studies. Acta Psychiatr Scand. 2019;140(3):227–243. doi:10.1111/acps.13066
- Correll CU, Frederickson AM, Kane JM, Manu P. Does antipsychotic polypharmacy increase the risk for metabolic syndrome? Schizophr Res. 2007;89(1–3):91–100. doi:10.1016/j.schres.2006.08.017
- Lin ST, Chen CC, Tsang HY, et al. Association between antipsychotic use and risk of acute myocardial infarction: a nationwide case-crossover study. Circulation. 2014;130(3):235–243. doi:10.1161/CIRCULATIONAHA.114.008779
- Malekizadeh Y, Williams G, Kelson M, et al. Whole transcriptome in silico screening implicates cardiovascular and infectious disease in the mechanism of action underlying atypical antipsychotic side effects. Alzheimers Dement (N Y). 2020;6(1):e12078. doi:10.1002/trc2.12078
- Beauchemin M, Geguchadze R, Guntur AR, et al. Exploring mechanisms of increased cardiovascular disease risk with antipsychotic medications: risperidone alters the cardiac proteomic signature in mice. Pharmacol Res. 2020;152:104589. doi:10.1016/j.phrs.2019.104589
- May M, Beauchemin M, Vary C, Barlow D, Houseknecht KL. The antipsychotic medication, risperidone, causes global immunosuppression in healthy mice. PLoS One. 2019;14(6):e0218937. doi:10.1371/journal.pone.0218937
- Nielsen R-E, Lolk A, Rodrigo-Domingo M, Valentin J-B, Andersen K. Antipsychotic treatment effects on cardiovascular, cancer, infection, and intentional self-harm as cause of death in patients with Alzheimer’s dementia. Eur Psychiatry. 2017;42:14–23. doi:10.1016/j.eurpsy.2016.11.013
- Steinberg M, Lyketsos CG. Atypical antipsychotic use in patients with dementia: managing safety concerns. Am J Psychiatry. 2012;169(9):900–906. doi:10.1176/appi.ajp.2012.12030342
- Jones KHFD, Lyons RA. The SAIL databank: 10 years of spearheading data privacy and research utility, 2007–2017. University S; 2017.
- Robinson D, Schulz E, Brown P, Price C. Updating the Read Codes: user-interactive maintenance of a dynamic clinical vocabulary. J Am Med Inform Assoc. 1997;4(6):465–472. doi:10.1136/jamia.1997.0040465
- Parkinson’s UK. The prevalence and incidence of Parkinson’s in the UK. Parkinson’s UK; 2017. Available from: https://www.parkinsons.org.uk/sites/default/files/2018-01/Prevalence%20%20Incidence%20Report%20Latest_Public_2.pdf. Accessed January 25, 2018.
- Rochon PA, Stukel TA, Sykora K, et al. Atypical antipsychotics and parkinsonism. Arch Intern Med. 2005;165(16):1882–1888. doi:10.1001/archinte.165.16.1882
- Van Den Eeden SK, Tanner CM, Bernstein AL, et al. Incidence of Parkinson’s disease: variation by age, gender, and race/ethnicity. Am J Epidemiol. 2003;157(11):1015–1022. doi:10.1093/aje/kwg068
- Schrag A, Schott JM. Epidemiological, clinical, and genetic characteristics of early-onset parkinsonism. Lancet Neurol. 2006;5(4):355–363. doi:10.1016/S1474-4422(06)70411-2
- Faustino PR, Duarte GS, Chendo I, et al. Risk of developing parkinson disease in bipolar disorder: a systematic review and meta-analysis. JAMA Neurol. 2020;77(2):192–198. doi:10.1001/jamaneurol.2019.3446
- Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 2011;46(3):399–424. doi:10.1080/00273171.2011.568786
- Stewart J, Manmathan G, Wilkinson P. Primary prevention of cardiovascular disease: a review of contemporary guidance and literature. JRSM Cardiovasc Dis. 2017;6:2048004016687211. doi:10.1177/2048004016687211
- Levine GN, Bates ER, Bittl JA, et al. 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease: a Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines: an Update of the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention, 2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery, 2012 ACC/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease, 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction, 2014 AHA/ACC Guideline for the Management of Patients With Non-ST-Elevation Acute Coronary Syndromes, and 2014 ACC/AHA Guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery. Circulation. 2016;134(10):e123–55. doi:10.1161/CIR.0000000000000404
- Nezafati MH, Vojdanparast M, Nezafati P. Antidepressants and cardiovascular adverse events: a narrative review. ARYA Atheroscler. 2015;11(5):295–304.
- McGettigan P, Henry D. Cardiovascular risk with non-steroidal anti-inflammatory drugs: systematic review of population-based controlled observational studies. PLoS Med. 2011;8(9):e1001098. doi:10.1371/journal.pmed.1001098
- Kalbfleisch JD, Prentice RL. The statistical analysis of failure time data. John Wiley & Sons; 2011.
- Vittinghoff E, McCulloch CE. Relaxing the rule of ten events per variable in logistic and Cox regression. Am J Epidemiol. 2007;165(6):710–718. doi:10.1093/aje/kwk052
- Vrettos I, Voukelatou P, Katsoras A, Theotoka D, Kalliakmanis A. Diseases linked to polypharmacy in elderly patients. Curr Gerontol Geriatr Res. 2017;2017:4276047. doi:10.1155/2017/4276047
- Csoti I, Herbst H, Urban P, Woitalla D, Wullner U. Polypharmacy in Parkinson’s disease: risks and benefits with little evidence. J Neural Transm (Vienna). 2019;126(7):871–878. doi:10.1007/s00702-019-02026-8
- Marras C, Austin PC, Bronskill SE, Diong C, Rochon PA. Antipsychotic drug dispensing in older adults with parkinsonism. Am j Geriatric Psychiatry. 2018;26(12):1244–1257. doi:10.1016/j.jagp.2018.08.003
- Richtand NM, Welge JA, Logue AD, Keck PE Jr, Strakowski SM, McNamara RK. Dopamine and serotonin receptor binding and antipsychotic efficacy. Neuropsychopharmacology. 2007;32(8):1715–1726. doi:10.1038/sj.npp.1301305
- Rogers G, Davies D, Pink J, Cooper P. Parkinson’s disease: summary of updated NICE guidance. BMJ. 2017;358:j1951. doi:10.1136/bmj.j1951
- Forsaa EB, Larsen JP, Wentzel-Larsen T, Alves G. What predicts mortality in Parkinson disease?: a prospective population-based long-term study. Neurology. 2010;75(14):1270–1276. doi:10.1212/WNL.0b013e3181f61311
- Jackson JW, VanderWeele TJ, Blacker D, Schneeweiss S. Mediators of first- versus second-generation antipsychotic-related mortality in older adults. Epidemiology. 2015;26(5):700–709. doi:10.1097/EDE.0000000000000321
- Zhang H, Wang L, Fan Y, et al. Atypical antipsychotics for Parkinson’s disease psychosis: a systematic review and meta-analysis. Neuropsychiatr Dis Treat. 2019;15:2137–2149. doi:10.2147/NDT.S201029
- Patel RS, Bhela J, Tahir M, Pisati SR, Hossain S. Pimavanserin in parkinson’s disease-induced psychosis: a literature review. Cureus. 2019;11(7):e5257. doi:10.7759/cureus.5257
- Sprenger F, Poewe W. Management of motor and non-motor symptoms in Parkinson’s disease. CNS Drugs. 2013;27(4):259–272. doi:10.1007/s40263-013-0053-2