Abstract
Atrial fibrillation (AF) is a common arrhythmia that is associated with an increased risk of stroke, particularly in the elderly. Traditionally, a vitamin K antagonist such as warfarin is prescribed for stroke prevention. Warfarin is effective at lowering stroke risk but has several limitations due to food restrictions, drug interactions, and a narrow therapeutic window. Various novel oral anticoagulants (NOACs) are available or under development to provide alternative treatment options. This article reviews the efficacy and safety of three NOACs (dabigatran etexilate, rivaroxaban, and apixaban) in addition to warfarin and aspirin, for prevention of stroke in patients with AF, focusing on the elderly population. Results of clinical trials demonstrate that the efficacy of NOACs for stroke prevention in patients with AF is as good as or better than that of warfarin. The NOACs are also associated with an equivalent or lower risk of bleeding. Regardless of the medication chosen, older patients with AF must be treated cautiously due to an increased risk of stroke and bleeding, as well as potential challenges related to drug interactions and monitoring requirements. NOACs may be suitable alternatives to warfarin for stroke prevention in older patients due to several advantages, including a faster onset of action, few drug or food interactions, and no requirement for regular monitoring. However, dose adjustments may be required for certain patients, such as those with severe renal impairment or in the setting of drug interactions.
Introduction
Atrial fibrillation (AF) is a common cardiac arrhythmia and a well-established risk factor for stroke.Citation1,Citation2 Patients with AF have a four- to five-times greater risk of stroke or transient ischemic attack compared with those without AF.Citation1,Citation3 In addition, strokes that occur in patients with AF are associated with an increased risk of premature death and disability.Citation4–Citation10
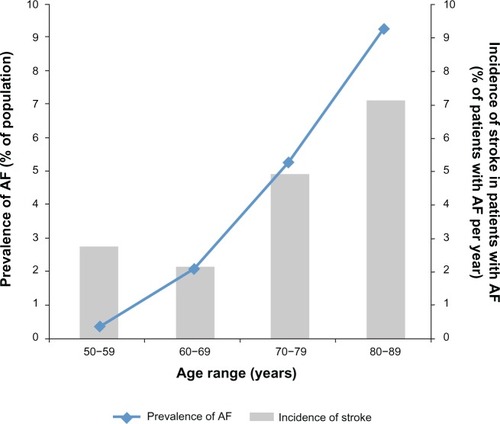
AF is an especially important concern among older adults. Prevalence of AF increases with patient age ()Citation3,Citation11 and, in the USA, approximately 82% of patients with AF are ≥ 65 years old and 37% are ≥ 80 years old.Citation3 The rate of stroke in patients with AF increases substantially in patients aged 80–89 years, with an attributable risk of 23.5%.Citation1 As age increases, the risk of complications from stroke increases. The CHADS2 score – calculated based on presence of Congestive heart failure (either systolic or diastolic), Hypertension, Age ≥ 75 years, Diabetes mellitus, and history of Stroke or transient ischemic attack – is used to estimate a patient’s long-term risk of stroke.Citation12 Points are assigned to each of the included risk factors, with two points assigned for history of stroke, and total scores range from 0 (low risk) to 6 (high risk).
Figure 1 Impact of atrial fibrillation (AF) by increasing age: overall prevalence of AF and annual incidence of stroke in patients with AF.
A modified version of the CHADS2, the CHA2DS2-VASc score, considers the following additional risk factors for stroke in patients with AF: vascular disease (such as myocardial infarction [MI], complex aortic plaque, and peripheral artery disease), female sex, and age 65–74 years.Citation13 The CHA2DS2-VASc score places greater emphasis on age ≥ 75 years by assigning two points to this risk factor. Because the prevalence of many of the risk factors included in CHADS2 and CHA2DS2-VASc also increases with age,Citation14–Citation16 age is a dichotomous variable in the calculation of CHADS2 and CHA2DS2-VASc scores.
Stroke prevention in patients with AF focuses on anticoagulant agents, including warfarin (a vitamin K antagonist), which effectively reduce the risk of stroke by preventing blood clots from forming. However, warfarin has a narrow therapeutic window, is associated with an increased risk of bleeding including intracranial hemorrhage (ICH), and requires frequent monitoring.Citation17 These limitations have prompted the development of a novel group of anticoagulants, which may be particularly helpful when considering stroke prevention in elderly patients with AF.
Use of warfarin for stroke prevention in older patients
Many clinical trials have demonstrated the efficacy of warfarin for stroke prevention in patients with AF. Warfarin-treated patients were 61% less likely to have a stroke and 66% less likely to have an ischemic stroke than patients in control groups.Citation18 Anticoagulant treatment remains effective in older patients with AF.Citation19 An analysis of almost 9000 patients with AF found that the benefit of oral anticoagulation in the prevention of stroke was maintained regardless of patient age. When viewed relative to the increase in stroke risk in older patients, these investigators concluded that the absolute benefit of anticoagulation increases as patients age.Citation19
Despite its efficacy, many patients with AF (50% or more) do not receive warfarin and remain at high risk of stroke.Citation20–Citation22 In the USA, only approximately one-third of office-based patient visits for AF included a mention of warfarin.Citation23 Potential contraindications are the most frequently cited reason for why warfarin is not prescribed. However, study conclusions vary on the extent to which true, rather than perceived, contraindications prevent warfarin treatment, particularly in elderly patients.Citation20,Citation21,Citation24 Among patients without contraindications to warfarin therapy, only 22% were prescribed warfarin in an observational study across five European countries.Citation21 Although some retrospective studies of charts or databases have found higher proportions (55%), it is clear that many patients who are candidates for anticoagulation do not receive treatment.Citation2,Citation25
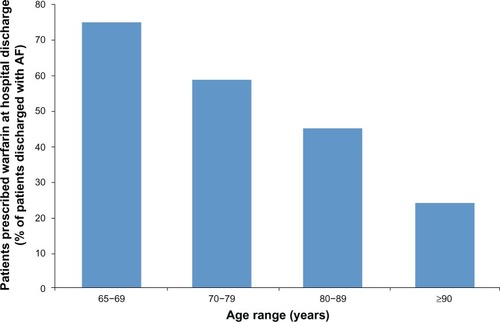
Multiple studies have found that patients of advanced age are less likely to receive anticoagulation therapy than younger patients ().Citation20,Citation24–Citation26 A retrospective review of hospital admissions for ischemic stroke in patients with AF found that 75% of patients aged < 75 years received anticoagulation therapy compared with only 33% of patients aged > 85 years.Citation25 Similarly, a prospective study found decreasing rates of anticoagulation therapy with increasing age: 75% of patients aged 65–69 years, 59% of patients aged 70–79 years, 45% of patients aged 80–89 years, and 24% of patients aged ≥ 90 years were treated with warfarin.Citation20
Figure 2 Rates of anticoagulation by patient age group.
Limited use of anticoagulation is attributed to a number of difficulties with warfarin, including drug interactions (), risk of bleeding, and dietary restrictions, as well as variability in patient response (eg, due to factors such as age, renal clearance, ethnicity, and genetic variability).Citation20,Citation21,Citation27–Citation29 The requirement for frequent monitoring can be a barrier and some patients may be unwilling to undertake treatment.Citation30 Amid these challenges, compliance with warfarin use has also been shown to decline over time. In a study of 1005 adults with AF in which 65% were prescribed warfarin, only 44% were still taking it 30 months later.Citation31
Table 1 Summary of drug–drug interactions for warfarin and the novel oral anticoagulants dabigatran, rivaroxaban, and apixaban
When warfarin is prescribed, the level of anticoagulation achieved varies, and this affects treatment effectiveness. Maintaining an international normalized ratio (INR) between two and three provides efficacy in reducing stroke risk and minimizes the excess risk of bleeding.Citation31,Citation32 Patients with an INR less than two have a significantly greater risk of ischemic stroke; patients with an INR greater than three are at a significantly increased risk of bleeding compared with those within the INR range of two to three.Citation31 Evidence from meta-analyses of clinical trials and cohort studies indicates that patients receiving warfarin spend, on average, only 51%–64% of the time in this therapeutic range.Citation33,Citation34 The amount of time spent in the therapeutic range is directly linked to the risk of stroke in patients aged ≥ 70 years.Citation35
A further restriction on appropriate warfarin use in patients of advanced age is the limited ability of risk-stratification schemes to predict stroke risk in patients aged ≥ 75 yearsCitation36 and perceived difficulty assessing when the benefits of anticoagulation outweigh the risks.Citation37 Several risk-stratification scoring systems to assess risk of bleeding with warfarin treatment have been developed. These include: HAS-BLED (Hypertension, Abnormal renal/liver function, Stroke, Bleeding history or predisposition, Labile INR, Elderly [≥ 65 years], and concomitant Drug/alcohol use),Citation38 HEMORR2HAGES (Hepatic or renal disease, Ethanol abuse, Malignancy, Older age, Reduced platelet count or function, Re-bleeding, Hypertension, Anemia, Genetic factors, Excessive fall risk and Stroke),Citation39 or that developed in the Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) study (anemia, severe renal disease, age ≥ 75 years, previous hemorrhage, and diagnosed hypertension).Citation40 A study comparing the predictive performance of these tools in patients with AF undergoing anticoagulation showed that the HAS-BLED, HEMORR2HAGES and ATRIA scores had only modest performance in predicting any clinically relevant bleeding, though the HAS-BLED score performed better than the other two. Only HAS-BLED was significantly predictive of ICH.Citation41
Beyond considering advanced age as a contraindication to warfarin, fear of elderly patients falling (leading to an increased risk of bleeding and ICH) is a frequently cited reason why clinicians do not prescribe anticoagulant therapy to older patients. This perceived risk of bleeding or ICH due to falls appears to be higher than the actual risk.Citation42–Citation44 Similarly, although clinicians may hesitate to use warfarin in elderly patients with cognitive impairment, mild-to-moderate cognitive impairment does not necessarily interfere with warfarin use.Citation45 Caution is warranted, however, as bleeding risk with warfarin treatment does increase with age. Among patients treated with warfarin, the relative risk of a life-threatening bleeding event in patients aged ≥ 80 years was 4.5 (95% confidence interval [CI], 1.3, 15.6) when compared with patients aged < 50 years.Citation46
Aspirin as an alternative to warfarin in older patients
Age is an independent risk factor for stroke, and complications from stroke increase as patients with AF age. This should increase the likelihood of preventive treatment but warfarin is under-prescribed in the elderly.Citation25 Due to the bleeding risks associated with warfarin, physicians may prefer to prescribe aspirin for stroke prevention in patients with AF.Citation20,Citation36 Among 405 inpatients with AF, aged 65 years or older, 199 (49%) did not receive warfarin on discharge and physicians preferred to prescribe aspirin in approximately 70% of these patients.Citation20 Guidelines include recommendations for the use of aspirin for stroke prevention in AF; however, these recommendations are generally restricted to patients considered to be at low risk for stroke or those with contraindications to the use of warfarin.Citation47–Citation49
Although viewed by many clinicians as an alternative to warfarin, the efficacy of antiplatelet treatment with aspirin for stroke reduction is limited. Pooled clinical trial data show a 21% reduction in the relative risk of stroke with aspirinCitation49 and a study in low-risk patients with AF observed that aspirin might be no better than placebo for reducing thromboembolic events and may be associated with an increased risk of major bleeding.Citation50 Trials comparing aspirin and warfarin have found aspirin treatment to be less effective in stroke prevention and to cause more bleeding events than treatment with warfarin.Citation51,Citation52 Similar limitations to aspirin therapy were found in patients of advanced age (≥ 75 years or 80–90 years).Citation52,Citation53 The Birmingham Atrial Fibrillation Treatment of the Aged (BAFTA) trial demonstrated the superiority of warfarin over aspirin in reducing the risk of ischemic stroke in patients with AF aged ≥ 75 years.Citation52 The risk of stroke was reduced by 54% (P = 0.003) and the combined risk of fatal or disabling stroke (ischemic or hemorrhagic), ICH, or clinically significant embolism was reduced by 52% in the warfarin group compared with the aspirin group (P = 0.003), with no difference in major bleeding events. Aspirin therapy is further limited in older patients because the efficacy of aspirin seems to decline beyond the age of 70 years, whereas the risk of bleeding increases.Citation19
Novel oral anticoagulants in AF
Limitations and concerns associated with warfarin therapy and lack of efficacy associated with aspirin therapy have led to the development of novel oral anticoagulants (NOACs), including dabigatran (a direct thrombin inhibitor),Citation54 rivaroxabanCitation55 and apixabanCitation56 (direct factor Xa inhibitors). Edoxaban is another direct factor Xa inhibitor that is currently in late-stage clinical trials.Citation57
Updated guidelines from the American College of Chest Physicians recommend oral anticoagulation in patients with AF at intermediate (CHADS2 score of 1) or high (CHADS2 score of ≥ 2) risk of stroke.Citation58 In such patients, the American College of Chest Physicians guidelines recommend use of dabigatran 150 mg twice daily rather than dose-adjusted warfarinCitation59; however, it should be noted that these guidelines were published prior to the approval of rivaroxaban and apixaban.
While dabigatran, rivaroxaban, and apixaban are all novel anticoagulants that are administered orally, clinical trial data provide some differentiation between these treatments ().
Table 2 Summary of study results for RE-LY, ROCKET-AF, ARISTOTLE, and AVERROES, for stroke and systemic embolism rates, major bleeding rates, and all-cause mortality
Dabigatran etexilate: RE-LY
Dabigatran is a direct inhibitor of thrombin, the enzyme that converts soluble fibrinogen into insoluble strands of fibrin.Citation55 The inhibition of thrombin prevents the formation of blood clots and, therefore, is an effective mechanism for anticoagulation.
The Randomized Evaluation of Long-term anticoagulation therapY (RE-LY) trialCitation60,Citation61 included 18,113 patients with AF who were at risk of stroke. The study subjects were randomized into three groups and received double-blinded dabigatran (150 or 110 mg) or open-label adjusted-dose warfarin. Patients had a mean age of 71 years and a mean CHADS2 score of 2.1.
In RE-LY, dabigatran 150 mg twice daily was associated with a 35% reduction in the relative risk of stroke or systemic embolism (P < 0.001 for superiority) and a similar rate of major bleeding compared with warfarin.Citation60,Citation61 The rate of ischemic or unspecified stroke was 0.92% per year for dabigatran 150 mg and 1.21% per year for warfarin (P = 0.03), and the rate of hemorrhagic stroke was 0.10% per year in the dabigatran 150 mg group compared with 0.38% per year in the warfarin group (P < 0.001). The rate of ICH was significantly lower for dabigatran 150 mg than with warfarin (0.32% vs 0.76% per year; P < 0.001). A lower dose of dabigatran (110 mg twice daily) was associated with a similar rate of stroke or systemic embolism compared with warfarin, but a lower rate of major bleeding. The rate of all-cause mortality was 4.13% per year in the warfarin group compared with 3.64% per year with 150 mg of dabigatran (P = 0.051) and 3.75% per year with 110 mg of dabigatran (P = 0.13).
In patients aged ≥ 75 years, dabigatran (150 mg)-treated patients had lower rates of stroke and systemic embolism (relative risk, 0.67; 95% CI, 0.49, 0.90) than warfarin-treated patients, and there was no significant difference in the rate of major bleeding (relative risk, 1.18; 95% CI, 0.98, 1.42).Citation62 Rates of stroke and hemorrhage were compared in subgroups aged < 75 years and ≥75 years: for dabigatran 150 mg, the rate of stroke or systemic embolism was 0.90% per year in patients aged < 75 years compared with 1.43% per year in patients aged ≥ 75 years. A similar difference between age groups was found among warfarin-treated patients (1.43% per year in patients aged < 75 years; 2.14% per year in patients aged ≥ 75 years). However, based on these age subgroups (< 75 and ≥75 years) the interaction between age and treatment for the outcome of stroke or systemic embolism was not significant (P = 0.81).
The interaction between age and treatment for major bleeding was significant (P < 0.001).Citation62 Dabigatran 150 mg twice daily compared with warfarin was associated with a lower risk of major bleeding in patients aged < 75 years (2.12% vs 3.04% per year; P < 0.001).
For patients aged ≥ 75 years, the risk of ICH was lower in dabigatran-treated patients (0.41% per year for dabigatran 150 mg vs 1.00% per year for warfarin).Citation62 Patients aged < 75 years had ICH rates of 0.26% per year for dabigatran 150 mg and 0.61% per year for warfarin. However, the test for interaction between age and treatment for ICH was not significant (P = 0.92).
The risk of MI in patients taking dabigatran has been investigated in a number of analyses. In RE-LY, the relative risk of MI was increased by 38% in patients treated with dabigatran 150 mg compared with warfarin (P = 0.048).Citation60 However, a re-analysis of the RE-LY results, including newly identified events, found no significant increase in MI among dabigatran-treated patients compared with warfarin-treated patients (relative risk, 1.27; P = 0.12).Citation61 A meta-analysis of seven dabigatran trials, across different indications, investigated risk of MI or acute coronary syndrome (ACS) associated with dabigatran. The analysis found that the risk of MI or ACS with dabigatran compared with warfarin was increased by 33% (P = 0.03) based on the original RE-LY results, and increased by 27% (P = 0.05) when the newly identified events from the RE-LY trial were added to this analysis.Citation63 A post-hoc analysis of the RE-LY results investigated risk of MI and risk of cardiac events based on an expanded definition, including MI, unstable angina, coronary artery bypass grafting, percutaneous coronary intervention, cardiac arrest, and cardiac death.Citation64 The analysis demonstrated no significant increase in MI with dabigatran compared with warfarin (hazard ratio [HR], 1.27; P = 0.12). Using the expanded definition of cardiac events, there was no statistically significant difference in event rates between the dabigatran 150 mg twice daily and warfarin groups (HR, 0.98; P = 0.77).
While the results from RE-LY demonstrated that both the 150 mg and 110 mg twice daily doses of dabigatran were safe and effective, the US Food and Drug Administration (FDA) approved only the 150 mg dose of dabigatran twice daily.Citation65 The FDA attempted to find a population for whom a lower dose would yield a more favorable balance between risks and benefits, given that dabigatran 110 mg twice daily demonstrated only non-inferiority in the overall population. Use of lower doses in patients with advanced age, impaired renal function, or a history of hemorrhage was considered, but the FDA did not find an improved benefit–risk profile with the lower dose. In assessing the benefit–risk profile, the benefit of superior efficacy in the prevention of stroke and systemic embolism with dabigatran 150 mg twice daily and the lack of a subgroup for whom a lower dose decreased risks led the FDA to approve only the 150 mg dose of dabigatran.
Rivaroxaban: ROCKET-AF
Rivaroxaban is a highly selective, direct factor Xa inhibitor taken orally once daily with the evening meal (20 mg). Inhibition of factor Xa prevents the development of thrombin, thereby disrupting the coagulation cascade and preventing the formation of blood clots.Citation55
The Rivaroxaban Once daily oral direct factor Xa inhibition Compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation (ROCKET-AF)Citation66 was a double-blinded global study. It included patients with AF and a history of prior stroke, transient ischemic attack, or non-neurologic systemic embolism. Patients received 20 mg of rivaroxaban or dose-adjusted warfarin. In total, 14,264 patients with a median age of 73 years and a mean CHADS2 score of 3.5 were assessed.
In ROCKET-AF, rivaroxaban was non-inferior to warfarin for the prevention of stroke (ischemic or hemorrhagic) or systemic embolism (HR for the intention-to-treat population, 0.88; 95% CI, 0.75, 1.03; P < 0.001 for non-inferiority).Citation66 Rates of major bleeding were not significantly different between the rivaroxaban and warfarin safety populations. There was no significant difference in the rate of ischemic stroke between treatment groups (P = 0.58); the rate of hemorrhagic stroke was 0.26% per year in the rivaroxaban group and 0.44% per year in the warfarin group (P = 0.02). Rates of MI were similar between treatment groups (P = 0.12). The rate of ICH was significantly reduced for rivaroxaban compared with warfarin (0.5% vs 0.7% per year; HR, 0.67; 95% CI, 0.47, 0.93; P = 0.02). In the intention-to-treat population, the rate of all-cause mortality did not differ between groups (P = 0.15).
A sub-analysis of ROCKET-AF investigated the efficacy and safety of rivaroxaban in patients aged ≥ 75 years, and investigators noted that the results for older patients were consistent with the overall study results.Citation67 There was no significant interaction between treatment and age for major bleeding (P = 0.34 for interaction). Rates of major bleeding in patients aged ≥ 75 years were 4.86% per year in the rivaroxaban group and 4.40% per year in the warfarin group, compared with 2.69% and 2.79% per year for patients aged < 75 years in the rivaroxaban and warfarin groups, respectively. Clinically relevant non-major bleeding was significantly higher for patients aged ≥ 75 years compared with patients aged < 75 years (P = 0.01). Based on the rates of ICH in patients aged ≥ 75 years (0.66% per year rivaroxaban vs 0.83% per year warfarin) and in patients aged < 75 years (0.37% per year rivaroxaban vs 0.68% per year warfarin), there was no significant interaction for ICH (P = 0.27 for interaction).
Apixaban
Apixaban is a highly selective direct factor Xa inhibitor that binds directly to factor Xa, preventing amplification of the coagulation process. Thrombin cannot be activated and clotting does not occur. Apixaban is taken orally, 5 mg twice daily.Citation56
ARISTOTLE
The Apixaban for Reduction In STroke and Other Throm-boemboLic Events in atrial fibrillation (ARISTOTLE) trial included patients with non-valvular AF.Citation68 Patients had one or more risk factors for stroke and received either apixaban (5 mg twice daily) or dose-adjusted warfarin. Patients randomized to treatment with apixaban received 2.5 mg twice daily if they met at least two of the following criteria: age ≥ 80 years, weight ≤ 60 kg, and/or a serum creatinine level ≥ 1.5 mg/dL. A total of 18,201 patients with a median age of 70 years and a mean CHADS2 score of 2.1 participated in the double-blinded trial.
In ARISTOTLE, apixaban reduced the risk of stroke or systemic embolism by 21% compared with warfarin; the effect of apixaban was statistically significant (P = 0.01) and demonstrated superiority of apixaban over warfarin for this primary outcome.Citation68 The rate of ischemic or uncertain strokes was similar in the two treatment arms. However, the rate of hemorrhagic stroke was significantly reduced in the apixaban group (0.24% per year) compared with the warfarin group (0.47% per year; HR, 0.51; 95% CI, 0.35, 0.75; P < 0.001).
The rate of major bleeding was 31% lower with apixaban (2.13% per year) compared with warfarin (3.09% per year; HR, 0.69; 95% CI, 0.60, 0.80; P < 0.001), and the rate of ICH was significantly reduced with apixaban versus warfarin (0.33% vs 0.80% per year; HR, 0.42; 95% CI, 0.30, 0.58; P < 0.001).Citation68 Rates of MI were similar between treatment groups (P = 0.37). All-cause mortality was significantly lower with apixaban than with warfarin (3.52% vs 3.94% per year; HR, 0.89; 95% CI, 0.80, 0.998; P = 0.047).
Overall, in the older patient subgroups (65–74 years and ≥ 75 years), the reductions in stroke and systemic embolism and in major bleeding with apixaban compared with warfarin were statistically significant and consistent with findings in the overall study population. Within the < 65 years age group, the differences between treatment groups in the rates of stroke and systemic embolism and major bleeding were not significant. The efficacy and safety of apixaban for stroke prevention in patients of advanced age with AF was also demonstrated in a sub-analysis of ARISTOTLE.Citation69 An age of 65 years or older was associated with an increased risk of stroke and bleeding in patients with AF based on risk-stratification scales such as the CHADS2 and HAS-BLED. The sub-analysis found that the efficacy and safety of apixaban were consistent across patients with different levels of risk for stroke or bleeding.
AVERROES
Apixaban Versus acEtylsalicylic acid to pRevent stROke in AF patients who have failed or are unsuitablE for vitamin K antagoniSt treatment (AVERROES)Citation70 was a NOAC study that included patients for whom warfarin treatment was unsuitable. The study included 5599 patients with AF who received apixaban (5 mg twice daily, or 2.5 mg twice daily in patients meeting specific criteria, as described for the ARISTOTLE trial) or aspirin. The mean age of the patients was 70 years and they had a mean CHADS2 score of 2.0.
The AVERROES trial was stopped early due to clear evidence of the benefit of apixaban over aspirin.Citation70 Apixaban reduced the risk of stroke or systemic embolism by 55% compared with aspirin (1.6% vs 3.7% per year; HR, 0.45; 95% CI, 0.32, 0.62; P < 0.001). Analysis of ischemic stroke risk showed a significant reduction for apixaban compared with aspirin (1.1% vs 3.0% per year; HR, 0.37; 95% CI, 0.25, 0.55; P < 0.001). The risk of ICH, hemorrhagic stroke, or major bleeding was not significantly different between the groups (P = 0.69, 0.45, and 0.57, respectively). Rates of MI were similar between treatment groups (P = 0.59). Rates of all-cause mortality were 3.5% per year in the apixaban group and 4.4% per year in the aspirin group (P = 0.07).
For AVERROES, the effects of apixaban compared with aspirin in the older patient (age ≥ 75 years) subgroups were consistent with effects in the overall study population.Citation70 Both apixaban and aspirin were well tolerated and no significant difference was observed for all-cause mortality rates (3.5% vs 4.4% per year; HR, 0.79; 95% CI, 0.62, 1.02; P = 0.07). Subgroup analysis showed that in patients treated with aspirin, the risk of stroke or systemic embolism was increased from 2.7% per year for those aged 65–74 years to 6.1% per year for those aged ≥ 75 years. The risk of major bleeding increased with age for both the aspirin and apixaban groups (aspirin: 0.5% per year for those aged < 65 years compared with 2.2% per year for those aged ≥ 75 years; apixaban: 0.7% per year for those aged < 65 years compared with 2.6% per year for those aged ≥ 75 years). This highlights the increased stroke risk in the elderly population.
Practical considerations for NOAC use in older patients
The NOACs have many benefits over warfarin for stroke prevention in patients with AF; however, treatment decisions also require an assessment of the practical considerations associated with these treatments including the need for dose adjustment in specific patients, cost-effectiveness, limitations in monitoring the extent of anticoagulation, and the lack of a specific reversal agent.
Such considerations are particularly important in the treatment of older patients, who may experience different reactions to drugs than younger patients. This is often due to older patients having poor renal clearance, a lower body weight, and polypharmacy.Citation71 Dabigatran exposure may be up to 1.3-times higher in the older population (≥75 years compared with patients aged 65–75 years).Citation72 Rivaroxaban results in increased plasma concentration levels (1.5-times higher) in the population aged ≥ 65 years compared with younger patients receiving the same dose.Citation55 Apixaban exposure has been reported 1.3-times higher in patients aged > 65 years.Citation73 Due to the age-related variation in drug exposure, modified dosing may be required for some elderly patients; however, this is primarily based on an assessment of renal function rather than age, per se.
Community-level data will be helpful in understanding the benefits and risks of these agents and physicians have begun to make observations in the clinical setting. Bleeding rates both higher and lower than those seen in clinical trials have been observed,Citation74,Citation75 and one study noted higher rates of bleeding in patients > 75 years of age.Citation75 The need for clarity around an optimal approach to dose adjustments with dabigatran and rivaroxaban for elderly patients, beyond the guidance currently provided in prescribing information will probably become more apparent as use of these agents in clinical practice increases.Citation76 Patients taking apixaban should be treated with a lower dose (2.5 mg twice daily) when they meet at least 2 of the following characteristics: age ≥ 80 years, body weight ≤ 60 kg, or serum creatinine ≥ 1.5 mg/dL. Therefore, elderly patients (≥ 80 years) should receive 2.5 mg twice daily if they also have body weight ≤ 60 kg or serum creatinine ≥ 1.5 mg/dL. Real-world experience will also be valuable as apixaban is used in clinical practice.
Adherence to dosing regimens and monitoring requirements may be a particular challenge for the elderly.Citation77 Patient education is required for elderly patients to highlight the importance of compliance, efficacy, and safety.Citation71 Patients and physicians need to understand the various therapeutic options and the corresponding benefits and risks.
Renal insufficiency
Renal insufficiency may affect drug exposure in older patients. The selection of anticoagulant therapy must be individualized according to patient characteristics, needs, and perceived risk of stroke or bleeding. For example, prescribing information for dabigatran recommends dose adjustment for renal impairment and notes an increased bleeding risk among patients aged > 75 years.Citation54 There have been two reported cases of prolonged bleeding time (one fatal) for patients treated with dabigatranCitation78; both patients were elderly with poor renal function and low body weight. In addition, a Japanese report identified 75 cases of serious bleeding in patients > 70 years of age. Mortalities included eight patients aged ≥ 75 years, seven of whom were >80 years old.Citation79
Renal clearance of dabigatran is higher than that of rivaroxaban and apixaban.Citation80 With dabigatran, in patients with a creatinine clearance (CrCl) of 30–50 mL/min, there is a 2.7-fold increase in exposure compared with patients with CrCl of 97–137 mL/min, and lower dosing is recommended in these patients.Citation54 Dabigatran is contraindicated in patients with severe renal impairment (CrCl < 30 mL/min). With rivaroxaban in patients with a CrCl of 30–49 mL/min, there is a 1.5-fold increase in exposure compared with patients with normal CrClCitation55 and a lower dose is recommended in patients with a CrCl of 15–50 mL/min. Rivaroxaban is not recommended for use in patients with a CrCl < 15 mL/min. With apixaban, there is a 1.29-fold increase in exposure in patients with moderate renal impairment (CrCl of 30–50 mL/min) but no dose adjustment for apixaban is required for patients with mild or moderate renal impairment and apixaban should be used with caution in patients with severe renal impairment (CrCl of 15–29 mL/min).Citation56 As described above, a lower dose of apixaban (2.5 mg twice daily) is indicated in patients meeting two of the following three criteria: age ≥ 80 years, body weight ≤ 60 kg, or serum creatinine ≥ 1.5 mg/dL. A sub-analysis of the ARISTOTLE trial looking at patients with a CrCl of 25 mL/min or higher divided into three different levels of renal function/impairment found that apixaban was more effective than warfarin at preventing stroke or systemic embolism and reducing mortality regardless of renal function.Citation81
Cost-effectiveness
Several studies assessing the cost-effectiveness of dabigatran compared with warfarin in elderly patients have been published. These suggest that dabigatran is cost-effective relative to warfarin for stroke prevention in patients with AF.Citation82–Citation84 Based on patients aged ≥ 70 years in the RE-LY trial, dabigatran 150 mg twice daily was cost-effective compared with warfarin in patients at high risk of hemorrhage, in patients at high risk of stroke unless INR control was excellent, and in patients with a prior stroke or transient ischemic attack.Citation82,Citation83 This study also found warfarin to be cost-effective in patients at moderate risk for stroke (CHADS2 score of 1–2), unless hemorrhagic risk was high or time in therapeutic range was low (< 57.1%). In addition, rivaroxaban appears to be cost-effective compared with warfarin.Citation85
Apixaban treatment also appears to be cost-effective. Among patients aged ≥ 70 years with a history of prior stroke or transient ischemic attack, apixaban would be cost-effective relative to warfarin assuming that it is introduced at a price similar to that of dabigatran.Citation86 Apixaban was also more effective and less costly than aspirin over a 10-year follow-up period based on a model developed using data from the AVERROES trial.Citation87 A study evaluating medical cost reductions associated with the use of individual NOACs compared with warfarin from the US payer perspective found lower medical costs with use of the NOACs (dabigatran, rivaroxaban, and apixaban) relative to warfarin, with apixaban offering the most substantial reduction in medical cost.Citation88
Monitoring and reversal of anticoagulant effect
Unlike the importance of monitoring INR with warfarin, routine monitoring is not required with NOACs, as they exhibit predictable therapeutic effects with fixed doses.Citation80 The INR cannot be used to measure the anticoagulant activity of these agents and there are no commercially available tests to monitor anticoagulation intensity with NOACs. This limits options for assessing treatment adherence and presents challenges in emergencies (eg, when there is active bleeding or the need for urgent medical procedures).
The anticoagulant effects of warfarin can be reversed using vitamin K or prothrombin complex concentrates (PCCs). There is currently no such pharmacologic antidote for the NOACs, but their shorter half-lives mean that the anticoagulant effect wanes rapidly once treatment is discontinuedCitation54–Citation56 and specific reversal agents are under development. It is possible that therapies such as recombinant factor VIIa and activated PCCs may be used to reverse the effects of direct factor Xa inhibitors and hemodialysis may be effective in removing dabigatran from the blood,Citation89 but PCCs have not been shown to be effective.Citation90 Activated PCCs mitigated the effect of rivaroxaban in healthy subjectsCitation90 and results from in vitro testing suggest that activated PCCs and recombinant factor VIIa may reverse the effect of apixaban.Citation91 Control of the bleeding site, regular fluids, and routine monitoring are advised for moderate bleeding. Hemodialysis for dabigatran and PCCs to enhance thrombin generation should be considered for life-threatening bleeding.Citation92,Citation93
Conclusion
This review highlights the benefits of NOACs for the elderly population with AF; these novel agents reduce stroke risk in this population, providing a suitable alternative to warfarin. The results from large randomized clinical trials provide a broad evidence base for the use of new anticoagulant therapies in patients with non-valvular AF at risk of stroke. Although the NOACs are often discussed collectively, consideration of the pharmacologic properties of individual agents may help clinicians to identify the most appropriate agent for individual patients. Properties such as drug metabolism and route of elimination may be important considerations in the treatment of stroke prevention in AF in specific patient groups, such as older patients with decreased renal function.
Despite the effectiveness of warfarin at lowering stroke risk in the elderly, this treatment has several disadvantages such as food restrictions, drug interactions and the need for frequent monitoring. NOACs such as dabigatran, rivaroxaban and apixaban overcome many of these disadvantages. They have a rapid onset of action, predictable anticoagulant effects that remove the requirement for routine coagulation monitoring and a low risk of drug-drug and drug-food interactions. Although clinical trials have not been powered to investigate differences between treatment groups within subgroups of older and younger patients, emerging data suggest that these agents are safe and have efficacy in patients of advanced age. However, the reduction in stroke risk must be balanced against the increased risk of bleeding in older patients and an antidote to reverse the anticoagulant effect of NOACs does not currently exist. Elderly patients must be evaluated carefully for impaired renal function which may increase the risk of bleeding.
Acknowledgments
Editorial support was provided by Bernadette Janas, PhD, and Meredith Kalish, MD, of Caudex Medical, and funded by Pfizer Inc and Bristol-Myers Squibb.
Disclosure
The author is an investigator for the RE-LY (Boehringer Ingelheim), ROCKET-AF (Bayer, Johnson & Johnson), and ARISTOTLE (Bristol-Myers Squibb/Pfizer Inc) clinical trials. In addition, he has been involved in clinical trials in various therapeutic areas sponsored by Gilead Sciences, Inc; Boehringer Ingelheim Pharma GmbH and Co; Eli Lilly and Company; Forest Pharmaceuticals; Bio-Cryst Pharmaceuticals; sanofi-aventis; Wyeth Research; Bristol-Myers Squibb; GlaxoSmithKline plc; Kowa; Pfizer Pharmaceuticals; Takeda Pharmaceuticals; Myogen; Akros Pharma, Inc; Novo Nordisk; Johnson and Johnson; Novartis; Alba; Mannkind Corporation; Ingenix, Inc; Auxilium; Ono Pharma USA, Inc; Merck; Amylin Pharmaceuticals; Acambis; AstraZeneca; Janssen Pharmaceutica; Schering-Plough; Perlegen; Kos; and Cubist Pharmaceuticals. Editorial support for this article was funded by Pfizer Inc and Bristol-Myers Squibb.
References
- WolfPAAbbottRDKannelWBAtrial fibrillation as an independent risk factor for stroke: the Framingham StudyStroke19912289839881866765
- WangTJMassaroJMLevyDA risk score for predicting stroke or death in individuals with new-onset atrial fibrillation in the community: the Framingham Heart StudyJAMA200329081049105612941677
- GoASHylekEMPhillipsKAPrevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) StudyJAMA2001285182370237511343485
- BenjaminEJWolfPAD’AgostinoRBSilbershatzHKannelWBLevyDImpact of atrial fibrillation on the risk of death: the Framingham Heart StudyCirculation199898109469529737513
- HannonNSheehanOKellyLStroke associated with atrial fibrillation–incidence and early outcomes in the north Dublin population stroke studyCerebrovasc Dis2010291434919893311
- KannelWBWolfPABenjaminEJLevyDPrevalence, incidence, prognosis, and predisposing conditions for atrial fibrillation: population-based estimatesAm J Cardiol1998828A2N9N
- MiyasakaYBarnesMEBaileyKRMortality trends in patients diagnosed with first atrial fibrillation: a 21-year community-based studyJ Am Coll Cardiol200749998699217336723
- PenadoSCanoMAchaOHernándezJLRianchoJAAtrial fibrillation as a risk factor for stroke recurrenceAm J Med2003114320621012637135
- StewartSHartCLHoleDJMcMurrayJJA population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley studyAm J Med2002113535936412401529
- VidailletHGranadaJFChyouPHA population-based study of mortality among patients with atrial fibrillation or futterAm J Med2002113536537012401530
- FitzmauriceDAHobbsFDRJowettSScreening versus routine practice in detection of atrial fibrillation in patients aged 65 or over: cluster randomised controlled trialBMJ2007335761638317673732
- GageBFWatermanADShannonWBoechlerMRichMWRadfordMJValidation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial FibrillationJAMA2001285222864287011401607
- LipGYNieuwlaatRPistersRLaneDACrijnsHJRefining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the Euro Heart Survey on atrial fibrillationChest2010137226327219762550
- HoKKPinskyJLKannelWBLevyDThe epidemiology of heart failure: the Framingham StudyJ Am Coll Cardiol1993224 Suppl A6A13A8509564
- National Center for Health StatisticsBlood Pressure Levels in Persons 18–74 Years of Age in 1976–1980 and Trends in Blood Pressure from 1960 to 1980 in the United States Vital and Health Statistics, series 11Washington DCUS Government Printing Office1986 DHHS publication 86-1684
- WilsonPWAndersonKMKannelWBEpidemiology of diabetes mellitus in the elderly. The Framingham StudyAm J Med1986805A393706388
- SinnaevePRBrueckmannMClemensAOldgrenJEikelboomJHealeyJSStroke prevention in elderly patients with atrial fibrillation: challenges for anticoagulationJ Intern Med20122711152421995885
- AguilarMIHartROral anticoagulants for preventing stroke in patients with non-valvular atrial fibrillation and no previous history of stroke or transient ischemic attacksCochrane Database Syst Rev20053CD00192716034869
- van WalravenCHartRGConnollySEffect of age on stroke prevention therapy in patients with atrial fibrillation: the atrial fibrillation investigatorsStroke20094041410141619182090
- HylekEMD’AntonioJEvans-MolinaCSheaCHenaultLEReganSTranslating the results of randomized trials into clinical practice: the challenge of warfarin candidacy among hospitalized elderly patients with atrial fibrillationStroke20063741075108016527999
- DeplanqueDLeysDParnettiLSAFE II InvestigatorsStroke prevention and atrial fibrillation: reasons leading to an inappropriate management. Main results of the SAFE II studyBr J Clin Pharmacol200457679880615151526
- GoASHylekEMBorowskyLHPhillipsKASelbyJVSingerDEWarfarin use among ambulatory patients with nonvalvular atrial fibrillation: the anticoagulation and risk factors in atrial fibrillation (ATRIA) studyAnn Intern Med19991311292793410610643
- Allen LaPointeNMGovernaleLWatkinsJMulgundJAnstromKJOutpatient use of anticoagulants, rate-controlling drugs, and antiarrhythmic drugs for atrial fibrillationAm Heart J2007154589389817967595
- BrophyMTSnyderKEGaehdeSIvesCGagnonDFioreLDAnticoagulant use for atrial fibrillation in the elderlyJ Am Geriatr Soc20045271151115615209654
- PartingtonSLAbidSTeoKOczkowskiWO’DonnellMJPreadmission warfarin use in patients with acute ischemic stroke and atrial fibrillation: the appropriate use and barriers to oral anticoagulant therapyThromb Res2007120566366917434577
- SavageMTeelingMBennettKFeelyJAdherence to clinical guidance in the prescribing of oral antithrombotic medication in patients with atrial fibrillationIr J Med Soc200617524649
- Bristol-Myers SquibbCoumadin® (warfarin sodium) [prescribing information]New York, NYBristol-Myers Squibb2011 Available from: http://packageinserts.bms.com/pi/pi_coumadin.pdfAccessed August 8, 2012
- GattellariMWorthingtonJZwarNMiddletonSBarriers to the use of anticoagulation for nonvalvular atrial fibrillation: a representative survey of Australian family physiciansStroke200839122723018048861
- ReynoldsMWFahrbachKHauchOWarfarin anticoagulation and outcomes in patients with atrial fibrillation: a systematic review and metaanalysisChest200412661938194515596696
- EsmerioFGSouzaENLeiriaTLLunelliRMoraesMAConstant use of oral anticoagulants: implications in the control of their adequate levelsArg Bras Cardiol2009935549554
- ReynoldsMRShahJEssebagVPatterns and predictors of warfarin use in patients with new-onset atrial fibrillation from the FRACTAL RegistryAm J Cardiol200697453854316461052
- WanYHeneghanCPereraRAnticoagulation control and prediction of adverse events in patients with atrial fibrillation: a systematic reviewCirc Cardiovasc Qual Outcomes200812849120031794
- BakerWLCiosDASanderSDColemanCIMeta-analysis to assess the quality of warfarin control in atrial fibrillation patients in the United StatesJ Manag Care Pharm200915324425219326955
- van WalravenCJenningsAOakeNFergussonDForsterAJEffect of study setting on anticoagulation control: a systematic review and metaregressionChest200612951155116616685005
- MasakiNSuzukiMMatsumuraAMaruyamaYHashimotoYQuality of warfarin control affects the incidence of stroke in elderly patients with atrial fibrillationIntern Med201049161711171620720347
- HobbsFDRoalfeAKLipGYFletcherKFitzmauriceDAMantJBirmingham Atrial Fibrillation in the Aged Investigators and Midland Research Practices Consortium NetworkPerformance of stroke risk scores in older people with atrial fibrillation not taking warfarin: comparative cohort study from BAFTA trialBMJ2011342d365321700651
- RuttenFHHakEStalmanWAVerheijTJHoesAWIs treatment of atrial fibrillation in primary care based on thromboembolic risk assessment?Fam Pract2003201162112509365
- PistersRLaneDANieuwlaatRde VosCBCrijnsHJLipGYA novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart SurveyChest201013851093110020299623
- GageBFYa nYMilliganPEClinical classification schemes for predicting hemorrhage: results from the National Registry of Atrial Fibrillation (NRAF)Am Heart J2006151371371916504638
- FangMCGoASChangYA new risk scheme to predict warfarin-associated hemorrhage: The ATRIA (Anticoagulation and Risk Factors in Atrial Fibrillation) StudyJ Am Coll Cardiol201158439540121757117
- ApostolakisSLaneDAGuoYBullerHLipGYPerformance of the HEMORR(2)HAGES, ATRIA, and HAS-BLED bleeding risk-prediction scores in patients with atrial fibrillation undergoing anticoagulation: the AMADEUS (evaluating the use of SR34006 compared to warfarin or acenocoumarol in patients with atrial fibrillation) studyJ Am Coll Cardiol201260986186722858389
- BondAJMolnarFJLiMMackeyMMan-Son-HingMThe risk of hemorrhagic complications in hospital in-patients who fall while receiving antithrombotic therapyThromb J200531115638939
- Man-Son-HingMLaupacisAAnticoagulant-related bleeding in older persons with atrial fibrillation: physicians’ fears often unfoundedArch Intern Med2003163131580158612860581
- Man-Son-HingMNicholGLauALaupacisAChoosing antithrombotic therapy for elderly patients with atrial fibrillation who are at risk for fallsArch Intern Med1999159767768510218746
- KhreizatHSWhittakerPCurtisKDTurloGGarwoodCLThe effect of cognitive impairment in the elderly on the initial and long-term stability of warfarin therapyDrugs Aging201229430731722462629
- FihnSDCallahanCMMartinDCMcDonellMBHenikoffJGWhiteRHThe risk for and severity of bleeding complications in elderly patients treated with warfarin. The National Consortium of Anticoagulation ClinicsAnn Intern Med1996124119709798624064
- Authors/Task Force MembersCammAJLipGY2012 focused update of the ESC Guidelines for the management of atrial fibrillation: An update of the 2010 ESC Guidelines for the management of atrial fibrillation * Developed with the special contribution of the European Heart Rhythm AssociationEur Heart J201233212719274722922413
- FusterVRydénLECannomDS2011 ACCF/AHA/HRS focused updated incorporated into the ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines developed in partnership with the European Society of Cardiology and in collaboration with the European Heart Rhythm Association and the Heart Rhythm SocietyCirculation201112310e269e36721382897
- YouJJSingerDEHowardPAAmerican College of Chest PhysiciansAntithrombotic therapy for atrial fibrillation: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice GuidelinesChest2012141Suppl 2e531Se575S22315271
- SatoHIshikawaKKitabatakeAJapan Atrial Fibrillation Stroke Trial GroupLow-dose aspirin for prevention of stroke in low-risk patients with atrial fibrillation: Japan Atrial Fibrillation Stroke TrialStroke200637244745116385088
- OlesenJBLipGYLindhardsenJRisks of thromboembolism and bleeding with thromboprophylaxis in patients with atrial fibrillation: A net clinical benefit analysis using a ‘real world’ nationwide cohort studyThromb Haemost2011106473974921789337
- MantJHobbsFDRFletcherKWarfarin versus aspirin for stroke prevention in an elderly community population with atrial fibrillation (the Birmingham Atrial Fibrillation Treatment of the Aged Study, BAFTA): a randomised controlled trialLancet2007370958649350317693178
- RashADownesTPortnerRYeoWWMorganNChannerKSA randomised controlled trial of warfarin versus aspirin for stroke prevention in octogenarians with atrial fibrillation (WASPO)Age Ageing200736215115617175564
- Boehringer IngelheimPradaxa® (dabigatran etexilate mesylate) [prescribing information]Ridgefeld, CTBoehringer Ingelheim2012 Available from: http://bidocs.boehringer-ingelheim.com/BIWebAccess/ViewServlet.ser?docBase=renetnt&folderPath=/Prescribing%20Information/PIs/Pradaxa/Pradaxa.pdfAccessed February 25, 2013
- Bayer PharmaXarelto® (rivaroxaban) [prescribing information]LeverkusenBayer Pharma2011 Available from: http://www.xareltohcp.com/sites/default/files/pdf/xarelto_0.pdf#zoom=100Accessed February 25, 2013
- Bristol-Myers SquibbEliquis® (apixaban) [prescribing information]Princeton, NJBristol-Myers Squibb2012 Available from: http://packageinserts.bms.com/pi/pi_eliquis.pdfAccessed January 4, 2013
- RuffCTBraunwaldEWill warfarin ever be replaced?J Cardiovasc Pharmacol Ther201015321021920484119
- GuyattGHAklEACrowtherMGuttermanDDSchuünemannHJAmerican College of Chest Physicians Antithrombotic Therapy and Prevention of Thrombosis PanelExecutive summary: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice GuidelinesChest20121417S47S22315257
- WannLSCurtisABEllenbogenKA2011 ACCF/AHA/HRS focused update on the management of patients with atrial fibrillation (update on dabigatran): a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelinesJ Am Coll Cardiol201157111330133721324629
- ConnollySJEzekowitzMDYusufSRE-LY Steering Committee and InvestigatorsDabigatran versus warfarin in patients with atrial fibrillationN Engl J Med2009361121139115119717844
- ConnollySJEzekowitzMDYusufSReillyPAWallentinLRandomized Evaluation of Long-Term Anticoagulation Therapy InvestigatorsNewly identified events in the RE-LY trialN Engl J Med2010363191875187621047252
- EikelboomJWWallentinLConnollySJRisk of bleeding with 2 doses of dabigatran compared with warfarin in older and younger patients with atrial fibrillation: an analysis of the randomized evaluation of long-term anticoagulant therapy (RE-LY) trialCirculation2011123212363237221576658
- UchinoKHernandezAVDabigatran association with higher risk of acute coronary events: meta-analysis of noninferiority randomized controlled trialsArch Intern Med2012172539740222231617
- HohnloserSHOldgrenJYangSMyocardial ischemic events in patients with atrial fibrillation treated with dabigatran or warfarin in the RE-LY (Randomized Evaluation of Long-Term Anticoagulation Therapy) trialCirculation2012125566967622215856
- BeasleyBNUngerEFTempleRAnticoagulant options–why the FDA approved a higher but not a lower dose of dabigatranN Engl J Med2011364191788179021488759
- PatelMRMahaffeyKWGargJROCKET AF InvestigatorsRivaroxaban versus warfarin in nonvalvular atrial fibrillationN Engl J Med20113651088389121830957
- HalperinJLWojdylaDPicciniJPEfficacy and safety of rivaroxaban compared with warfarin among elderly patients with nonvalvular AF in the ROCKET-AF trialStroke201243A148
- GrangerCBAlexanderJHMcMurrayJJARISTOTLE Committees and InvestigatorsApixaban versus warfarin in patients with atrial fibrillationN Engl J Med20113651198199221870978
- LopesRDAl-KhatibSMWallentinLefficacy and safety of apixaban compared with warfarin according to patient risk of stroke and of bleeding in atrial fibrillation: a secondary analysis of a randomised controlled trialLancet201238098551749175823036896
- ConnollySJEikelboomJJoynerCAVERROES Steering Committee and InvestigatorsApixaban in patients with atrial fibrillationN Engl J Med2011364980681721309657
- GurwitzJHFieldTSHarroldLRIncidence and preventability of adverse drug events among older persons in the ambulatory settingJAMA200328991107111612622580
- Boehringer Ingelheim LimitedPradaxa® (Dabigatran) [summary of product characteristics]Electronic Medicines Compendiumupdated 9212012 Available from: http://www.medicines.org.uk/EMC/medicine/24839/SPC/Pradaxa+150+mg+hard+capsules/Accessed January 3, 2013
- Bristol-Myers Squibb–PfizerEliquis® (Apixaban) [summary of product characteristics]Electronic Medicines Compendiumupdated 3122012 Available from: http://www.medicines.org.uk/EMC/medicine/24988/SPC/Eliquis+2.5+mg+film-coated+tablets/Accessed February 3, 2012
- ParikhVChainaniVHowardMIs dabigatran safe in “real life”?J Am Coll Cardiol20125913s1E602
- RajdevABradleyJPetriniJAlexanderJA community experience of the novel anticoagulant PradaxaJ Am Coll Cardiol20125913s1E601
- SkanesACHealeyJSCairnsJACanadian Cardiovascular Society Atrial Fibrillation Guidelines CommitteeFocused 2012 update of the Canadian Cardiovascular Society atrial fibrillation guidelines: recommendations for stroke prevention and rate/rhythm controlCan J Cardiol201228212513622433576
- KimmelSEChenZPriceMThe influence of patient adherence on anticoagulation control with warfarin: results from the International Normalized Ratio Adherence and Genetics (IN-RANGE) StudyArch Intern Med2007167322923517296877
- LegrandMMateoJAribaudAThe use of dabigatran in elderly patientsArch Intern Med2011171141285128621788545
- [Deaths of 15 patients as a side effect five months after commercial release: interim report survey]National Purazakisa2011928 Available from: http://www.mixonline.jp/tabid/55/artid/41434/Default.aspxAccessed January 31, 2013Japanese
- ErikssonBIQuinlanDJEikelboomJWNovel oral factor Xa and thrombin inhibitors in the management of thromboembolismAnnu Rev Med201162415721226611
- HohnloserSHHijaziZThomasLefficacy of apixaban when compared with warfarin in relation to renal function in patients with atrial fibrillation: insights from the ARISTOTLE trialEur Heart J201233222821283022933567
- KamelHJohnstonSCEastonJDKimASCost-effectiveness of dabigatran compared with warfarin for stroke prevention in patients with atrial fibrillation and prior stroke or transient ischemic attackStroke201243388188322308255
- ShahSVGageBFCost-effectiveness of dabigatran for stroke prophylaxis in atrial fibrillationCirculation2011123222562257021606397
- FreemanJVZhuRPOwensDKCost-effectiveness of dabigatran compared with warfarin for stroke prevention in atrial fibrillationAnn Intern Med2011154111121041570
- LeeSAngladeMWPhamDPisacaneRKlugerJColemanCICosteffectiveness of rivaroxaban compared to warfarin for stroke prevention in atrial fibrillationAm J Cardiol2012110684585122651881
- KamelHEastonJDJohnstonSCKimASCost-effectiveness of apixaban vs warfarin for secondary stroke prevention in atrial fibrillationNeurology201279141428143422993279
- LeeSAngladeMWMengJHagstromKKlugerJColemanCICost-effectiveness of apixaban compared with aspirin for stroke prevention in atrial fibrillation among patients unsuitable for warfarinCirc Cardiovasc Qual Outcomes20125447247922740012
- DeitelzweigSAminAJingYMedical cost reductions associated with the usage of novel oral anticoagulants vs warfarin among atrial fibrillation patients, based on the RE-LY, ROCKET-AF, and ARISTOTLE trialsJ Med Econ201215477678522449118
- De CaterinaRHustedSWallentinLCoordinating CommitteeNew oral anticoagulants in atrial fibrillation and acute coronary syndromes: ESC Working Group on Thrombosis-Task Force on Anticoagulants in Heart Disease position paperJ Am Coll Cardiol201259161413142522497820
- EerenbergESKamphuisenPWSijpkensMKMeijersJCBullerHRLeviMReversal of rivaroxaban and dabigatran by prothrombin complex concentrate: a randomized, placebo-controlled, crossover study in healthy subjectsCirculation2011124141573157921900088
- EscolarGArellano-RodrigoEReverterJCReversal of apixaban induced alterations of hemostasis by different coagulation factor concentrates: studies in vitro with circulating human bloodCirculation20121264520521
- BarillariGPascaSBarillariADe AngelisVEmergency reversal of anticoagulation: from theory to real use of prothrombin complex concentrates. A retrospective Italian experienceBlood Transfus2012101879422044952
- BruceDNokesTJProthrombin complex concentrate (Beriplex P/N) in severe bleeding: experience in a large tertiary hospitalCrit Care2008124R10518706082
- WolfPAAbbottRDKannelWBAtrial fibrillation: a major contributor to stroke in the elderly. The Framingham StudyArch Intern Med19871479156115643632164