
Abstract
Background
Neonatal hypoxic-ischemic encephalopathy (HIE) leads to different degree of neurological sequelae. The incidence of HIE is relatively high, and the risk factors associated with HIE are still controversial. It is necessary to identify the risk factors associated with HIE.
Methods
A total of 258 neonates (110 HIE patients and 148 controls) were enrolled in this study. The characteristics of pregnant women and fetuses during pregnancy and delivery were compared between HIE patients and controls, and the risk factors of HIE were analyzed.
Results
The proportions of premature infants, low-birth-weight infants and the levels of 1-minute Apgar score, 5-minute Apgar score in HIE group were significantly lower than those in control group, while the proportion of amniotic fluid contamination in the HIE group was significantly higher than those of the controls. When HIE was taken as the end point of 1-minute Apgar score, and 5-minute Apgar score, the cut-off value of 1-minute Apgar score was 3, and 5-minute Apgar score was 7 by receiver operating characteristic (ROC) curve analysis. The results of multivariate logistic regression analysis showed that low birth weight (<2.5 kg) (OR 1.780, 95% CI: 0.124–25.463, P=0.016), amniotic fluid contamination (OR 3.223, 95% CI: 1.049–9.901, P=0.041), low 1-minute Apgar score (≤3) (OR 92.425, 95% CI: 15.522–550.343, P<0.001), and low 5-minute Apgar score (≤7) (OR 12.641, 95% CI: 2.894–55.227, P=0.001) may increase risk of HIE. In addition, amniotic fluid contamination, low 1-minute Apgar score (≤3), and low 5-minute Apgar score (≤7) may increase risk of HIE among newborns born to women without previous childbearing history, but not in newborns born to women with previous childbearing history.
Conclusion
Low birth weight (<2.5 kg), amniotic fluid contamination, low 1-minute Apgar score (≤3), and 5-minute Apgar score (≤7) may increase risk of HIE.
Introduction
Neonatal hypoxic-ischemic encephalopathy (HIE) refers to the various degrees of brain injury due to suffocation caused by partial or total lack of oxygen, reduce or suspend of the cerebral blood flow during the perinatal period.Citation1 It is a common central nervous system disease in fetuses or neonates, and severe children can be the legacy of different degree of neurological sequelae. Globally, the incidence of HIE in full-term live infants ranges from 1 to 8 per 1000, and even in developed countries, the incidence is 1.5 to 2 per 1000.Citation2 Around 400,000 babies develop neurodevelopmental disorders caused by HIE worldwide each year.Citation3 HIE affects about 100,000 infants each year in China.Citation4
HIE can be divided into different levels according to the evaluation system. At present, there are several major scoring systems for HIE evaluation in clinical practice. Thompson score is a scoring system created by Thompson et al in 1997 to predict the neurodevelopmental outcomes of HIE patients.Citation5 While the Sarnat scoring system defines most characteristics of the three stages.Citation6 Apgar score was first introduced in 1952 by an American anesthesiologist named Virginia Apgar, and it is a widely utilized tool in neonates to describe an infant’s condition after birth.Citation7 Generally speaking, HIE can be divided into mild, moderate and severe hypoxic-ischemic encephalopathy.Citation8,Citation9
At present, the risks of HIE are mainly based on the characteristics of pregnant women and fetuses during pregnancy and delivery. Due to maternal or fetal abnormalities, fetal dyspepsia leads to fetal brain asphyxia leading to neuronal destruction, which may evolve into ischemic hypoxic encephalopathy.Citation10 One study has shown that the risk of HIE is higher in the presence of fetal growth restriction, nonreassuring cardiotocography, emergency cesarean section, meconium contamination, and chorioamnionitis.Citation11 Umbilical cord pathology, inflammatory changes in the placenta, and placental weight were associated with HIE.Citation12 Intrapartum period risk factors appear to be important for the development of HIE.Citation13 Placenta previa, medicals during pregnancy, fetal distress, abnormal labor stage, Apgar score, amniotic fluid contamination, and cesarean section were independent risk factors for HIE.Citation14 However, a study has found that mode of delivery and premature rupture of membrane have nothing to do with HIE.Citation11 There are still some inconsistent results in the study of HIE risk factors. It is necessary to identify the risk factors associated with HIE. Due to the variety of risk factors causing HIE, this study adopted the retrospective case-control study method to analyze the related factors in the whole perinatal period of pregnant women, and adopted the logistic regression analysis methods to screen the related risk factors.
Materials and Methods
Subjects
A total of 110 neonates with HIE admitted to Meizhou People’s Hospital from January 2016 to May 2022 were selected as the observation group, including 76 males and 34 females. A total of 148 neonates without HIE in the same period were selected as the control group, including 99 males and 49 females. Neonates were diagnosed as HIE according to “Diagnosis of Hypoxic-ischemic Encephalopathy in Term Infants”,Citation15 “Guideline of Evidence-based Treatment for Hypoxic-ischemic Encephalopathy in Term Infants”,Citation16 and “Protocol of Hypothermia Treatment for Hypoxic-ischemic Encephalopathy in Neonates”.Citation4
Inclusion criteria were as follows: (1) all neonates met the diagnostic criteria of hypoxic-ischemic encephalopathy formulated by the neonatal Group of the Pediatric Society of Chinese Medical AssociationCitation15; (2) all the neonates were confirmed as hypoxic-ischemic encephalopathy by magnetic resonance imaging (MRI) or computed tomography (CT) examination; (3) clinical data were complete. Exclusion criteria were as follows: (1) severe cardiac, liver and kidney dysfunction at birth; (2) neonates with hematological diseases; (3) neonates with congenital genetic diseases; (4) neonates with convulsions caused by childbirth injury and intracranial hemorrhage.
Observed Indicators
Clinical data of the two groups of neonates and their mothers were collected, including (1) maternal factors: pregnancy history, pregnancy conditions (amniotic fluid contamination, placental abnormalities, nuchal cord, pregnancy history); (2) fetal factors: gestational age, gender, birth weight, 1-minute Apgar score, and 5-minute Apgar score; and (3) delivery factors: delivery mode, and so on.
Statistical Analyses
Data analysis was performed using SPSS 21.0 (IBM Inc., USA). The measurement data were expressed as mean±standard deviation (SD), and the distributions of continuous variables were evaluated by Student’s t-test or the Mann–Whitney U-test. Demographics and clinical characteristics of infants were calculated by χ2 test. In this study, newborns were classified as premature infant (<37 weeks), full-term infant (37–42 weeks), and postterm infant (>42 weeks) according to neonatal gestational age at birth. Neonatal birth weight was categorized as low birth weight (1500–2499 g), normal birth weight (2500–4000 g), and macrosomia (>4000 g). When HIE was taken as the end point of birth weight, receiver operating characteristic (ROC) curve analysis was used to determine the optimal cut-off values of 1-minute Apgar score, and 5-minute Apgar score. Logistic regression analysis was applied to assess the association between the characteristics of pregnant women and fetuses during pregnancy and delivery and HIE. P<0.05 was considered statistically significant.
Results
A total of 258 neonates (110 HIE patients and 148 controls) were enrolled in this study, including 175 male neonates (67.8%) and 83 female neonates (32.2%). A total of 149 cases (57.8%) delivered by vaginal delivery, 109 cases (42.2%) delivered by cesarean section. There were 68 cases (26.4%) whose gestational age was <37 weeks at the time of delivery, and 190 cases (73.6%) whose gestational age was 37–42 weeks. There were 63 cases (24.4%), 186 cases (72.1%), and 9 cases (3.5%) with the birth weight <2.5 kg, 2.5–4.0 kg, and >4.0 kg, respectively. Sixty-one mothers (23.6%) of these newborns had a history of adverse pregnancy. Amniotic fluid contamination occurred in 81 cases (31.4%), nuchal cord occurred in 62 cases (24.0%), and placental abnormality occurred in 9 cases (3.5%). The 1-minute Apgar score and 5-minute Apgar score were 6.16±3.54 and 7.91±2.57, respectively ().
Table 1 Comparison of Clinical Characteristics between the Two Groups
The proportion of premature infants in the HIE group was lower than that in the control group (16.4% vs 33.8%, P=0.003). The proportion of low-birth-weight infants in the HIE group was lower than that in the control group (12.7% vs 33.1%, P<0.001). And the proportion of amniotic fluid contamination in the HIE group was significantly higher than that in the control group (47.3% vs 19.6%, P<0.001), and the proportion of nuchal cord was significantly lower than that of the control group (16.4% vs 29.7%, P=0.002). In addition, the 1-minute Apgar score (2.72±2.06 vs 8.72±1.80, P<0.001) and 5-minute Apgar score (5.72±2.38 vs 9.53±1.05, P<0.001) were significantly lower in the HIE group than those in the control group. There were no statistically significant differences between the two groups in proportion of gender, mode of delivery, adverse pregnancy history, and placental abnormality ().
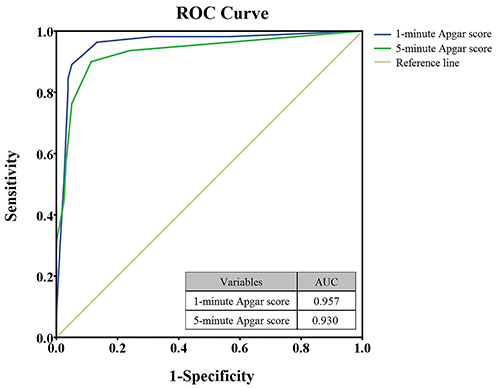
Receiver operating characteristic (ROC) curve analysis was used to determine the optimal cut-off values of 1-minute Apgar score, and 5-minute Apgar score. When HIE was taken as the end point of 1-minute Apgar score, and 5-minute Apgar score, the cut-off value of 1-minute Apgar score was 3 (the area under the receiver operating characteristic [ROC] curve [AUC] was 0.957) and for 5-minute Apgar score was 7 (the AUC was 0.930) (). The results of multivariate logistic regression showed that low birth weight (<2.5 kg) (odds ratio (OR) 1.780, 95% confidence interval (CI): 0.124–25.463, P=0.016), amniotic fluid contamination (OR 3.223, 95% CI: 1.049–9.901, P=0.041), low 1-minute Apgar score (≤3) (≤3 vs >3, OR 92.425, 95% CI: 15.522–550.343, P<0.001), and low 5-minute Apgar score (≤7) (≤7 vs >7, OR 12.641, 95% CI: 2.894–55.227, P=0.001) may increase risk of HIE in infants ().
Table 2 Logistic Regression Analysis of Risk of Neonatal Hypoxic-Ischemic Encephalopathy
Figure 1 ROC curves of 1-minute Apgar score and 5-minute Apgar score for HIE.
According to the reproductive history of the mothers (with or without previous childbearing history) of these newborns, the subjects were divided into two groups: those with at least one childbearing history and those without childbearing history, and logistic regression analysis was conducted respectively. Among newborns born to women without previous childbearing history, the results of multivariate logistic regression showed that amniotic fluid contamination (OR 5.695, 95% CI: 1.345–24.120, P=0.018), low 1-minute Apgar score (≤3) (≤3 vs >3, OR 32.518, 95% CI: 3.326–317.891, P=0.003), and low 5-minute Apgar score (≤7) (≤7 vs >7, OR 15.411, 95% CI: 2.570–92.417, P=0.003) may increase risk of HIE. In newborns born to women with previous childbearing history, gender, mode of delivery, gestational age, birth weight, adverse pregnancy history, amniotic fluid contamination, nuchal cord, placenta abnormality, 1-minute Apgar score, and 5-minute Apgar score were not associated with HIE ().
Table 3 Independent Risk Factors of Hypoxic-Ischemic Encephalopathy in Neonates Born to Women with or without Previous Childbearing History
Discussion
Many factors can contribute to the development of HIE. A series of fetal and maternal factors including fetal gender, mode of delivery, gestational age at birth, birth weight, adverse pregnancy history, amniotic fluid, umbilical cord, placenta, and Apgar score were included in this study. This retrospective cohort study showed that birth weight, amniotic fluid contamination, 1-minute Apgar score, and 5-minute Apgar score may have some effect on HIE. Specifically, the low birth weight (<2.5 kg), amniotic fluid contamination, low 1-minute Apgar score (≤3), and low 5-minute Apgar score (≤7) may increase risk of HIE in infants. In addition, in newborns born to women without previous childbearing history, amniotic fluid contamination, low 1-minute Apgar score (≤3), and low 5-minute Apgar score (≤7) may increase the risk of HIE in infants.
Neonatal hypoxia-ischemia is a common occurrence in low-birth-weight infants. Studies have shown that the infants who developed HIE had significantly lower birth weight than the infants who did not develop HIE.Citation17,Citation18 Low birth weight significantly increased the risk of neonatal moderate or severe HIE.Citation19 Birth weight less than 3.0kg or greater than 4.0kg is a risk factor for moderate-to-severe neonatal HIE.Citation20 In the present study, low birth weight was an independent risk factor for HIE. Our results are consistent with those of previous studies. In one study, a cohort of infants with perinatal asphyxia was analyzed based on machine learning methods, and a predictive risk model for HIE was constructed using some clinical indicators such as Apgar score, maternal age, and infant birth weight.Citation21
Amniotic fluid contamination was an independent risk factor for HIE.Citation14 And meconium-stained amniotic fluid was significantly associated with HIE.Citation22 Moderate-to-heavy meconium stained amniotic fluid is a risk factor for HIE.Citation13 Amniotic fluid contamination significantly increased the risk of neonatal moderate or severe HIE.Citation19 Meconium stained liquor is a major risk factor for birth asphyxia, so amniotic fluid contamination is also one of the risk factors for HIE.Citation23 Our results are consistent with the results of these researches.
Apgar score is used as an indicator to judge the degree of neonatal asphyxia. The lower the Apgar score is, the more severe the degree of neonatal asphyxia is.Citation24 Some studies have shown that low Apgar score was an independent risk factor for HIE.Citation14 1-min Apgar score <7 significantly increased the risk of neonatal moderate or severe HIE.Citation19 The Apgar score is the most commonly used score to quantify the postnatal state of the newborn, especially after fetal asphyxia.Citation25 In one study, a cohort of infants with perinatal asphyxia was analyzed based on machine learning methods to construct a predictive risk model for HIE, incorporating clinical indicators including Apgar score.Citation21
In addition, gender of neonate, mode of delivery, gestational age, adverse pregnancy history, nuchal cord, and placenta abnormality were not associated with the risk of HIE in this study. Studies have shown that male fetuses are prone to HIE.Citation26,Citation27 The difference of HIE between males and females may be related to the difference of steroid hormone level and motor function level between males and females.Citation28 About mode of delivery, cesarean section was an independent risk factor for HIE.Citation14 Another study also showed that HIE was associated with mode of delivery other than unassisted vaginal birth.Citation29 However, the results of this study showed that delivery mode was not associated with the risk of HIE. In addition, gestational age was an antepartum risk factor for moderate-to-severe HIE.Citation20 Another study has shown that gestational age ≥41 weeks was associated with HIE.Citation30 In the present study, gestational age was not an antepartum risk factor for HIE. One study has shown that nuchal cord was associated with HIE,Citation30 but not shown in this study.
HIE is also associated with a number of other factors: gestational hypertension is positively associated with the risk of neonatal HIECitation31; maternal age ≥35 years as a potential risk factor for HIECitation32; fetal blood advanced oxidation protein products (AOPP) and non-protein-bound iron (NPBI) can be used as early diagnostic markers of HIE.Citation27 HIE is associated with the polymorphisms in angiotensinogen (AGT) gene,Citation33 tachykinin receptor 3 (TACR3) gene,Citation34 caspase recruitment domain family member 8 (CARD8) gene,Citation35,Citation36 nitric oxide synthase 3 (NOS3) gene,Citation37,Citation38 oligodendrocyte transcription factor (OLIG2) gene,Citation39 but not associated with the polymorphisms in hypoxia-inducible factor 1 subunit alpha (HIF1A) functional polymorphisms.Citation40 Some non-coding RNAs may also play an important role in the development of HIE, such as microRNA-210,Citation41 microRNA-30b,Citation42 microRNA-204,Citation43 microRNA-374a-5p,Citation44 microRNA-139-5p,Citation45 microRNA-363-3p,Citation46 and so on.
Overall, the risk of HIE is associated with multiple factors, and more researches are needed to discover these risk factors and their associations with HIE. In clinical practice, the examination of pregnant women during pregnancy and perinatal period should be strengthened to detect risk factors as early as possible to prevent the occurrence of HIE. In detail, firstly, strengthen the examination before pregnancy and during pregnancy, actively treat the high-risk factors affecting fetal development such as gestational hypertension, diabetes, anemia, and try to remove the adverse effects on the fetus caused by prenatal and during pregnancy. Secondly, strengthen fetal monitoring during pregnancy, timely evaluate the child’s intrauterine condition, and understand the growth and development of the fetus, such as the condition of amniotic fluid. Fetal distress in utero should be corrected, and termination of pregnancy should be considered if necessary. Thirdly, in the process of delivery, to prevent delayed labor caused by fetal or neonatal cerebral hypoxia, using appropriate delivery methods to shorten or end the process of labor, when necessary, appropriate relaxation of cesarean section indication, as soon as possible to end the delivery. In addition, medical institutions should standardize the resuscitation operation of neonatal asphyxia, fully prepare for the rescue of children with HIE, so that newborns with asphyxia after birth can be effectively treated at the first time.
Conclusions
In conclusion, the goal of analyzing the risk of neonatal HIE is to avoid HIE as much as possible. Based on the findings of this study, clinicians should take care to assess the risk of HIE based on fetal weight, amniotic fluid status, Apgar score at birth, and of course other reported risk factors. It is hoped that these findings will provide valuable information to obstetricians and neonatologists.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval
The study was performed under the guidance of the Declaration of Helsinki and approved by the Ethics Committee of Medicine, Meizhou People’s Hospital, Meizhou Academy of Medical Sciences. The parents or legal guardians of all neonates signed informed consent forms.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
Acknowledgments
The author would like to thank other colleagues whom were not listed in the authorship of Department of Neonatology, and Department of Pediatrics, Meizhou People’s Hospital, Meizhou Academy of Medical Sciences for their helpful comments on the manuscript.
Additional information
Funding
References
- Bonifacio SL, Hutson S. The term newborn: evaluation for hypoxic-ischemic encephalopathy. Clin Perinatol. 2021;48(3):681–695. doi:10.1016/j.clp.2021.05.014
- Greco P, Nencini G, Piva I, et al. Pathophysiology of hypoxic-ischemic encephalopathy: a review of the past and a view on the future. Acta Neurol Belg. 2020;120(2):277–288. doi:10.1007/s13760-020-01308-3
- Victor S, Rocha-Ferreira E, Rahim A, Hagberg H, Edwards D. New possibilities for neuroprotection in neonatal hypoxic-ischemic encephalopathy. Eur J Pediatr. 2022;181(3):875–887. doi:10.1007/s00431-021-04320-8
- Wang Z, Zhang P, Zhou W, et al. Neonatal hypoxic-ischemic encephalopathy diagnosis and treatment: a National Survey in China. BMC Pediatr. 2021;21(1):261. doi:10.1186/s12887-021-02737-6
- Thompson CM, Puterman AS, Linley LL, et al. The value of a scoring system for hypoxic ischaemic encephalopathy in predicting neurodevelopmental outcome. Acta Paediatr. 1997;86(7):757–761. doi:10.1111/j.1651-2227.1997.tb08581.x
- Sarnat HB, Sarnat MS. Neonatal encephalopathy following fetal distress. A clinical and electroencephalographic study. Arch Neurol. 1976;33(10):696–705. doi:10.1001/archneur.1976.00500100030012
- Ayrapetyan M, Talekar K, Schwabenbauer K, et al. Apgar scores at 10 minutes and outcomes in term and late preterm neonates with hypoxic-ischemic encephalopathy in the cooling era. Am J Perinatol. 2019;36(5):545–554. doi:10.1055/s-0038-1670637
- Michniewicz B, Al Saad SR, Karbowski LM, Gadzinowski J, Szymankiewicz M, Szpecht D. Organ complications of infants with hypoxic ischemic encephalopathy before therapeutic hypothermia. Ther Hypothermia Temp Manag. 2021;11(1):58–63. doi:10.1089/ther.2020.0035
- Pouppirt NR, Martin V, Pagnotto-Hammitt L, Spittle AJ, Flibotte J, DeMauro SB. The general movements assessment in neonates with hypoxic ischemic encephalopathy. J Child Neurol. 2021;36(8):601–609. doi:10.1177/0883073820981515
- Torres AR, Naranjo JD, Salvador C, Mora M, Papazian O. Predominant factors of neonatal encephalopathy: hypoxic and ischemia, a global problem. Medicina. 2019;79(Suppl 3):15–19.
- Rossi AC, Prefumo F. Antepartum and intrapartum risk factors for neonatal hypoxic-ischemic encephalopathy: a systematic review with meta-analysis. Curr Opin Obstet Gynecol. 2019;31(6):410–417. doi:10.1097/GCO.0000000000000581
- Fox A, Doyle E, Geary M, Hayes B. Placental pathology and neonatal encephalopathy. Int J Gynaecol Obstet. 2023;160(1):22–27. doi:10.1002/ijgo.14301
- Peebles PJ, Duello TM, Eickhoff JC, McAdams RM. Antenatal and intrapartum risk factors for neonatal hypoxic ischemic encephalopathy. J Perinatol. 2020;40(1):63–69. doi:10.1038/s41372-019-0531-6
- Wang J, Tao E, Mo M, et al. Perinatal risk factors influencing neonatal hypoxic ischemic encephalopathy in Southern China: a case-control study. Am J Perinatol. 2021;38(S 01):e182–e186. doi:10.1055/s-0040-1708884
- Group of Neonatology; Chinese Pediatric Society; Chinese Medical Association. Diagnostic criteria for neonatal hypoxic-ischemic encephalopathy. Chin J Pediatr. 2005;43(8):584.
- Wang X. Guideline of evidence-based treatment for hypoxic-ischemic encephalopathy in full-term infants(standard version, 2011). Chin J Evidence-Based Pediatr. 2011;1:548.
- Pálsdóttir K, Thórkelsson T, Hardardóttir H, Dagbjartsson A. Birth asphyxia, neonatal risk factors for hypoxic ischemic encephalopathy. Laeknabladid. 2007;93(10):669–673.
- Ali A, Yalçın R, Ünlüer-Gümüştaş A. Cranial MR characteristics of Cerebral Palsy cases and correlation of findings with clinical results. Turk J Pediatr. 2019;61(4):525–537. doi:10.24953/turkjped.2019.04.009
- Wang Y, Luo S, Wang K, Hou Y, Yan H, Zhang Y. Maternal and neonatal exposure to risk factors for neonates with moderate or severe hypoxic ischemic encephalopathy: a cross-sectional study. Ital J Pediatr. 2022;48(1):188. doi:10.1186/s13052-022-01380-w
- Liljestrom L, Wikstrom AK, Agren J, Jonsson M. Antepartum risk factors for moderate to severe neonatal hypoxic ischemic encephalopathy: a Swedish national cohort study. Acta Obstet Gynecol Scand. 2018;97(5):615–623. doi:10.1111/aogs.13316
- Mooney C, O’Boyle D, Finder M, et al. Predictive modelling of hypoxic ischaemic encephalopathy risk following perinatal asphyxia. Heliyon. 2021;7(7):e07411. doi:10.1016/j.heliyon.2021.e07411
- Torbenson VE, Tolcher MC, Nesbitt KM, et al. Intrapartum factors associated with neonatal hypoxic ischemic encephalopathy: a case-controlled study. BMC Pregnancy Childbirth. 2017;17(1):415. doi:10.1186/s12884-017-1610-3
- Nadeem G, Rehman A, Bashir H. Risk Factors Associated With Birth Asphyxia in Term Newborns at a Tertiary Care Hospital of Multan, Pakistan. Cureus. 2021;13(10):e18759. doi:10.7759/cureus.18759
- Khorram B, Kilmartin KC, Dahan M, et al. Outcomes of Neonates with a 10-min Apgar Score of Zero: a Systematic Review and Meta-Analysis. Neonatology. 2022;119(6):669–685. doi:10.1159/000525926
- Michel A. Review of the Reliability and Validity of the Apgar Score. Adv Neonatal Care. 2022;22(1):28–34. doi:10.1097/ANC.0000000000000859
- Hayes BC, McGarvey C, Mulvany S, et al. A case-control study of hypoxic-ischemic encephalopathy in newborn infants at >36 weeks gestation. Am J Obstet Gynecol. 2013;209(1):29.e21–29.e19. doi:10.1016/j.ajog.2013.03.023
- Negro S, Benders M. Early Prediction of Hypoxic-Ischemic Brain Injury by a New Panel of Biomarkers in a Population of Term Newborns. Oxid Med Cell Longev. 2018;2018:7608108. doi:10.1155/2018/7608108
- Murden S, Borbélyová V, Laštůvka Z, Mysliveček J, Otáhal J, Riljak V. Gender differences involved in the pathophysiology of the perinatal hypoxic-ischemic damage. Physiol Res. 2019;68(Suppl 3):S207–s217. doi:10.33549/physiolres.934356
- Lundgren C, Brudin L, Wanby AS, Blomberg M. Ante- and intrapartum risk factors for neonatal hypoxic ischemic encephalopathy. J Matern Fetal Neonatal Med. 2018;31(12):1595–1601. doi:10.1080/14767058.2017.1321628
- Martinez-Biarge M, Diez-Sebastian J, Wusthoff CJ, Mercuri E, Cowan FM. Antepartum and intrapartum factors preceding neonatal hypoxic-ischemic encephalopathy. Pediatrics. 2013;132(4):e952–959. doi:10.1542/peds.2013-0511
- Yang W, Wang L. Maternal hypertensive disorders in pregnancy and risk of hypoxic-ischemia encephalopathy. J Matern Fetal Neonatal Med. 2021;34(11):1754–1762. doi:10.1080/14767058.2019.1647529
- Parker SJ, Kuzniewicz M, Niki H, Wu YW. Antenatal and intrapartum risk factors for hypoxic-ischemic encephalopathy in a US birth cohort. J Pediatr. 2018;203:163–169. doi:10.1016/j.jpeds.2018.08.028
- Chen HM, Gao LX, Wang JJ, Gao C. The correlation between AGT gene polymorphism and neonatal hypoxic-ischemic encephalopathy (HIE). Eur Rev Med Pharmacol Sci. 2019;23(5):2194–2199. doi:10.26355/eurrev_201903_17266
- Xue LL, Wang F, Xiong LL, et al. A single-nucleotide polymorphism induced alternative splicing in Tacr3 involves in hypoxic-ischemic brain damage. Brain Res Bull. 2020;154:106–115. doi:10.1016/j.brainresbull.2019.11.001
- Esih K, Goričar K, Rener-Primec Z, Dolžan V, Soltirovska-šalamon A. CARD8 and IL1B polymorphisms influence mri brain patterns in newborns with hypoxic-ischemic encephalopathy treated with hypothermia. Antioxidants. 2021;10(1):96. doi:10.3390/antiox10010096
- Esih K, Goričar K. Genetic polymorphisms, gene-gene interactions and neurologic sequelae at two years follow-up in newborns with hypoxic-ischemic encephalopathy treated with hypothermia. Antioxidants. 2021;10(9):1495. doi:10.3390/antiox10091495
- Kuzmanić Šamija R, Primorac D, Rešić B, et al. Association of NOS3 gene variants and clinical contributors of hypoxic-ischemic encephalopathy. Braz J Med Biol Res. 2014;47(10):869–875. doi:10.1590/1414-431x20143938
- Wu Y, Zhu Z. The association between NOS3 gene polymorphisms and hypoxic-ischemic encephalopathy susceptibility and symptoms in Chinese Han population. Biomed Res Int. 2016;2016:1957374. doi:10.1155/2016/1957374
- Sun L, Xia L, Wang M, et al. Variants of the OLIG2 gene are associated with cerebral palsy in Chinese Han infants with hypoxic-ischemic encephalopathy. Neuromolecular Med. 2019;21(1):75–84. doi:10.1007/s12017-018-8510-1
- Kukec E, Goričar K, Dolžan V, Rener-Primec Z. HIF1A polymorphisms do not modify the risk of epilepsy nor cerebral palsy after neonatal hypoxic-ischemic encephalopathy. Brain Res. 2021;1757:147281. doi:10.1016/j.brainres.2021.147281
- Li B, Dasgupta C, Huang L, Meng X, Zhang L. MiRNA-210 induces microglial activation and regulates microglia-mediated neuroinflammation in neonatal hypoxic-ischemic encephalopathy. Cell Mol Immunol. 2020;17(9):976–991. doi:10.1038/s41423-019-0257-6
- Wang W, Jia L. Regulatory mechanism of MicroRNA-30b on neonatal hypoxic-ischemic encephalopathy (HIE). J Stroke Cerebrovasc Dis. 2021;30(3):105553. doi:10.1016/j.jstrokecerebrovasdis.2020.105553
- Chen R, Wang M, Fu S, Cao F, Duan P, Lu J. MicroRNA-204 may participate in the pathogenesis of hypoxic-ischemic encephalopathy through targeting KLLN. Exp Ther Med. 2019;18(5):3299–3306. doi:10.3892/etm.2019.7936
- Chen Z, Hu Y, Lu R, Ge M, Zhang L. MicroRNA-374a-5p inhibits neuroinflammation in neonatal hypoxic-ischemic encephalopathy via regulating NLRP3 inflammasome targeted Smad6. Life Sci. 2020;252:117664. doi:10.1016/j.lfs.2020.117664
- Fei S, Cao L, Li S. microRNA-139-5p alleviates neurological deficit in hypoxic-ischemic brain damage via HDAC4 depletion and BCL-2 activation. Brain Res Bull. 2021;169:73–80. doi:10.1016/j.brainresbull.2020.12.020
- Jia Y, Liu J, Hu H, Duan Q, Chen J, Li L. MiR-363-3p attenuates neonatal hypoxic-ischemia encephalopathy by targeting DUSP5. Neurosci Res. 2021;171:103–113. doi:10.1016/j.neures.2021.03.003