
Abstract
Purpose
To compare the diagnostic performance and unnecessary ultrasound-guided fine-needle aspiration (US-FNA) biopsy rate of the 2015 American Thyroid Association (ATA), 2016 Korean Society of Thyroid Radiology (KSThR), and 2017 American College of Radiology (ACR) guidelines for patients with and without Hashimoto’s thyroiditis (HT).
Patients and Methods
This retrospective study included 716 nodules from 696 consecutive patients, which were classified using the categories defined by the three guidelines: ATA, KSThR, and ACR. The malignancy risk in each category was calculated and the diagnostic performance and unnecessary fine-needle aspiration (FNA) rates of the three guidelines were compared.
Results
In total, 426 malignant and 290 benign nodules were identified. Patients with malignant nodules had lower total thyroxine levels and higher thyroid-stimulating hormone, thyroid peroxidase antibody, and thyroglobulin antibody levels than those without malignant nodules (all P<0.01). The margin difference was significant in non-HT patients (P<0.01), but comparable in HT patients (P=0.55). The calculated malignancy risks of high and intermediate suspicion nodules in the ATA and KSThR guidelines and moderately suspicious nodules in the ACR guidelines were significantly lower in non-HT patients compared with HT patients (P<0.05). The ACR guidelines showed the lowest sensitivity, highest specificity, and lowest unnecessary FNA rates in patients with and without HT. Compared to non-HT patients, HT patients had significantly lower unnecessary FNA rates (P<0.01).
Conclusion
HT was associated with a higher malignancy rate of thyroid nodules with intermediate suspicion according to the ATA, KSThR, and ACR guidelines. The three guidelines, especially ACR, were likely to be more effective and could allow a greater reduction in the percentage of benign nodules biopsied in patients with HT.
Introduction
The prevalence of thyroid cancers is increasing all over the world, especially papillary thyroid cancer (PTC).Citation1 Accurate diagnosis of PTC is essential to avoid misdiagnosis and unnecessary thyroidectomy. Ultrasound-guided fine-needle aspiration (US-FNA) serves as a useful tool for accurate PTC diagnosis, and there are different ultrasound (US)-based malignant risk stratification systems to help make decisions about the use of fine-needle aspiration (FNA). Of the various systems, the following guidelines are newly published and widely used in practice: the 2015 American Thyroid Association (ATA) management guidelines,Citation2 the 2016 Korean Society of Thyroid Radiology (KSThR) guidelines,Citation3 and the 2017 American College of Radiology (ACR) guidelines.Citation4 Each guideline stratifies thyroid nodules into different categories according to their own malignancy risks, and FNA biopsies are recommended because of the nodule category and largest diameter. However, these guidelines recommend different US features and size cut-off for FNA, and a deep understanding of the US-FNA criteria is required to optimize patient management.
Hashimoto’s thyroiditis (HT) is the most common autoimmune endocrine disease and is characterized by extensive lymphocytic infiltration of the thyroid gland. Thyroid nodules are common in HT patients.Citation5 The association between PTC and HT has been a topic of discussion,Citation6–12 and some researchers have suggested that HT is more positively associated with PTC.Citation6,Citation7,Citation12 However, the association between HT and PTC is poorly understood. The sonographic characteristics of HT are complex and show different changes in the course of the disease,Citation13,Citation14 especially when coexisting with nodules. Echogenic septations, inhomogeneous parenchyma, and diffuse hypoechogenicity and pseudonodules, are the characteristics of HT under US imaging, which may influence the identification of nodulesCitation14,Citation15 and make it difficult to differentiate between cancers and benign lesions.Citation16 These difficulties are commonly aggravated by small nodules. Therefore, to precisely identify thyroid cancer with HT, a better understanding of US images of thyroid nodules in HT patients is required. Several studies have been conducted to compare the diagnostic performance of two or more guidelines in predicting the likelihood of malignancy of each category and the need for FNA. The results have been inconsistent, with most studies focusing on the nodules with a normal thyroid background.Citation17–22 However, it remains unclear whether HT background influences the diagnostic performance of these sonographic classification guidelines.
Therefore, the study aimed to retrospectively compare the diagnostic efficiency and effectiveness at reducing the number of FNA biopsies of the ATA, ACR, and KSThR guidelines in patients with and without HT.
Materials and Methods
Study Participants
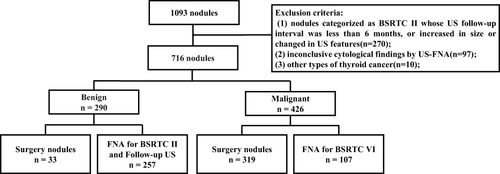
This retrospective study was conducted on 1064 consecutive patients who underwent US-FNA from January 2018 to March 2020 in Hangzhou First People’s Hospital, Hangzhou, China. The final diagnoses of the nodules were determined by the cytopathological results of the Bethesda System for Reporting Thyroid Cytology (BSRTC)Citation23 or surgical findings. Nodules with the following criteria were included: (1) definitive diagnostic cytological finding of benignity (BSRTC II) or malignancy (BSRTC VI) on US-FNA, (2) definitive cytological findings of benignity or malignancy by repeated US-FNA or surgery, (3) complete US images, and (4) with results of serum thyroid peroxidase antibody (TPOAb) and thyroglobulin antibody (TgAb) or postoperative pathological diagnosis of HT. The nodules were excluded as follows: (1) nodules categorized as BSRTC II whose US follow-up interval was < 6 months, or increased in size or changed in US features; (2) inconclusive cytological findings by US-FNA; and (3) other types of thyroid cancer. Finally, 716 nodules from 696 participants were included in the present study (). The protocol was followed in accordance with Declaration of Helsinki and approved by the local ethical committee of Hangzhou First People’s Hospital. Written informed consent was obtained from all the patients.
Figure 1 Flowchart of the study.
Laboratory Assays
Participants blood samples were collected early in the morning after an 8–10 h fasting window. Plasma total triiodothyronine (TT3), total thyroxine (TT4), free triiodothyronine (FT3), free thyroxine (FT4), thyroid-stimulating hormone (TSH), TPOAb, and TgAb levels were measured using chemiluminescence methods with an ADVIA Centaur XP Immunoassay System (Siemens, Munich, Germany).
The Diagnostic Criteria for HT
HT diagnosis was based on high serum levels of thyroid antibodies (TPOAb and TgAb) in combination with the cytological and/or histological pathology of patients or abnormalities in thyroid US features including reduced echo or diffused heterogeneity echo of the thyroid.Citation24
US Examination and Image Analysis
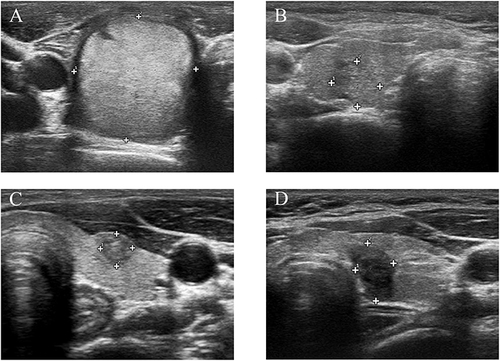
All US examinations were performed using various commercially real-time US systems. The US features of the nodules, including composition, echogenicity, shape, margin, and echogenic foci, were recorded by experienced radiologists using one set of standards according to the published literature.Citation25 The composition was classified as cystic or almost completely cystic, spongiform, mixed solid and cystic, and solid or almost completely solid. Echogenicity was classified as anechoic, hyper- to isoechoic, hypoechoic, or markedly hypoechoic. Shape was classified as wider than tall or taller than wide. Margin was classified as smooth or ill-defined, and lobulated or irregular. Echogenic foci were classified as none or large comet-tail artifacts, macro-calcifications, peripheral calcifications, or punctate echogenic foci. shows the US images of the four thyroid nodules with or without HT. One radiologist (20 years of experience with thyroid US) who was blinded to the clinical information and pathology results independently categorized the degree of suspicion of thyroid nodules according to the Thyroid Imaging Reporting and Data System (TIRADS) (proposed by the ACR or KSThR guidelines) and ATA guidelines. The ATA guidelines categorize thyroid nodules into the following categories: benign, very low suspicion, low suspicion, intermediate suspicion, and high suspicion based on different US patterns, which combine several individual sonographic characteristics.Citation2 According to the ACR TIRADS,Citation4 all the US features in a nodule were scored, with additional points awarded for more suspicious features. The sum of scores determines the TIRADS level of nodules, which ranges from benign, not suspicious, mildly suspicious, moderately suspicious, and highly suspicious nodules. For the KSThR TIRADS, thyroid nodules were categorized as benign, low suspicion, intermediate suspicion, and high suspicion nodules based on their malignancy risks stratified by the US patterns, which consisted of integrated solidity, echogenicity, and suspicious US features (irregular margins, taller than wide shape, and microcalcification).Citation3
Figure 2 The ultrasound images of four thyroid nodules with or without HT. (A) Benign nodule without HT, solid, hyperechoic, wider than tall shape, smooth margin, no echogenic foci; (B) Benign nodule with HT, almost completely solid, isoechoic, wider than tall shape, smooth margin, no echogenic foci; (C) Malignant nodule without HT, solid, hypoechoic, taller than wide shape, smooth margin, macro-calcifications; (D) Malignant nodule with HT, solid, hypoechoic, taller than wide shape, irregular margin, no echogenic foci.
US-FNA Performance
The US-FNA was performed by several experienced radiologists (5–10 years of experience with US-FNA). Perpendicular puncture using a 21-/23-gauge needle without local anesthesia was performed under US guidance. US imaging was performed using a MyLab™70 XVG 6–10 MHz linear probe (Esaote Group, Barcelona, Spain). During US visualization, the needle tip was placed in the target nodule, and then tissue samples were collected using the “mixed sampling technique”,Citation26,Citation27 during which the operator moved the needle up and down rapidly for 5 to 10 seconds, and the same procedure was repeated approximately two to three times. The specimens were smeared on the glass slides and then fixed with 95% alcohol. Three to four slides were obtained from each nodule and were sent for cytopathological diagnosis. All cytological smears were evaluated by two expert cytopathologists according to the BSRTC.
Statistical Analyses
Data are expressed as mean ± standard deviation for normal distribution, or as median (interquartile range, 25–75%) for skewed variables. For variables that were not normally distributed, we performed logarithmic transformation. Qualitative data are expressed as frequencies. Statistical analyses were performed using SPSS version 23.0 (SPSS, Chicago, IL, USA) for Windows. Differences in continuous and ratio variables were compared using two-sample t-tests and the chi-squared or Fisher’s exact test, respectively. Linear-by-linear association for trends was performed by entering the frequencies of each category of different guidelines. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were measured. The sensitivity, specificity, and rate of unnecessary FNA biopsies were compared using the McNemar test. For all analyses, two-sided P values < 0.05 were considered statistically significant.
Results
Patients’ Baseline Characteristics
Of the 716 thyroid nodules, 426 were malignant, and 290 were benign (). The final diagnoses were determined via surgical resection in 319 malignant and 33 benign nodules, and the remaining 107 malignant and 257 benign nodules were diagnosed via US and FNA (). The mean age of patients was 46.56±12.73 years, and patients with benign nodules were significantly older than those with malignant nodules (49.9±12.40 vs 44.29±12.46, P <0.01, ). Both sexes were equally represented across the two groups. Compared with patients with benign nodules, patients with malignant nodules had lower TT4 levels and higher TSH, TgAb, and TPOAb levels (all P <0.05, ). No significant differences were observed among TT3, FT3, and FT4 levels.
Table 1 Clinical Characteristics of the Study Population
The participants were further divided according to the presence of HT. Similarly, non-HT patients with malignant nodules were significantly younger and had lower TT4 and higher TSH levels than those with benign nodules (45.41±12.57 vs 50.10±12.21, P <0.01; 84.53±18.97 vs 88.69±19.94, P <0.05; 1.96±1.26 vs 1.69±1.09, P <0.05 ()). TT3, FT3, FT4, TgAb and TPOAb levels were comparable between the groups. For HT patients, significant difference was only observed in age between patients with malignant nodules and benign nodules (42.44±12.11 years vs 49.2±13.15 years, P <0.01, ), whereas TT3, TT4, FT3, FT4, TSH, TgAb, and TPOAb levels were comparable between groups.
Ultrasound Features of Nodules in Different Groups
The mean size of malignant nodules was significantly smaller than that of benign nodules in patients with and without HT (P<0.001, Table S1). Malignant nodules had significantly higher rates of solid composition, hypo-echogenicity or markedly hypo-echogenicity, taller than wide shape, and punctate echogenic foci than benign nodules in patients with and without HT (all P<0.01, Table S1). There were no differences between the benign and malignant groups for the left, isthmus, or right site (P=0.11, HT patients; P=0.203, non-HT patients (Table S1)). Notably, non-HT patients who had malignant nodules had significantly higher rates of lobulated or irregular margins (P<0.001), whereas the rates were comparable in HT patients (P=0.55, Table S1).
Malignancy Risks of Different Categories in the ATA, ACR, and KSThR Guidelines
In HT patients, for the ATA, the malignancy rates of nodules categorized as very low suspicion to high suspicion were 0%, 7.7%, 57.4%, and 87.9% (), all of which were generally within the ranges of the suggested risk, except the “intermediate suspicion” category, which was higher than the suggested risk. Regarding the ACR, the malignancy rates of nodules categorized as not suspicious to highly suspicious were 0%, 7.7%, 61.1%, and 90.5% (). Similarly, the “moderately suspicious” category had a higher malignancy risk than the suggested category. Based on the KSThR, the percentages of malignancy from benign to high suspicion were 0%, 5.6%, 58.6%, and 88.8% (), and the calculated malignancy of all categories was almost within the ranges of the suggested ones. In non-HT patients, the calculated malignancy risks of intermediate suspicion nodules in ATA (35.3%) and the moderately suspicious nodules in the ACR guidelines (34%) were also higher than the recommended ones (10–20%, intermediate suspicion nodules in ATA; 5–20%, moderately suspicious nodules in ACR). Moreover, compared to HT patients, the calculated malignancy risks of high and intermediate suspicion nodules in the ATA and KSThR guidelines and the moderately suspicious nodules in the ACR guidelines were significantly lower in non-HT patients (P<0.05, ), which were closer to the recommended risks.
Table 2 The Malignancy Rates of Various Categories of the ATA, ACR and KSThR Guidelines
Comparison of the Diagnostic Performance of the ATA, ACR, and KSThR Guidelines
High suspicion was used as the malignant cutoff value to distinguish between benign and malignant nodules. Regarding the diagnostic performance among the three guidelines, the ACR guidelines showed the lowest sensitivity (P<0.01, ) and NPV, followed by the KSThR and ATA guidelines in HT patients. Specificity was higher in the ACR than in the ATA guidelines (P<0.05, ). The specificity between the ATA and KSThR guidelines (P=0.5, ) and the ACR and KSThR guidelines (P=0.219, ) did not reach statistical significance. Similarly, for non-HT patients, the ACR guidelines showed the lowest sensitivity and highest specificity among the three guidelines (P<0.01, ), followed by the KSThR and ATA guidelines. The specificity between the ATA and KSThR guidelines did not reach statistical significance (P=0.063, ).
Table 3 The Diagnostic Performance of the ATA, ACR and KSThR Guidelines in Detecting Malignant Thyroid Nodules
Comparison of Unnecessary Rates of FNA
Among the 716 thyroid nodules, 246 (34.4%), 167 (23.3%), and 257 (35.9%) were recommended according to the FNA criteria by the ATA, ACR and KSThR guidelines, which revealed 101 (41.1%), 78 (46.7%), and 102 (39.7%) malignant lesions, respectively. Of the 272 nodules larger than 1 cm, 72 and 200 belonged to patients with and without HT, respectively. The unnecessary biopsy rates for patients with HT were 37.5%, 18.1%, and 40.3% for the ATA, ACR, and KSThR guidelines, respectively (). For non-HT patients, the unnecessary biopsy rates were 59%, 38%, and 63% for the ATA, ACR, and KSThR guidelines, respectively (). The ACR guidelines were associated with the lowest unnecessary FNA rates in patients with and without HT (all P<0.01), whereas the difference in the unnecessary FNA rate between the ATA and KSThR guidelines was not significant. Compared to patients without HT, those with HT had significantly lower unnecessary FNA rates in the three guidelines (all P<0.01, ).
Table 4 Comparison of Unnecessary FNA Rates for the Diagnosis of Thyroid Cancer (≥1cm)
Discussion
In our study, the incidence rates of HT were 37.9% in patients diagnosed with PTC and 21.2% in patients without PTC. The higher prevalence of PTC in patients with HT was similar to those of some previous studies.Citation10,Citation28 The rate of lobulated or irregular margin was comparable between malignant and benign thyroid nodules in the HT background, which raised the difficulty of US in evaluating thyroid cancer in HT patients. The ATA guidelines had the highest sensitivity, and the ACR guidelines had the highest specificity in patients with and without HT. The ACR guidelines had the lowest unnecessary FNA rates, and HT patients had significantly lower unnecessary FNA rates than those without HT did.
A growing number of studies have reported the association between thyroid hormones and PTC,Citation29–33 but no clear conclusions have been drawn. Higher FT4 levels were reported to be positively associated with thyroid cancer risk.Citation30 Another study by Gul et alCitation32 found that lower FT3 and FT4 levels, within the normal range, increased the risk of thyroid cancer. Most of the aforementioned studies investigating the association between thyroid hormones and thyroid malignancy did not include TT3 and TT4, which also play an important role in evaluating thyroid function.Citation34,Citation35 Jonklaas et alCitation33 found an association between low TT3 levels and thyroid cancer. In our study, we observed an inverse association between TT4 and PTC in non-HT patients. Compared to TT3, TT4 originates from the thyroid gland and may better reflect thyroid function. A lower TT4 level may result in a remarkably higher TSH level, which was previously reported to be positively associated with PTC.Citation36 TSH plays a major role in regulating thyroid hormone levels. TSH receptors are widely distributed on the surface of differentiated thyroid cancer cells. These cells respond to TSH stimulation by increasing the expression of several thyroid specific proteins.Citation37 Serum TSH concentrations are positively correlated with the risk of thyroid cancer-related death and relapse.Citation38 The present study also found a positive association between TSH levels and PTC in non-HT patients. TgAb and TPOAb levels are independent risk factors for PTC at the cytological and histological levels.Citation36,Citation39 Spencer et alCitation40 reported that the incidence of positive TgAb and TPOAb was approximately two-fold higher in patients with differentiated thyroid cancer. Our results are consistent with those of previous studies. However, for HT patients, there was no difference in TT4, TSH, TgAb and TPOAb levels between malignant and benign nodules. This may be partly due to the lower TT4 levels and higher TgAb, TPOAb, and TSH levels in HT, and their effect on thyroid malignancy may not be evident. However, further studies are required to evaluate the association between thyroid-related hormones and PTC in HT patients.
We found no differences in nodule sites between the benign and malignant groups. This may be due to the same foregut endodermal cells from which they originated. Notably, we found that the rate of lobulated or irregular margins was comparable in HT patients between the benign and malignant groups, indicating that margins may not be an independent factor in differentiating thyroid nodules with HT. This result was consistent with those of previous studies demonstrating that lobulated or irregular margins of benign thyroid nodules were more frequently observed in the thyroid glands with HT.Citation41
We found that each category in the ATA and ACR guidelines were generally within the ranges of the suggested malignancy risks, except the “intermediate suspicion” category, whose malignancy risk was significantly higher than the suggested one. According to the KSThR guidelines, the calculated malignancy of all categories was within the ranges of the suggested risks. Similar results have been observed in a previous study.Citation17 Regarding the intermediate risk categories, the ATA and ACR were relatively close to one another (5–10% and 5–20%, respectively), but the range of the KSThR was wider (15–50%). Therefore, we hypothesized that the ATA and ACR guidelines partly underestimated the malignant risks of the intermediate category, especially in HT patients. Moreover, our results showed a higher malignancy rate of thyroid nodules in patients with HT than in patients without HT, especially for nodules with high and intermediate suspicion. The higher malignancy rate of HT may be attributed to the close association between PTC and HT. Therefore, thyroid nodules with malignant features in HT patients deserve more attention than they are currently receiving.
Our results on the different strengths of three guidelines in diagnosing thyroid nodules are consistent with those of recent studies.Citation17,Citation18 A retrospective study in patients with thyroidectomy reported that the ACR guidelines were less sensitive and had a higher specificity than the ATA guidelines.Citation17 Ha et alCitation18 demonstrated that the ATA guidelines had a higher diagnostic sensitivity and a lower specificity than the ACR guidelines. However, in other studies, the ACR guidelines showed a higher sensitivity, whereas specificity and PPV were higher in the ATA guidelines.Citation19,Citation20 The differences in these studies may be attributed to the differences in the study population and the size of the nodules. Recently, Xu et alCitation20 indicated that the ATA guidelines had a higher specificity than the ACR guidelines, especially in nodules larger than 2 cm. However, more than 50% of nodules in our study were smaller than 1 cm, which was analyzed by Wu et alCitation21 and they suggested that the ACR guidelines have a higher specificity and a larger PPV than the ATA guidelines in thyroid nodules smaller than 1 cm. In our study, the diagnostic performance of the three guidelines showed almost no difference between patients with and without HT. However, based on the ATA guidelines, nodules with hyperechoic and microcalcification were not classified, which would restrict their application.
Regarding the less aggressive natural history of thyroid cancer, we should also focus on minimizing the false-negative rates, and the unnecessary biopsy rates to reduce health-care burden, patient anxiety, and unnecessary interventions. Data from previous studies agree that the ACR guidelines recommend fewer nodules for biopsy than other guidelines.Citation19–22 In our study, we confirmed these results in patients with and without HT. One of the reasons may be the different cut-offs of each FNA guideline. They all agreed on the 10-mm cut-off for highly suspicious nodules; however, the cut-offs for intermediate and low suspicion were higher in the ACR guidelines. Notably, the unnecessary FNA rate of each guideline was significantly lower in HT patients than in non-HT patients, indicating that the three guidelines, especially the ACR, were more effective for HT patients.
This study has some limitations. First, this was a retrospective study, and all the data were based on recorded static images, which implies a risk of misclassification owing to the inadequate and non-standard image acquisition during the examination. Second, some of the nodules were diagnosed based on cytopathological data, which may have caused false-negative and false-positive results. Third, the number of HT patients was small, and a larger sample size is required in future analyses. Fourth, the malignancy rate was relatively high in our study, possibly because the institution was a tertiary referral center in which patients always had more serious diseases. This may have caused a selection bias, and the diagnostic performance of the three guidelines may have been affected by this bias.
Conclusion
In summary, all three guidelines performed well in predicting thyroid malignancy and enabled more optimized FNA in patients with and without HT, whereas the ACR guidelines showed a statistically lower unnecessary FNA rates especially in HT. The ATA guidelines had the highest sensitivity, and the ACR guidelines had the highest specificity in patients with and without HT. HT was associated with a higher malignancy rate of thyroid nodules with intermediate suspicion according to the ATA, KSThR and ACR guidelines. Thus, clinicians can have a better understanding of the benefits and risks of US-FNA criteria in different guidelines, especially for patients with HT.
Abbreviations
PTC, papillary thyroid cancer; US-FNA, ultrasound-guided fine-needle aspiration; US, ultrasound; FNA, fine-needle aspiration; TIRADS, Thyroid Imaging Reporting and Data System; ATA, American Thyroid Association; KSThR, Korean Society of Thyroid Radiology; ACR, American College of Radiology; HT, Hashimoto’s thyroiditis; BSRTC, Bethesda System for Reporting Thyroid Cytology; TPOAb, thyroid peroxidase antibody; TgAb, thyroglobulin antibody; TT3, total triiodothyronine; TT4, total thyroxine; FT3, free triiodothyronine; FT4, free thyroxine; TSH, thyroid-stimulating hormone; PPV, positive predictive value; NPV, negative predictive value.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
We would like to thank Editage for English language editing.
Additional information
Funding
References
- Singh ON, Iniguez-Ariza NM, Castro MR. Thyroid nodules: diagnostic evaluation based on thyroid cancer risk assessment. BMJ. 2020;368:l6670. doi:10.1136/bmj.l6670
- Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26(1):1–133. doi:10.1089/thy.2015.0020
- Shin JH, Baek JH, Chung J, et al. Ultrasonography diagnosis and imaging-based management of thyroid nodules: revised Korean Society of thyroid radiology consensus statement and recommendations. Korean J Radiol. 2016;17(3):370–395. doi:10.3348/kjr.2016.17.3.370
- Tessler FN, Middleton WD, Grant EG, et al. ACR Thyroid Imaging, Reporting and Data System (TI-RADS): white paper of the ACR TI-RADS committee. J Am Coll Radiol. 2017;14(5):587–595. doi:10.1016/j.jacr.2017.01.046
- Won JH, Lee JY, Hong HS, et al. Thyroid nodules and cancer in children and adolescents affected by Hashimoto’s thyroiditis. Br J Radiol. 2018;91(1087):20180014. doi:10.1259/bjr.20180014
- Vita R, Ieni A, Tuccari G, et al. The increasing prevalence of chronic lymphocytic thyroiditis in papillary microcarcinoma. Rev Endocr Metab Disord. 2018;19(4):301–309. doi:10.1007/s11154-018-9474-z
- Lee JH, Kim Y, Choi JW, et al. The association between papillary thyroid carcinoma and histologically proven Hashimoto’s thyroiditis: a meta-analysis. Eur J Endocrinol. 2013;168(3):343–349. doi:10.1530/EJE-12-0903
- Liu Y, Lv H, Zhang S, et al. The impact of coexistent Hashimoto’s thyroiditis on central compartment lymph node metastasis in papillary thyroid carcinoma. Front Endocrinol. 2021;12:772071. doi:10.3389/fendo.2021.772071
- Baser H, Ozdemir D, Cuhaci N, et al. Hashimoto’s thyroiditis does not affect ultrasonographical, cytological, and histopathological features in patients with papillary thyroid carcinoma. Endocr Pathol. 2015;26(4):356–364. doi:10.1007/s12022-015-9401-8
- Osborne D, Choudhary R, Vyas A, et al. Hashimoto’s thyroiditis effects on papillary thyroid carcinoma outcomes: a systematic review. Cureus. 2022;14(8):e28054. doi:10.7759/cureus.28054
- Yu Z, Yu Y, Wan Y, et al. Iodine intake level and incidence of thyroid disease in adults in Shaanxi province: a cross-sectional study. Ann Transl Med. 2021;9(20):1567. doi:10.21037/atm-21-4928
- Cappellacci F, Canu GL, Lai ML, et al. Association between Hashimoto thyroiditis and differentiated thyroid cancer: a single-center experience. Front Oncol. 2022;12:959595. doi:10.3389/fonc.2022.959595
- Guan H, de Morais NS, Stuart J, et al. Discordance of serological and sonographic markers for Hashimoto’s thyroiditis with gold standard histopathology. Eur J Endocrinol. 2019;181(5):539–544. doi:10.1530/EJE-19-0424
- Wu G, Zou D, Cai H, et al. Ultrasonography in the diagnosis of Hashimoto’s thyroiditis. Front Biosci. 2016;21:1006–1012. doi:10.2741/4437
- Ralli M, Angeletti D, Fiore M, et al. Hashimoto’s thyroiditis: an update on pathogenic mechanisms, diagnostic protocols, therapeutic strategies, and potential malignant transformation. Autoimmun Rev. 2020;19(10):102649. doi:10.1016/j.autrev.2020.102649
- Slowinska-Klencka D, Klencki M, Wojtaszek-Nowicka M, et al. Validation of four thyroid ultrasound risk stratification systems in patients with Hashimoto’s thyroiditis; impact of changes in the threshold for nodule’s shape criterion. Cancers. 2021;13:19. doi:10.3390/cancers13194900
- Gao L, Xi X, Jiang Y, et al. Comparison among TIRADS (ACR TI-RADS and KWAK- TI-RADS) and 2015 ATA Guidelines in the diagnostic efficiency of thyroid nodules. Endocrine. 2019;64(1):90–96. doi:10.1007/s12020-019-01843-x
- Ha EJ, Na DG, Moon WJ, et al. Diagnostic performance of ultrasound-based risk-stratification systems for thyroid nodules: comparison of the 2015 American thyroid association guidelines with the 2016 Korean Thyroid Association/Korean Society of Thyroid Radiology and 2017 American College of Radiology Guidelines. Thyroid. 2018;28(11):1532–1537. doi:10.1089/thy.2018.0094
- Xu T, Wu Y, Wu RX, et al. Validation and comparison of three newly-released Thyroid Imaging Reporting and Data Systems for cancer risk determination. Endocrine. 2019;64(2):299–307. doi:10.1007/s12020-018-1817-8
- Xu T, Gu JY, Ye XH, et al. Thyroid nodule sizes influence the diagnostic performance of TIRADS and ultrasound patterns of 2015 ATA guidelines: a multicenter retrospective study. Sci Rep. 2017;7:43183. doi:10.1038/srep43183
- Wu XL, Du JR, Wang H, et al. Comparison and preliminary discussion of the reasons for the differences in diagnostic performance and unnecessary FNA biopsies between the ACR TIRADS and 2015 ATA guidelines. Endocrine. 2019;65(1):121–131. doi:10.1007/s12020-019-01886-0
- Middleton WD, Teefey SA, Reading CC, et al. Comparison of performance characteristics of American College of Radiology TI-RADS, Korean Society of Thyroid Radiology TIRADS, and American Thyroid Association Guidelines. AJR Am J Roentgenol. 2018;210(5):1148–1154. doi:10.2214/AJR.17.18822
- Cibas ES, Ali SZ. The 2017 Bethesda system for reporting thyroid cytopathology. Thyroid. 2017;27(11):1341–1346. doi:10.1089/thy.2017.0500
- Grani G, Carbotta G, Nesca A, et al. A comprehensive score to diagnose Hashimoto’s thyroiditis: a proposal. Endocrine. 2015;49(2):361–365. doi:10.1007/s12020-014-0441-5
- Frates MC, Benson CB, Charboneau JW, et al. Management of thyroid nodules detected at US: society of Radiologists in Ultrasound consensus conference statement. Radiology. 2005;237(3):794–800. doi:10.1148/radiol.2373050220
- Kim DW, Choo HJ, Park JS, et al. Ultrasonography-guided fine-needle aspiration cytology for thyroid nodules: an emphasis on one-sampling and biopsy techniques. Diagn Cytopathol. 2012;40(Suppl 1):E48–E54. doi:10.1002/dc.21669
- Gao Y, Qu N, Zhang L, et al. Preoperative ultrasonography and serum thyroid-stimulating hormone on predicting central lymph node metastasis in thyroid nodules as or suspicious for papillary thyroid microcarcinoma. Tumour Biol. 2016;37(6):7453–7459. doi:10.1007/s13277-015-4535-3
- Wang D, Du LY, Sun JW, et al. Evaluation of thyroid nodules with coexistent Hashimoto’s thyroiditis according to various ultrasound-based risk stratification systems: a retrospective research. Eur J Radiol. 2020;131:109059. doi:10.1016/j.ejrad.2020.109059
- Wang Z, Lin Y, Jiang Y, et al. The associations between thyroid-related hormones and the risk of thyroid cancer: an overall and dose-response meta-analysis. Front Endocrinol. 2022;13:992566. doi:10.3389/fendo.2022.992566
- Liang L, Zheng XC, Hu MJ, et al. Association of benign thyroid diseases with thyroid cancer risk: a meta-analysis of prospective observational studies. J Endocrinol Invest. 2019;42(6):673–685. doi:10.1007/s40618-018-0968-z
- Huang H, Rusiecki J, Zhao N, et al. Thyroid-stimulating hormone, thyroid hormones, and risk of papillary thyroid cancer: a nested case-control study. Cancer Epidemiol Biomarkers Prev. 2017;26(8):1209–1218. doi:10.1158/1055-9965
- Gul K, Ozdemir D, Dirikoc A, et al. Are endogenously lower serum thyroid hormones new predictors for thyroid malignancy in addition to higher serum thyrotropin? Endocrine. 2010;37(2):253–260. doi:10.1007/s12020-010-9316-6
- Jonklaas J, Nsouli-Maktabi H, Soldin SJ. Endogenous thyrotropin and triiodothyronine concentrations in individuals with thyroid cancer. Thyroid. 2008;18(9):943–952. doi:10.1089/thy.2008.0061
- Wang X, Jiang F, Chen W, et al. The association between circulating trans fatty acids and thyroid function measures in U.S. adults. Front Endocrinol. 2022;13:928730. doi:10.3389/fendo.2022.928730
- Külz M, Fellner S, Rocktäschel J, et al. Dubiously increased FT4 and FT3 levels in clinically euthyroid patients: clinical finding or analytical pitfall? Clin Chem Lab Med. 2022;60(6):877–885. doi:10.1515/cclm-2021-1211
- Fiore E, Vitti P. Serum TSH and risk of papillary thyroid cancer in nodular thyroid disease. J Clin Endocrinol Metab. 2012;97(4):1134–1145. doi:10.1210/jc.2011-2735
- Song YS, Kim MJ, Sun HJ, et al. Aberrant thyroid-stimulating hormone receptor signaling increases VEGF-A and CXCL8 secretion of thyroid cancer cells, contributing to angiogenesis and tumor growth. Clin Cancer Res. 2019;25(1):414–425. doi:10.1158/1078-0432.CCR-18-0663
- Hovens GC, Stokkel MP, Kievit J, et al. Associations of serum thyrotropin concentrations with recurrence and death in differentiated thyroid cancer. J Clin Endocrinol Metab. 2007;92(7):2610–2615. doi:10.1210/jc.2006-2566
- Wu X, Lun Y, Jiang H, et al. Coexistence of thyroglobulin antibodies and thyroid peroxidase antibodies correlates with elevated thyroid-stimulating hormone level and advanced tumor stage of papillary thyroid cancer. Endocrine. 2014;46(3):554–560. doi:10.1007/s12020-013-0121-x
- Spencer CA. Clinical review: clinical utility of thyroglobulin antibody (TgAb) measurements for patients with differentiated thyroid cancers (DTC). J Clin Endocrinol Metab. 2011;96(12):3615–3627. doi:10.1210/jc.2011-1740
- Park M, Park SH, Kim EK, et al. Heterogeneous echogenicity of the underlying thyroid parenchyma: how does this affect the analysis of a thyroid nodule? BMC Cancer. 2013;13:550. doi:10.1186/1471-2407-13-550