Abstract
Background
The double burden of communicable and noncommunicable diseases (NCD) is an increasing trend in low- and-middle income developing countries. Rural and minority populations are underserved and likely to be affected severely by these burdens. Knowledge among young people could provide immunity to such diseases within a community in the long term. In this study we aimed to assess the knowledge of several highly prevalent NCDs (diabetes, hypertension, and chronic obstructive pulmonary disease [COPD]) and several highly incident communicable diseases (malaria and diarrheal diseases) among Karen high school students in a rural district in far northwest of Thailand. The aim of the study is to explore information for devising life-course health education that will be strategically based in schools.
Method
A cross-sectional survey approved by the ethics committee of Boromarajonani College of Nursing Nakhon Lampang (BCNLP), Lampang, Thailand was conducted in Thasongyang, Tak province, from September 2011 to January 2012. Questionnaires for assessing knowledge regarding diabetes, hypertension, COPD, malaria, and diarrheal diseases were delivered to all 457 Karen high school students attending Thasongyang high school. A total of 371 students returned the questionnaires. Experts’ validation and split-half reliability assessment was applied to the instrument.
Results
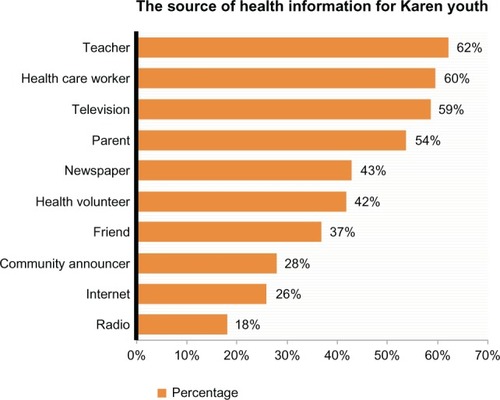
Students’ main sources of health information were their teachers (62%), health care workers (60%), television (59%), and parents (54%). Familial risk factors of diabetes and hypertension were not known to more than two thirds of the students. Except obesity and physical inactivity, lifestyle-related risk factors were also not known to the students. Though living in a malaria-endemic area, many of the Karen students had poor knowledge about preventive behaviors. Half of the students could not give a correct answer about the malaria and hygienic practice, which might normally be traditionally relayed messages.
Conclusion
Health education and knowledge about common NCD and communicable diseases are yet to be prompted among the Karen students. A broader and more comprehensive school-based health education strategy for prevention of double burden diseases would benefit the rural minority population at the Thai-Myanmar border.
Introduction
Ethnic minority groups are prone to health disparity and poor health education.Citation1 The Karen people are an ethnic minority group living along the Thailand and Myanmar border.Citation2 Recent studies in Thasongyang reported poor health education among the middle-aged and old-aged population regarding diabetes and hypertension.Citation3–Citation5
In low- and middle-income countries, the double burden of communicable diseases and noncommunicable diseases (NCDs) is trending upwards.Citation6 Epidemiological transition occurs in such a setting, with the increasing burden of lifestyle-related diseases such as diabetes and hypertension presenting, in addition to the existing burden of infectious diseases such as malaria and diarrheal diseases. Thailand is one such country.Citation7
Minority people are likely to be among those more severely affected because of language barriers, lack of power, and underrepresentation.Citation8–Citation10 Moreover, geographically remote and rural areas are likely to suffer from inequality in many aspects of health care need.Citation11 Situated at the northwestern-most edge of Thailand and populated by a Karen ethnic population, Thasongyang, a rural district and the site of our current study, is a good example of such an area facing inequality.
Diabetes, hypertension, and chronic obstructive pulmonary disease (COPD) are top-ranked causes of morbidity and mortality in Thailand, despite the waning incidence of malaria and diarrheal diseases in recent years, in most urban settings.Citation12–Citation15 In the study site area, diabetes and hypertension are highly prevalent; moreover, malaria is still a high burden disease, as was the case decades ago.Citation15,Citation16 Locally reported data show that the incidence of diarrheal diseases is also very high.Citation17 However, there is limited literature and few research studies on knowledge of such diseases among the Karen minority, particularly among the youth group.
Schools are where health education can be delivered to youth groups, together with educational packages;Citation18 Life-course health education can be launched in schools as part of the curriculum. Thus, it would be beneficial to assess the knowledge that an ethnic minority’s high school students have about nationally and locally high-burden diseases.
In this study, we aimed to assess the knowledge of highly prevalent noncommunicable diseases (NCDs) (diabetes, hypertension, and COPD), as well as highly incident communicable diseases (malaria and diarrheal diseases) among high school students of Karen ethnicity, in a rural district in the northwestern-most edge of Thailand.
Materials and methods
The study was conducted in the Thasongyang district, in Thailand’s Tak province. The district borders Myanmar via the narrow Moei River. The areas along the Thai-Myanmar border are usually populated with Karen ethnic residents, as well as migrants with different immigration statuses.Citation19
A cross-sectional study was conducted to survey the knowledge among Karen minority students who were attending high school in Thasongyang district. The study obtained the approval of the Boromarajonani College of Nursing, Nakhon Lampang (BCNLP)’s institutional review board, Thailand, and permission of the school. The study was conducted from September 2011 to January 2012.
The targeted population was approached directly because at the time of this study there was only one high school which provided high school education up to grade nine in Thasongyang, Since we wanted to assess the minority Karen high school students’ knowledge, we delivered the questionnaires to all 457 Karen students in grade 7 and 6 purposively. Five sets of paper-based knowledge assessment questionnaires underwent content validation by experts from BCNLP and split-half reliability assessment. Readability and comprehension of questions by the students were confirmed by schoolteachers in Thasongyang. Self-administered questionnaires were returned by the students.
Data was descriptively analyzed by applying STATA 11 (StataCorp LP, College Station, TX, USA). Reliability assessment used SPSS version 11.5 (IBM, Chicago, IL, USA). The reliability coefficients of each set of questions are shown under the knowledge assessment result table (–).
Table 2 Diabetes knowledge of Karen high school students
Table 6 Diarrhea knowledge among Karen high school students
Results
A total of 371 students filled and returned questionnaires. The response rate was 81%. Two-thirds of students were female. The average age was 17 years. Karen minority students attending four different levels of classes, from level one to level six, were included. Most of their family members’ occupations were farmers and day laborers. Half of the students’ family heads were uneducated. A complete characteristic of the sample is presented in .
Table 1 Characteristic of the study sample
Teachers, health care workers, and televisions were the top-ranked source of health information reported by the respondents. Internet use was limited to 26%, and only 18% listened to the radio (see ).
Figure 1 The source of health information for Karen youth.
Diabetes
Most of the students in the study sample were familiar with diabetes (93%). About two-thirds of students knew it as an NCD, but only 28.69% realized that it was incurable. The risk factors of diabetes that were well known to students were obesity (81.69%), childhood obesity (75.41%), and lack of exercise (71.58%). Almost two-thirds of students answered that those who ate too much fatty food and sweets could have diabetes. However, 77.13% of the sample did not know that a family history of diabetes is a risk factor for diabetes, and half answered that diabetes was a disease more likely to occur in the elderly. Moreover, half of the students in the study sample had knowledge about well-known symptoms of diabetes such as thirst and frequent urination, and diabetes complications such as slow wound healing (53%), kidney damage (46%), and numbness of the feet (36%). However, seven out of ten students did not have any knowledge of normal blood sugar levels.
Hypertension
Most of the respondents knew hypertension, and two-thirds correctly recognized hypertension as an NCD and as a disease which is not curable. However, only one third of them knew about normal and high blood pressure levels. The risk factors of hypertension that are well-known to them were old age (72.63%) and obesity (83.52%). Lifestyle-related risk factors which were not known by students included smoking, which was not known by 64.74% of students, eating a high salt diet (63.54%), stress and strain (40%), drinking alcohol (40%), consuming large amounts of coffee and tea (58.68%), and lack of regular exercise (31.13%). Moreover, two-thirds of the students did not notice family history of hypertension as a risk factor.
COPD
The term COPD was known to only 66.67% of students, but most of them did not realize that COPD was an NCD (56.42%). Only one of five students recognized COPD as an incurable disease. Most of students identified smoking as a risk for COPD (70.42%), but just half answered environmental pollution and inhalation of dust (50.56%) as a risk factor for COPD, and more than one-third (39.61%) thought chewing tobacco might cause COPD. Shortness of breath was recognized as a feature of COPD; reduced functional status was also known to be a consequence of COPD to more than 50% of the students.
Malaria
Almost all respondents knew about malaria. More than two-thirds of students identified malaria as a mosquito-borne disease. Regarding preventive behavior, more than half knew to sleep under an insecticide-impregnated net and that wearing long sleeved shirts and trousers while working in the forest could prevent malaria. Moreover, more than two-thirds identified fever, chills, and headache as symptoms of malaria. A large percentage of students knew it could lead to life threatening disease (74%), but only half of them knew that it could not be treated by over-the-counter drugs (55.2%).
More than half of students answered that general well-being was a protective factor (53.3%); half of them answered that chemical insecticides would be effective to control mosquitoes. However, some were mistaken in their knowledge, answering incorrectly that malaria is a bacterial disease (32%); one-third also thought that malaria was caused by drinking creek water. A third of students also answered that a malaria mosquito would bite only at night.
Despite being familiar with diarrheal disease and its symptoms, only 60% of students realized that diarrhea can be fatal. More than 85% of the students recognized unclean food and fly-landed food as a cause of diarrhea, as well as recognizing hand-washing before meals and after toilet use as preventive practices. However, half of the students chose the option on the questionnaire of washing hands without soap after using the toilet.
Regarding food hygiene, almost two-thirds of students knew to eat freshly cooked food, and to keep food well-covered to avoid mice, flies, and cockroaches. However, half of the students thought that adults could eat uncooked food, without worry of diarrhea.
Discussion
In this study, we assessed Karen high school students’ knowledge of common and burdensome diseases, focusing on a rural setting in Thailand. Health knowledge will prevent adolescent students from establishing unhealthy behavior and risky lifestyles;Citation20 thus, it will consequently contribute to preventing NCDs. Knowledge of malaria and diarrheal diseases will lead to preventive behavior and consequently reduce the transmission and burden of disease. Hence, the information explored by the current school-based survey may benefit the minority health by helping devise strategies and means of school-based health education.
Most of the respondents were from low-income and poorly educated families (). Most of them were informed by teachers, health care workers, television programs, and parents; traditionally held beliefs, common misbelief, and wrong beliefs may pass from parents to offspring. Based on , class-, family- and television-based health education may reach the targeted population.
NCD
The survey findings showed that diabetes was known to more than 80% of students (). The majority of students also noticed lifestyle-related risk factors such as obesity and physical inactivity;Citation21 some students even knew the complications of diabetes. However, the majority lacked any knowledge about blood glucose levels and did not know that genetic predisposition and family history are strong indicators of diabetes mellitus risk.Citation21,Citation22 A recent study in Thasongyang reported the risk of prediabetes among those with a family history of diabetes (adjusted odds ratio 4.6, 95% confidence interval 1.81–11.71) among the Karen adults.Citation5 Therefore, it is necessary to educate high school students; among those with a family history of diabetes, the knowledge could help lead to a choice of healthy lifestyle and prevention of diabetes by simply alerting students that they are at risk of diabetes.Citation22 Knowledgeable young adults may adopt healthy ways to eat, live, and avoid risky behaviors such as smoking, alcohol, and physical inactivity.
Likewise, the majority of students knew about hypertension. However, they did not know the exact limits of a healthy blood pressure. Many of them also did not know that family history can be an indication of hypertension risk (). Moreover, the lifestyle-related risk factors which were common to all cardiovascular diseases were not well known among the students. This situation necessitated health education lessons regarding hypertension and related cardiovascular diseases.
Table 3 Hypertension knowledge of Karen high school students
Adolescence is the period of life when children develop their behaviors and habits.Citation23 Health education delivered in the classroom would enable students to refuse tobacco, to refuse unhealthy diet choices such as salty food, and to adopt practicing regular physical exercise in the long run.
The number of deaths caused by COPD has increased globally, but it is still less well known to many people compared to other diseases;Citation24,Citation25 this was the case in our study, where COPD was less known to the Karen high school students than diabetes and hypertension. A recently reported smoking rate among Karen adults was as high as 70% among both male and female subjects, indicating a need for tobacco control intervention.Citation4 Meanwhile, students’ knowledge about smoking as a risk factor for COPD was certainly high (67%), even though they did not know that COPD was a NCD (). Nonsmoking risk factors such as outdoor air pollution were also known to less than half of the students.Citation26 A comprehensive and well introduced health education class regarding COPD is necessary for these adolescents. It might also lead to strong knowledge of the health risk caused by smoking and result in Karen youth groups avoiding tobacco use.
Table 4 Chronic obstructive pulmonary diseases knowledge among Karen high school students
Communicable diseases
Thasongyang has been one of the districts with the highest malaria incidence in Thailand.Citation16 Personal protection is one of the key elements in prevention of malaria, while vector control and human vector interface were less successfully controlled. The majority of the participants knew malaria and recognized it as a vector-borne disease caused by mosquito bites (). However, knowledge of personal protection was confined to not more than half of the sample. Moreover, many of them had wrong knowledge or held incorrect beliefs; for example, the belief that general wellbeing would prevent malaria, and that malaria was caused by drinking creek water. These could be traditional beliefs relayed by parents. Even though these students were residents of a malaria-endemic area, their knowledge on personal protective behavior was less than satisfactory. It is worth to educate these students with health informations.
Table 5 Malaria knowledge among Karen high school students
Diarrheal diseases were leading causes of illness in the areas along the Thai-Myanmar border.Citation17 Diarrhea is a hygiene-related disease and hand washing is a basic and critical personal behavior which can cut down on infections, prevent illness, and save lives.Citation27 Three quarters of the students in the study knew to wash their hands before every meal and after using the toilet. However, half of them thought washing hands without soap after using the toilet was acceptable ().
Hygienic practices are influenced not only by acquired knowledge but also by the sanitation facilities in the local community and civil structures such as the municipal water supply system. In this study setting, most of the houses had a periodically accessible tap water supply. The use of sanitation facilities in Thailand has improved in the last decade.Citation28 However, in rural areas, piped-into-premises coverage is only 31%.Citation28 Many rural areas still rely on community water resources, which might lead to inconvenience if washing one’s hands with soap frequently. However a recent observational study in Bangladesh reported that washing hands with water alone, before preparing food, could reduce the incidence of diarrhea, given that both hands were washed; on the other hand, washing with water only and without soap after defecation could not significantly prevent diarrhea.Citation29 Moreover, the responses relating to the food hygiene questions was poor. Some students thought adults could eat uncooked food; only six out of ten students answered that they needed to avoid uncooked food to prevent diarrhea. This response reveals the need for health education to improve the students’ knowledge of diarrhea prevention and hygienic practices.
Limitation
Because of access difficulties, we approached high school students directly and purposively sampled the Karen minority students. This approach might have an impact on the generalizability of this study, since there could be minority youths who did not have the opportunity to attend school. Likewise, difficult access did not allow us to run a test-retest reliability assessment of questionnaires. Nonetheless, the split-half assessment showed sound reliability indicators for the questionnaires.
Conclusion
Despite the limitations cited, this survey’s findings may provide a spotlight on the health knowledge of Karen youth along the rural Thai-Myanmar border area. We also identified the entry points for promoting students’ health education in the future. These might lead us to achieve our ultimate objective of finding ways to start life-course health education of ethnic minorities in rural communities.
Health inequalities and disparities in knowledge are common in minority populations.Citation11 The current study’s findings clearly disclosed the need for promoting health knowledge among high school students of Karen ethnicity. Based on these findings, we recommend broader and more comprehensive health education in high schools classes to prevent the double burden of NCD and communicable diseases in minority populations.
Author contributions
TL and MNA were lead authors. TL designed the study. All authors contributed to the research process, data management and drafting. TL and PN developed the questionnaires. PJ translated the questionnaires into English and MNA edited those. MNA designed and performed analysis. TL, MNA and all authors interpreted the results. All authors have seen and confirmed the final draft and discussions written by MNA.
Acknowledgments
The authors acknowledged Saiyud Moolphate, Department of Tropical Hygeine, Faculty of Tropical Medicine, Mahidol University, Bangkok, Thailand and Janthila Srikrajang, Department of Research and Community Engagement, BCNLP, Lampang, Thailand for their important suggestions for data analysis and data presentation.
Disclosure
The authors report no conflicts of interest in this work.
References
- Disease Burden and Risk Factors [webpage on the Internet]AtlantaCenters for Disease Control and Prevention2007 Available from: http://www.cdc.gov/omhd/amh/dbrf.htmAccessed February 18, 2013
- RajahARemaining Karen: a Study of Cultural Reproduction and the Maintenance of IdentityCanberraANU E Press2008 Available from: http://www.burmalibrary.org/docs6/Remaining_Karen.pdfAccessed February 18, 2013
- LorgaTSrithongKManokulananPAungTNNAungMNPublic knowledge of diabetes in Karen Ethnic rural residents: a community-based questionnaires study in the far north-west of ThailandInt J Gen Med2012579980423055769
- AungMNLorgaTSrikrajangJAssessing awareness and knowledge of hypertension in an at-risk population in the Karen ethnic rural community, Thasongyang, ThailandInt J Gen Med2012555356122807644
- LorgaTAungMNNaunboonruangPPredicting prediabetes in a rural community: a survey among the Karen ethnic community, Thasongyang, ThailandInt J Gen Med2012521922522399865
- BygbjergICDouble burden of noncommunicable and infectious diseases in developing countriesScience201233761011499150122997329
- KaufmanNDChasombatSTanomsinghSRajataramyaBPotempaKPublic health in Thailand: emerging focus on non-communicable diseasesInt J Health Plann Manage2011263e197e21221796679
- EgedeLEDagogo-JackSEpidemiology of type 2 diabetes: focus on ethnic minoritiesMed Clin North Am9200589594997516129107
- KurianAKCardarelliKMRacial and ethnic differences in cardiovascular disease risk factors: a systematic reviewEthn Dis200717114315217274224
- World Health Organizationglobal atlas on cardiovascular disease prevention and control2011http://www.who.int/cardiovascular_diseases/publications/atlas_cvd/en/index.htmlAccessed 04.04.2012
- ThammatachareeNTisayaticomKSuphanchaimatRPrevalence and profiles of unmet healthcare need in ThailandBMC Public Health201212192323110321
- KearneyPMWheltonMReynoldsKMuntnerPWheltonPKHeJGlobal burden of hypertension: analysis of worldwide dataLancet2005365945521722315652604
- TiptaradolSAekplakornWPrevalence, awareness, treatment and control of coexistence of diabetes and hypertension in Thai populationInt J Hypertens2012201238645322888406
- World Malaria Report 2012: Country profiles: Thailand 2012 [webpage on the internet]GenevaWorld Health Organization2010 Available from: http://www.who.int/malaria/publications/country-profiles/profile_tha_en.pdfAccessed February 19, 2013
- SriwattanapongseWPrasitwattanasereeSKhanabsakdiSMortality Rate due to Malaria in ThailandWalailak Journal of Science and Technology (WJST)201292135139http://wjst.wu.ac.th/index.php/wjst/article/view/296
- ThimasarnKJatapadmaSVijaykadgaSSirichaisinthopJWongsrichanalaiCEpidemiology of malaria in ThailandJ Travel MEd19952259659815363
- International Organization for MigrationThailand Migration Report 2011GenevaIOM: International Organization for Migration2013 Available from: http://publications.iom.int/bookstore/free/TMR_2011.pdfAccessed February 15, 2012
- World Health OrganizationSchool health and youth health pro motion 2013http://www.who.int/school_youth_health/en/Accessed June 6, 20132013
- 2013 UNHCR country operations profile – Thailand [webpage on the internet]GenevaUnited Nations High Commissioner for Refugees2012 Available from: http://www.unhcr.org/pages/49e489646.htmlAccessed February 15, 2012
- AbelsonPHGreat transitionsScience199527052388957481778
- AekplakornWBunnagPWoodwardMA risk score for predicting incident diabetes in the Thai populationDiabetes Care20062981872187716873795
- AlbertiKGZimmetPShawJInternational Diabetes Federation: a consensus on type 2 diabetes preventionDiabet Med200724545146317470191
- AldermanEMRiederJCohenMIThe history of adolescent medicinePediatr Res200354113714712672903
- COPD predicted to be third leading cause of death in 2030 [webpage on the internet]GenevaWorld Health Organiztion2008 Available from: http://www.who.int/respiratory/copd/World_Health_Statistics_2008/en/index.htmlAccessed February 18, 2013
- TanWCTrends in chronic obstructive pulmonary disease in the Asia-Pacific regionsCurr Opin Pulm Med2011172566121178626
- ManninoDMBuistASGlobal burden of COPD: risk factors, prevalence, and future trendsLancet2007370958976577317765526
- Centers for Disease Control and PreventionHandwashing: Clean hands save lives. [webpage on the internet]AtlantaCenters for Disease Control and Prevention2013 Available from: http://www.cdc.gov/handwashing/Accessed February 22, 2013
- WHO/UNICEF Joint Monitoring Programme (JMP) for Water Supply and Sanitation [webpage on the internet]GenevaWorld Health Organization2010 Available from: http://www.wssinfo.org/data-estimates/table/Accessed February 27, 2013
- LubySPHalderAKHudaTUnicombLJohnstonRBThe effect of handwashing at recommended times with water alone and with soap on child diarrhea in rural Bangladesh: an observational studyPLoS Med [Epub June 28, 2011]