Abstract
Aim
To determine the prevalence of erectile dysfunction (ED) in a sample of the Belgian men who have sex with men (MSM) population, and to assess the relevance of major predictors such as age, relationship, and education. We investigated the use of phosphodiesterase type 5 (PDE5) inhibitors among Belgian MSM.
Methods
An internet-based survey on sexual behavior and sexual dysfunctions, called GAy MEn Sex StudieS (GAMESSS), was administered to MSM, aged 18 years or older, between the months of April and December 2008. The questionnaire used was a compilation of the Kinsey’s Heterosexual–Homosexual Rating Scale, Erection Quality Scale (EQS), and the shortened version of the International Index of Erectile Function (IIEF-5).
Results
Of the 1752 participants, 45% indicated having some problems getting an erection. In this group of MSM, 71% reported mild ED; 22% mild to moderate ED; 6% moderate ED; and 2% severe ED. Independent predictors for the presence of ED were: age (odds ratio [OR] = 1.04, P < 0.0001), having a steady relationship (OR = 0.59, P < 0.0001), frequency of sex with their partner (OR = 1.22, P < 0.0001), versatile sex role (OR = 1.58, P = 0.016), passive sex role (OR = 3.12, P < 0.0001), problems with libido (OR = 1.15, P = 0.011), ejaculation problems (OR = 1.33, P < 0.0001), and anodyspareunia (OR = 0.87, P < 0.0001). Ten percent of the Belgian MSM used a PDE5 inhibitor (age 43 ± 11 years; mean ± standard deviation) and 83% of them were satisfied with the effects. “Street drugs” were used by 43% of MSM to improve ED.
Conclusion
Forty-five percent of participating Belgian MSM reported some degree of ED and 10% used a PDE5 inhibitor to improve erections. Older MSM reported more ED. MSM, who were in a steady relationship or frequently had sex with a partner, reported less ED. MSM with ejaculation problems indicated having more ED.
Introduction
Erectile dysfunction (ED) is defined as the persistent inability to obtain and maintain an erection sufficient to permit a satisfactory sexual performance.Citation1 ED is considered one of the most commonly occurring male sexual disorders and one of the most frequent chronic health conditions in men older than 40 years of age.Citation2 In 1995 it was estimated that over 152 million men worldwide experienced ED.Citation3 In projections for 2025 the prevalence will increase by nearly 170 million men to 322 million worldwide, with the largest increases in Africa, Asia, and South America.Citation3,Citation4
Epidemiological research on ED is rapidly growing and several studies showed large variations in the prevalence of ED.Citation5,Citation6 In 1994 in the Massachusetts Male Aging Study (MMAS), with a study group of 1709 men aged between 40–70 years, the prevalence of ED was 52% (10% severe, 25% moderate, and 17% mild).Citation7 A Belgian survey by Mak et al using a smaller study group of 799 men aged 40–70 years, also showed a high prevalence of ED of 62% (10% severe, 25% moderate, and 27% mild).Citation8 Other studies reported lower prevalence of ED. The Kimpen study (n = 1688, aged 40–80 years),Citation9 the Boxmeer study (n = 1233, aged 40–70 years),Citation10 and the ENIGMA study (n = 2117, aged 18–91 years)Citation11 showed prevalences of 26%, 13%, and 17% (7% complete, 4% moderate, and 6% mild), respectively. All studies reported a distinct correlation between age and the prevalence (and severity) of ED. The sexual preference of the participants in these studies was not documented.
Limited data are available on ED in the “men who have sex with men” (MSM) population. Sandfort and de Keizer summarized 19 empirical studies of sexual problems in MSM and provided some data on the prevalence of ED ranging from 20% till 90%.Citation12 Bancroft et al studied erectile and ejaculatory problems in gay and heterosexual men and found that ED was reported more frequently by MSM and premature ejaculation more frequently by heterosexual men.Citation13 Hirshfield et al recently found in an internet sample of 7001 American MSM a prevalence of ED of 45%.Citation14
A variety of psychosocial causes for EDs in MSM have been described in the literature. Paff attributed a major role to performance anxiety, closely tied to an individual’s masculine identification.Citation15 The increased emphasis in the gay scene on being macho might have promoted the stress on performance and induced the anxiety that one is unable to perform. According to Paff, ED is also commonly found in intimate gay relationships, where it can express a variety of conflicts between the partners, as well as fear of intimacy or fear of rejection.Citation15
HIV infection is also associated with sexual dysfunction.Citation18 The use of antiviral therapy for HIV infection has negative side effects on the ability to get an erection. Additionally, psychological issues such as depression, performance anxiety, or fear of infecting others can cause ED.Citation16 HIV-positive status and homosexuality make people more vulnerable for the development of sexual dysfunctions.Citation17 Shindel et al found a greater prevalence of ED in MSM with progressive HIV infection.Citation18
In recent years, the use of phosphodiesterase type 5 (PDE5) inhibitors has become popular as a sexual enhancement aid among some men with ED. There are no specific data available on the use of these drugs among MSM. Shindel et al reported that the use of PDE5 inhibitor drugs was much more common in HIV-infected men.Citation18
The objective of this study was to determine the prevalence and severity of ED in a sample of the Belgian MSM population, without HIV-infection. In addition, we evaluated the relevance of patient characteristics (such as age, relationship, and education) and their sexual behavior on the presence of ED. We hypothesized that these factors would influence ED in the MSM population and heterosexual men in a similar manner. Finally, we investigated the use of PDE5 inhibitors among Belgian MSM.
Methods
Participants
The participants were recruited by references to the “GAy MEn Sex StudieS” (GAMESSS) website (http://www.gamesss.be) in various media. Links to the survey were posted on the websites of most gay organizations and a number of commercial gay-oriented websites. A list of the websites is shown in . In addition, 25,000 flyers, to which a condom had been attached, were handed out during various events, including the Gay Pride in Brussels and Antwerp. The registration period ran from April to December 2008.Citation19
Table 1 Websites that had a link to www.gamesss.be
Women, men under the age of 18, and men who have sexual relations exclusively with women were excluded. To exclude heterosexuals, we used the Kinsey’s Heterosexual–Homosexual Rating Scale, which describes a person’s sexual activity or experience.Citation20 We restricted our population to a sample of the Belgian MSM. These men indicated that they were currently engaging or interested in engaging in sexual contact with another man. Participants from outside Belgium and men with HIV-infection were filtered out.
Participation in this survey was voluntary and anonymous. The privacy of the participants was guaranteed. The study protocol was approved by the ethical committee of the university hospital of the Vrije Universiteit Brussel (Approval number BUN B14320083192).
Questionnaire
We developed an online questionnaire, which was available in three languages: Dutch, French, and English. For the translation in Dutch and French the forward/backward method was used. The GAMESSS questionnaire combined several comprehensive structured questionnaires that investigate several areas of male sexual experience. The online survey was placed on a tailor-made website, developed by the software engineers of our department. The website included an introduction to the study and its aims. The questionnaire incorporated the following items: socio-demographic data, sexual experience, getting erections, orgasm experience, experience with anal sex, and sex addiction. Internationally used and validated questionnaires were grouped into one online survey. For the detection of ED, the Erection Quality Scale (EQS) was used instead of the widely used International Index of Erectile Function (IIEF), the reason being the fact that the IIEF can only be used in a population of heterosexual men.Citation21 The EQS is a self-report measure assessing the quality of penile erections which can be used in both homosexual and heterosexual men (with or without their current partner). It’s a questionnaire consisting of eleven items, validated in different languages, including the three languages used in this study.Citation22 The EQS had an intraclass correlation coefficient of 0.85. Rosen et al developed a shortened version of the 15-item IIEF that contained five items: the IIEF-5.Citation23 The items focus on erectile function and intercourse satisfaction and allowed us to make a distinction between mild, moderate, or severe ED. The possible scores range from 5 to 25, and ED was classified into five categories based on the cutoff scores: severe (5–7), moderate (8–11), mild to moderate (12–16), mild (17–21), and no ED (22–25).Citation24 These five questions, consisting of a five-point Likert-scale, had a Cronbach’s alpha of 0.91 and were also part of the EQS.
The questionnaire was presented in a respondent-friendly manner, mostly as multiple choice questions. Participants had to indicate the most corresponding answer. For most questions answering was mandatory in order to continue the survey. Only when they indicated not having used PDE5 inhibitors for erectile dysfunction, were the three questions concerning the use of the substances skipped automatically.
In total, the questionnaire consisted of 90 questions. It took a considerable time to complete (>20 minutes), which increased the possibility that participants abandoned the survey prematurely. Visitors of the website were motivated to participate and to complete all the questions correctly. Therefore, the activation of intrinsic and extrinsic motivation of the respondents was used. We pointed out the importance of this survey to improve equal opportunities policy on MSM. To prevent the participants from giving up before finishing the questionnaire, we included a “teasing” factor. A tasteful black and white non-explicit photograph of one or two male nudes in various positions was added on each webpage. This stimulated the curiosity of the participants to continue the questionnaire.
Data management and statistical analysis
The data of this study were entered in an online registration system by the participants themselves. The recording of the data began only after the participants confirmed their male gender. At that time, the registration number (ID), a unique identifier (UID), and also the date and time of registration were recorded. The ID is simply an arithmetic sequence in the database. The UID is a random number between 150,000 and 999,999,999,999 which is stored in a cookie on the PC of the participant during registration. The cookie was automatically erased at the end of the questionnaire. The use of a cookie with a UID is necessary because the data should be written in the appropriate record as different participants simultaneously are entering data online. Date and time are not strictly necessary for the analysis of the data, but provide extra information on the evolution of the number of registrations. No IP address or other personal data from the computer of the registered participants were recorded. All of the data were stored in a MySQL database. The data can only be consulted through a secure web page with an Apache security login and password.
The databases were stored on a central secure server at the Faculty of Medicine and Pharmacy of the Vrije Universiteit Brussel. Several control measures ensured data quality and limited missing data by repeating some multiple choice questions with the possible answers in a different order. Data cleaning and data analyses for this study were performed using IBM SPSS Statistics 19.0.0 (IBM Corporation, Armonk, NY, USA) and Microsoft Excel (Microsoft Corporation, Redmond, WA, USA).
Data cleaning was performed in two steps: detection of errors in the dataset and correction of these errors. The data cleaning software looked for missing data, typing errors on data entry, coding errors, systematic repetitive answers, discordant answers, and errors related to misinterpretation of questions. Errors were detected by using descriptive statistics, scatter plots, and histograms. Presence of systematic repetitive answers was considered when the same option was entered systematically in consecutive questions.
Overall and age-specific prevalence estimates were calculated. Both bivariate and multivariate backwards stepwise logistic regression analyses were performed, with ED as the dependent variable. The following parameters were examined for their influence on the odds of having ED: age, level of education, number of sex partners (present and/or past), number of multiple sex partners in one period of time, age of the first sexual experience with a man, frequency of masturbation, frequency of sex with a partner, having a steady relationship, and the active/passive sex role. The variable “level of education” was dichotomized into “higher educational level,” defined as higher education course and (post) university, and “lower educational level,” defined as primary and secondary school.
Results
Participants
A total of 1752 Belgian men (age 35 ± 12 years; mean ± standard deviation [SD]), who identified themselves as MSM, answered the questions about erectile problems and current relationship status. The average age of their first sexual experience with a same-sex partner was 19 years. The first partner was usually 4 years older. shows the characteristics of the study population. The majority (70%) had a higher educational level. Of the 994 participants (57%) who had a steady relationship, 523 respondents (30% of the total study population) declared to be in an exclusive, monogamous relationship. A non-exclusive “open” relationship was indicated by 471 MSM (27% of the total study population). The remaining 758 participants (43%) were not in a relationship.
Table 2 Characteristics of the study population (n = 1752)
The mean frequency of sexual intercourse among Belgian MSM in our study population was 118 times a year. A majority of 66% had sexual intercourse with a man “at least” once a week. Only 2% of the MSM older than 55 years reported that they do not have any sexual relationship anymore. MSM younger than 26 years indicated that they masturbate nearly every day. Older men, over the age of 55, masturbated every three days. More than one third of the responders declared to have had more than 50 sex partners in their lifetime, and 47% indicated having sexual experience with more than three partners in the same period of time.
Prevalence of ED
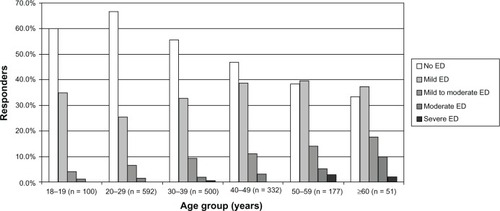
In the EQS, 784 participants (45%) indicated having a problem getting an erection (age 37 ± 12 years; mean ± SD). In this group of MSM, 71% had mild ED (IIEF-5 scoring between 17 and 21), 22% had mild to moderate ED (IIEF-5 scoring between 12 and 16), 6% had moderate ED (IIEF-5 scoring between 8 and 11), and 2% had severe ED (IIEF-5 scoring between 5 and 7). The prevalence and the severity of ED among MSM increased with age, as shown in .
Figure 1 IIEF-5 score in the study population of 1752 Belgian MSM.
Logistic regression analysis
We dichotomized into “ED” (IIEF-5 score less than 22) and “no ED” (IIEF-5 score between 22 and 25). shows the results of bivariate and multivariate logistic regression analyses to identify independent predisposing factors for developing ED, with ED as the dependent variable. When comparing subjects with or without ED, the bivariate analysis showed that the odds of having ED were influenced by the variables age, number of sex partners, age of first sexual experience with a same-sex partner, frequency of masturbation, frequency of sex with their partner, steady relationship, versatile sex role, passive sex role, problems with libido, ejaculation problems, and anodyspareunia.
Table 3 Odds ratios estimated by logistic regression analysis in a group of 1752 Belgian MSM
In the multivariate analysis, age, frequency of sex with their partner, steady relationship, versatile sex role, passive sex role, problems with libido, ejaculation problems, and anodyspareunia remained as independent predictors for having ED.
Treatment of ED
Ten percent of the participating Belgian MSM used a PDE5 inhibitor (age 43 ± 11 years; mean ± SD). Sildenafil (Viagra®) and tadalafil (Cialis®) were preferred for use by 24%. Vardenafil (Levitra®) was used by only 9%. Street drugs such as Kamagra, Libido Forte, and Viapro were used by 43%. After taking the drug, 83% were satisfied with the quality of the erections and 85% were satisfied with the timing of getting the erection.
Discussion
Our online study showed a 45% prevalence of some degree of ED in the participating MSM population. This is less than the 62% found by Mak et al in the general Belgian population.Citation8 They used a different methodology of interviewing an age-stratified random sample of the male population aged 40–70 years of two cities: Ghent and Charleroi. Compared with the MMAS,Citation7 the prevalence and the severity of ED are lower in the GAMESSS survey. The prevalence of ED in our survey is similar to what Hirshfield et al found.Citation14 Most cases of ED are – depending on age – related to a physical cause such as hypertension, diabetes, or cardiovascular or prostate diseases.Citation25 Among MSM, ED may have a negative impact on self-image and can cause frustration and anxiety for future sexual relationships. Sandfort and de Keizer speculated that MSM, as compared to heterosexual men, might find sexual problems more embarrassing and difficult to admit to, and are more vulnerable to performance anxiety because of a need to assert their masculinity.Citation12 This raises the complex issue of different patterns and expectations of relationships in the gay community. The sooner the patient raises the issue with his doctor, the sooner the diagnosis of ED can be made and a good treatment can be found for ED and the underlying problem(s) and/or disease(s). However, only 7%–30% of men with ED currently seek medical help, leaving the majority of men untreated.Citation6,Citation26
It’s still difficult for some MSM to reveal their sexual orientation and experience to their physician or pharmacist. In the Zzzip-report, a survey on the living conditions of gay men and women in Flanders between 2004–2006, Vincke et al concluded that 61% of the responders had informed their physicians about their sexual orientation, and 25% were not satisfied with the physician’s knowledge about the sexual problems among MSM.Citation27 If they were aware of the sexual orientation of their physician, being also gay, 94% were satisfied with the medical assistance they had received.Citation27
MSM who were in a steady relationship reported significantly (P < 0.001) less ED than MSM who did not have a steady relationship. The stress and anxiety of finding a new sex partner can cause a blockage of the ability to have an erection. MSM who are searching for a sex partner can fear HIV infection. Not knowing straight away the sexual preference of the new partner, being active, passive, or versatile can put pressure on erectile function. MSM who are in a steady relationship have a variety of sexual techniques to please one another, not only by penetration. MSM who are more passive in the sexual relation – also called “bottoms” – can have a pleasant sex life being penetrated by their partner with or without having an erection themselves – and thus without possible associated ED. The more MSM have sex with a partner, the less they suffer from ED. MSM who reported to have ejaculation problems also indicated having significantly more ED (P < 0.001).
The GAMESSS survey showed that 10% of the participating MSM took a drug to improve their erection and that the majority were satisfied with the effects. There were a remarkable number of street drugs used to treat ED. Usually, these drugs were purchased anonymously over the internet and without a medical prescription. These drugs are not approved for the treatment of ED. Little is known about the quality, the effectiveness, the side effects, and the dangers of these products. Features that attract the counterfeit market of these drugs are the high costs of the original PDE5 inhibitors and a specialized demand for such products by those willing to pay anonymously in order to avoid exposure or embarrassment.Citation28 Sildenafil, tadalafil, and vardenafil are the most common “embarrassment” counterfeit prescription drugs in the world. Physicians who treat patients with ED need to inform them about the true dangers of fake drugs. The counterfeiting of medications is a growing global problem that needs to be combated on all fronts.Citation28 Schnetzler et al reported that in Europe alone, approximately 6 million men bypass the official healthcare system to obtain a PDE5 inhibitor.Citation29 They not only expose themselves to the risks of using unapproved and uncontrolled products, but also miss out on the information on product use. Furthermore, by not consulting a doctor, they miss useful medical information on ED and underlying diseases related to ED.Citation29
More epidemiological work is required to generate solid assumptions of the prevalence rates in such subgroups of the population as the MSM population.
Limitations
Because there are limited studies of ED in the MSM population, cross-study comparisons are difficult to make. This study was designed as an exploratory, hypothesis-generating investigation. In the past, there usually was a representation problem for gay studies. Not all groups based on age, gender, and education within the gay population were equally represented. Older MSM and less educated people were less represented. Medical disorders such as diabetes mellitus, hypertension, obesity, autonomic nervous disorders, neuropathy, and the use of medication (for instance antihypertensive therapy) are associated with ED. There were no questions about the medical history of the participants, except the knowledge of their HIV status and the use of PDE5 inhibitors. We can only generalize findings to Belgian MSM, who used the online website from which participants were recruited. Mainly for MSM, the internet has become an important source of social networking and dating and they are early adaptors of new gadgets. In Western post-industrialized countries, asking people about their sexual preference is becoming more and more acceptable. In computer-assisted interviews, anonymous respondents are more willing to answer sensitive questions, such as on sexual preferences, than in person-to-person interviews. A disadvantage of e-research is that men without access to the internet could not participate. Because older people have less access to the internet, older MSM were likely to be underrepresented.
Strengths
Among the strengths of our population-based study are its large size and the coverage of different sexual dysfunctions. Not only ED, but also problems of libido, ejaculation, and pain during sexual activity were questioned. These other sexual dysfunctions will be reported later. To our knowledge, this is the first study on the prevalence of ED and the use of medication to improve the erection among MSM in Belgium.
Conclusion
The GAMESSS study provides the first population-based analysis of ED among MSM in Belgium. Some degree of ED was reported by 45% of the participants and 10% used a PDE5 inhibitor to improve erections. Further investigation of sexual dysfunctions is needed to improve the care for sexual problems in the MSM population.
Ethical approval
The study protocol was approved by the ethical committee of the university hospital of the Vrije Universiteit Brussel. The approval number was BUN B14320083192.
Acknowledgments
The authors thank all participating men for the registration and David Proot for the language editing.
Funding
The study was not funded by an external organization. The condoms for the promotion of the questionnaire were provided by LSE Holland.
Disclosure
Johan Vansintejan reports that he serves as a consultant to Menarini Belgium, Boehringer Ingelheim, and Eli Lilly. He has no stock or ownership to report.
The other authors have no conflicts of interest in this work.
References
- WespesEAmarEHatzichristouDMontorsiFPryorJVardiYGuidelines on erectile dysfunctionEuropean Urology20024111511999460
- DeBerardis GPellegriniFFranciosiMEDEN Study GroupManagement of erectile dysfunction in general practiceJ Sex Med2009641127113419138378
- AytaIAMcKinlayJBKraneRJThe likely worldwide increase in erectile dysfunction between 1995 and 2005 and some possible policy consequencesBJU Int1999841505610444124
- BenerAAl-AnsariAAl-HamaqAOElbagiIEAfifiMPrevalence of erectile dysfunction among hypertensive and nonhypertensive Qatari menMedicina (Kaunas)2007431187087818084144
- PrinsJBlankerMHBohnenAMThomasSBoschJLPrevalence of erectile dysfunction: a systematic review of population-based studiesInt J Impot Res200214642243212494273
- KubinMWagnerGFugl-MeyerAREpidemiology of erectile dysfunctionInt J Impot Res2003151637112605242
- FeldmanHAGoldsteinIHatzichristouDGKraneRJMcKinlayJBImpotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging StudyJ Urol1994151154618254833
- MakRDe BackerGKornitzerMDe MeyerJMPrevalence and correlates of erectile dysfunction in a population-based study in BelgiumEur Urol200241213213812074399
- BlankerMHBohnenAMGroeneveldFPCorrelates for erectile and ejaculatory dysfunction in older Dutch men: a community-based studyJ Am Geriatr Soc200149443644211347788
- MeulemanEJDonkersLHRobertsonCKeechMBoylePKiemeneyLAErectile dysfunction: prevalence and effect on the quality of life; Boxmeer studyNed Tijdschr Geneeskd200114512576581 Dutch11293998
- de BoerBJBotsMLNijeholtAAMoorsJPPietersHMVerheijTJErectile dysfunction in primary care: prevalence and patient characteristics. The ENIGMA studyInt J Impot Res200416435836414961062
- SandfortTGde KeizerMSexual problems in gay men: an overview of empirical researchAnnu Rev Sex Res2001129312012666738
- BancroftJCarnesLJanssenEGoodrichDLongJSErectile and ejaculatory problems in gay and heterosexual menArch Sex Behav200534328529715971011
- HirshfieldSChiassonMAWagmillerRLJrSexual dysfunction in an Internet sample of US men who have sex with menJ Sex Med2010793104311419968773
- PaffBASexual dysfunction in gay men requesting treatmentJ Sex Marital Ther19851113183989875
- LambaHGoldmeierDMackieNEScullardGAntiretroviral therapy is associated with sexual dysfunction and with increased serum oestradiol levels in menInt J STD AIDS200415423423715075015
- PlatteauTvan LankveldJSexual dysfunctions in homosexual men with hiv: a review of the literatureTijdschrift Voor Seksuologie200529205214 Dutch
- ShindelAWHorbergMASmithJFBreyerBNSexual dysfunction, HIV, and AIDS in men who have sex with menAIDS Patient Care STDS201125634134921501095
- VansintejanJVandevoordeJDevroeyDThe GAy MEn Sex StudieS: design of an online registration of sexual behaviour of men having sex with men and preliminary results (GAMESSS-study)Cent Eur J Public Health2013211485323741901
- KinseyACPomeroyWRMartinCESexual behavior in the human male. 1948Am J Public Health200393689489812773346
- RosenRCRileyAWagnerGOsterlohIHKirkpatrickJMishraAThe international index of erectile function (IIEF): a multidimensional scale for assessment of erectile dysfunctionUrology19974968228309187685
- WinczeJRosenRCarsonCErection quality scale: initial scale development and validationUrology200464235135615302493
- RosenRCCappelleriJCSmithMDLipskyJPenaBMDevelopment and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunctionInt J Impot Res199911631932610637462
- RhodenELTelökenCSogariPRVargas SoutoCAThe use of the simplified Inernational Index of erectile Function (IIEF-5) as a diagnostic tool to study the prevalence of erectile dysfunctionInt J Impot Res200214424525012152112
- LueTFErectile dysfunctionN Engl J Med2000342241802181310853004
- MulhallJKingRGlinaSHvidstenKImportance of and satisfaction with sex among men and women worldwide: results of the global better sex surveyJ Sex Med20085478879518284556
- VinckeJDewaeleAVan den BergheQCoxNZzzip, een statistisch onderzoek met het oog op het verzamelen van basismateriaal over de doelgroep holebi’s [Zzzip report: a statistical study in order to collect basic material on the gay community]BrusselsMinisterie van de Vlaamse gemeenschap gelijke kansen in Vlaanderen2006 Dutch
- HellstromWJThe growing concerns regarding counterfeit medicationsJ Sex Med2011811321199373
- SchnetzlerGBanksIKirbyMZouKHSymondsTCharacteristics, behaviors, and attitudes of men bypassing the healthcare system when obtaining phosphodiesterase type 5 inhibitorsJ Sex Med2010731237124620136707