
Abstract
Purpose
To explore the early diagnostic value of superb microvascular imaging (SMI) features within the rotator cuff gap for frozen shoulder.
Patients and Methods
This prospective study enrolled patients with acute early-stage frozen shoulder seeking treatment at Zhabei Central Hospital in Jing’an District, Shanghai, between July 2021 and December 2022 were enrolled in this study. Healthy controls were collected in a 1:1 ratio from the same hospital’s physical examination center. All participants underwent SMI and power Doppler ultrasound (PDUS) of the rotator cuff gap.
Results
The study included 79 patients with frozen shoulder and 77 healthy controls. Compared with the healthy control group, the patient group had a higher proportion of hypoechoic rotator cuff gap (81.0% vs 48.1%, P<0.001), a thicker coracohumeral ligament (2.60±1.01 vs 2.03±0.97, P<0.001), a thicker glenohumeral joint capsule (3.10±0.99 vs 2.46±1.17, P<0.001), and elevated blood grading using SMI (P<0.001) and PDUS (P=0.014). The highest area under the curve (AUC) was observed for SMI blood flow grading (AUC=0.824, 95% CI: 0.755–0.880, P<0.001), resulting in 82% sensitivity and 77% specificity when using a cutoff of 1. SMI blood flow grading was associated with external rotation <30° (P=0.007) and abduction <30° (P=0.013) but not with internal rotation <30° (P=0.630) or flexion <30° (P=0.562).
Conclusion
The grading of SMI blood flow may emerge as a valuable predictive indicator for the early stages of frozen shoulder. This simple ultrasound technique holds the potential to enhance the diagnostic process, enabling early initiation of treatment and potentially improving patient outcomes.
Introduction
Frozen shoulder, also known as adhesive capsulitis of the shoulder, is a debilitating condition characterized by the development of excessive scar tissue or adhesions within the glenohumeral joint capsule, leading to stiffness, severe pain, and restricted passive and active range of motion in the shoulder.Citation1–4 The prevalence of frozen shoulder is 2%-5% in the general population,Citation3,Citation4 5%-11% after shoulder surgery,Citation4 about 10 after breast cancer surgery,Citation4 and 10%-20% of patients with diabetes (type 1 or 2).Citation2 While a frozen shoulder typically resolves on its own within 1–3 years, it can persist long-term in 20%-50% of patients. Early diagnosis and intervention are crucial, as they can significantly alleviate shoulder pain, enhance joint mobility, expedite recovery, and reduce the overall burden of the disease.Citation4,Citation5
A primary pathological mechanism appears to center around chronic inflammatory reactions and fibrosis affecting various tissues, including shoulder muscles, ligaments, tendons, synovial sacs, and joint capsules.Citation6 These early pathophysiological changes are associated with angiogenesis and vascular endothelial growth factor in these structures, with angiogenesis preceding both organic and functional alterations.Citation7,Citation8 Furthermore, vascular abnormalities have been linked to increased adjacent nerve abnormalities.Citation9 As a result, early changes in local blood flow due to inflammatory reactions could be early events in the pathogenesis of frozen shoulder. The rotator cuff gap is located between the supraspinatus and subscapularis and is a crucial structure for maintaining shoulder joint stability. Frozen shoulder often involves the rotator cuff gap and surrounding soft tissues early in the disease, leading to corresponding pathological changes captured by imaging techniques.Citation10
Among these imaging techniques, ultrasound provides real-time dynamic examination with high soft tissue resolution. Color Doppler ultrasound (CDFI) and power Doppler ultrasound (PDUS) hold diagnostic values for frozen shoulder by detecting increased blood flow in the rotator cuff gap and subacromial fat triangle, early features of the condition.Citation11–13 However, the shallow location of these anatomical structures and the prevalence of low-velocity microvascular blood supply limit the blood flow display rates of CDFI and PDUS. Superb microvascular imaging (SMI) represents an innovative ultrasound blood flow imaging technique that effectively distinguishes blood flow signals from tissue motion artifacts, enabling the visualization of extremely low flow microvessels without the need for contrast agents.Citation14,Citation15 While research has extensively explored SMI in conditions associated with angiogenesis, such as breast cancer,Citation16 rheumatoid arthritis,Citation17 and thyroid nodules,Citation18 the application of SMI in the context of the frozen shoulder has been notably limited. Only two studies, conducted in South Korea and Singapore, have investigated the use of SMI in frozen shoulder and exhibited superior diagnostic value for frozen shoulder compared to CDFI and PDUS.Citation19,Citation20 Despite the promising findings, both studies had limited sample sizes, and research on SMI in the context of frozen shoulder remains scarce.
Therefore, this study aimed to explore the early diagnostic value of SMI features within the rotator cuff gap for frozen shoulder. We hypothesized that SMI could be used to diagnose frozen shoulder, even in its early stages.
Materials and Methods
Study Design and Participants
This prospective study enrolled patients with acute early-stage frozen shoulder who sought treatment at Zhabei Central Hospital in Jing’an District, Shanghai, between July 2021 and December 2022. The healthy controls were enrolled from the same hospital at the physical examination center with a 1:1 ratio.
The diagnosis of frozen shoulder relied primarily on medical history and clinical presentation, characterized by progressive restrictions in both active and passive shoulder movements, accompanied by pain. Early cases were defined as those presenting symptoms for 1–3 months. Patients who were 30–75 years of age, complained of persistent shoulder pain with nocturnal exacerbation for 0–3 months, and displayed multi-directional restrictions in both active and passive shoulder movements were enrolled. Patients with shoulder joint trauma or surgery within the past 6 months, those with bilateral shoulder movement restrictions or pain, or patients with a history of rotator cuff tear, rheumatoid arthritis, or previous frozen shoulder were excluded. Healthy controls of 30–75 years of age and without frozen shoulder diagnosis at physical examination were enrolled. The exclusion criteria were the same with frozen shoulder patients.
This study adhered to the principles outlined in the Declaration of Helsinki, and was approved by the ethics committee of Zhabei Central Hospital in Jing’an District, Shanghai (ZBLL2022020904). All participants provided signed informed consent.
Procedure
The participants’ demographic and clinical data were retrieved from the electronic patient chart, including demographic data (age, sex, height, and weight), current medical history (symptoms related to frozen shoulder and treatment history), past medical history (comorbidities such as diabetes, hypertension, and hyperlipidemia), and medication history. The pain intensity was evaluated using the visual analogue scale (VAS).
Two attending physicians, each with over 10 years of experience in ultrasound, conducted shoulder joint range of motion (external rotation, internal rotation, abduction, and flexion) examinations on the enrolled study population using a standard goniometer for measurement and evaluation. The intraclass correlation coefficient (ICC) was determined between the two physicians.
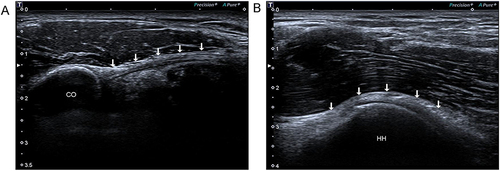
A Toshiba Aplio 400 color Doppler ultrasound diagnostic apparatus with a probe frequency of 14 MHz was used for SMI. The participants assumed a seated position with the shoulder joint in a neutral position. The probe was obliquely oriented to display the rotator cuff gap between the supraspinatus and subscapularis. The echogenicity of the rotator cuff gap was assessed. Subsequently, the shoulder joint was externally rotated, placing the probe on the lateral aspect of the acromion to visualize the coracohumeral ligament and measure its maximum thickness ().
Figure 1 Measurement of coracohumeral ligament and capsule thickness. (A) Coracohumeral ligament. The arrow indicated coracohumeral ligament; (B) Glenohumeral joint capsule. The arrow indicated glenohumeral joint capsule.
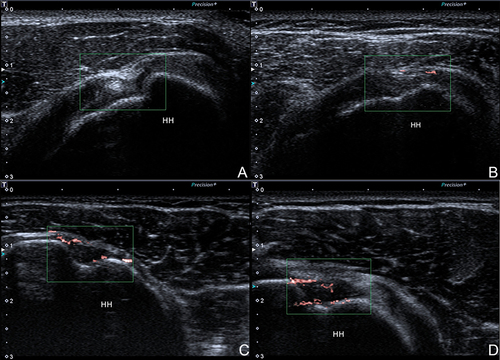
Blood flow information was collected in the rotator cuff gap using SMI and PDUS. For SMI, the image depth range in B-mode was 3 cm, with a fixed-size (1.5x1 cm) region of interest (ROI) box used for SMI to maintain a high frame rate of over 50 frames per second. The velocity range was less than 2.5 cm/s, the SMI frequency was 7 MHz, low-grade filter levels were applied, and maximum SMI gain was achieved before the occurrence of background color aliasing. The PDUS examination was performed at the same level, with the color velocity range adjusted to less than 2.5 cm/s, color frequency set at 7 MHz, and gain adjusted just below the level of aliasing. The blood flow signals were graded on a scale of 0–3: 0: no blood flow signals in the rotator cuff gap (); Grade I: one or two dot-like blood flow signals visible in the rotator cuff gap (); Grade II: three or four short linear blood flow signals visible in the rotator cuff gap, not exceeding 50% of the gap (); Grade III: branching or mesh-like blood flow signals visible in the rotator cuff gap, exceeding 50% of the gap ().Citation19
Figure 2 The blood flow signals. (A) Grade 0: no blood flow signals; (B) Grade 1: one or two dot-like blood flow signals; (C) Grade 2: three or four short linear blood flow signals; (D) Grade 3: branching or mesh-like blood flow signals.
Sample Size Calculation
The sample size for this study was calculated using the following formula:
Where N represents the sample size per group, α=0.05, δ=0.1, Z1-α/2=1.96, and p represents the estimated sensitivity or specificity of the diagnostic test. In this study, the estimated sensitivity was approximately 0.90, and the specificity was approximately 0.80. Therefore, the required sample size was 62 participants per group. Considering potential data invalidity during sample collection, it was anticipated to collect at least 70 participants in each group.
Statistical Analysis
SPSS 26.0 (IBM, Armonk, NY, USA) was used for statistical analysis. The categorical data were presented as n (%) and analyzed using the chi-square test. The continuous data were tested for normality using the Shapiro–Wilk test. The continuous data with a normal distribution were presented as means ± standard deviations (SD) and analyzed using the independent samples t-test. The continuous data with a skewed distribution were presented as medians (ranges) and analyzed using the Mann–Whitney U-test. Receiver operating characteristics (ROC) curve analysis was conducted using MedCalc (MedCalc Software bvba, Ostend, Belgium). Two-sided P <0.05 were considered statistically significant.
Results
Characteristics of the Participants
The study enrolled 79 patients with frozen shoulder and 77 healthy controls. There were no significant differences in sex, hypertension, diabetes, medication and rehabilitation history, body mass index (BMI), age, height, and weight between the two groups (all P>0.05). Compared with the healthy controls, the patients had a higher frequency of thyroid diseases (19.0% vs 5.2%, P=0.008) and higher pain scores (6.00±2.00 vs 1.00±0.00, P<0.001) ().
Table 1 Characteristics of the Patients
Ultrasound Characteristics
The ICC between the two physicians was 0.906. Compared with the healthy control group, the patient group had a higher proportion of hypoechoic rotator cuff gap (81.0% vs 48.1%, P<0.001), a thicker coracohumeral ligament (2.60±1.01 vs 2.03±0.97, P<0.001), a thicker glenohumeral joint capsule (3.10±0.99 vs 2.46±1.17, P<0.001), and a higher blood grading using SMI (P<0.001) and PDUS (P=0.014) ().
Table 2 Ultrasound Feature Indicators Between the Two Groups
Receiver Operating Characteristics Analysis
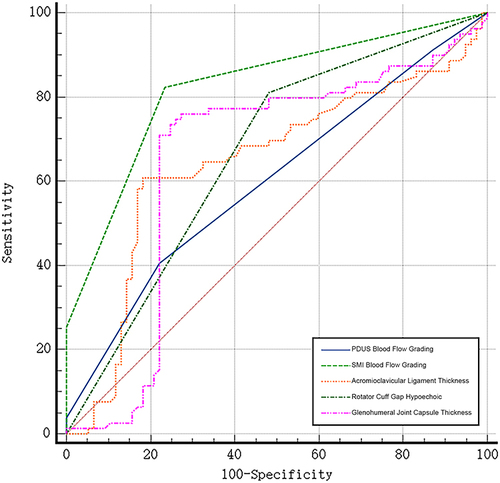
The highest area under the curve (AUC) was observed for SMI blood flow grading (AUC=0.824, 95% CI: 0.755–0.880), resulting in 82% sensitivity and 77% specificity when using a cutoff of 1. The DeLong test indicated the SMI blood flow grading had superior diagnostic value compared to other characteristics (all P<0.05): hypoechoic rotator cuff gap (AUC=0.665), glenohumeral joint capsule thickness (AUC=0.651), coracohumeral ligament thickness (AUC=0.643), and PDUS blood flow grading (AUC=0.600) ( and ).
Table 3 ROC Analysis
Figure 3 Receiver operating characteristics (ROC) curves for different features.
Association Between SMI and Clinical Features
As shown in , the SMI blood flow grading was associated with external rotation <30° (P=0.007) and abduction <30° (P=0.013) but not with internal rotation <30° (P=0.630) or flexion <30° (P=0.562).
Table 4 Activity in the Patient Group in Relation to the SMI Blood Flow Grading
Discussion
This prospective study explored the early diagnostic value of SMI features in the rotator cuff gap for frozen shoulder. The Results indicate that the grading of SMI blood flow in the rotator cuff gap may serve as a predictive indicator for the early stages of frozen shoulder. These findings offer compelling evidence supporting the application of SMI in the diagnosis of frozen shoulder. The integration of SMI into diagnostic protocols has the potential to facilitate the earlier identification of frozen shoulder, enabling prompt initiation of treatment and possibly improving prognosis.
Increased vascular responses are observed in rotator cuff tendinopathy, which has been hypothesized to result from microtrauma.Citation21,Citation22 That increased microvessel density is considered to participate in the weakening of the mechanical properties of the tendons and other fibrous structures, predisposing them to degeneration.Citation22,Citation23 Studies on frozen shoulder revealed higher vascularity using MRI,Citation12,Citation24 arthroscopy,Citation25 histology,Citation8 and angiography.Citation7 Accordingly, in the present study, SMI and PDUS blood flow signals were higher in the patients with frozen shoulder than in healthy controls. Those results are supported by studies that reported higher neovascularization in symptomatic tendons than in asymptomatic ones.Citation26,Citation27
The present study is supported by previous ones that showed higher SMI signals than conventional Doppler ultrasound or PDUS in affected tendinous and fibrous structures.Citation19,Citation28,Citation29 Kim et alCitation19 showed that SMI was superior to PDUS in depicting blood flow in patients with frozen shoulder. Kim et alCitation19 also reported that SMI blood flow signals in patients with frozen shoulder correlated to the range of shoulder motion. In the present study, the SMI blood flow signals correlated to the external rotation <30° and abduction <30°, but not with internal rotation <30° or flexion <30°. Since SMI measures blood flow, it could be that specific movements block or impair blood flow from specific intraarticular sources. The findings need to be explained by further pathology or anatomy studies.
Previous studies reported changes like tendon thickening, hypoechogenicity, and/or heterogeneity between symptomatic and asymptomatic tendons using MRI and conventional ultrasound.Citation30,Citation31 Cook & PurdamCitation32 and Abate et alCitation33 suggested that the progression of fibrous tissue diseases is a continuing process, progressing from asymptomatic to symptomatic conditions. All patients in the present study were with early frozen shoulder. Various indicators were tested, including SMI blood flow grading, hypoechoic rotator cuff gap, glenohumeral joint capsule thickness, coracohumeral ligament thickness, and PDUS blood flow grading. SMI blood flow grading displayed the highest AUC for early frozen shoulder diagnosis. The findings indicated although the initial signs of fibrous structure neovascularization and degeneration are usually asymptomatic,Citation34 they can be used for early diagnosis. Nevertheless, longitudinal studies of SMI in patients with frozen shoulder would be necessary to examine the changes in time.
This study had limitations. It was performed at a single center, limiting the generalizability of the conclusions. Only ultrasound was performed, and there were no comparisons with X-ray, CT, or MRI. A previous study showed that exercise could produce a vascular response in tendons,Citation35 and the dose-response between exercise and SMI signal in relation to frozen shoulder diagnosis is unknown. Even though good reliability in SMI assessment has been reported, it was not examined in the present study.Citation36,Citation37 Prospective, multicenter, large-sample studies are needed to provide higher-level evidence.
Conclusion
In Conclusion, the grading of SMI blood flow in the rotator cuff gap may serve as a predictive indicator for the early stages of frozen shoulder. It is a simple ultrasound technique that could be used to improve the diagnosis of frozen shoulder and start treatments early.
Disclosure
The authors report no conflicts of interest in this work.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Additional information
Funding
References
- Ewald A. Adhesive capsulitis: a review. Am Fam Physician. 2011;83(4):417–422.
- Le HV, Lee SJ, Nazarian A, Rodriguez EK. Adhesive capsulitis of the shoulder: review of pathophysiology and current clinical treatments. Shoulder Elbow. 2017;9(2):75–84. doi:10.1177/1758573216676786
- Ramirez J. Adhesive capsulitis: diagnosis and management. Am Fam Physician. 2019;99(5):297–300.
- Redler LH, Dennis ER. Treatment of adhesive capsulitis of the shoulder. J Am Acad Orthop Surg. 2019;27(12):e544–e554. doi:10.5435/JAAOS-D-17-00606
- Wong CK, Levine WN, Deo K, et al. Natural history of frozen shoulder: fact or fiction? A systematic review. Physiotherapy. 2017;103(1):40–47. doi:10.1016/j.physio.2016.05.009
- Fields BKK, Skalski MR, Patel DB, et al. Adhesive capsulitis: review of imaging findings, pathophysiology, clinical presentation, and treatment options. Skeletal Radiol. 2019;48(8):1171–1184. doi:10.1007/s00256-018-3139-6
- Okuno Y, Iwamoto W, Matsumura N, et al. Clinical outcomes of transcatheter arterial embolization for adhesive capsulitis resistant to conservative treatment. J Vasc Interv Radiol. 2017;28(2):161–167e161. doi:10.1016/j.jvir.2016.09.028
- Ryan V, Brown H, Minns Lowe CJ, Lewis JS. The pathophysiology associated with primary (idiopathic) frozen shoulder: a systematic review. BMC Musculoskelet Disord. 2016;17(1):340. doi:10.1186/s12891-016-1190-9
- McKean D, Yoong P, Brooks R, et al. Shoulder manipulation under targeted ultrasound-guided rotator interval block for adhesive capsulitis. Skeletal Radiol. 2019;48(8):1269–1274. doi:10.1007/s00256-018-3105-3
- Date A, Rahman L. Frozen shoulder: overview of clinical presentation and review of the current evidence base for management strategies. Future Sci OA. 2020;6(10):FSO647. doi:10.2144/fsoa-2020-0145
- Walmsley S, Osmotherly PG, Walker CJ, Rivett DA. Power Doppler ultrasonography in the early diagnosis of primary/idiopathic adhesive capsulitis: an exploratory study. J Manipulative Physiol Ther. 2013;36(7):428–435. doi:10.1016/j.jmpt.2013.05.024
- Sasanuma H, Sugimoto H, Fujita A, et al. Characteristics of dynamic magnetic resonance imaging of idiopathic severe frozen shoulder. J Shoulder Elbow Surg. 2017;26(2):e52–e57. doi:10.1016/j.jse.2016.06.003
- Park J, Choi YH, Chai JW, et al. Anterior capsular abnormality: another important MRI finding for the diagnosis of adhesive capsulitis of the shoulder. Skeletal Radiol. 2019;48(4):543–552. doi:10.1007/s00256-018-3064-8
- Ohno Y, Fujimoto T, Shibata Y. A new era in diagnostic ultrasound, superb microvascular imaging: preliminary results in pediatric hepato-gastrointestinal disorders. Eur J Pediatr Surg. 2017;27(1):20–25. doi:10.1055/s-0036-1593381
- Jiang ZZ, Huang YH, Shen HL, Liu XT. Clinical Applications of Superb Microvascular Imaging in the liver, breast, thyroid, skeletal muscle, and carotid plaques. J Ultrasound Med. 2019;38(11):2811–2820. doi:10.1002/jum.15008
- Arslan FZ, Altunkeser A, Korez MK, et al. The importance of superb microvascular imaging for the differentiation of malignant breast lesions from benign lesions. Eur J Breast Health. 2022;18(1):48–54. doi:10.4274/ejbh.galenos.2021.2021-6-1
- Diao XH, Shen Y, Chen L, et al. Superb microvascular imaging is as sensitive as contrast-enhanced ultrasound for detecting synovial vascularity in rheumatoid arthritis. Quant Imaging Med Surg. 2022;12(5):2866–2876. doi:10.21037/qims-21-859
- Jin H, Wang C, Jin X. Superb microvascular imaging for distinguishing thyroid nodules: a meta-analysis (PRISMA). Medicine. 2022;101(24):e29505. doi:10.1097/MD.0000000000029505
- Kim DH, Choi YH, Oh S, Kim HJ, Chai JW. Ultrasound microflow imaging technology for diagnosis of adhesive capsulitis of the shoulder. J Ultrasound Med. 2020;39(5):967–976. doi:10.1002/jum.15181
- Ooi CC, Wong SK, Ma VC, et al. The prevalence of neovascularity in rotator cuff tendinopathy: comparing conventional Doppler with superb microvascular imaging. Clin Radiol. 2022;77(6):e442–e448. doi:10.1016/j.crad.2022.03.003
- Lewis J, McCreesh K, Roy JS, Ginn K. Rotator cuff tendinopathy: navigating the diagnosis-management conundrum. J Orthop Sports Phys Ther. 2015;45(11):923–937. doi:10.2519/jospt.2015.5941
- Levy O, Relwani J, Zaman T, et al. Measurement of blood flow in the rotator cuff using laser Doppler flowmetry. J Bone Joint Surg Br. 2008;90(7):893–898. doi:10.1302/0301-620X.90B7.19918
- Silvestri E, Biggi E, Molfetta L, et al. Power Doppler analysis of tendon vascularization. Int J Tissue React. 2003;25(4):149–158.
- Ahn KS, Kang CH, Kim Y, Jeong WK. Diagnosis of adhesive capsulitis: comparison of contrast-enhanced MRI with noncontrast-enhanced MRI. Clin Imaging. 2015;39(6):1061–1067. doi:10.1016/j.clinimag.2015.08.006
- Wiley AM. Arthroscopic appearance of frozen shoulder. Arthroscopy. 1991;7(2):138–143. doi:10.1016/0749-8063(91)90098-I
- Lewis JS, Raza SA, Pilcher J, Heron C, Poloniecki JD. The prevalence of neovascularity in patients clinically diagnosed with rotator cuff tendinopathy. BMC Musculoskelet Disord. 2009;10(1):163. doi:10.1186/1471-2474-10-163
- Visnes H, Tegnander A, Bahr R. Ultrasound characteristics of the patellar and quadriceps tendons among young elite athletes. Scand J Med Sci Sports. 2015;25(2):205–215. doi:10.1111/sms.12191
- Lim AKP, Satchithananda K, Dick EA, Abraham S, Cosgrove DO. Microflow imaging: new Doppler technology to detect low-grade inflammation in patients with arthritis. Eur Radiol. 2018;28(3):1046–1053. doi:10.1007/s00330-017-5016-4
- Arslan S, Karahan AY, Oncu F, et al. Diagnostic performance of superb microvascular imaging and other sonographic modalities in the assessment of lateral epicondylosis. J Ultrasound Med. 2018;37(3):585–593. doi:10.1002/jum.14369
- Giombini A, Dragoni S, Di Cesare A, et al. Asymptomatic A chilles, patellar, and quadriceps tendinopathy: a longitudinal clinical and ultrasonographic study in elite fencers. Scand J Med Sci Sports. 2013;23(3):311–316. doi:10.1111/j.1600-0838.2011.01400.x
- Gill TK, Shanahan EM, Allison D, Alcorn D, Hill CL. Prevalence of abnormalities on shoulder MRI in symptomatic and asymptomatic older adults. Int J Rheum Dis. 2014;17(8):863–871. doi:10.1111/1756-185X.12476
- Cook JL, Purdam CR. Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. Br J Sports Med. 2009;43(6):409–416. doi:10.1136/bjsm.2008.051193
- Abate M, Silbernagel KG, Siljeholm C, et al. Pathogenesis of tendinopathies: inflammation or degeneration? Arthritis Res Ther. 2009;11(3):235. doi:10.1186/ar2723
- Yamaguchi K, Tetro AM, Blam O, et al. Natural history of asymptomatic rotator cuff tears: a longitudinal analysis of asymptomatic tears detected sonographically. J Shoulder Elbow Surg. 2001;10(3):199–203. doi:10.1067/mse.2001.113086
- Boesen MI, Boesen A, Koenig MJ, Bliddal H, Torp-Pedersen S. Ultrasonographic investigation of the Achilles tendon in elite badminton players using color Doppler. Am J Sports Med. 2006;34(12):2013–2021. doi:10.1177/0363546506290188
- Orlandi D, Gitto S, Perugin Bernardi S, et al. Advanced power Doppler technique increases synovial vascularity detection in patients with rheumatoid arthritis. Ultrasound Med Biol. 2017;43(9):1880–1887. doi:10.1016/j.ultrasmedbio.2017.05.004
- Cook JL, Ptazsnik R, Kiss ZS, et al. High reproducibility of patellar tendon vascularity assessed by colour Doppler ultrasonography: a reliable measurement tool for quantifying tendon pathology. Br J Sports Med. 2005;39(10):700–703. doi:10.1136/bjsm.2004.016410