
Abstract
Background
Hemorrhoids, common benign anorectal conditions, are associated with various factors, such as low fiber intake, constipation, and pregnancy. Treatment typically involves procedures such as banding and surgery.
Objective
This retrospective investigation aimed to assess the frequency and demography of hemorrhoids in Kabul, Afghanistan.
Materials and Methods
This study was conducted at Jamhuriat Hospital in Kabul, Afghanistan. Two hundred and fifty-two patients who were diagnosed with hemorrhoids were included. All pertinent demographic data were collected from the medical records and analyzed using IBM SPSS Statistics 25.
Results
Males composed 83.7% of the patients, and 32.9% were aged 30–40 years. A lower socioeconomic status was common (61.1%). Bleeding, prolapse, and pain were frequent symptoms. Surgical management was common for third- and fourth-degree hemorrhoids (51.6%).
Conclusion
This study found a high prevalence of hemorrhoids among males (83.7%) and low-income individuals (61.1%), highlighting the need for further research into risk factors for delayed presentation.
Introduction
Hemorrhoids, or piles, are clusters of enlarged blood vessels in the anus and anal canal, causing symptoms like swelling, itching, pain during bowel movements, and rectal bleeding.Citation1 Hemorrhoids are a frequent cause of anal issues and the most common benign anorectal disorder identified in clinical practice, present in about 50% of colorectal examinations.Citation2
Globally, hemorrhoids affect about 4.4% of the population, with the highest prevalence in Australia (38.93%), Israel (16%), and Korea (14.4%).Citation3–5 They are classified into internal and external types, with internal hemorrhoids further categorized into four degrees based on their severity.Citation6 Risk factors include a low-fiber diet, chronic constipation or diarrhea, frequent straining, pregnancy, a sedentary lifestyle, and obesity.Citation7–10
The American College of Gastroenterology (ACG) recommends dietary and lifestyle changes for early-stage hemorrhoids and more invasive treatments for advanced cases.Citation11 Despite extensive global research, there is a significant gap in the literature regarding the prevalence and demographic characteristics of hemorrhoids in Afghanistan. Understanding the demographics in this region is crucial due to its unique socio-economic conditions, cultural norms, and healthcare access, which may result in different prevalence and presentation patterns compared to other regions.
This study aims to fill this gap by assessing the demographic characteristics and prevalence of hemorrhoids in a tertiary hospital in Kabul, Afghanistan, thereby bridging the gap between existing literature and the clinical presentations observed in Kabul.
Materials and Methods
Place of Study
This study was conducted at Jamhuriat Hospital, a governmental hospital in Kabul. Jamhuriat Hospital is a multi-specialty facility with a capacity to accommodate 350 patients. It operates under government funding and provides a wide range of treatment services including, urology, nephrology, neurosurgery, oncology, ENT, heart surgery, colorectal surgery, and etc. The hospital primarily serves patients referred from all parts of Afghanistan, offering comprehensive healthcare to a diverse population.
The Type of Study
A retrospective study.
Sampling Method
Consecutive.
Data Collection
Data were collected from the medical records of patients admitted with hemorrhoids to the surgery ward of Jamhuriat Hospital from March 2021 to March 2022. The study aimed to investigate various factors including demographic information such as age, sex, place of residence, occupation, and medical history, degree of hemorrhoids, treatment type (all patients undergone surgical treatment), signs and symptoms, types of hemorrhoids, economic status, and marital status. These variables were selected based on their potential relevance to understanding the demography, clinical presentation and management of hemorrhoids in our patient population.
The Inclusion Criteria for Patients Were as Follows
Aged 18 to 80 years, diagnosed with hemorrhoids, and admitted to the surgery ward with complete medical records.
The Exclusion Criteria for Patients Were as Follows
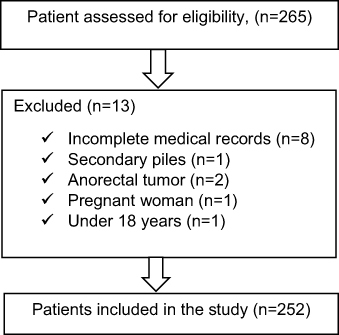
Patients with secondary piles or anorectal tumors, pregnant women, and those under 18 years of age. Additionally, 8 patients were excluded from the study due to incomplete medical records ().
Figure 1 Illustrating the flow of participants through the study.
Statistical Analysis
The findings are displayed in tables, where numbers and percentages are analyzed and compared using descriptive statistics in SPSS Statistics 25.
Ethical Issues
Ethics approval was obtained from the Scientific Research Center at Kateb University in Afghanistan (Approval code: AF.KU.SRC.22002, dated 18th December 2022), and the study was conducted in adherence to the principles outlined in the Declaration of Helsinki. Given the retrospective nature of the study, patient consent was not required. Measures to uphold data confidentiality were strictly observed throughout the study process.
Results
In this study, 252 records of patients diagnosed with hemorrhoids between March 2021 and March 2022 were identified (). The mean age of the patients was 40.53 ± 15.08 years, and the ratio of males to females was approximately 5.15:1 ().
Table 1 The Sociodemographic Characteristics of Adult Patients Admitted to the Surgery Ward of Jamhuriat Hospital in Kabul from 2021 to 2022
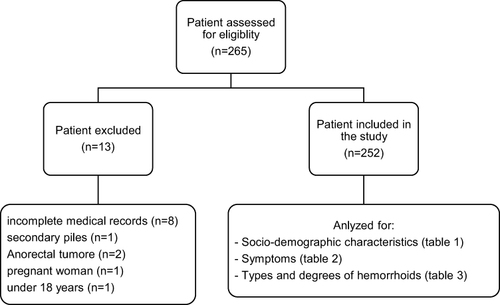
Figure 2 This CONSORT diagram outlines the flow of participants in the study conducted at Jamhuriat Hospital, Kabul from 2021 to 2022. Initially, 265 patients were admitted to the surgery ward. After applying exclusion criteria (incomplete medical records, secondary piles, anorectal tumor, pregnant woman, and age < 18 years), 252 patients were eligible for the study. All 252 eligible patients were included in the analysis for sociodemographic characteristics (as detailed in ), symptoms (as detailed in ), and types/degrees of hemorrhoids (as detailed in ).
The majority of patients (69.4%, 175 out of 252) were from the Kabul province of Afghanistan. Additionally, unemployment was the predominant occupation among patients, accounting for 57.1% (144 out of 252) of the sample. In contrast, policemen, carpenters, and pharmacists constituted the least represented occupational groups, each comprising only 0.4% (1 out of 252). Moreover, a significant proportion of patients were married, with a ratio of 5.63:1 ().
Regarding medical history, while most patients (49.2%, 124 out of 252) had unremarkable medical records, constipation (34.9%, 88 out of 252) was among the most prevalent conditions. Furthermore, a notable proportion of patients (61.1%, 154 out of 252) reported insufficient family income, indicating widespread financial constraints within the patient population (). This high proportion of low-income patients reflects the hospital’s role as a provider of free healthcare services, suggesting that individuals with better financial status often seek treatment at private hospitals or overseas.
The most prevalent symptoms observed among the patients were bleeding (64.6%, 163 out of 252), prolapse (63.5%, 160 out of 252), and pain (63.1%, 159 out of 252). In contrast, swelling was the least reported symptom, accounting for only 1.6% (4 out of 252) of the patients ().
Table 2 symptoms
illustrates that internal hemorrhoids were the most prevalent (52%, 131 out of 252), with third-degree internal hemorrhoids being particularly common (27%, 68 out of 252). Additionally, mixed hemorrhoids, indicating both external and internal involvement, were observed to various degrees, with third-degree involvement being the most prevalent (6.4%, 16 out of 252).
Table 3 Types and Degrees of Hemorrhoids
Patients with first- and second-degree hemorrhoids (48.4%, 122 out of 252) received conservative management procedures. Conversely, patients with third- and fourth-degree hemorrhoids (51.6%, 130 out of 252) underwent operative management.
Discussion
Our findings revealed a male predominance (83.7%) and a high prevalence among individuals with lower socioeconomic status (61.1%). Constipation has emerged as a notable risk factor.
Hemorrhoids are prevalent anorectal conditions that predominantly affect adults.Citation12 Analysis of the age distribution in our dataset indicated that the predominant age group affected by hemorrhoids was young adults, typically between 30 and 40 years of age. These findings are consistent with those of previous studies by Ravindranath et al and Ali et al, who reported that the most common age group affected by hemorrhoids was individuals younger than 40 years of age.Citation13,Citation14 However, this finding contrasts with the findings of studies by Khan et al and Johanson et al.Citation15,Citation16
In our study, the distribution of hemorrhoids by sex indicated a male: female ratio of 5.15:1. Of the total admissions of 252 patients, the majority, comprising 83.7%, were male. This imbalance may be attributed to a greater propensity of men to seek treatment for hemorrhoids, possibly influenced by societal perceptions and the reluctance of women to seek medical consultation for anorectal issues due to feelings of embarrassment. Ravindranath et alCitation9 reported a male predominance of 66.7% compared with 33.3% for females, consistent with Ali et al’sCitation14 observation of a 55% male predominance in their study.
Our study revealed that socioeconomic status significantly influenced patients with hemorrhoids, with the most commonly affected group being those with insufficient family income, accounting for 61.1% of cases. The socioeconomic data from our study must be contextualized considering the hospital’s status as a government facility offering free treatment. This likely results in a higher proportion of low-income patients compared to private hospitals or overseas facilities, where individuals with better financial status might seek treatment. According the study of Forootan et al constipation is more prevalent among people with low-income.Citation17 In the present study, the author also identified constipation as a risk factor, affecting 34.9% of the patients, which aligns with findings from previous research.Citation14–16
Furthermore, research conducted at the Milwaukee VA Medical CenterCitation18 has established diarrhea, rather than constipation, as the primary cause of hemorrhoids. This finding is corroborated by a national study utilizing data from the VA, which identified comorbidities linked to hemorrhoids, all of which are conditions associated with diarrhea, including colitis, malabsorption, intestinal bypass, and chronic pancreatitis, instead of constipation.Citation19 According to a study by Sepanlou SG, Afghanistan exhibits persistently high rates of diarrhea,Citation20 exacerbated by decades of conflict that have hindered efforts to improve public health and led to a significant increase in internally displaced persons. The rapid urbanization and influx of displaced persons into Afghan cities have strained infrastructure, forcing many to reside in slums and underdeveloped areas lacking adequate water and sanitation services, thereby heightening the risk of diarrheal illnesses.Citation21
In our study, a significant proportion of patients diagnosed with hemorrhoids were from Kabul (69.5%), likely due to the hospital’s accessibility to patients residing in this area. Additionally, the majority of patients in this study were unemployed (57.1%), which may be attributed to the high rates of unemployment in Afghanistan, particularly following the collapse of democracy.
The analysis of symptoms observed in patients with hemorrhoids revealed a high prevalence of multiple complaints. Our study identified bleeding (64.6%), prolapse (63.5%), and pain (63.1%) as the most common symptoms, which are consistent with findings reported by Ali et al.Citation14 However, this data contrasts with the findings of Nikooiyan et al, where the most common symptom reported was pruritus (45.8%), followed by discharge (41.6%) and anal pain (22.5%).Citation2 For patients with hemorrhoidal disease (HD) mainly experiencing bleeding, Hemorrhoidal Artery Ligation and Rectoanal Repair (HAL-RAR) is preferred over Milligan-Morgan (MM) hemorrhoidectomy. HAL-RAR targets hemorrhoidal blood supply, effectively reducing bleeding and improving patient satisfaction compared to MM, which involves excisional surgery. HAL-RAR’s non-excisional approach also leads to reduced postoperative discomfort and faster recovery, making it favorable for managing bleeding symptoms in HD.Citation22
While our study provides comprehensive data on the demographics and clinical presentation of hemorrhoid patients, future research should incorporate classification scoring systems to measure the severity of symptoms. This would enhance the scientific rigor and comparability of findings.
In our study, the majority of admitted patients presented with internal hemorrhoids, constituting approximately 52% of the patients. Among these, third- and fourth-degree internal hemorrhoids predominated, necessitating surgical intervention. The high rate of surgical treatment can be attributed to the advanced stages of hemorrhoids observed at the time of presentation, likely resulting from delays in seeking medical care. These delays are often influenced by social, economic, and cultural factors. The need for surgical intervention imposes a considerable demand on hospital resources, including operating room time, surgical staff, and postoperative care facilities.
This pattern is consistent with findings from Malviya et al,Citation22 where third- and fourth-degree internal hemorrhoids were also most prevalent and typically required surgical treatment. Future research should focus on risk factors contributing to late presentation to develop preventive strategies and early diagnosis of hemorrhoids.
The study has several limitations. Firstly, data from the outpatient department was unavailable, which may have resulted in an incomplete understanding of the full spectrum of hemorrhoid cases and their management. Secondly, the study was conducted at a single center, limiting the generalizability of the findings to other settings within Afghanistan or beyond. Lastly, the retrospective design of the study may introduce biases related to the accuracy and completeness of recorded data. However, comprehensive analysis of demographic and clinical factors provides valuable insights into hemorrhoids in Kabul, Afghanistan, providing a foundation for future research.
Conclusion
In conclusion, this study reveals the demographic characteristics and prevalence of hemorrhoids in a tertiary hospital in Kabul, Afghanistan, highlighting a significant prevalence among males (83.7%) and low-income individuals (61.1%). These findings align with global studies in terms of age and sex distribution but differ in the socio-economic context. The higher prevalence among low-income groups in Kabul likely reflects dietary differences, limited healthcare access, and social stigma, leading to delayed medical consultations and more advanced disease stages at presentation.
These unique socio-economic and cultural factors emphasize the need for targeted public health interventions in Afghanistan. Addressing these delays through improved awareness, accessible healthcare services, and early intervention strategies could enhance patient outcomes. Further research is essential to identify additional risk factors and refine these interventions, bridging the gap between existing literature and clinical realities in this region.
Disclosure
The authors report no conflicts of interest in this work.
References
- Marx JA, Hockberger RS, Walls R. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 6th ed. Philadelphia, PA: Elsevier; 2006:1509–1512.
- Nikooiyan P, Sardo HM, Poursaeidi B, Zaherara M, Ahmadi B. Evaluating the safety, efficacy and complications of electrotherapy and its comparison with conventional method of hemorrhoidectomy. Gastroenterol Hepatol Bed Bench. 2016;9(4):259–267.
- Riss S, Weiser FA, Schwameis K, et al. The prevalence of hemorrhoids in adults. Int J Colorect Dis. 2012;27(2):215–220. doi:10.1007/s00384-011-1316-3
- Carter D, Beer Gabel M, Zbar A, Segev S, Kopylov U. Prevalence and clinical associations of hemorrhoids at screening colonoscopy. World J Colorectal Surg. 2013;3(2):10.
- Lee J-H, Kim H-E, Kang J-H, Shin J-Y, Song Y-M. Factors associated with hemorrhoids in Korean adults: Korean national health and nutrition examination survey. Korean J Fam Med. 2014;35(5):227. doi:10.4082/kjfm.2014.35.5.227
- Banov L, Knoepp L, Erdman L, Alia R. Management of hemorrhoidal disease. J South Carolina Med Assoc. 1985;81(7):398–401.
- Jacobs D, Solomon CG; Clinical practice. Hemorrhoids. New Engl J Med. 2014;371(10):944–951. doi:10.1056/NEJMcp1204188
- Rivadeneira DE, Steele SR, Ternent C, Chalasani S, Buie WD, Rafferty JL; Standards Practice Task Force of The American Society of Colon and Rectal Surgeons. Practice parameters for the management of hemorrhoids (revised 2010). Dis Colon Rectum. 2011;54(9):1059–1064. doi:10.1097/DCR.0b013e318225513d
- Altomare DF, Roveran A, Pecorella G, Gaj F, Stortini E. The treatment of hemorrhoids: guidelines of the Italian Society of Colorectal Surgery. Tech Coloproctol. 2006;10(3):181. doi:10.1007/s10151-006-0277-y
- Buntzen S, Christensen P, Khalid A, et al. Diagnosis and treatment of haemorrhoids. Dan Med J. 2013;60(12):B4754.
- Wald A, Bharucha AE, Cosman BC, Whitehead WE. ACG clinical guideline: management of benign anorectal disorders. Off J Am Coll Gastroenterol. 2014;109(8):1141–1157. doi:10.1038/ajg.2014.190
- Ravindranath G, Rahul B. Prevalence and risk factors of hemorrhoids: a study in a semi-urban centre. Inter Surg J. 2018;5(2):496–499. doi:10.18203/2349-2902.isj20180339
- Ali SA, Shoeb MFR. Study of risk factors and clinical features of hemorrhoids. Inter Surg J. 2017;4(6):1936–1939. doi:10.18203/2349-2902.isj20172051
- Khan R, Itrat M, Ansari A, Zulkifle M. A study on associated risk factors of haemorrhoids. J Biol Sci Opinion. 2015;3(1):36–38. doi:10.7897/2321-6328.0318
- Johanson JF, Sonnenberg A. Constipation is not a risk factor for hemorrhoids: a case-control study of potential etiological agents. Am J Gastroenterol. 1994;89(11):1981–1986.
- Forootan M, Bagheri N, Darvishi M. Chronic constipation: a review of literature. Medicine. 2018;97(20):e10631. doi:10.1097/MD.0000000000010631
- Loder P, Kamm M, Nicholls R, Phillips R. Haemorrhoids: pathology, pathophysiology and aetiology. Br J Surg. 1994;81(7):946–954. doi:10.1002/bjs.1800810707
- Delcò F, Sonnenberg A. Associations between hemorrhoids and other diagnoses. Dis Colon Rectum. 1998;41(12):1534–1541; discussion1541–2. doi:10.1007/BF02237302
- Sepanlou SG, Malekzadeh F, Delavari F, et al. Burden of gastrointestinal and liver diseases in Middle East and North Africa: results of Global burden of diseases study from 1990 to 2010. Middle East J Digest Dis. 2015;7(4):201–215.
- Mubarak MY, Wagner AL, Asami M, Carlson BF, Boulton ML. Hygienic practices and diarrheal illness among persons living in at-risk settings in Kabul, Afghanistan: a cross-sectional study. BMC Infect Dis. 2016;16(1):1–9. doi:10.1186/s12879-016-1789-3
- Symeonidis D, Spyridakis M, Zacharoulis D, et al. Milligan–Morgan hemorrhoidectomy vs hemorrhoid artery ligation and recto-anal repair: a comparative study. BMC Surg. 2022;22(1):416. doi:10.1186/s12893-022-01861-z
- Malviya V, Diwan S, Sainia T, Apte A. Demographic study of hemorrhoid with analysis of risk factors. Surg Update Int J Surg Orthopaedics. 2019;5(1):7–13.