
Abstract
Purpose
Asymptomatic cerebral carotid artery stenosis (ACCAS) benefits from secondary prevention via statins and antiplatelets; nonetheless, the impact of medication alone is often limited. Evidence has suggested enhanced therapeutic outcomes when Chinese patent medicine—specifically, compound dilong capsules (CDC)—is integrated with conventional secondary prevention measures.
Patients and Methods
We retrospectively analyzed 319 ACCAS patients from January 2018 to December 2022 at Xuanwu Hospital, Capital Medical University. Depending on the clinical outcomes—improvement or stabilization versus progression—patients were classified into effective or ineffective treatment groups. Patient medical records and questionnaire responses were the primary data sources. The study accounted for demographic variables, clinical history, and medication details, with the primary focus on CDC use and its duration. Treatment outcomes were gauged alongside Transcranial color-coded sonography and Carotid Doppler ultrasonography findings. We employed both univariate and multivariate statistical methods to assess the data.
Results
CDC administration (aOR=2.51, 95% CI 1.39–4.54, P=0.002) and extended usage beyond six months (aOR=3.54, 95% CI 1.71–7.32, P=0.001) demonstrate a statistically significant correlation with treatment efficacy. Gender (aOR=2.54, 95% CI 1.30–5.00, P=0.007), hypertension management (aOR=0.56, 95% CI 0.33–0.95, P=0.031), and antiplatelet therapy with aspirin (aOR=9.53, 95% CI 1.15–78.89, P=0.037) or clopidogrel (aOR=9.97, 95% CI 1.10–90.12, P=0.041) also influenced the therapeutic outcome significantly.
Conclusion
Incorporating CDC as part of a secondary prevention strategy for over six months can beneficially modulate and limit the progression of vascular stenosis in ACCAS. These findings underscore the value of combining traditional Chinese medicine with modern pharmacological interventions in ACCAS management.
Introduction
Stroke remains the leading cause of mortality in China, distinguished by its high rates of recurrence, disability, and death. Estimates from the Centers for Disease Control and Prevention suggest that 10% to 15% of approximately 700,000 new ischemic strokes annually are attributed to thromboembolism from asymptomatic carotid artery stenosis (ACAS).Citation1 Similarly, asymptomatic intracranial atherosclerotic stenosis (AICAS) constitutes a significant etiology of ischemic stroke, incurring an approximate annual incidence rate of 2.8%.Citation2 Early recognition and timely intervention in patients with asymptomatic cerebral carotid artery stenosis (ACCAS), which includes both ACAS and AICAS, are imperative for symptom prevention and stroke incidence reduction.
The current therapeutic strategies for ACAS, which include carotid endarterectomy (CEA) and carotid artery stenting (CAS), have proven efficacy in warding off stroke and preventing the recurrence of severe carotid stenosis over mid to long-term intervals. The 2020 updated German–Austrian clinical guidelines advocate for the consideration of CEA in patients showcasing 60% to 99% stenosis, provided there is no escalated risk associated with surgery.Citation3 Concurrent research from a Chinese trial on carotid artery stenosis revascularization exhibited a preference for avoiding CEA and CAS in asymptomatic individuals.Citation4 The latest studies, moreover, indicate that severe intracranial atherosclerotic stenosis does not benefit from CAS during ongoing medical therapy.Citation5 With the treatment of AICAS, while the intensive modulation of adjustable risk factors and antiplatelet therapy continues to play a secondary preventive role,Citation6 the repertoire of therapeutic modalities is currently limited.Citation7,Citation8 Although combination therapy with lipid-lowering agents may decelerate atherosclerosis progression, exemplified by reductions in plaque and intima-media thickness, it also heightens the prospect of adverse effects. Previous investigations have posited that compound dilong capsules (CDC) have the potential to diminish blood viscosity, amplify intracranial blood flow, and alleviate symptoms of stroke.Citation9
In light of these considerations, our study embarks on a retrospective, non-matched case-control analysis, examining 157 ACCAS patients treated with CDC against 162 controls refraining from CDC application. All subjects had attended Xuanwu Hospital, Capital Medical University, between January 2018 and December 2022. The objective of this research is to discern the influence of CDC on ACCAS treatment outcomes.
Material and Method
Study Population
This retrospective case-control study enrolled patients diagnosed with ACCAS in the outpatient department of Xuanwu Hospital, Capital Medical University, from January 2018 to December 2022. Information was extracted from electronic medical records and questionnaires conducted during outpatient visits. The inclusion criteria were as follows: individuals aged 18 to 80 years; no history of cerebrovascular disease or ischemic events; confirmation of intracranial atherosclerotic stenosis by transcranial color-coded sonography (TCCS); detection of carotid artery stenosis by carotid Doppler ultrasonography (CDU); presence of cerebrovascular risk factors. The exclusion criteria included nonatherosclerotic intracranial stenosis (such as dissection, vasculitis, or moyamoya); history of stroke; CEA or CAS; allergic reactions to any study drug (such as aspirin, statin, CDC); uncontrolled diabetes, hypertension, or familial hypercholesterolemia; Traditional Chinese medicines, proprietary Chinese medicines, and traditional Chinese medicine injections that promote blood circulation and eliminate blood stasis were also excluded.
Drug Administration
The patients diagnosed with ACA received conventional secondary preventive therapy, including (a) aspirin and (b) atorvastatin (if atorvastatin was ineffective, other equivalent statins were chosen). Patients in the case group took two CDC capsules three times daily on the basis of secondary prevention;
The CDC in this study contained Dilong (Pheretima), Chuanxiong (Chuanxiong Rhizoma), Huangqi (Astragali Radix), and Niuxi (Achyranthis Bidentatae Radix) and were produced by Nanjing Hence Pharmaceutical Co., Ltd. (Chinese Medicine Approval No. Z19991007). The quality criteria for herbs comply with the Chinese Pharmacopoeia.
Data Collection
The demographic and clinical characteristics of the patients were collated, including age, gender, BMI, smoking, drinking, dietary habits, exercise habits, hypertension, diabetes, aspirin, clopidogrel, statin, CDC and duration of taking CDC, curative effect including effective (improvement, stable) and ineffective (progression); TCCS, and noninvasive CDU results will be collated.
Typical TCCS and CDU Examination
TCCS and CDU examinations were performed by experienced ultrasound physicians at the Department of Vascular Ultrasonography, Xuanwu Hospital. The examination followed the vascular ultrasound protocol of Zwiebel and PelleritoCitation10 and the guidelines of the Chinese Medical Doctor Association of Ultrasonography.Citation11
TCCS was examined using a Hitachi ultrasound system (Asendarce, Hitachi, Japan). Intracranial arteries, including the terminal internal carotid artery, middle cerebral artery, anterior cerebral artery, posterior cerebral artery, basilar artery, and vertebral artery (intracranial) were detected. Methods of measurement and recording followed the guidelines for vascular Doppler ultrasonography in China. The degree of cerebral artery stenosis was divided into three grades according to the peak systolic flow velocity: mild (140–180 cm/s), moderate (180–220 cm/s), and severe (≥220 cm/s). CDU was examined using Philips ultrasound system (IU-22, Philips, USA) and Hitachi ultrasound system (Ascendus, Hitachi, Japan) to examine the carotid arteries, including the common carotid artery, internal carotid artery, vertebral artery (extracranial), and subclavian arteries. The size and echogenicity of atherosclerotic plaques and the PSV and end-diastolic velocity of the arteries were recorded. According to the NACET arterial stenosis grading method, the degree of stenosis of these arteries was classified as <50%, 50%-69%, 70%-99%, and occlusion.Citation12 The results of TCCS and CDU were compared before and after treatment to determine the degree of stenosis progress or regression, if the degree of stenosis did not change, the artery was classified as stable.
Statistical Analysis
SPSS (version 26.0; SPSS IBM). was used for statistical analysis. Normal distribution quantitative data such as patients’ age and BMI were expressed as mean ± standard deviation and Student’s t-test was used for continuous variables and the chi-squared or Fisher’s exact tests were used for comparison of categorical variables. All tests are two-sided tests, and P values <0.05 are considered statistically significant. Duration of taking CDC was encoded as an ordinal variable from 0 to 1 (< 6, ≥6). Univariate and multivariate logistic regression for analysis was used to determine whether CDC was associated with efficacy. Potential covariates that may affect this associations like hypertension, diabetes, aspirin, clopidogrel, statin and social-demographic data were included in the models. The odds ratio (OR) for efficacy and its 95% confidence interval (95% CI) were used to represent the relative risk. The adjusted odds ratio (aOR) was also calculated.
Result
This study included a total of 319 participants, categorized into two groups based on the effectiveness of treatment outcomes for ACCAS. Comparison of baseline characteristics in case group and control group are presented in . Age, gender, BMI, smoking, drinking, dietary habits, exercise habits, hypertension, diabetes, aspirin, clopidogrel and statin did not differ between case and control groups (p > 0.05). There was a statistically significant difference in CDC and duration of taking CDC between the two groups (p < 0.05). The results of the univariate regression analysis which are presented in are similar to the results of the baseline differences analysis.
Table 1 Differential Analysis of Factors Influencing the Therapeutic Outcomes in Head and Carotid Artery Stenosis (n=319)
Table 2 Logistic Regression Analysis of the Impact of Dichotomous Variables on Head and Carotid Artery Stenosis
A logistic regression equation was constructed by incorporating age, gender, BMI, smoking, drinking, dietary habits, exercise habits, hypertension, diabetes, aspirin, clopidogrel, statins, CDC and the duration of taking CDC. Results of logistic regression analysis are presented in . In addition, the results of the multivariable regression analysis, including CDC and duration of taking CDC are presented in . The results revealed that CDC (aOR=2.51, 95% CI 1.39–4.54, P=0.002), the duration of taking CDC (aOR=3.54, 95% CI 1.71–7.32, P=0.001), gender (aOR=2.54, 95% CI 1.30–0.00, P=0.007), hypertension (aOR=0.56, 95% CI 0.33–0.95, P=0.031), and aspirin (aOR=9.53, 95% CI 1.15–78.89, P=0.037), as well as clopidogrel (aOR=9.97, 95% CI 1.10–90.12, P=0.041), had statistically significant differences in the therapeutic efficacy for ACCAS. Other factors. Including age, BMI, smoking, drinking, dietary habits, exercise habits, diabetes, and statin, showed no statistically significant differences in the therapeutic efficacy for ACCAS. Moreover, the results suggest that secondary prevention and combined treatment could stabilize the vascular stenosis process and reverse part of the stenosis. Combining CDC with treatment can significantly improve the condition of cerebral arterial stenosis. For instance, the case of a patient demonstrated in illustrates this point effectively.
Figure 1 The impact of CDC for efficacy of asymptomatic cerebral carotid artery stenosis. CDC: compound dilong capsules.
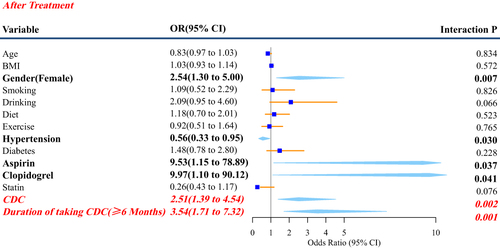
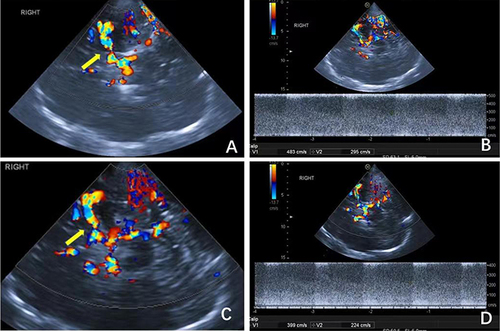
Figure 2 Patient with Asymptomatic cerebral carotid artery stenosis in the Secondary Prevention Combined compound dilong capsules. (A and B) at baseline. (C and D) after treatment. (A) CDFI image showing stenosis of the right MCA (yellow arrow). (B) Color Doppler spectrum showing that the PSV at stenosis increased by 483 cm/s. (C) CDFI image of the same patient after treatment showing that the stenosis of the right MCA improved compared with the baseline (yellow arrow). (D) Color Doppler spectrum of the same patient after treatment showing that the PSV at the stenosis was reduced to 399 cm/s.
Discussion
Our study’s findings suggest that the administration of CDC has a significant independent effect on the treatment of ACCAS, regardless of variables such as age, BMI, gender, smoking habits, alcohol consumption, diet, exercise, and concurrent standard pharmacotherapy with antiplatelets and statins. The extended use of CDC beyond six months correlates with increased effectiveness, substantiating CDC as a potential supplement to secondary prophylaxis for patients with ACCAS. Gender-specific responses indicate that females may exhibit a more pronounced therapeutic benefit, and while the concomitant use of aspirin and clopidogrel also enhances treatment efficacy, the presence of hypertension seems to impede it.
Evidence from prior studies aligns with our observations that CDC can positively influence the clinical manifestation of stroke, enhancing outcomes when used in combination with antithrombotic drugs.Citation12–14 The effectiveness of CDC in mitigating the flow velocities in intracranial stenotic vessels further underscores the compound’s therapeutic potential in cerebrovascular disease management.Citation15 The CDC is believed to work by enhancing cerebral blood flow, decreasing cerebral vascular resistance, and inhibiting platelet adhesion, thereby extending the thrombosis timeframe.Citation16
Additionally, CDC contains ingredients with known pharmacodynamics such as Dilong, which activates blood flow and resolves stasis, and Chuanxiong, which stimulates qi movement and blood circulation—a concept rooted in traditional Chinese medicine.Citation17 Huangqi and Niuxi function synergistically to supplement qi and bolster liver and kidney health, respectively. These pharmacological effects are instrumental in improving the hemorheology of patients with symptoms indicative of qi deficiency and blood stasis. They achieve this by reducing blood viscosity and improving microcirculation, thus supporting the amelioration of lipid metabolism disorders.Citation18
Comparable to atherosclerotic carotid artery disease, AICAS is considered an independent risk factor for impending ischemic strokes in otherwise healthy individuals.Citation19,Citation20 The management of ACCAS is a subject of ongoing debate. The current therapeutic strategies predominantly focus on the management of risk factors, which include the regulation of blood pressure, lipid profiles, and blood sugar levels; engagement in suitable physical activity; adoption of a healthier lifestyle; and cessation of tobacco use. Medical therapy encompasses the use of lipid-lowering agents, antihypertensive agents, and antiplatelet therapy.Citation21,Citation22 Furthermore, in recent years, there has been a notable increase in the application of traditional Chinese medicine, patent Chinese medicine, and other ethnic medicines in treating conditions such as stroke and atherosclerosis. Interventional and surgical treatments, including Carotid Endarterectomy (CEA), are indicated under specific circumstances and necessitate a thorough evaluation that takes into account the patient’s age, gender, the degree of stenosis, the rate of stenosis progression, the characteristics of arterial plaques, the presence of silent emboli or microemboli, and the cerebrovascular reserve capacity.Citation23 This comprehensive approach aims to optimize the patient’s outcomes and ensure the greatest possible benefit. Although CEA and CAS demonstrate effectiveness in stroke prevention, the inherent surgical risks and possibility of non-disabling strokes require careful assessment.Citation24 The current pharmacotherapy focuses on lowering LDL-C levels and delivering anticoagulants.Citation25 While a high dosage of statins, possibly with additional non-statin lipid-lowering agents, may confer benefits, risks of side effects make the pursuit of safer and curative modalities warranted.Citation6,Citation7,Citation25
Despite compelling findings, this study is not without limitations. Being single-centered, limited in sample size, and exhibiting inconsistent follow-up durations diminishes the generalizability of its outcomes. The small sample size precluded meaningful subgroup analysis and assessment of Chinese patent medicines on alternate risk factors. Due to the asymptomatic nature of ACA, patient treatment adherence is a potential issue, as the lack of symptoms may result in reduced vigilance toward the condition. Moreover, ethical considerations prevented the use of CDC as a stand-alone treatment, complicating direct efficacy comparisons with standard secondary prevention measures. Future studies envisioning a multi-centric, larger sample size with rigorous randomized controlled trials are imperative to validate our findings further and establish a more definitive treatment protocol for ACCAS.
Conclusions
In conclusion, we present a clear directive for integrating proprietary Chinese medicines with Western therapeutic practices in ACCAS management. Clinicians can consider CDC as an effective adjunct therapy, potentially elevating prophylactic strategies and enhancing quality of life. This dual-modality approach could pave the way for reducing the global financial burden of stroke management and patient care.
Abbreviations
ACCAS, asymptomatic cerebral carotid artery stenosis; CDC, compound dilong capsules; ACAS, asymptomatic carotid artery stenosis; AICAS, asymptomatic intracranial atherosclerotic stenosis; CEA, carotid endarterectomy CAS, carotid artery stenting; TCCS, transcranial color-coded sonography; CDU, carotid Doppler ultrasonography; OR, odds ratio; 95% CI, 95% confidence interval; aOR: adjusted odds ratio.
Ethics Approval
The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). This study has been reviewed and approved by the Ethics Committee of Xuanwu Hospital, Capital Medical University. (No.2018075)
Consent to Participate
This study is a retrospective study, and according to the regulations of the Ethics Committee of Xuanwu Hospital, Capital Medical University, patient consent to review their medical records is not required. Therefore, this study has been granted a waiver of consent by the Ethics Committee. Furthermore, we assure that the confidentiality of patient data will be strictly observed throughout the research process. All personal information of the patients has been anonymized to ensure that their privacy is not violated.
Consent for Publication
Measures will be implemented to protect patient privacy, and any publication or presentation of the study results will not disclose any information that could potentially identify individual patients.
Disclosure
The authors declare no competing interest in this work.
Acknowledgments
The funder was not involved in the study design, data collection and analysis, or writing of study-related manuscripts.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Additional information
Funding
References
- Farber A. Modern treatment of asymptomatic carotid stenosis-the importance of both medical therapy and carotid endarterectomy. JAMA Surg. 2022;157(8):653–654. doi:10.1001/jamasurg.2022.2081
- Kern R, Steinke W, Daffertshofer M, Prager R, Hennerici M. Stroke recurrences in patients with symptomatic vs asymptomatic middle cerebral artery disease. Neurology. 2005;65(6):859–864. doi:10.1212/01.wnl.0000175983.76110.59
- Eckstein HH, Kühnl A, Berkefeld J, Lawall H, Storck M, Sander D. Diagnosis treatment and follow-up in extracranial carotid stenosis. Dtsch Arztebl Int. 2020;117(47):801–807. doi:10.3238/arztebl.2020.0801
- Yang B, Ma Y, Wang T, et al. Carotid endarterectomy and stenting in a Chinese population: safety outcome of the revascularization of extracranial carotid artery stenosis trial. Transl Stroke Res. 2021;12(2):239–247. doi:10.1007/s12975-020-00835-8
- Gao P, Wang T, Wang D, et al. Effect of stenting plus medical therapy vs medical therapy alone on risk of stroke and death in patients with symptomatic intracranial stenosis: the CASSISS randomized clinical trial. JAMA. 2022;328(6):534–542. doi:10.1001/jama.2022.12000
- Gutierrez J, Turan TN, Hoh BL, Chimowitz MI. Intracranial atherosclerotic stenosis: risk factors, diagnosis, and treatment. Lancet Neurol. 2022;21(4):355–368. doi:10.1016/S1474-4422(21)00376-8
- Daida H, Nohara R, Hata M, et al. Can intensive lipid-lowering therapy improve the carotid intima-media thickness in Japanese subjects under primary prevention for cardiovascular disease?: the JART and JART extension subanalysis. J Atheroscler Thromb. 2014;21(7):739–754. doi:10.5551/jat.19109
- Paraskevas KI, Gloviczki P, Antignani PL, et al. Benefits and drawbacks of statins and non-statin lipid lowering agents in carotid artery disease. Prog Cardiovasc Dis. 2022;73:41–47. doi:10.1016/j.pcad.2022.05.003
- Yao QP. Clinical study of compound Dilong capsule combined with fibrinolytic enzyme in the treatment of acute cerebral infarction. Mod Med Clin. 2021;36(4):4.
- Zwiebel WJ, Pellerito JS. Introduction to Vascular Ultrasonography. Philadelphia: Elsevier Saunders; 2005.
- Chinese Medical Doctor Association U. Guideline of Vascular Ultrasound Examination. Beijing: People’s military medical press; 2011.
- Song XR, Wang LJ. Observation on the curative effect of compound Dilong capsule in the treatment of posterior circulation ischemic vertigo. Zhejiang Clin Med. 2014; 16(10):1627–1628.
- Li SZ. Analysis of treatment of 80 cases of acute cerebral infarction. Chin Pract Med. 2010;5(1):84–85.
- Yu J. Clinical study of compound Dilong capsule in treating acute cerebral infarction. J Clin Emerg Care. 2002;3(5):237–238.
- Guo X, Yan SY, Song JX. Therapeutic effect of compound earthworm capsule combined with antithrombotic drugs on carotid stenosis of qi deficiency and blood stasis type. Chin J Pract Neurol. 2023;26(2):133–138.
- Zhang JL. Lumbrokinase and compound lumbrical capsule. Chin J New Drugs. 2002;11(3):203–205.
- Cao XL, Guan XH, Sun XQ, Li YB. Clinical study of cerebral apoplexy treated by compound earth worm capsule. J Cardiocerebrovasc Dis Integr Med. 2003;1(5):271–273.
- Keyhani S, Cheng EM, Hoggatt KJ, et al. Comparative effectiveness of carotid endarterectomy vs initial medical therapy in patients with asymptomatic carotid stenosis. JAMA Neurol. 2020;77(9):1110–1121. doi:10.1001/jamaneurol.2020.1427
- Bonati LH, Jansen O, de Borst GJ, Brown MM. Management of atherosclerotic extracranial carotid artery stenosis. Lancet Neurol. 2022;21(3):273–283. doi:10.1016/S1474-4422(21)00359-8
- Matsui R, Nakagawa T, Takayoshi H, et al. A prospective study of asymptomatic intracranial atherosclerotic stenosis in neurologically normal volunteers in a Japanese cohort. Front Neurol. 2016;7:39. doi:10.3389/fneur.2016.00039
- Kailash P. Pathophysiology and medical treatment of carotid artery stenosis. Int J Angiol. 2015;24(3):10–1055.
- Mathiesen EB, Joakimsen O, Bønaa KH. Prevalence of and risk factors associated with carotid artery stenosis: the Tromsø Study. Cerebrovasc Dis. 2001;12(1):10–1159. doi:10.1159/000047680
- Mariana C, Luís D, João R, José PA, José F. Management of The Carotid Artery Stenosis in Asymptomatic Patients. Rev Port Cir Cardiotorac Vasc. 2020;27(3):159–166.
- Miao H, Yang Y, Wang H, et al. Intensive lipid-lowering therapy ameliorates asymptomatic intracranial atherosclerosis. Aging Dis. 2019;10(2):258–266. doi:10.14336/AD.2018.0526
- Gong GQ, Qian ZY, Zhou S. The pharmacodynamics of compound lumbrical capsule. Chin New Drugs J. 2001;10(11): 821–823. doi:10.3321/j.issn:1003-3734.200