
Abstract
Background
Atrial fibrillation (AF) is associated with an increased risk of stroke. This study assessed treatment patterns associated with stroke prevention among patients with AF in three major cities of the People’s Republic of China.
Methods
A random sample of 2,862 medical charts for patients with AF at six tertiary hospitals located in Beijing, Shanghai, and Guangzhou between 2003 and 2008 were reviewed. Patient demographics, clinical characteristics, and treatment patterns were extracted from medical charts. Antithrombotic regimens included antiplatelets, anticoagulants, and a combination of both. Descriptive analyses were performed to summarize basic antithrombotic patterns. A logistic regression model examined demographic and clinical factors associated with antithrombotic treatment patterns.
Results
Of the patient sample, 55% were male, the average age was 72 years (49% ≥75 years), 15% had valvular AF, 78% had nonvalvular AF, and the remainder had unspecified AF. CHADS2 scores ≥2 were reported for 53% of patients. Antithrombotic treatment was not received by 17% of patients during hospitalization, and 66% did not receive warfarin. Among patients with valvular or nonvalvular AF, 33%, 30%, and 20% received antiplatelet, anticoagulation, and antiplatelet plus anticoagulation treatments, respectively. For patients with CHADS2 scores of 0, 1, 2, 3, and ≥4, 52%, 42%, 28%, 21%, and 21%, respectively, were treated with warfarin. Predictors of no antithrombotic treatment included age and hospital location.
Conclusion
Anticoagulation therapy was underused in Chinese patients with AF. Antithrombotic treatment was not associated with stroke risk. Further studies need to examine the clinical consequences of various antithrombotic treatment patterns in Chinese patients with AF.
Introduction
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia. This irregular heart rhythm occurs when circuits of disorganized electrical activity in the atria replace the organized electrical activity normally generated by the heart. Age, hypertension, congestive heart failure, valvular disease, and diabetes are known risk factors for the development of AF.Citation1–Citation4 More than 5 million people in the US and over 6 million in Europe are affected.Citation5,Citation6 A large epidemiologic survey conducted in 2002 reported a 0.77% prevalence of AF in the People’s Republic of China, which is close to the 1%–2% prevalence rates reported for the general population in developed regions.Citation6,Citation7
Nearly 18% of all cerebrovascular events in Europe are associated with AF.Citation8 AF increases the risk of ischemic stroke five-fold when compared with normal sinus rhythm.Citation9,Citation10 About one in five strokes is attributed to AF, and the ratio is even higher in the elderly.Citation11 AF-related stroke has become a prominent source of morbidity and mortality and is associated with a high cost of care, so stroke prevention is considered an independent cornerstone strategy for patients with AF. Anticoagulation or antiplatelet therapy has been well documented in both guidelines for stroke prevention and guidelines for the management of AF.Citation6,Citation12
The People’s Republic of China has been following the development of international AF treatment guidelines from the American College of Cardiology/American Heart Association/European Society of Cardiology,Citation13,Citation14 European Society of Cardiology,Citation6 American College of Chest Physicians,Citation15 and American Heart Association/American Stroke Association.Citation16
Central to these guidelines is stratification of stroke risk to balance the risks of bleeding and of thromboembolism. Recently, these guidelines have introduced new antithrombotic alternatives to warfarin that may lower the risk threshold for initiating antithrombotic therapy in patients with AF. In the People’s Republic of China, informal guidelines were published 10 years ago, with an expert consensus issued in 2006.Citation17 AF studies in the People’s Republic of China have indicated a direct correlation between the burden of AF-related stroke and underuse of anticoagulation therapy.Citation7,Citation18 Taking into consideration the findings of recent studies and of the recent AF treatment guideline updates, this study sought to identify and assess treatment patterns associated with stroke prevention in three major cities of the People’s Republic of China in an effort to inform future preventive strategies for AF-related stroke in that country.
Materials and methods
Medical charts recorded for patients hospitalized with a primary diagnosis of AF (International Classification of Diseases, Ninth Revision,Citation19 Clinical Modification, diagnosis code 427.31) at six tertiary hospitals located in three major cities of the People’s Republic of China (Beijing, Shanghai, and Guangzhou) between 2003 and 2008 were used for this study.
All six hospitals had a specific center or cardiology department for AF treatment and were selected based on their willingness to participate in the study. In each hospital, the charts for 480 patients (400 with nonvalvular and 80 with valvular AF) were randomly chosen. A proportional sampling method, based on the annual number of patients with AF at each hospital from 2003 to 2008, was employed so that the 480 patients would adequately represent the distribution of patients with AF by year. Trained physicians and medical students reviewed the medical charts and extracted data using the structured data extraction form, including patient demographics, clinical characteristics, and antithrombotic treatment patterns. Specific variables included age, sex, AF diagnosis, and CHADS2 scoreCitation20 (determined by assigning and adding points for the following conditions: one point each for congestive heart failure, hypertension, age ≥75 years, and diabetes, and two points for prior stroke or transient ischemic attack).Citation20 The CHADS2 score is a clinical predictor of stroke risk in patients with AF and a useful instrument for determining whether or not to initiate anticoagulation therapy.Citation21 In addition to descriptive statistics, a logistic regression model was used to investigate the effect of clinical and demographic factors on antithrombotic treatment patterns.
Independent predictors in the logistic regression model included age, sex, type of AF, CHADS2 score, and city dummies. A two-sided P-value less than 0.05 was considered to be statistically significant. All analyses were performed using Stata version 12 statistical software (Stata Corporation, College Station, TX, USA).
Results
Patient characteristics
Of the 2,862 patient charts reviewed between January 2003 and December 2008, 34% were from Beijing, 33% from Shanghai, and 33% from Guangzhou. Fifty-five percent of the total charts reviewed were for male patients. The average patient age was 72 years (standard deviation 13.3), and nearly one half of all patients (49%) were 75 years or older. Among all patients, 15% had valvular AF, 78% had nonvalvular AF, and 8% had an unidentified type of AF. The mean ages of patients with valvular and nonvalvular AF were 67 and 72 years, respectively. A greater proportion of males had nonvalvular (60%) than valvular (36%) AF. The CHADS2 score was calculated for each of the study patients. Among patients with nonvalvular AF, 53% had a CHADS2 score ≥2. Although not designed for use in valvular AF, when CHADS2 scores were assessed in patients with valvular AF, 45% had a CHADS2 score ≥2. About 36% of the patients in the study were diagnosed with a first episode of AF. Paroxysmal, permanent, and persistent AF accounted for 47%, 33%, and 7% of the patients studied, respectively. In those patients for whom the AF was not a first episode, the median duration of AF was 4.2 years. summarizes the characteristics of the study population.
Table 1 Patient characteristics
Antithrombotic treatment patterns for stroke prevention
displays the distribution of antithrombotic treatment patterns by number of therapy types. Approximately 17% of patients did not receive any antiplatelet or anticoagulation treatment during their hospital stay. For patients with valvular or nonvalvular AF, 42% received one treatment (19% received aspirin, 13% warfarin, 5% clopidogrel, and 4% low molecular weight heparin [LMWH]); 30% received a two-drug regimen (12% received warfarin plus LMWH, 7% aspirin plus clopidogrel, 3% warfarin plus aspirin, 3% aspirin plus LMWH, and 5% other combinations); 9% received a three-drug regimen (4% aspirin plus clopidogrel and LMWH, 2% warfarin plus aspirin and LMWH, 1% warfarin plus aspirin and clopidogrel, 1% warfarin plus clopidogrel and LMWH, and 1% other combinations); and 2% received a four-drug or five-drug regimen. The antithrombotic treatment patterns differed significantly (P=0.000, Fisher’s exact test) between patients with valvular and nonvalvular AF. The proportion of patients receiving a one-drug antithrombotic regimen was much higher among patients with valvular than nonvalvular AF (57% versus 39%, respectively). Further, antithrombotic treatment patterns for the three cities showed a higher proportion of patients with AF not receiving any antithrombotic therapy in Guangzhou than in Beijing or Shanghai. A lower proportion of patients with AF received a one-drug antithrombotic regimen in Beijing than in Shanghai, whereas a higher proportion received at least a two-drug regimen in Beijing than in Guangzhou. In general, significant differences (P=0.000, Pearson’s chi-square test when putting together patterns with two or more types of drugs) in antithrombotic treatment patterns existed among the three cities in the People’s Republic of China.
Table 2 Distribution of antithrombotic treatment patterns
and further depict the distribution of antithrombotic treatment patterns for patients with valvular and nonvalvular AF. Antiplatelet, anticoagulation, and antiplatelet plus anticoagulation therapies were used in 33%, 30%, and 20% of patients, respectively, whereas 17% did not receive any antithrombotic treatment. The combined percentage of patients with valvular AF treated with anticoagulation alone or antiplatelet plus anticoagulation therapy was higher than that of patients with nonvalvular AF (66% versus 48%). The percentages of all patients receiving no antithrombotic regimen, aspirin only, warfarin only or combinations, and other were 17%, 19%, 36%, and 28%, respectively. The four antithrombotic treatment patterns differed significantly between patients with valvular AF and those with nonvalvular AF (P=0.001, Pearson’s chi-square test). A higher percentage of patients with valvular AF were receiving warfarin only or combinations (59% versus 31% for patients with nonvalvular AF), whereas a lower percentage were receiving aspirin only (13% versus 21%, respectively).
Figure 1 Overall treatment patterns for patients with (A) valvular and nonvalvular AF, (B) valvular AF, and (C) nonvalvular AF.
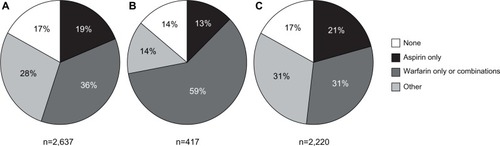
Table 3 Antiplatelet and anticoagulation treatment patterns
Factors associated with antithrombotic treatment
The CHADS2 score is a simple and well validated prediction tool.Citation20 Although recently developed,Citation22,Citation23 the CHADS2 score is commonly used to help elucidate antithrombotic treatment patterns in clinical settings. In this study, 86%, 83%, 81%, 78%, and 85% of patients with AF and CHADS2 scores of 0, 1, 2, 3, and 4 or above, respectively, were treated with any antithrombotic regimen (). No significant difference in the proportion of patients using any antithrombotic treatment was discerned among the CHADS2 score categories of 0, 1, and ≥2 (P=0.067, Fisher’s exact test). However, when patients with an unidentified AF type were excluded, the differences in antithrombotic treatment were significant (P=0.046, Fisher’s exact test). Further, patients with higher CHADS2 scores (≥2) were less likely to receive warfarin or combinations, whereas patients with CHADS2 scores of 0 or 1 were more likely to receive warfarin or combinations ().
Table 4 Patients treated with an antithrombotic regimen, by CHADS2 score
shows the association between stroke risk factors and antithrombotic regimen used under the framework of multivariate regression analysis. The logistic regression model incorporated a dichotomous dependent variable of antithrombotic use and dummy variables for CHADS2 score (0, 1, and ≥2), type of AF (valvular or nonvalvular), sex, age, and city as predictors.
Table 5 Multivariate regression analysis of the association between stroke risk factors and antithrombotic regimen used (n=2,601)
The choice of antithrombotic regimen was not associated with CHADS2 score. Patients ≥75 years of age were significantly less likely than younger patients to receive an anti-thrombotic regimen. Antithrombotic practices in hospitals in Guangzhou and Shanghai differed significantly, although in opposite ways, from those in Beijing. Antithrombotic regimens seemed to be given more consideration in Shanghai than in Beijing or Guangzhou.
Discussion
Cerebral vascular disease has become the leading cause of death in China, accounting for 22.5% of all deaths. Stroke, the cost of which is substantial in all countries,Citation24–Citation27 contributes to a major portion of cerebral vascular deaths.Citation28 Given that approximately 20% of all strokes are attributed to AF, a comprehensive program of stroke prevention must pay close attention to antithrombotic treatments.Citation8,Citation11
Vitamin K antagonists (eg, warfarin) and aspirin are commonly prescribed to prevent stroke in patients with AF. In patients with nonvalvular AF, the risk of stroke is reduced by approximately 20% with aspirin and by approximately 60% with adjustable-dose warfarin.Citation29 However, the risk of bleeding and the difficulty of monitoring and maintaining international normalized ratio (INR) values in the therapeutic range with vitamin K antagonists limit their usefulness. The effects of warfarin on the clotting cascade vary from patient to patient, in part because of individual genetics but also because of the interaction of warfarin with foods, alcohol, and other medications. Concerns over bleeding can lead to undertreatment, causing a measurable increased risk of thrombosis.
Underuse of anticoagulant therapy in patients with AF has been well documented around the world. Studies have shown that nearly one half of patients with AF and additional risk factors for stroke and without contraindications did not receive vitamin K antagonists.Citation30,Citation31 A study in the People’s Republic of China showed that less than 3% of patients with AF received warfarin, and even fewer patients taking warfarin had adequate monitoring of INR. Only 20.1% of patients with AF in the People’s Republic of China take aspirin, which is much lower than rates of aspirin use in the US and Europe.Citation32–Citation34
The current study provides evidence of relatively stable aspirin use (19%) and improved warfarin use (36%) among patients with AF in three major cities of the People’s Republic of China. However, the fact that 17% of patients with both valvular and nonvalvular AF did not receive any antithrombotic regimen underscores the need to further increase use of antithrombotic treatment in these patients. Identified predictors of no treatment included age and hospital location.
The CHADS2 score is an effective predictor of stroke risk, with higher scores indicating increased risk. However, the current study showed that an antithrombotic regimen was not prescribed according to stroke risk based on the CHADS2 score. Further modeling using a multinomial logit model (results not presented) revealed no significant association between CHADS2 score and preference for no antithrombotic treatment, a one-drug antithrombotic regimen, or a multidrug regimen. Further, a CHADS2 score of 2 or above did not associate well with warfarin use. The existing reluctance to use warfarin in clinical practice suggests that the entry of novel oral anticoagulants could replace warfarin.
It is well acknowledged that stroke risk increases with age. An expanded version of the CHADS2 score, ie, the CHA2DS2-VASc score, includes additional stroke risk factors and gives “age 75 years or above” extra weight (with two points).Citation25,Citation35 However, the current study’s logistic regression model did not show age ≥75 years to be a significant predictor of antithrombotic use. The study showed that, in the People’s Republic of China, the elderly (aged ≥75 years) were treated more often with antiplatelet therapy than were younger patients (42% versus 27%, results not presented), whereas the elderly were treated less often with anticoagulation (or antiplatelet plus anticoagulation) therapy than were younger patients (35% versus 59%, results not presented). The result of the logistic regression analysis, ie, that patients 75 years of age or older are less likely to receive antithrombotics, might partly reflect the fact that the CHADS2 score did not accurately predict antithrombotic treatment patterns in the People’s Republic of China (age ≥75 years is a component of CHADS2). That the antithrombotic treatment pattern in China does not follow current clinical practice guidelines warrants further study to determine the reasons why this is so.
The logistic regression model also did not show any significant association between sex and choice of antithrombotic regimen. Although all of the hospitals studied, irrespective of location, preferred use of warfarin in antithrombotic practice, hospitals in Guangzhou were significantly less likely to prescribe an antithrombotic regimen for patients with AF than were hospitals in Shanghai and Beijing. Physicians in the tertiary hospitals selected in Shanghai and Beijing adhered more to international AF treatment guidelines than did those in the selected Guangzhou hospitals.
Several limitations may hinder the generalization of this study’s results. First, treatment patterns for stroke prevention in patients with AF from the six selected tertiary hospitals may not be indicative of such treatment patterns for all patients with AF hospitalized in the People’s Republic of China. Second, this study included hospitalized patients only, and third, retrospective chart reviews such as this study are subject to potential coding errors and unmeasured biases. Finally, many patient and clinical characteristics such as prior history of bleeding or stroke, comorbid conditions, and concomitant medications were not included in this analysis.
In conclusion, antithrombotic treatment is substantially underused in patients with AF in China, particularly in older patients. Varied antithrombotic treatment patterns in the People’s Republic of China could impact current and future antithrombotic treatment strategies. These include a strengthened approach to prescribing antithrombotic treatment by stroke risk, the prospective consideration of warfarin in antithrombotic regimens, and national coordination in adopting standardized antithrombotic practices that could help attenuate hospital costs for stroke in the People’s Republic of China.Citation36
Acknowledgments
Some of the data in this manuscript were previously presented at the American College of Cardiology’s 60th Annual Scientific Session and i2 Summit, New Orleans, LA, April 2–5, 2011. Editorial support was provided by Dana Fox of Caudex Medical, and funded by Bristol-Myers Squibb Company and Pfizer, Inc.
Disclosure
Financial support for this study was provided entirely by Bristol-Myers Squibb Company and Pfizer Inc. The funding agreement helped ensure the authors’ independence in designing the study, interpreting the data, and writing and publishing the report. BL is an employee of Fudan University, which received financial support from Bristol-Myers Squibb and Pfizer in connection with conducting this study and the development of this manuscript. LZL and JX are employees of Pfizer Inc. ML, YL, CD, HC, and XY received financial support from Bristol-Myers Squibb and Pfizer for collection of data for this study but were not paid for manuscript development. The authors report no other conflicts of interest.
References
- AnnéWWillemsRRoskamsTMatrix metalloproteinases and atrial remodeling in patients with mitral valve disease and atrial fibrillationCardiovasc Res200567465565615913581
- SandersPMortonJBKistlerPMVohraJKKalmanJMSparksPBReversal of atrial mechanical dysfunction after cardioversion of atrial fibrillation: implications for the mechanisms of tachycardia-mediated atrial cardiomyopathyCirculation2003108161976198414557372
- VaziriSMLarsonMGLauerMSBenjaminEJLevyDInfluence of blood pressure on left atrial size. The Framingham Heart StudyHypertension1995256115511607768556
- BenjaminEJLevyDVaziriSMD’AgostinoRBBelangerAJWolfPAIndependent risk factors for atrial fibrillation in a population-based cohort. The Framingham Heart StudyJAMA1994271118408448114238
- MiyasakaYBarnesMEGershBJSecular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalenceCirculation2006114211912516818816
- CammAJKirchhofPLipGYEuropean Heart Rhythm AssociationEuropean Association for Cardio-Thoracic SurgeryGuidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC)Europace201012101360142020876603
- ZhouZQHuDYChenJZhangRLiKZhaoXAn epidemiological survey of atrial fibrillation in ChinaChin J Intern Med200443491494 Chinese
- LamassaMDi CarloAPracucciGCharacteristics, outcome, and care of stroke associated with atrial fibrillation in Europe: data from a multicenter multinational hospital-based registry (The European Community Stroke Project)Stroke200132239239811157172
- NarayanSMCainMESmithJMAtrial fibrillationLancet199735090829439509314883
- RyderKMBenjaminEJEpidemiology and significance of atrial fibrillationAm J Cardiol1999849A131R138R
- WolfPAAbbottRDKannelWBAtrial fibrillation as an independent risk factor for stroke: the Framingham StudyStroke19912289839881866765
- GoldsteinLBBushnellCDAdamsRJAmerican Heart Association Stroke CouncilCouncil on Cardiovascular NursingCouncil on Epidemiology and PreventionCouncil for High Blood Pressure ResearchCouncil on Peripheral Vascular DiseaseInterdisciplinary Council on Quality of Care and Outcomes ResearchGuidelines for the primary prevention of stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke AssociationStroke201142251758421127304
- FusterVRydénLEAsingerRWACC/AHA/ESC guidelines for the management of patients with atrial fibrillation: executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines and Policy Conferences (Committee to Develop Guidelines for the Management of Patients With Atrial Fibrillation): developed in collaboration with the North American Society of Pacing and ElectrophysiologyCirculation2001104172118215011673357
- FusterVRydénLECannomDSACC/AHA/ESC 2006 Guidelines for the Management of Patients with Atrial Fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm SocietyCirculation20061147e257e35416908781
- YouJJSingerDEHowardPAAmerican College of Chest PhysiciansAntithrombotic therapy for atrial fibrillation: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice GuidelinesChest2012141Suppl 2e531Se575S22315271
- FurieKLGoldsteinLBAlbersGWAmerican Heart Association Stroke CouncilCouncil on Quality of Care and Outcomes ResearchCouncil on Cardiovascular NursingCouncil on Clinical CardiologyCouncil on Peripheral Vascular DiseaseOral antithrombotic agents for the prevention of stroke in nonvalvular atrial fibrillation: a science advisory for healthcare professionals from the American Heart Association/American Stroke AssociationStroke201243123442345322858728
- XinChenZhangSHuDWorking Group on Atrial Tachyarrhythmias of the Chinese Society of Pacing and ElectrophysiologyCurrent knowledge and management recommendations of atrial fibrillationChin J Card Arrhythm200156994 Chinese
- HuDYSunYHZhouZQRisk factors for stroke in Chinese with non valvular atrial fibrillation: a case-control studyChin J Intern Med200342157161 Chinese
- American Medical AssociationInternational Classification of Diseases, 9th RevisionClinical Modification 2005ChicagoAmerican Medical Association2005
- GageBFWatermanADShannonWBoechlerMRichMWRadfordMJValidation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial FibrillationJAMA2001285222864287011401607
- GageBFvan WalravenCPearceLSelecting patients with atrial fibrillation for anticoagulation: stroke risk stratification in patients taking aspirinCirculation2004110162287229215477396
- KarthikeyanGEikelboomJWThe CHADS2 score for stroke risk stratification in atrial fibrillation – friend or foe?Thromb Haemost20101041454820458437
- LipGYNieuwlaatRPistersRLaneDACrijnsHJRefining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the Euro Heart Survey on Atrial FibrillationChest2010137226327219762550
- TaylorTNDavisPHTornerJCHolmesJMeyerJWJacobsonMFLifetime cost of stroke in the United StatesStroke1996279145914668784113
- DeweyHMThriftAGMihalopoulosCLifetime cost of stroke subtypes in Australia: findings from the North East Melbourne Stroke Incidence Study (NEMESIS)Stroke200334102502250712970517
- GhatnekarOPerssonUGladerELTeréntACost of stroke in Sweden: an incidence estimateInt J Technol Assess Health Care200420337538015446769
- WangYLWuDLiaoXZhangWZhaoXWangYJBurden of stroke in ChinaInt J Stroke20072321121318705946
- ChenZReport of the 3rd National Retrospective Sampling Survey on the Cause of Death in ChinaBeijing, People’s Republic of ChinaPeking Union Medical College Press2008
- HartRGBenaventeOMcBrideRPearceLAAntithrombotic therapy to prevent stroke in patients with atrial fibrillation: a meta-analysisAnn Intern Med1999131749250110507957
- BuckinghamTAHatalaRAnticoagulants for atrial fibrillation: why is the treatment rate so low?Clin Cardiol2002251044745412375802
- HollowellJIs warfarin still underused in patients with atrial fibrillation? A literature reviewCerebrovasc Dis200417Suppl 5125
- GageBFBoechlerMDoggetteALAdverse outcomes and predictors of underuse of antithrombotic therapy in Medicare beneficiaries with chronic atrial fibrillationStroke200031482282710753982
- GoldsteinLBAdamsRAlbertsMJPrimary prevention of ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council: cosponsored by the Atherosclerotic Peripheral Vascular Disease Interdisciplinary Working Group; Cardiovascular Nursing Council; Clinical Cardiology Council; Nutrition, Physical Activity, and Metabolism Council; and the Quality of Care and Outcomes Research Interdisciplinary Working Group: the American Academy of Neurology affirms the value of this guidelineStroke20063761583163316675728
- NieuwlaatRCapucciACammAJEuropean Heart Survey InvestigatorsAtrial fibrillation management: a prospective survey in ESC member countries: the Euro Heart Survey on Atrial FibrillationEur Heart J200526222422243416204266
- LipGYHalperinJLImproving stroke risk stratification in atrial fibrillationAm J Med2010123648448820569748
- WeiJWHeeleyELJanSChinaQUEST InvestigatorsVariations and determinants of hospital costs for acute stroke in ChinaPLoS One201059pii:e13041