Abstract
Introduction
The last decade has seen a growth in the utilization of complementary and alternative medicine therapies, and one of the most popular and sought-after complementary and alternative medicine therapies for nonspecific low back pain is massage. Massage may often be perceived as a safe therapeutic modality without any significant risks or side effects. However, despite its popularity, there continues to be ongoing debate on the effectiveness of massage in treating nonspecific low back pain. With a rapidly evolving research evidence base and access to innovative means of synthesizing evidence, it is time to reinvestigate this issue.
Methods
A systematic, step-by-step approach, underpinned by best practice in reviewing the literature, was utilized as part of the methodology of this umbrella review. A systematic search was conducted in the following databases: Embase, MEDLINE, AMED, ICONDA, Academic Search Premier, Australia/New Zealand Reference Centre, CINAHL, HealthSource, SPORTDiscus, PubMed, The Cochrane Library, Scopus, Web of Knowledge/Web of Science, PsycINFO, and ProQuest Nursing and Allied Health Source, investigating systematic reviews and meta-analyses from January 2000 to December 2012, and restricted to English-language documents. Methodological quality of included reviews was undertaken using the Centre for Evidence Based Medicine critical appraisal tool.
Results
Nine systematic reviews were found. The methodological quality of the systematic reviews varied (from poor to excellent) although, overall, the primary research informing these systematic reviews was generally considered to be weak quality. The findings indicate that massage may be an effective treatment option when compared to placebo and some active treatment options (such as relaxation), especially in the short term. There is conflicting and contradictory findings for the effectiveness of massage therapy for the treatment of nonspecific low back pain when compared against other manual therapies (such as mobilization), standard medical care, and acupuncture.
Conclusion
There is an emerging body of evidence, albeit small, that supports the effectiveness of massage therapy for the treatment of non-specific low back pain in the short term. Due to common methodological flaws in the primary research, which informed the systematic reviews, recommendations arising from this evidence base should be interpreted with caution.
Introduction
Recent times have witnessed dramatic changes to health care. There is now an overt recognition for quality to inform health care practices and this recognition for change has been driven by an increasingly well-informed consumer of health service, the patient, and other stakeholders who strive to underpin their service delivery within the quality health care framework. The key components of this framework include safety, effectiveness, patient centeredness, timeliness, efficiency, and equity.Citation1 Much of the drive towards quality health care has been championed by evidence-based practice, which recognizes the need for health care practices to be underpinned by an integration of research evidence, clinical expertise, and patient values.Citation2
Low back pain is one of the most common musculoskeletal disorders in modern society and is a major reason for health care utilization.Citation3,Citation4 The impact of low back pain is widespread, including physical, social, psychological, and economic aspects of an individual’s life. Low back pain can include discomfort in any area of the spine from the 12th rib to the inferior gluteal fold, and is only considered to be specific if its etiology is known (such as diagnoses of degenerative or other disease, infection, fracture, etc).Citation3–Citation5 Low back pain is usually reported as self-limiting (acute or subacute durations), but it is estimated that approximately 10% of this population will develop chronic pain.Citation3,Citation4,Citation6 However, it has been suggested that this may be an underestimation, with the true number of low back pain sufferers who progress to chronic pain ranging from 16–62% at 6–12 months post injury.Citation7 This imposes a large burden on the health care system.Citation4–Citation8 In spite of a large body of research evidence and a plethora of interventions being available in this area, how best to manage this condition continues to pose a challenge.
The last decade has seen a growth in the utilization of complementary and alternative medicine (CAM) for a variety of health conditions, including musculoskeletal disorders such as nonspecific low back pain.Citation3–Citation9 Awareness in the general public about CAM therapies is growing and their use is becoming increasingly widespread.Citation3,Citation4 The total extrapolated cost in Australia of CAMs and CAM therapists in 2004 was AUD1. 8 billion.Citation9 Common CAM therapies for nonspecific low back pain include acupuncture, massage, and manipulation.Citation4
One of the most popular and sought-after CAM interventions for nonspecific low back pain is massage.Citation4 There are many types of massage, including but not limited to Swedish massage; Thai massage (a form of body work involving assisted stretching); Shiatsu (a Japanese form of massage utilizing finger and palm pressure and stretching techniques); reflexology (the application of pressure to the zones of the feet, hands, or ears, which are thought to correspond to various body parts); and myofascial release (a manual therapy involving deep tissue work). Massage may often be perceived as a safe therapeutic modality without any significant risks or side effectsCitation3 and has been recommended by the Chartered Society of Physiotherapy for the management of various pain-related conditions, especially those of musculoskeletal origin.Citation10 Despite its popularity, there continues to be ongoing debate on the effectiveness of massage in treating nonspecific low back pain. While there is a large body of primary research evidence, such as randomized controlled trials (RCTs), historically, secondary research evidence such as systematic reviews often fail to draw any clear conclusions with which to inform health care practice and policies. With a rapidly evolving research evidence base, and access to innovative means of synthesizing evidence, it is time to reinvestigate this issue.
This systematic review of systematic reviews (umbrella review) sets out to provide a synthesis of the best available research evidence for the effectiveness of massage therapy for adults suffering from nonspecific low back pain. Systematic reviews are considered to be the highest level of evidence for intervention questions.Citation11
Methods
Review question
This review determined the effectiveness of various forms of massage therapy on nonspecific low back pain in adults by answering the question “What is the evidence for the effectiveness of massage therapy in adults with nonspecific low back pain?”
Types of participants
Included participants were adults (≥18 years) suffering from non-specific acute, sub-acute or chronic low back pain (low back pain is defined as pain that is localized from the 12th rib to the inferior gluteal fold).Citation3,Citation4 “Non-specific” means that there is no specific cause of the low back pain such as neoplasms, infection, osteoporosis, arthritic conditions, fracture, radicular syndrome or inflammatory processes.Citation3,Citation12,Citation16
Types of exposure
The treatment of interest in this review was massage therapy. For the purpose of this review, massage is defined as the manual manipulation of the soft tissues of the body for therapeutic purposes.Citation3,Citation5,Citation12
Types of comparators
Comparators included but were not limited to: sham or placebo treatment, medical interventions, physical therapy, electrical therapy (transcutaneous electrical nerve stimulation, ultrasound, etc), pharmaceutical interventions, and other forms of alternative therapy.
Types of outcomes
Outcomes included but were not limited to: patient self-report/subjective change of symptoms, assessment of pain, functional status as measured by validated tools, and assessment of range of motion.
Search strategy
Databases
A systematic search was conducted in the following databases: Embase, MEDLINE, AMED, ICONDA, Academic Search Premier, Australia/New Zealand Reference Centre, CINAHL, HealthSource, SPORTDiscus, PubMed, The Cochrane Library, Scopus, Web of Knowledge/Web of Science, PsycINFO, and ProQuest Nursing and Allied Health Source, investigating systematic reviews and meta-analyses from January 2000 to December 2012, and restricted to English-language documents. The key words used to develop the search terms used can be found in . The appropriate truncation symbols and Boolean operators were used for each database searched and MeSH terms were used where applicable. Two researchers independently conducted the search with cross-checking of random databases to ensure consistency across the search.
Table 1 Concepts searched and the keywords related to these concepts
Pearling
Reference lists of any umbrella reviews returned in this search were also pearled for additional systematic reviews or meta-analyses that may not have been found in the original search.
Selection process
Articles were included if they were systematic reviews or meta-analyses that addressed massage therapy for the treatment of nonspecific low back pain, as defined in this umbrella review. Massage could have been administered in either the treatment or control group, but information regarding massage groups had to be reported separately to any other complementary medicines or placebo treatments administered. Articles that did not meet the PRISMACitation13 definition of a systematic review or meta-analysis were excluded, as were any previous versions of updated systematic reviews. Articles that investigated massage therapy as applied by chiropractors or physiotherapists were also excluded, as these practitioners are not classified as massage therapists and therefore do not fit the criteria for this umbrella review.
Methodological quality assessment
Once relevant publications were identified, two reviewers independently evaluated the methodological quality using the Centre for Evidence Based Medicine (CEBM) critical appraisal tool.Citation14
Data extraction
The data were extracted into a custom-built table based on the CEBM questions. At this point, further exclusions were made based on the full text of the articles.
Results
Search findings
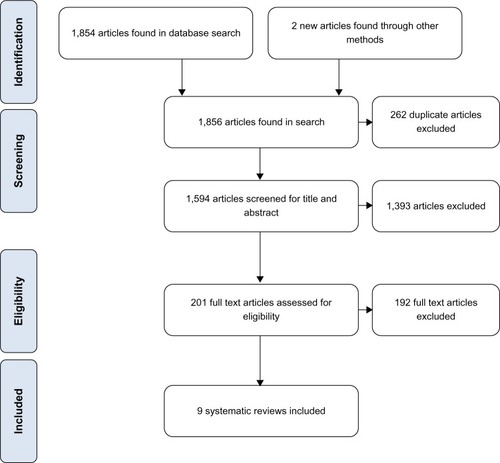
A total of 1,854 articles were returned in the initial search of the abovementioned databases, and two new systematic reviews were found by pearling the reference lists of other umbrella reviews. Of these 1,856 articles, 262 were duplicate articles and 1,393 were removed based on title, abstract, and study descriptors. The full text of the remaining 201 articles was assessed by two independent researchers for relevance, resulting in the exclusion of a further 192 articles that did not match the inclusion criteria. Any disputes were sent to a third researcher for arbitration. The remaining nine systematic reviews were included in this umbrella review. provides an overview of the selection process using the PRISMA flowchart format.Citation13
Figure 1 Flowchart of study selection.
Methodological quality of included reviews
The nine included systematic reviews were critically appraised with the CEBM critical appraisal tool.Citation14 The overall quality scoring of the nine included systematic reviews ranged from poor to excellent. provides an overview of critical appraisal scores for individual reviews.
Table 2 Score of included articles as per the Centre for Evidence Based Medicine review validity appraisal sheetCitation14
The identified systematic reviews classified their findings into three categories of low back pain: acute, chronic, or mixed (where acute and chronic were reported together). In order to maintain standardization and keep true to the research evidence, the following section summarizes the findings based on these three categories.
Category one: the effectiveness of massage therapy for acute/subacute nonspecific low back pain in adults
Furlan et alCitation4 identified ten trials, comprising 1,424 participants, that focused on the effectiveness of massage for low back pain. Of these, two trials were on acute/subacute nonspecific low back pain and included 158 participants. These trials showed significant short-term posttreatment benefits on pain and disability measures after massage when compared to placebo or no treatment. The assessment of methodological quality was only reported overall and the potential bias in massage-specific studies cannot be reported. However, it was reported that, overall (ie, in studies of acupuncture, massage, mobilization, and spinal manipulation), the quality of the studies was poor.
Pengel et alCitation15 identified two high quality RCTs, comprising 164 participants, which compared the use of massage to spinal manipulative therapy and corsets to treat non-specific low back pain. It was reported that spinal manipulative therapy and corsets both improved disability scores in comparison with massage (effect size 1.5, confidence interval [CI]: 0.8,2.2; effect size -0.9 CI -1.6, -0.1) when using the Roland Morris Disability Questionnaire (RMDQ).
Therefore, to summarize this research evidence, it is likely that massage therapy may offer some positive benefits in terms of reduction in pain and disability in the short term, when compared to placebo or no treatment. However, this was not the case when massage therapy was compared with spinal manipulative therapy and corsets.
Category two: the effectiveness of massage therapy for chronic nonspecific low back pain in adults
Bronfort et alCitation16 identified one RCT, comprising 164 participants, which investigated spinal manipulation therapy and various forms of massage therapy for the treatment of chronic low back pain. The findings from this RCT, of low methodological quality (38%), indicated that massage therapy was less effective than spinal manipulative therapy applied by a chiropractor for disability outcomes (statistically significant), but not for pain improvement (statistically nonsignificant).
Ernst et alCitation17 identified two trials, comprising 249 participants, investigating reflexology for chronic low back pain. The authors assessed the methodological quality of the two trials they found using the Jadad scale and found that one of the RCTs was moderate (3/5) and the other was high quality (5/5). Results from both included trials were similar with no significant change found between groups in either trial. While effects were found in one of the two included trials, this was not significant for reflexology in the treatment of low back pain. This systematic review failed to provide evidence that reflexology has benefits beyond that of a placebo effect. Ernst et al state: “In conclusion, the notion that reflexology is an effective treatment option is currently not based on the evidence from independently replicated, high-quality, clinical trials.”Citation17
Furlan et alCitation4 identified ten trials, comprising 1,424 participants, which focused on the efficacy of massage for low back pain. Of these ten trials, eight investigated chronic nonspecific low back pain in 1,266 participants. The evidence indicated that massage was either no different or better than mobilization in terms of immediate and intermediate pain intensity (Short Form-36 pain scale, McGill Pain Questionnaire [two trials]) and disability (two trials), determined using the Oswestry Disability Index and RMDQ. According to two meta-analyses, massage was significantly better in terms of pain reduction (using the visual analog scale [VAS]) in comparison with relaxation and physical therapy (defined by Furlan et alCitation4 as exercise and/or electrotherapy) immediately following treatment, for those with chronic nonspecific low back pain. In terms of the intermediate effect of massage for patients with chronic nonspecific low back pain, there were no significant differences in disability (according to RMDQ) or pain (VAS) when compared with usual care (exercise and advice). Furlan et alCitation4 also found one trial indicating that massage significantly reduced pain intensity and disability in both immediate and long-term follow-ups compared to acupuncture. The assessment of quality was only reported overall; the potential bias in massage-specific studies cannot be reported. However, it was reported that, overall (ie, in studies of acupuncture, massage, mobilization, and spinal manipulation), the quality of the studies was poor.
Kim et alCitation18 identified two RCTs, comprising 275 participants, which reported on the use of acupressure (pressing acupuncture points with a finger or device) for the treatment of chronic low back pain compared to routine physical therapy. Both trials showed significant effects on pain reduction compared to the routine physical therapy. A meta-analysis was conducted for the two RCTs reporting pain intensity posttreatment (4 weeks) and at 6-month follow-up for acupressure versus routine physical therapy for participants with chronic low back pain. This revealed that acupressure was more effective than physical therapy at 4 weeks. The authors state:
… meta-analysis demonstrated acupressure to be superior to physical therapy in terms of pain [N = 275; SMD −0.71; 95 per cent CI −0.96 to −0.47; P < 0.00001; heterogeneity: χ2 = 0.15, P = 0.70, I2 = 0 per cent] after four weeks post-treatment.Citation18
At the 6-month follow-up, acupressure had a significant effect on pain, but the authors report presence of heterogeneity in the data analysis.
van Middelkoop et alCitation19 identified three low-quality RCTs, comprising 163 participants, which indicated that there was no statistically significant reduction in pain when the massage groups were compared with the control groups (relaxation therapy and acupuncture; pooled weighted mean difference was −0.93 [95% CI −8.51] [sic]). They conclude there is insufficient good-quality data with which to come to a firm decision on the efficacy of massage therapy in the treatment of chronic low back pain.
Therefore, to summarize this research evidence, massage therapy may offer some positive benefits in terms of reduction in pain and disability in the short term, when compared to relaxation. However, this was not the case when massage therapy was compared with spinal manipulative therapy. There is equivocal evidence of effectiveness of massage therapy when compared to mobilization and usual care (advice and exercise).
Category three: the effectiveness of massage therapy for mixed acute, subacute, and chronic nonspecific low back pain in adults
Bronfort et alCitation16 identified three RCTs, comprising 197 participants, which investigated spinal manipulation therapy and various forms of massage therapy for the treatment of both acute and chronic low back pain. They found evidence to suggest that spinal manipulative therapy may be more effective in reducing pain (nonsignificant findings) than placebo massage, and a single session of spinal manipulative therapy resulted in fewer sick-leave days than friction massage. The final study found a nonsignificant advantage of spinal manipulation therapy over myofascial therapy for pain and disability reduction. All three studies had low- to moderate-quality scores (13%, 25%, and 63%).
Brosseau et alCitation20 identified eleven trials regarding massage for the treatment of acute, subacute, or chronic non-specific low back pain. However, the authors reported on only four trials, comprising 954 participants, which scored 3 or more on the Jadad scaleCitation21 (high methodological quality). They found statistically significant results in favour of pain reduction in comparison to sham laser treatment but only “clinically important”Citation20 results in decreased disability and symptoms for massage (structural, therapeutic, and relaxation massage) in comparison to usual care and sham laser treatment.
Lewis and JohnsonCitation10 identified seven relevant studies, with a total of 787 participants. These studies were critically appraised using the Centre for Reviews and Dissemination methodological scale.Citation22 The included studies scored between 3 and 7 out of a maximum score of 9. The Centre for Reviews and Dissemination methodological scale was modified to a maximum score of 9 (rather than the original maximum score of 11) by Lewis and Johnson, as they recognized the inability to blind practitioners and clients for this type of intervention (loss of 2 points).Citation10 There was considerable variation between the studies, limiting the ability to compare the findings. Therapeutic massage resulted in better pain and disability scores by end of trial than sham laser, and was found to be superior to self-care, acupuncture, exercise and education, and muscle relaxation. Soft tissue manipulation (six sessions, over a 1-month period) was more effective in terms of reducing disability and pain than exercise with posture education or treatment with sham laser for people with subacute low back pain. Massage (three 30-minute sessions per week for 3 weeks) was better than mental relaxation, while massage (two 30-minute sessions per week for 5 weeks) reduced pain in comparison with standard medical care (pharmacology and chronic pain education). The authors concluded that, as therapeutic massage was superior to comparison groups in only three of seven studies, the effectiveness of massage to relieve low back pain was inconclusive.
Lin et alCitation23 identified one RCT with low risk of bias, comprising 579 participants, which investigated the cost-effectiveness of massage therapy as compared to general practice (GP) health care. This study indicated that massage alone was less effective and more expensive from the health care sector’s perspective than GP care. However, when exercise and behavioral counseling were added to massage, it was more cost-effective than GP care.
Therefore, to summarize this research evidence, massage therapy may offer some positive benefits in terms of reduction in pain and disability in the short term, when compared to sham and placebo interventions. However, this was not the case when massage therapy was compared with spinal manipulative therapy. There is equivocal evidence of effectiveness of massage therapy when compared to acupuncture, exercise and education, and relaxation. There is limited evidence on the cost-effectiveness of massage therapy when compared to other standard interventions for nonspecific low back pain.
Discussion
The aim of this umbrella review was to provide a synthesis and judgment of best available research evidence related to the effectiveness of massage therapy for the treatment of nonspecific low back pain. With increasing consumption of CAM therapies, in an era of evidence-based practice, it is only appropriate to investigate the evidence underpinning the effectiveness of CAM therapies.
The systematic reviews included in this umbrella review ranged from poor methodological qualityCitation10,Citation16 to moderate,Citation18,Citation19 good,Citation4,Citation15,Citation20 or excellent methodological quality.Citation17,Citation23 Therefore, we recommend that caution be used when interpreting the conclusions of these reviews, as the primary research relating to massage and non-specific low back pain, for the most part, had a high risk of bias.
While there are a number of systematic reviews investigating the effectiveness of massage therapy for nonspecific low back pain, there is mixed and conflicting evidence on outcomes from massage therapy. There is emerging evidence that massage may be an effective treatment option for treating low back pain when compared to placebo or sham therapies and other interventions (such as relaxation techniques) in improving short-term pain and disability. The role of massage as a moderately effective nonpharmacological treatment option has also been discussed by Chou et alCitation24 and Imamura et alCitation8 as a recommendation for chronic low back pain therapy.
The evidence is contradictory for the effectiveness of massage when compared to other popular treatment options, such as standard medical care, mobilization, and acupuncture in improving short-term pain and disability. Spinal manipulative therapy seems consistently to provide better outcomes when compared to massage therapy. There was no evidence found for the long-term (beyond 6 months) effectiveness of massage therapy.
The methodology underpinning the primary research, which informed the systematic reviews, was, for the most part, classified as weak. This is a significant issue that has plagued the evidence base for massage therapy and has also been acknowledged by other researchers (Airaksinen et alCitation25). The methodological issues reported by the systematic reviews include small sample size, lack of adequate blinding of assessors, and varied intervention parameters and outcome measures. This is demonstrated by the finding that only one of the nine included systematic reviews was able to undertake a meta-analysis of the included primary literature.Citation18 This was due to the variability in the description of intervention parameters, operational definition of massage therapy, comparators, and outcome measures utilized in the remaining eight included systematic reviews.
The poor quality of the primary research evidence base may be partly due to the conflict between what occurs in clinical practice and rigorous standards required within research settings. In a clinical practice context, massage therapy may often be offered as a “package of care” in addition to advice and education and using a combination of modalities. However, in a research context, a package of care is rarely offered in order to avoid cointervention bias. Therefore, the primary research undertaken may not truly capture and replicate what occurs in a clinical practice context. This is a challenge and a limitation when undertaking and interpreting findings of research evidence for massage therapy.
Limitations of this review
This umbrella review, like any other research, has its limitations, and these need to be acknowledged in the context of the findings. Firstly, while all attempts were made to interrogate and access all relevant literature, it is possible some publications may have been missed in the search process. This is especially relevant for CAM topics, as publications in other languages, originating from countries where English may not be a first language, such as the People’s Republic of China and India, may not be captured in Western databases. Secondly, as there was a lack of clarity around the type, use, and comparators of massage therapy in these systematic reviews, the heterogeneity made it impossible to combine the findings across all included systematic reviews and come to an absolute conclusion. Thirdly, one of the recurrent issues when interpreting these systematic review findings was the imperfect primary research designs included in these reviews. Several of the primary research studies had poor evaluations with several methodological issues (such as lack of adequate descriptions of interventions and poor long-term follow-up).
Conclusion
Implications for practice
The findings of this umbrella review indicate that massage may be an effective treatment option in the short term when compared to placebo and some active treatment options (such as relaxation). However, there are conflicting and contradictory findings for the effectiveness of massage therapy for the treatment of nonspecific low back pain when compared against other manual therapies (such as mobilization, standard medical care, and acupuncture). Given that there were no reported side effects or adverse events as a result of massage therapy, it may be considered as a viable treatment option, provided that cost implications are considered.
The diversity and complexity of the evidence base for the effectiveness of massage therapy for the treatment of nonspecific low back pain underscores the importance of a collaborative, patient-centered decision making process between the patient and the health professional, which is informed by best available evidence. In addition to this, sound clinical reasoning, expertise of individual health professionals, and health outcome data, collected using rigorous outcome measures, should underpin the integration of the findings from this umbrella review into clinical practice. These processes build on the philosophy of evidence-based practice in health care.
Implications for research
Massage therapy seems to be a well-researched field of therapy within CAMs. However, there are key knowledge gaps in the literature that need to be addressed. Further research is required to unpack the “black box” of massage therapy, as there is ambiguity on the operational definition of massage therapy. Various systematic reviews defined and searched for many different types and modalities of massage, with some discussing massage techniques as a separate modality and some considering massage therapy as part of a suite of interventions. This variability extended to massage therapy parameters such as dosage, duration, and intervention protocols. There is a scarcity of data on the cost-effectiveness of massage therapy for the treatment of nonspecific low back pain. As there is currently a dearth of high-quality/low risk of bias primary research on the effectiveness of massage for the treatment of nonspecific low back pain, further research, such as RCTs, with sound methodological rigor, are required. While there are a number of systematic reviews investigating the effectiveness of massage therapy for nonspecific low back pain, the mechanism underlying its action remains elusive. While physiological and psychotherapeutic models have been proposed, the precise mechanism of action continues to be debated, requiring ongoing further research.
Acknowledgments
The authors gratefully acknowledge Ms Khushnum Pastakia for her assistance and feedback during the preparation of this manuscript.
Disclosure
The funding for the conduct of this umbrella review was provided by the Australian Association of Massage Therapists. The authors report no other conflicts of interest in this work.
References
- KohnLTCorriganJMDonaldsonMSTo err is human: building a safer health systemInstitute of Medicine2000 Available from: http://wps.pearsoneducation.nl/wps/media/objects/13902/14236351/H%2007_To%20Err%20Is%20Human.pdfAccessed September 14, 2012
- SackettDLRosenbergWMGrayJAHaynesRBRichardsonWSEvidence based medicine: what it is and what it isn’tBMJ199631271728555924
- FurlanADBrosseauLImamuraMIrvinEMassage for low-back pain: a systematic review within the framework of the Cochrane Collaboration Back Review GroupSpine (Phila PA 1976)2002271896191012221356
- FurlanADYazdiFTsertsvadzeAA systematic review and meta-analysis of efficacy, cost-effectiveness, and safety of selected complementary and alternative medicine for neck and low-back painEvid Based Complement Alternat Med2012201295313922203884
- FurlanAImamuraMDrydenTIrvinEMassage for low back pain: an updated systematic review within the framework of the Cochrane Back Review GroupSpine (Phila Pa 1976)200934161669168419561560
- AnderssonGBEpidemiological features of chronic low-back painLancet199935458158510470716
- HestbaekLLeboeuf-YdeCMannicheCLow back pain: what is the long-term course? A review of studies of general populationsEur Spine J20031214916512709853
- ImamuraMFurlanADDrydenTIrvinEEvidence-informed management of chronic low back pain with massageSpine J20088112113318164460
- MacLennanAHMyersSPTaylorAWThe continuing use of complementary and alternative medicine in South Australia: costs and beliefs in 2004Med J Aust2006184273116398628
- LewisMJohnsonMIThe clinical effectiveness of therapeutic massage for musculoskeletal pain: a systematic reviewPhysiotherapy200692146158
- MerlinTWestonATooherRExtending an evidence hierarchy to include topics other than treatment: revising the Australian ‘levels of evidence’BMC Med Res Methodol2009934
- MoyerCARoundsJHannumJWA meta-analysis of massage therapy researchPsychol Bull200413031814717648
- LiberatiAAltmanDGTetzlaffJThe PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaborationBMJ2009339b270019622552
- Centre for Evidence Based MedicineSystematic Review Critical Appraisal SheetOxfordUniversity of Oxford2005 Available from: http://www.cebm.net/index.aspx?o=1157Accessed November 16, 2012
- PengelHMMaherCGRefshaugeKMSystematic review of conservative interventions for subacute low back painClin Rehabil20021681182012501942
- BronfortGHaasMEvansRLBouterLMEfficacy of spinal manipulation and mobilization for low back pain and neck pain: a systematic review and best evidence synthesisSpine J2004433535615125860
- ErnstEPosadzkiPLeeMSReflexology: an update of a systematic review of randomised clinical trialsMaturitas20116811612021111551
- KimYCLeeMSParkESLewJHLeeBJAcupressure for the treatment of musculoskeletal pain conditions: a systematic reviewJ Musculoskelet Pain201220116121
- van MiddelkoopMRubinsteinSMKuijpersTA systematic review on the effectiveness of physical and rehabilitation interventions for chronic non-specific low back painEur Spine J201120193920640863
- BrosseauLWellsGAPoitrasSOttawa Panel evidence-based clinical practice guidelines on therapeutic massage for low back painJ Bodyw Mov Ther20121642445523036876
- JadadARMooreRACarrollDJenkinsonCReynoldsJMGavaghanDJMcQuayHJAssessing the quality of reports of randomized clinical trials: is blinding necessary?Control Clin Trials1996171128721797
- KhanKSTer RietGGlanvilleJSowdenAJKleijnenJThe NHS Centre for Reviews and Dissemination (CRD)Undertaking systematic reviews of research on effectivenessCRD’s guidance for carrying out or commissioning reviews2nd ed CRD Report No. 4YorkNHS Centre for Reviews and Dissemination, University of York2000
- LinCWHaasMMaherCGMachadoLAvan TulderMWCost-effectiveness of guideline-endorsed treatments for low back pain: a systematic reviewEur Spine J2011201024103821229367
- ChouRQaseemASnowVClinical Efficacy Assessment Subcommittee of the American College of PhysiciansAmerican College of PhysiciansAmerican Pain Society Low Back Pain Guidelines PanelDiagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain SocietyAnn Intern Med2007147747849117909209
- AiraksinenOBroxJICedraschiCCOST B13 Working Group on Guidelines for Chronic Low Back PainChapter 4. European guidelines for the management of chronic nonspecific low back painEur Spine J200615Suppl 2S192S30016550448