
Abstract
Objective
The purpose of this research was to assess the functional brain activity and perceptual rating of innocuous somatic pressure stimulation before and after exercise rehabilitation in patients with chronic pain.
Materials and methods
Eleven chronic pain patients and eight healthy pain-free controls completed 12 weeks of supervised aerobic exercise intervention. Perceptual rating of standardized somatic pressure stimulation (2 kg) on the right anterior mid-thigh and brain responses during functional magnetic resonance imaging (fMRI) were assessed at pre- and postexercise rehabilitation.
Results
There was a significant difference in the perceptual rating of innocuous somatic pressure stimulation between the chronic pain and control groups (P=0.02) but no difference following exercise rehabilitation. Whole brain voxel-wise analysis with correction for multiple comparisons revealed trends for differences in fMRI responses between the chronic pain and control groups in the superior temporal gyrus (chronic pain > control, corrected P=0.30), thalamus, and caudate (control > chronic, corrected P=0.23). Repeated measures of the regions of interest (5 mm radius) for blood oxygen level-dependent signal response revealed trend differences for superior temporal gyrus (P=0.06), thalamus (P=0.04), and caudate (P=0.21). Group-by-time interactions revealed trend differences in the caudate (P=0.10) and superior temporal gyrus (P=0.29).
Conclusion
Augmented perceptual and brain responses to innocuous somatic pressure stimulation were shown in the chronic pain group compared to the control group; however, 12-weeks of exercise rehabilitation did not significantly attenuate these responses.
Introduction
Chronic pain refers to the persistence of pain beyond the period normally associated with healing from illness or initial injury.Citation1,Citation2 The level of mechanical somatic pressure stimulation required to produce pain is lower in patients with chronic pain compared to pain-free participants. Previous research has identified a somatic sensitization in patientsCitation3–Citation6 with chronic pain. Allodynia and hyperalgesia have been identified in several chronic pain conditions.Citation7 A characteristic of central sensitization in chronic pain patients is an enhanced sensitivity to mechanical somatic pressure.Citation8,Citation9
Chronic pain has been associated with dysfunctional descending pain inhibitionCitation10,Citation11 and enhancedCitation12,Citation13 sensitization. Previous research on somatic pressure stimulation in chronic pain patients shows that exercise rehabilitation reduces somatic pressure sensitivityCitation14 and inhibits experimental pain response in patientsCitation15 with chronic pain. The mechanism by which exercise rehabilitation attenuates the sensitivity to somatic pressure is not fully established. However, a plausible basis for the reduced somatic sensitivity in chronic pain following exercise rehabilitation is by a functional restoration of the descending pain-inhibition pathways and/or desensitisation.Citation16 The insular cortex is one brain site that has common connections with cardiovascular and pain-regulatory functions.Citation17,Citation18 Additionally, physical exercise may engage central systems associated with pain inhibition.Citation19 On this basis, exercise rehabilitation may favorably modulate brain responses associated with central sensitization in chronic pain.
Technological advances offer the noninvasive assessment of brain activity in pain research through functional magnetic resonance imaging (fMRI). Previous research has revealed a collection of brain areas that are active during experimental pain stimuli, but not unique to pain.Citation20 Additional areas of the brain may be recruited to enhance or reduce intensity and unpleasantness.Citation21 Functional brain imaging in patients with chronic pain has shown several regions of enhanced activity during somatic pressure pain provocation compared to pain-free controls.Citation22 Prominent brain regions with enhanced neuronal activity include the contralateral primary (S1) and secondary (S2) somatosensory cortices, inferior parietal lobule, cerebellum, and ipsilateral S2 in chronic pain patients.Citation22 The same somatic pressure stimulus resulted in only a single activation in the contralateral S2 in pain-free controls. Additional areas of enhanced brain activity have been observed in the basal ganglia, operculo-insula, inferior parietal cortex,Citation23 and the prefrontal cortex,Citation20 but these may be active depending on the set of circumstances.
Few studies have ascertained functional brain responses during innocuous somatic pressure stimulation in chronic pain.Citation24 In order to further elucidate brain activation in chronic pain, innocuous somatic pressure may reveal brain regions that are active under central sensitization. Areas of enhanced neuronal activity during innocuous stimulation have been previously observed in the medial frontal gyrus, insula, superior temporal gyrus, cerebellum, sensory cortex, and the cingulate.Citation24 Therefore, the purpose of this study was to compare perceptual and functional brain responses to innocuous somatic pressure in patients with chronic pain and pain-free controls. We also examined for mediation of perceptual and brain responses to somatic pressure stimulation during fMRI after 12 weeks of aerobic exercise rehabilitation.
Materials and methods
The participants included eleven patients with chronic pain disorder (nine women and two men) and eight healthy control participants (seven women and one man). Participants with chronic pain included eight subjects with fibromyalgia, two with back pain, and one individual with complex regional pain. Chronic pain patients were diagnosed by a general medical practitioner, rheumatologist, or pain specialist with persistent pain for a period of at least 12 months prior to participating in the study. All participants were screened with a physical activity-readiness questionnaire.Citation25 The exclusion criteria for chronic pain participants were persons with acute inflammatory conditions, acute pain, cancer pain, and inability to perform moderate-intensity aerobic exercise. The healthy control participants were required to be pain-free and have no illness or disease.
The study was conducted with the approval of the University Ethics in Human Research Committee (approval 08/07) and Area Health Ethics in Human Research Committee 2008/5/4.23 (2753). Participants were provided with study information, and signed a letter of informed consent prior to research participation.
All chronic pain patients reported regular use of nonprescription anti-inflammatory and analgesic medications, four reported using prescription opioid-based medicine, and three chronic pain participants were using prescription medication for mild depression. The chronic pain patients maintained their regular medication during the course of the study; however, they abstained from medication for 12 hours prior to functional brain imaging.
Experimental design
The design of the study is a comparative age-matched cross section involving within- (pre- and postexercise intervention) and between- (chronic pain and control)-group analyses. Exercise intervention was performed by both the chronic pain and control participants, and comprised 20 minutes of supervised aerobic exercise twice per week over 12 weeks. The body mass index (BMI), health status (Short Form [36] Health Survey [SF-36] total),Citation26 and pain appraisal (McGill Pain Questionnaire [MPQ] total score)Citation27 were assessed prior to the exercise rehabilitation program. Exercise modalities included aerobic activity of treadmill walking or stationary cycling. Cardiovascular fitness was assessed before and after aerobic rehabilitation by heart-rate (HR) response to a standard submaximal exercise power output (HR/W).
Functional magnetic resonance imaging acquisition
Participants were imaged on a 3T GE Signa Excite MRI scanner (GE Healthcare, Little Chalfont, UK) with an eight-channel MRI Devices (Waukesha, WI, USA) head coil. The fMRI utilized a single-shot echo planar imaging sequence (TR-3000 ms, TE-35 ms, 24 cm field of view, 4 mm slices, 39 slices, 128× 128 matrix). The fMRI procedure was a block-design paradigm consisting of five rest and five stimulus periods of 30 seconds each. Coronal 3-D spoiled gradient-echo and T2 axial datasets were also acquired for structural brain information. Imaging was performed within 2 weeks prior to aerobic exercise rehabilitation and within 1 week after aerobic exercise rehabilitation.
Mechanical somatic pressure stimulation
Somatic pressure stimulation was applied during the fMRI procedure. The somatic pressure consisted of a 2 kg mass with a flat surface-contact diameter of 2 cm positioned on the anterior surface of the right mid-thigh. This location was marked at the midpoint between the superior aspect of the patella and mid-inguinal fold. The pressure stimulus at this site elicited a dull compression of the tissues between the superior surface of the thigh and femur. Participants were requested to rate the somatic pressure sensation on the mid-thigh using a 0–10 sensory category-ratio scaleCitation28 immediately following the fMRI scanning procedure. The numerical anchors and verbal descriptors were graded as 0= no sensation, 2= slight sensation, 4= moderate sensation, 6= pain sensation, 8= strong pain sensation, and 10= pain tolerance. Prior to each fMRI scanning procedure, participants were familiarized with the numerical anchors and descriptors of the sensory scale.
Image processing and analysis
Images were processed using MatLab version 7.11 (MathWorks, Natick, MA, USA) and Statistical Parametric Mapping (SPM)-8 software (Wellcome Trust Centre for Neuroimaging, London, UK). Data preprocessing consisted of motion correction using realignment, normalizing to standard Montreal Neurological Institute space, and smoothing using an 8 mm Gaussian kernel. Data were filtered using a high-pass filter (cutoff period of 128 seconds).
Preprocessed images for individual participants were then analyzed in a first-level fixed-effects analysis using a canonical hemodynamic response-convolved box-car function to model the blood oxygen-dependent (BOLD) response during stimulus. A contrast image of stimulus versus rest was derived for each participant at each time point.
Whole-brain analysis was performed by repeated-measures analysis of variance (ANOVA) within the SPM8 General Linear Model framework with group (chronic pain and control) as the between-subjects factor and time point (before and after) as the within-subjects factor. Error correction (false-discovery rate) for multiple comparisons using a height threshold of P<0.05 was performed. Spatial coordinates from the obtained maps were ascertained hierarchically to the nearest gray matter in Talairach space.Citation29 Sites showing significant or trends for main group effects (chronic pain versus control) in the whole-brain analysis were further assessed by a region of interest (ROI) approach. BOLD signal change for each ROI was extracted from individual participant data at pre and post-aerobic exercise rehabilitation using a MarsBaR (MARSeille Boîte À Région d’Intérêt) toolbox.Citation30 The ROIs comprised 5 mm radii around the peak-cluster coordinates, as identified in whole-brain analysis.
Statistical analysis
Repeated-measures ANOVA was performed for the somatic pressure rating, aerobic fitness (HR/W), and the BOLD signal change in the ROIs. Group comparisons were performed for SF-36 total health score and BMI.
Results
Group characteristics
Characteristics including BMI, MPQ pain score, SF-36 total health status for the chronic pain and control groups (mean ± standard deviation [SD]) are shown in . Group comparisons between the chronic pain and control groups revealed a significant difference for BMI (P<0.01) and for SF-36 total health status (P<0.001). Repeated measures showed a significant difference in HR/W between groups (P=0.05), and there was a significant improvement in aerobic fitness (HR/W) for the chronic pain and control groups following exercise rehabilitation (P<0.001).
Table 1 Group characteristics prior to aerobic exercise rehabilitation
Perceptual responses to somatic pressure stimulation during fMRI
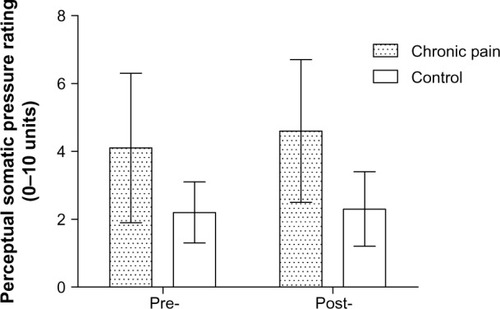
The perceptual rating of a standard 2 kg weight on the right mid-thigh was assessed to confirm somatic pressure hypersensitivity in the chronic pain group. The mean perceptual ratings (sensory scale units ± SD) to the somatic pressure stimulus during the fMRI scanning procedure for the chronic pain and control groups at pre- and post-aerobic exercise rehabilitation are shown in . The chronic pain group revealed a 46% elevated perceptual rating compared to the control group during fMRI to the somatic pressure stimulus at pre-aerobic exercise rehabilitation, and 50% higher perceptual rating at post-aerobic exercise rehabilitation. Results for repeated-measures ANOVA revealed a significant difference between chronic pain and control groups for the perceptual rating of the somatic pressure stimulus (P=0.01), but no group-by-time interaction.
Figure 1 Mean (± standard deviation) perceptual rating (0–10 units) of somatic pressure stimulation during functional brain imaging for chronic pain and control groups at pre- and post-aerobic exercise rehabilitation.
fMRI whole-brain analysis
Whole-brain voxel-wise analyses for between groups (chronic pain and control) are shown in . The associated images are shown in . None of these tests survived multiple comparisons for the whole brain (threshold P<0.05); however, we have listed sites showing trends between the chronic pain and control groups. We report these findings as preliminary results given the small sample size.
Figure 2 Brain regions showing enhanced neuronal responses to innocuous somatic pressure stimulation between the chronic pain group and the control group.
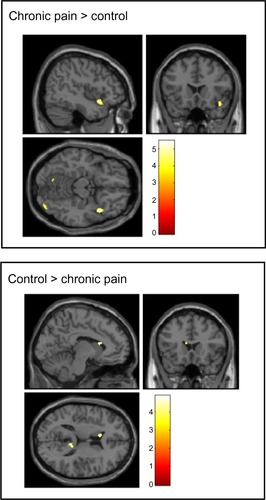
Table 2 Whole-brain voxel-wise analysis, showing sites for elevated trends between the chronic pain and control groups
BOLD signal changes in the regions of interest (pre- versus postexercise rehabilitation)
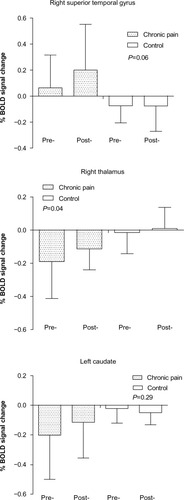
The BOLD signal change in the ROIs for the chronic pain and control groups at pre- and postexercise (± SD) are shown in . Repeated-measures ANOVA showed a significant difference between groups (P=0.04). Group comparisons for the ROIs revealed trend differences in the superior temporal gyrus (P=0.06), thalamus (P=0.04), and caudate (P=0.21). Contrasts for time revealed some trend differences in the superior temporal gyrus (P=0.29), thalamus (P=0.12), and caudate (P=0.37). Trends for group-by-time interaction within the ROIs were seen in the caudate (P=0.10) and superior temporal gyrus (P=0.29).
Figure 3 Percentage blood oxygen level-dependent (BOLD) signal changes (means ± standard deviation) between chronic pain patients and controls within the right superior temporal gyrus, thalamus, and caudate at pre- and post-aerobic exercise rehabilitation.
Discussion
The present study hypothesized that aerobic exercise rehabilitation would reduce the perceptual rating and brain responses to mechanical somatic pressure stimulation (reduced central sensitization) in the chronic pain group. Following the exercise rehabilitation program, both groups showed enhanced cardiovascular fitness. However, the perceptual rating of the somatic pressure in the chronic pain group was not statistically different after the aerobic exercise rehabilitation. The main findings in the fMRI results show differences in brain responses between the chronic pain and control groups during innocuous somatic pressure stimulation in the right superior temporal gyrus, right thalamus, and left caudate ( and ).
Perceptual rating of innocuous somatic pressure stimulation
Previous research shows that the perceptual rating of somatic pressure stimulation is elevated in patients with chronic pain compared to pain-free control participants.Citation23 In the present results, enhanced perceptual rating of the innocuous somatic pressure () indicated somatosensory augmentation and central sensitization in the chronic pain group. The mechanism underlying central sensitization in chronic pain may be associated with enhanced activity from low-threshold cutaneous mechanoreceptive fibers.Citation5 Additionally, previous research has revealed a relationship between increased body-weight status and enhanced pain sensitivity in chronic pain patients.Citation31,Citation32 Results in the present study showed a significant difference in BMI between the chronic pain group and control group, and this may have contributed to the elevated perceptual rating of the innocuous somatosensory stimulus. The mechanism underlying the relationship between body-weight status and pain sensitivity in chronic pain patients has not been fully elucidated, although increased proinflammatory markers in overweight patients may be associated with enhanced pain sensitivity.Citation33
Previous studies have shown a reduction in the perceptual rating of noxious mechanical somatic pressure in chronic pain patients following exercise rehabilitation.Citation14 The present study investigated the effects of innocuous somatic pressure ratings following exercise rehabilitation. However, the perceptual rating of the innocuous somatic pressure in the present study did not reveal a reduced perceptual response. One possible explanation for this outcome is that the exercise rehabilitation period was not sufficient to develop significant changes in central sensitization. Further research could increase the intervention period and monitor changes in somatic pressure sensation and brain responses during exercise rehabilitation within a larger sample of chronic pain patients.
Superior temporal gyrus
Brain regions that revealed differences between the groups included the right superior temporal gyrus, left caudate, and the right thalamus (). Notably, neuronal activity from the somatosensory area was not prominent in the chronic pain group. This suggests that differences in brain responses during the innocuous somatic pressure were more associated with activity in regions not involved in somatosensory processing, but with regions involved with anticipation and emotion. A prominent brain region involved in anticipation is the entorhinal complex,Citation34 which includes neuronal areas in the medial temporal lobe.Citation35 Previous research has shown direct projections between the superior temporal gyrus and the entorhinal cortex.Citation36 The superior temporal gyrus featured prominently in the present results in the chronic pain group, and this has previously been observed in chronic pain patients.Citation24 From this, the increased anticipation and activity from the superior temporal gyrus during the mechanical somatic pressure stimulation partially explains the elevated perceptual ratings in the chronic pain group compared to the control group. However, the response of the superior temporal gyrus was not attenuated following the aerobic exercise rehabilitation. Previous experimental pain studies have shown that anxiety-related increases in perceived pain are associated with activation in the entorhinal cortex of the hippocampus.Citation35 Therefore, the increased activity in the superior temporal gyrus in the chronic pain group at the postexercise-rehabilitation period may have been associated with enhanced anticipation during the innocuous stimulation procedure.
Thalamus
The present results showed a significant difference in the BOLD signal within the thalamus in the chronic pain group compared to the control group (). Enhanced thalamic activity has been shown in pain-free healthy participants compared to patients with chronic pain during noxious stimulation.Citation24 Moreover, regional blood flowCitation37,Citation38 and neuronal activityCitation10 in the thalamus has been shown to be reduced in chronic pain patients compared to controls. It has previously been suggested that thalamic response is inhibited in chronic pain due to a functional plasticity from persistent pain signaling. This is supported by research showing that reduced thalamic activity was enhanced following analgesic treatment in chronic pain patients.Citation39
Caudate
The present results revealed that neuronal activity in the caudate was reduced in the chronic pain group compared to the control group ( and ). In accord with this, previous research has shown that regional blood-flow activity in the caudate is reduced in chronic pain participants compared to controls.Citation38 Enhanced activity in the caudate has previously been observed in healthy controls compared to chronic pain participants,Citation24 although this difference was not observed in another study using cerebral blood-flow analysis.Citation37 In previous pain research, activation in the caudate suggested that this may be a likely source for pain inhibition.Citation40 The suppression of the feeling of pain has also been shown by activation of the caudate.Citation41 The present results showed some improvement in caudate response following exercise rehabilitation in the chronic pain group, although this was not statistically significant. Therefore, the present findings suggest a functional abnormality in the caudate during innocuous somatic pressure stimulation in patients with chronic pain.
Study limitations
Limitations in the present study include the small sample and the degree of variance in the duration of persistent pain in the patient group. Previous research has shown that persistent pain is associated with neurodegenerative changes, and that this corresponds with the duration of chronic pain.Citation42 The present study included patients with a duration of chronic pain of greater than 1 year. This may have provided a heterogeneous sample and influenced the effects of exercise rehabilitation. It is possible that the chronic pain patients may have had progressive neurodegenerative changes within the duration of the study. Also, the intervention period may not have been sufficient to substantially mediate brain responses in the chronic pain group, although there was some trend shown in the caudate. Pain medication could alter brain responses, although none of the chronic pain patients reported substantial changes during the study and prior to the brain-scanning procedure. Future studies could provide a more homogeneous duration of chronic pain patients and extend the exercise-intervention period.
Affective and cognitive factors, such as attention, anxiety, and anticipation, may mediate the perception of somatosensation. Within the present study, the influence of central factors, such as emotion and cognitive components, was not assessed. In one study, anxiety and depression were cofactored among participants, and this revealed that cognitive and affective factors during the anticipation of pain played an important role in pain processing.Citation4 It has been suggested that attentional mechanisms, such as hypervigilance, may influence the evoked cerebral response in structures similar to those observed in the present study.Citation24
Conclusion
The present study showed that innocuous somatic pressure stimulation in the chronic pain patients revealed elevated perceptual ratings and enhanced brain activity compared to the pain-free control group. Innocuous somatic pressure stimulation resulted in differences in brain responses within the superior temporal gyrus, thalamus, and caudate. Exercise rehabilitation did not reveal a significant reduction in the perceptual rating to innocuous stimulation in the chronic pain group; however, there was some trend toward improved BOLD-signal response in the caudate. In contrast, there was an enhanced response in the superior temporal gyrus within the chronic pain group, which may have been associated with increased anticipation. These observations of augmented perceptual and brain responses lead toward further understanding of the consequences of chronic pain and the effects of exercise rehabilitation.
Acknowledgments
We wish to thank Dr Lavier Gomes, Mrs Megan Cromer, and Mr Arthur Escalona at Westmead Hospital Radiology, Sydney, for assistance with fMRI data collection. Also, thanks to Mr Gary McKenzie for systems support in the Spatial Analysis Unit, Charles Sturt University. We also wish to recognize the Charles Sturt University write-up award scheme for this manuscript development.
Disclosure
The authors report no conflicts of interest in this work.
References
- MerskeyHBogdukNClassification of Chronic Pain2nd edSeattleIASP1994
- SiddallPJCousinsMJPersistent pain as a disease entity: implications for clinical managementAnesth Analg200499251052015271732
- Graven-NielsenTArendt-NielsenLAssessment of mechanisms in localized and widespread musculoskeletal painNat Rev Rheumatol201061059960620664523
- BurgmerMPogatzki-ZahnEGaubitzMWessoleckEHeuftGPfleidererBAltered brain activity during pain processing in fibromyalgiaNeuroimage200944250250818848998
- WoolfCJCentral sensitization: implications for the diagnosis and treatment of painPain2011152Suppl 3S2S1520961685
- LatremoliereAWoolfCJCentral sensitization: a generator of pain hypersensitivity by central neural plasticityJ Pain200910989592619712899
- VierckCJJrMechanisms underlying development of spatially distributed chronic pain (fibromyalgia)Pain2006124324226316842915
- ClauwDJWilliamsDLauermanWPain sensitivity as a correlate of clinical status in individuals with chronic low back painSpine (Phila Pa 1976)199924192035204110528381
- KosekEEkholmJHanssonPSensory dysfunction in fibromyalgia patients with implications for pathogenic mechanismsPain1996682–33753839121827
- JensenKBKosekEPetzkeFEvidence of dysfunctional pain inhibition in fibromyalgia reflected in rACC during provoked painPain20091441–29510019410366
- HendersonLAPeckCCPetersenETChronic pain: lost inhibition?J Neurosci201333177574758223616562
- BingelUTraceyIImaging CNS modulation of pain in humansPhysiology (Bethesda)20082337138019074744
- PorrecaFOssipovMHGebhartGFChronic pain and medullary descending facilitationTrends Neurosci200225631932512086751
- Carbonell-BaezaAAparicioVAOrtegaFBDoes a 3-month multidisciplinary intervention improve pain, body composition and physical fitness in women with fibromyalgia?Br J Sports Med201045151189119520542976
- RichardsSCScottDLPrescribed exercise in people with fibromyalgia: parallel group randomised controlled trialBr Med J2002325735718512142304
- NaugleKMRileyJL3rdSelf-reported physical activity predicts pain inhibitory and facilitatory functionMed Sci Sports Exerc201446362262923899890
- BruehlSChungOYInteractions between the cardiovascular and pain regulatory systems: an updated review of mechanisms and possible alterations in chronic painNeurosci Biobehav Rev200428439541415341037
- RandichAMaixnerWInteractions between cardiovascular and pain regulatory systemsNeurosci Biobehav Rev1984833433676095151
- OlaussonBErikssonEEllmarkerLRydenhagBShyuBCAnderssonSAEffects of naloxone on dental pain threshold following muscle exercise and low frequency transcutaneous nerve stimulation: a comparative study in manActa Physiol Scand198612622993053486546
- LeeMCTraceyIUnravelling the mystery of pain, suffering, and relief with brain imagingCurr Pain Headache Rep201014212413120425201
- TraceyIMantyhPWThe cerebral signature for pain perception and its modulationNeuron200755337739117678852
- GieseckeTGracelyRHGrantMAEvidence of augmented central pain processing in idiopathic chronic low back painArthritis Rheum200450261362314872506
- PujolJLópez-SolàMOrtizHMapping brain response to pain in fibromyalgia patients using temporal analysis of FMRIPLoS One200944e522419381292
- GracelyRHPetzkeFWolfJMClauwDJFunctional magnetic resonance imaging evidence of augmented pain processing in fibromyalgiaArthritis Rheum20024651333134312115241
- Canadian Society for Exercise PhysiologyPAR-Q forms Available from: http://www.csep.ca/english/view.asp?x=698Accessed June 30, 2014
- JenkinsonCCoulterAWrightLShort form 36 (SF36) health survey questionnaire: normative data for adults of working ageBMJ19933066890143714408518639
- MelzackRThe McGill pain questionnaire: from description to measurementAnesthesiology2005103119920215983473
- MicalosPSDrinkwaterEJCannonJArendt-NielsenLMarinoFEReliability of the nociceptive flexor reflex (RIII) threshold and association with pain thresholdEur J Appl Physiol20091051556218818941
- LancasterJLWoldorffMGParsonsLMAutomated Talairach atlas labels for functional brain mappingHum Brain Mapp200010312013110912591
- BrettMAntonJValabregueRPolineJRegion of interest analysis using an SPM toolboxNeuroimage2002162497
- OkifujiADonaldsonGWBarckLFinePGRelationship between fibromyalgia and obesity in pain, function, mood, and sleepJ Pain201011121329133720542742
- Carbonell-BaezaAAparicioVASjöströmMRuizJRDelgado-FernándezMPain and functional capacity in female fibromyalgia patientsPain Med201112111667167521939495
- OkifujiABradshawDOlsonCEvaluating obesity in fibromyalgia: neuroendocrine biomarkers, symptoms, and functionsClin Rheumatol200928447547819172342
- FairhurstMWiechKDunckleyPTraceyIAnticipatory brainstem activity predicts neural processing of pain in humansPain20071281–210111017070996
- PloghausANarainCBeckmannCFExacerbation of pain by anxiety is associated with activity in a hippocampal networkJ Neurosci200121249896990311739597
- AmaralDGInsaustiRCowanWMEvidence for a direct projection from the superior temporal gyrus to the entorhinal cortex in the monkeyBrain Res198327522632776194854
- KwiatekRBarndenLTedmanRRegional cerebral blood flow in fibromyalgia: single-photon-emission computed tomography evidence of reduction in the pontine tegmentum and thalamiArthritis Rheum200043122823283311145042
- MountzJMBradleyLAModellJGFibromyalgia in women. Abnormalities of regional cerebral blood flow in the thalamus and the caudate nucleus are associated with low pain threshold levelsArthritis Rheum19953879269387612042
- HsiehJCBelfrageMStone-ElanderSHanssonPIngvarMCentral representation of chronic ongoing neuropathic pain studied by positron emission tomographyPain19956322252368628589
- WunderlichAPKlugRStuberGLandwehrmeyerBWeberFFreundWCaudate nucleus and insular activation during a pain suppression paradigm comparing thermal and electrical stimulationOpen Neuroimag J201151821643502
- FreundWKlugRWeberFStuberGSchmitzBWunderlichAPPerception and suppression of thermally induced pain: a fMRI studySomatosens Mot Res200926111019283551
- ApkarianAVSosaYSontySChronic back pain is associated with decreased prefrontal and thalamic gray matter densityJ Neurosci20042446104101041515548656