
Abstract
Migraine is a commonly occurring, chronic disorder that can cause significant disability. Eletriptan, a selective serotonin 5-hydroxytryptamine 1 receptor subtype B/D (5-HT1B/1D) agonist, is a clinically effective treatment for moderate to severe migraine. The objective of this literature review was to summarize the available data on the pharmacoeconomics of eletriptan relative to other triptans. Articles meeting the following three criteria were included in the review: 1) contained pharmacoeconomic data on a marketed dose of eletriptan; 2) included data on at least one other comparator triptan; and 3) was in English. A MEDLINE® search yielded a total of eight studies (from the European Union [n=5] and from the USA [n=3]) across multiple regions. Seven of the studies examined the pharmacoeconomics of eletriptan relative to other triptans, and a further study examined the health care costs of eletriptan 40 mg versus sumatriptan 100 mg. Eletriptan 40 mg was among a group of triptans, including rizatriptan 10 mg and almotriptan 12.5 mg, demonstrating the greatest cost-effectiveness. This result held across different definitions of efficacy (2 hours pain-free, sustained pain-free, and sustained pain-free with no adverse events) and also held when cost-effectiveness models accounted for second doses and use of rescue medication, management of adverse events, and productivity loss, in addition to drug acquisition costs. Only limited head-to-head comparator data were available. The majority of pharmacoeconomic studies utilized the same set of efficacy and/or tolerability data, and indirect costs were rarely included despite the fact that the majority of per capita migraine costs are attributable to indirect costs. In summary, although the market is now dominated by generics, eletriptan 40 mg is among the most clinically and cost-effective oral triptans available for the management of acute migraine. Increased effectiveness/efficacy of eletriptan may necessitate a lesser need for other migraine treatments and/or switching to other triptans.
Introduction
Acute migraine is a commonly occurring chronic, idiopathic headache disorder that is characterized by moderate to severe headache pain that is usually unilateral and throbbing.Citation1 Migraine pain can be exacerbated by physical activity and is often accompanied by other symptoms, including nausea, vomiting, and sensitivity to light (photophobia) and sound (phonophobia).Citation1 The typical duration of an attack ranges from 4–72 hours (median, 18 hours).Citation1 In approximately 10%–20% of patients, the onset of headache pain is preceded by transient focal neurological symptoms, most commonly visual disturbances, referred to as aura.Citation1–Citation3 Median migraine attack frequency is once a month, but at least 25% of patients report three or more headache days per month.Citation4 Furthermore, migraine can cause notable disability in some sufferers and is a major cause of workplace absenteeism and/or decreased productivity among workers.Citation5,Citation6
Migraine occurs more commonly in women than men.Citation4 For example, in the USA, migraine is estimated to have a lifetime prevalence of approximately 18% in females and 6% in males. Migraine markedly reduces work productivity, with 24% of sufferers missing at least a day of work every 3 months, and 45% having at least a day of reduced productivity every 3 months.Citation2,Citation7 Migraine attacks represent approximately 3% of all emergency department visits in the USA.Citation8
Triptans are usually the preferred treatment for moderate to severe migraine attacks or mild to moderate attacks not responding to analgesics or anti-inflammatory drugs.Citation9 They are potent selective serotonin 5-HT1B/1D receptor agonists. Although, the mechanism of action of triptans has not yet been established, they are hypothesized to work by various mechanisms, including vasoconstriction, inhibition of release of nociceptive neuropeptides from trigeminal pain afferents (substance P and calcitonin gene-related peptide), and inhibitory modulation of various central nervous system pathways (including the trigeminal nucleus caudalis, periaqueductal gray, and thalamus).Citation10
Sumatriptan was the first triptan to be marketed, followed by a further six triptans (almotriptan, eletriptan, frovatriptan, naratriptan, rizatriptan, and zolmitriptan), which exhibit improved pharmacokinetic properties. Although they can be relatively expensive,Citation11 triptans may improve quality of life, with treatment costs being offset by savings achieved by reduced demands on health care services and increased work productivity. Most triptans are currently available in cheaper generic forms (). In a meta-analysis of studies, all triptans relieved some pain within 2 hours in 49%–69% of individuals who had moderate to severe migraine (), with eletriptan 40 mg and rizatriptan 10 mg providing the greatest relief.Citation12
Table 1 Branded and generic oral triptans
Table 2 Meta-analysis of the effectiveness of oral triptans, shown in order of effectiveness for 2-hour pain relief
Here, we review the literature with respect to the socioeconomic burden of migraine, and we discuss the clinical profile and pharmacoeconomic data of eletriptan for the acute treatment of migraine.
Socioeconomic burden of migraine
The costs of migraine to society are due to the usage of health care resources and lost work productivity. Moreover, negative impact on quality of life experienced by migraine sufferers makes the condition costly to individuals as well as to society. The overall economic burden of productivity losses associated with migraine in the USA exceeds that of chronic conditions of heart disease, diabetes, asthma, and depression.Citation13 The indirect costs of migraine, such as lost days from work and reduced productivity, are hugely uncertain but are considered to exceed direct medical costs for medications, office, clinic or emergency department visits, outpatient services, laboratory and diagnostic tests, and the treatment of medication-related adverse effects. One reason cited for the heavier burden imposed by indirect costs is that migraine prevalence peaks when patients are at the height of their work productivity (aged 25–44 years).Citation14,Citation15
Different studies estimate that in the general population, the number of working days missed due to migraine per year per migraine sufferer ranges from 0.5–6.7 days.Citation16 For example, one large cross-sectional survey conducted in nine countries (Finland, Germany, Greece, Italy, Norway, Spain, Sweden, the Netherlands, and Israel) in female migraine sufferers aged 18–35 years over a 6-month period, reported a mean absence from work or school of 3.8 days per year due to migraine.Citation17 Further, the same study estimated that sufferers were unable to function properly at work or school for an additional 8.6 days per year because of migraine.Citation17
In the USA, the total costs of migraine (using 1992–1999 values) were estimated to be approximately $1 billion in direct costs annually and $4–$17 billion in indirect costs annually.Citation16,Citation18 The recent Eurolight project, a survey conducted in nine countries of the European Union, estimated societal losses attributable to all headache disorders (direct and indirect costs) at well over €100 billion per year,Citation19 with more than 90% indirectly attributable to lost productivity. In another national estimate of the annual cost of migraine, Hu et alCitation18 estimated that direct medical costs were responsible for 6.8% of total costs in men and 7.3% in women. The percent of the total cost attributable to drug costs was 1.6% in men and 2.2% in women. Other studies yield similar results, with direct medical costs consistently estimated to contribute less than 20% to the overall cost burden of migraine.Citation20
Clinical profile of eletriptan
Eletriptan, an orally administered, lipophilic, highly selective serotonin 5-HT1B/1D receptor agonist, has an established efficacy profile for the acute treatment of migraine in subjects experiencing moderate to severe migraine attacks.Citation3 Eletriptan 40 mg has shown superiority, based on results from head-to-head comparator studies versus sumatriptan 50 mg and 100 mg,Citation21–Citation23 naratriptan 2.5 mg,Citation24 and zolmitriptan 2.5 mg.Citation25 Based on the results of switch studies, eletriptan 40 mg has also demonstrated significant efficacy in migraine sufferers who did not respond to treatment with either sumatriptan or rizatriptan,Citation8,Citation26 or to nonsteroidal anti-inflammatory drugs.Citation27–Citation29
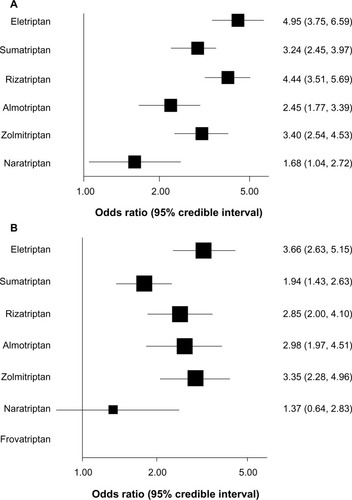
In two separate meta-analyses, eletriptan was found to be among the most effective of all marketed triptans.Citation30,Citation31 In the first meta-analysis, rizatriptan 10 mg, eletriptan 80 mg, and almotriptan 12.5 mg were the most likely triptans to provide consistent success.Citation30 The results of the most recent meta-analysis, based on a sophisticated multiple-treatment comparison methodology, showed that eletriptan 40 mg treatment had the highest probability, compared with other triptans, of patients being pain-free at 2 hours (), followed by rizatriptan 10 mg and then zolmitriptan 12.5 mg; eletriptan 40 mg also had the highest probability of patients being pain-free at 24 hours (), followed by zolmitriptan 12.5 mg.Citation31
Figure 1 Forest plots of the primary multiple treatment comparison meta-analysis results.
Eletriptan is generally safe and well tolerated. Adverse events rates are low for eletriptan 40 mg, and events are typically rated as mild or moderate. The most frequent adverse events for eletriptan 40 mg (versus placebo) are dizziness (6% versus 3%, respectively), somnolence (6% versus 4%, respectively), and asthenia (5% versus 3%, respectively).Citation32
Pharmacoeconomic analysis of eletriptan
The pharmacoeconomics of eletriptan were studied following a systematic literature review. Studies for inclusion in the review were identified through a MEDLINE® search using the following key words: “eletriptan”, “triptan”, “migraine”, “cost-effectiveness”, “cost utility”, “cost”, “cost-benefit”, “cost control”, “economic evaluation”, “drug cost”, “productivity”, and “ pharmacoeconomic’’. Identified articles were reviewed to determine whether they met the following three criteria: 1) the article contained cost-effectiveness or associated health care cost data on eletriptan; 2) the article included data on at least one other comparator triptan; and 3) the article was in English.
Applying these criteria to the search resulted in a final set of seven pharmacoeconomic studies () and one health care cost study.Citation12,Citation33–Citation39 Five of the pharmacoeconomic studies incorporated only efficacy data into cost-effectiveness ratios; three of the studies defined successful outcome in terms of being both pain-free and with no recorded adverse events. Only two of the studies included analyses of the effect of treatment on the indirect costs of migraine, and these analyses were limited.Citation12,Citation20 Six of the included studies were financed by manufacturers,Citation33–Citation38 and two were independent studies.Citation12,Citation39 The efficacy data used in most of the studies originated from a previous meta-analysis by Ferrari et al.Citation30 Most studies were conducted before patent-expiration of the original brand products; therefore, only the most recent report considered generic prices.Citation12 Study results are shown in and are reviewed individually.
Table 3 Characteristics of pharmacoeconomic studies involving triptans
Table 4 Pharmacoeconomic studies of triptans in the treatment of migraine
In 2004, BelseyCitation33 conducted a comprehensive cost-effectiveness analysis of all seven triptans in the treatment of an acute migraine attack, using data from a meta-analysis of 37 randomized, placebo-controlled trials studies conducted in six countries (UK, Germany, Netherlands, Italy, USA, and Canada). The effect sizes were numbers needed to treat based on the proportion of patients who were pain-free at 2 hours postdose in both treatment and placebo groups.Citation33 Incremental cost-effectiveness was compared for sumatriptan 100 mg, which was the first and most widely prescribed oral triptan. Rizatriptan 10 mg and eletriptan 40 mg and 80 mg were the most cost-effective oral triptans with respect to the outcome of pain-free at 2 hours postdose ().Citation33 Overall, rizatriptan 10 mg exhibited the most favorable absolute cost-effectiveness ratio in all six countries included in the analysis.Citation33 In a comparison with sumatriptan 100 mg, rizatriptan 10 mg and eletriptan 40 mg were consistently the most cost-effective therapeutic options in five of the six countries examined.Citation33 This study had several limitations. For example, the analysis was informal and only considered drug acquisition costs for branded products. In addition, the costs of extra doses/rescue medication were not considered.
In 2005, in a meta-analysis, Perfetto et alCitation36 evaluated the cost-effectiveness of six oral triptans (almotriptan, eletriptan, naratriptan, rizatriptan, sumatriptan, and zolmitriptan), using clinical data from the previously published meta-analysis conducted by Ferrari et al,Citation30 examining the total costs of triptans for treating 100 migraine attacks, as well as the costs per successfully treated patient. Two-hour response, pain-free response, and recurrence rate were used to estimate the number of doses that were used for treatment of each success and failure.Citation36 Total triptan cost was calculated by using the average wholesale price per dose, less 15% for use of a nongeneric triptan.Citation36 Overall, eletriptan 40 mg had the lowest total triptan cost for treating 100 migraine attacks ($1,560), followed by zolmitriptan 2.5 mg ($1,629), and almotriptan ($1,670).Citation36 Eletriptan 40 mg also had the lowest cost per successfully treated patient ($56.39) ().Citation36 Naratriptan 2.5 mg had the greatest total cost for treating 100 patients ($1,945), as well as the greatest cost for successfully treating a single patient ($111.44) ().Citation36 This study, again, had several key limitations; it was an informal analysis where only the costs of drug acquisition were taken into consideration, and the costs of rescue medication were not calculated.
A further study conducted in Spain examined the cost-effectiveness of six marketed triptans (almotriptan, eletriptan, naratriptan, rizatriptan, sumatriptan, and zolmitriptan).Citation37 Efficacy data were again taken from a previously published meta-analysis.Citation40 Measures of effectiveness included a sustained pain-free status, which was defined as being pain-free at 2 hours postdose with no recurrence and no rescue medication for 2–24 hours.Citation37 Costs included in the analysis were drug acquisition costs in addition to costs associated with the treatment of central nervous system- and chest-related adverse events.Citation37 Cost-effectiveness for each triptan was evaluated in comparison with sumatriptan 100 mg.Citation37 Combining clinical and economic considerations, rizatriptan 10 mg and almotriptan 12.5 mg were demonstrated to be the most cost-effective triptans in Spain.Citation37 Although this study is noteworthy for attempting to include the additional costs of treating adverse events, the costs associated with their management were estimated by clinical experts. Direct assessment of health care utilization costs would provide a more accurate accounting of the costs for treatment of adverse events.
Kelman and Von SeggernCitation34 conducted a cost-effectiveness analysis of triptans, using the efficacy and tolerability data from the published meta-analysis,Citation30 using sumatriptan 100 mg as the comparator. A successful outcome measure was described in terms of sustained pain-free plus no adverse events (SNAE). Costs per 100 SNAE patients were then calculated. This pharmacoeconomic study found that when using average wholesale prices, almotriptan 12.5 mg ($7,120), rizatriptan 10 mg ($7,427), followed by eletriptan 40 mg ($8,167) were the most cost-effective treatment options ().Citation34 A potential limitation of this study was that the calculation of SNAE was based on the assumption that efficacy and tolerability are uncorrelated.Citation34 However, the actual association between efficacy and tolerability of triptans is unknown. Again, this analysis only assessed drug acquisition costs.
Mullins et alCitation35 evaluated the pharmacoeconomics of six oral triptans (almotriptan, eletriptan, naratriptan, rizatriptan, sumatriptan, and zolmitriptan) from the perspective of Medicaid as a payor. Effectiveness data were again obtained from a previously published meta-analysis.Citation30,Citation40 Efficacy measures included: headache relief and pain-free at 2 hours, recurrence of headache pain, sustained pain-free, and recurrence.Citation35 Per dose acquisition costs were calculated using Medicaid reimbursement data from seven American states (Florida, Georgia, Illinois, North Carolina, Ohio, Wisconsin, and West Virginia). Among all marketed triptans across the seven states, eletriptan 20 mg (range $1,549–$1,658) and eletriptan 40 mg ($1,578–$1,661) exhibited the lowest costs to treat 100 migraine attacks.Citation35 Naratriptan 2.5 mg (range $1,734–$2,018), sumatriptan 25 mg ($1,853–$1,954), and zolmitriptan 5 mg ($1,854–$1,960) demonstrated the highest cost to treat 100 migraine attacks.Citation35 Eletriptan 40 mg exhibited the lowest cost/success (range $57.00–$60.10); naratriptan 2.5 mg ($99.40–$115.70), sumatriptan 25 mg ($107.10–$112.90 [data not shown]), and rizatriptan 5 mg ($99.40–$111.30 [data not shown]) had the highest cost/success values ().Citation35 As with other pharmacoeconomic studies, this was an informal analysis that had not accounted for rescue medication costs, and only drug acquisition costs of nongeneric drugs were considered.
Ramsberg and HenrikssonCitation39 used a decision-tree cost-effectiveness model to compare the costs and effects of five oral triptans (almotriptan, eletriptan, rizatriptan, sumatriptan, and zolmitriptan) in the treatment of a single attack in a typical migraine patient, from a Swedish societal perspective. Effectiveness data were again taken from a previously published meta-analysis.Citation30,Citation40 The primary end point was SNAE; other measures of efficacy included a status of pain-free at 2 hours and recurrence.Citation39 Costs comprised drug acquisition costs and productivity losses. Additional sensitivity analyses were conducted using data from meta-analyses of the efficacy of triptans in the treatment of migraine conducted by Oldman et alCitation41 and by Belsey.Citation33 The results indicated that eletriptan 40 mg and rizatriptan 10 mg were the most cost-effective, with other triptans having higher costs and worse health outcomes ().Citation39 Rizatriptan 10 mg had an incrementally higher cost per SNAE of about €100 versus eletriptan 40 mg.Citation39 Overall, rizatriptan 10 mg, eletriptan 40 mg, and almotriptan 12.5 mg were more likely to be cost-effective than were the other three triptans assessed.Citation39 This analysis did not compare triptans to no therapy or other nontriptan migraine treatments.
A recent independent cost-effectiveness/cost-utility analysis assessed all seven oral triptans following the introduction of generic sumatriptan to the Finnish market in 2008.Citation12 In this study, the decision-tree model assessing oral triptans in SwedenCitation39 was adapted to assess additional treatment arms and the related quality of life. Efficacy data were estimated from 56 publications following a systematic literature review and mixed treatment comparison. Efficacy measures included a response at 2 hours, a status of pain-free at 2 hours, and recurrence, with the primary efficacy end point being SNAE.Citation12 Sustained pain-free at 24 hours and rescue medication were not considered. Cost-effectiveness was calculated as the incremental cost per additional SNAE. Secondarily, the incremental cost per quality-adjusted life year (QALY) gained was also estimated. QALYs were calculated based on utility values estimated from the Quality of Well-Being Scale, using utility weights estimated by Thompson et al.Citation42 The least costly treatment per attack was generic sumatriptan 100 mg (€20.86).Citation12 Overall, eletriptan 40 mg was found to be the most cost-effective triptan in terms of the lowest incremental cost per additional SNAE.Citation12 The incremental cost-effectiveness ratio of eletriptan 40 mg relative to sumatriptan 100 mg was about €44 per additional SNAE.Citation12 The results for QALYs indicated that eletriptan 40 mg had the greatest probability of being the most cost-effective option at willingness-to-pay thresholds of about €20,000 per QALY gained or above.Citation12 In a one-way sensitivity analysis, the results were not sensitive to the costs of drug acquisition and utility values.Citation12
Although this independent study derived efficacy data from a systematic review employing a mixed-treatment comparison, the application of the results might be limited because the authors did not evaluate the costs of health care service use or adverse event management. Another limitation is uncertainty regarding the utility estimates for the QALYs obtained from the study by Thompson et al.Citation42 Non-preference-based measures were also employed to estimate quality of life.
Wells et alCitation38 performed a cost-effectiveness analysis of eletriptan (40 mg and 80 mg) compared with sumatriptan (100 mg), based on the results of a single randomized, double-blind, placebo-controlled trial using two efficacy end points. The first efficacy measure, defined as “success measure 1”, included 24-hour sustained pain-free with pain-free headache status at 2 hours, no recurrence within 24 hours of the first dosing, and no requirement for rescue medication;Citation38 “ success measure 2” was defined as positive headache response at 1 hour and achievement of pain-free status by 2 hours.Citation38 Costs included were drug acquisition costs, costs of a second dose, and the need for rescue medication.Citation38 Costs per successfully treated attack were significantly lower for eletriptan 40 mg versus sumatriptan 100 mg using both efficacy outcome measures. Specifically, for success measure 1, the costs per successfully treated migraine attack were £17.55 for eletriptan 40 mg and £80.50 for sumatriptan 100 mg.Citation38 Similarly, for success measure 2, costs were £29.61 for eletriptan 40 mg and £124.28 for sumatriptan 100 mg per successfully treated migraine attack.Citation38 A major limitation of this study was that only one other triptan (sumatriptan) was included besides eletriptan, where the results were from a single clinical trial.
One recent study has used a classification and regression tree (CART) analysis to identify subpopulations of patients with migraine with a favorable cost profile for a given drug.Citation43 In this study, a CART analysis was performed using propensity score-matched migraine populations treated with either eletriptan 40 mg or generic sumatriptan 100 mg. Cost data used in the analyses were based on a retrospective Truven Health Analytics MarketScan® commercial claims and encounters database (Truven Health Analytics®, Ann Arbor, MI, USA). CART analyses were used to determine variables relevant to the cost profile after initiating eletriptan, relative to generic sumatriptan.Citation43 Health care costs were compared between eletriptan and generic sumatriptan for the stratified populations, by comparing the pre- to postindex differences in mean annual costs for the two triptans.Citation43
The results of the CART analyses revealed that 1 year after the index date, total health care costs were comparable for eletriptan 40 mg and generic sumatriptan 100 mg.Citation43 However, in patients with higher health care utilization due to migraine, and in males, regardless of migraine severity, treatment with eletriptan 40 mg had lower total costs versus generic sumatriptan 100 mg.Citation43 Thus, for a certain subpopulation of migraine patients (males with higher health care utilization due to migraine), differences in annual health care costs were evident between eletriptan 40 mg and sumatriptan 100 mg.Citation43 Such differences in health care costs for a subpopulation raise the question of whether the cost-effectiveness of different triptans would also vary by subpopulation once the efficacy and tolerability of triptans in such subpopulations are incorporated in pharmacoeconomic models.
Discussion
In general, a consistent pattern of results emerged across the eight reviewed pharmacoeconomic studies: eletriptan 40 mg, rizatriptan 10 mg, and almotriptan 12.5 mg were shown to be more cost-effective than other triptans. This pattern was evident when efficacy was defined as 2 hours pain-free, sustained pain-free, and SNAE. Moreover, the pattern was evident when not only drug costs were included, but also, when cost-effectiveness models accounted for second doses of a triptan and use of rescue medication,Citation38 management of adverse events,Citation37 and productivity loss.Citation12,Citation39 In the most recent review of all seven triptans, which was independently conducted, eletriptan 40 mg was found to be one of the most cost-effective treatment options, even in comparison with generic sumatriptan.Citation12 Our findings in the current review are generally consistent with an earlier Canadian overview of pharmacoeconomic studies of triptans, which concluded that economic studies show that eletriptan, rizatriptan, and almotriptan were the most cost-effective triptans.Citation44
One important consideration is the recurrence of migraine. Approximately 35% of patients who respond to treatment with a triptan experience a recurrence of headache within 24 hours.Citation30,Citation40 However, in a pooled analysis of patients (n=742) with multiple risk factors for suffering a recurrence of their migraine, Dodick et alCitation45 found significantly lower recurrence rates with eletriptan 40 mg versus sumatriptan 100 mg (36% versus 51%, respectively) (P<0.01). In addition, eletriptan 40 mg has a favorable safety profile,Citation30 and this in particular, likely enhanced the cost-effectiveness ratio, which incorporated adverse events.
Conclusions from this review need to be framed in terms of limitations of the available data. It should be noted that cost-effectiveness metrics were calculated, in most studies, using meta-analytic data summarizing placebo-controlled studies of triptans. Ideally, cost-effectiveness analyses would be based on direct head-to-head comparator studies involving all relevant agents. Only limited head-to-head comparator data were available, and only one single study compared all of the available triptans.Citation12 The Ramsberg and Henriksson study included a secondary analysis focusing only on comparator trials, but none of the four comparator trials examined included eletriptan.Citation39 A related concern is that six of the eight available pharmacoeconomic studiesCitation12,Citation34–Citation37,Citation39 relied primarily or exclusively on the same meta-analysisCitation30 for efficacy and/or tolerability data. Future cost-effectiveness evaluations of triptans should incorporate updated efficacy/tolerability data, with more comparator trials, for computing cost-effectiveness ratios. Another important limitation is that the majority of the available studies did not include indirect costs in their pharmacoeconomic analysis.
It is also important to note that since the publication of some of the pharmacoeconomic studies reviewed here, additional generic versions of most of the triptans are now available. However, as noted earlier in this review, drug acquisition costs only make up a small portion of the total annual cost burden of migraine, even when triptan therapy is limited to prescription drugs. Because of the limited impact of drug costs, it is likely that eletriptan 40 mg remains a cost-effective option even when compared with triptans that are now available as generics. However, confirmation of the cost-effectiveness of eletriptan relative to generic triptans would require data from prospective, head-to-head migraine trials that include valid and current assessments of direct and indirect costs.
Conclusion
With these limitations in mind, the results of available studies consistently found eletriptan 40 mg was among the most clinically and cost-effective of the oral triptans for the treatment of acute migraine. This finding was evident across diverse countries and payers, including Medicaid in the USA.
Acknowledgments
Editorial support was provided by Sarah Knott of Engage Scientific and funded by Pfizer Inc. Additional support, composed of copyediting a late draft of the manuscript and collating authors’ responses to peer review comments, was provided by Anne Jakobsen, MSc; Abegale Templar, PhD; and Jon Edwards, PhD, of Engage Scientific and funded by Pfizer Inc.
Disclosure
The study was funded by Pfizer Inc. Drs Bhambri, Mardekian, Liu, and Ramos are full-time employees of Pfizer Inc. Dr Schweizer owns stock in Pfizer Inc. and Novartis, and has received payments for consulting and/or medical writing services from Alkermes, Sunovion Pharmaceuticals, Titan Pharmaceuticals, Novartis AG, and Pfizer Inc. Dr Schweizer is also the owner of Paladin Consulting Group, Inc., which was a paid consultant to Pfizer Inc. in connection with the development of this manuscript. The authors report no other conflicts of interest.
References
- Headache Classification Committee of the International Headache Society (IHS)The International Classification of Headache Disorders, 3rd edition (beta version)Cephalalgia201333962980823771276
- LiptonRBScherAIKolodnerKLibermanJSteinerTJStewartWFMigraine in the United States: epidemiology and patterns of health care useNeurology200258688589411914403
- McCormackPLKeatingGMEletriptan: a review of its use in the acute treatment of migraineDrugs20066681129114916789799
- LiptonRBBigalMEDiamondMFreitagFReedMLStewartWFAMPP Advisory GroupMigraine prevalence, disease burden, and the need for preventive therapyNeurology200768534334917261680
- Von KorffMStewartWFSimonDJLiptonRBMigraine and reduced work performance: a population-based diary studyNeurology1998506174117459633720
- LiptonRBDiamondSReedMDiamondMLStewartWFMigraine diagnosis and treatment: results from the American Migraine Study IIHeadache200141763864511554951
- BuseDCLiptonRBGlobal perspectives on the burden of episodic and chronic migraineCephalalgia2013331188589023482725
- GoldsteinJTiseoPTAlbertKSLiCSikesCREletriptan in migraine patients reporting unsatisfactory response to rizatriptanHeadache20064671142115016866718
- AukermanGKnutsonDMiserWFDepartment of Family Medicine, Ohio State University College of Medicine and Public Health, Columbus, OhioManagement of the acute migraine headacheAm Fam Physician200266112123213012484694
- OlesenJBursteinRAshinaMTfelt-HansenPOrigin of pain in migraine: evidence for peripheral sensitisationLancet Neurol20098767969019539239
- CaroJJGetsiosDPharmacoeconomic evidence and considerations for triptan treatment of migraineExpert Opin Pharmacother20023323724811866674
- AsseburgCPeuraPOksanenTTurunenJPurmonenTMartikainenJCost-effectiveness of oral triptans for acute migraine: mixed treatment comparisonInt J Technol Assess Health Care201228438238923013610
- LambCERatnerPHJohnsonCEEconomic impact of workplace productivity losses due to allergic rhinitis compared with select medical conditions in the United States from an employer perspectiveCurr Med Res Opin20062261203121016846553
- LiptonRBStewartWFScherAIEpidemiology and economic impact of migraineCurr Med Res Opin200117Suppl 1S4S1212463270
- StangPEOsterhausJTImpact of migraine in the United States: data from the National Health Interview SurveyHeadache199333129358436495
- de LissovoyGLazarusSSThe economic cost of migraine. Present state of knowledgeNeurology1994446 Suppl 4S56S628008226
- DuelandANLeiraRBurkeTAHillyerEVBolgeSThe impact of migraine on work, family, and leisure among young women – a multinational studyCurr Med Res Opin200420101595160415462692
- HuXHMarksonLELiptonRBStewartWFBergerMLBurden of migraine in the United States: disability and economic costsArch Intern Med1999159881381810219926
- LindeMGustavssonAStovnerLJThe cost of headache disorders in Europe: the Eurolight projectEur J Neurol201219570371122136117
- GoldbergLDThe cost of migraine and its treatmentAm J Manag Care200511Suppl 2S62S6716095269
- GoadsbyPJFerrariMDOlesenJEletriptan in acute migraine: a double-blind, placebo-controlled comparison to sumatriptan. Eletriptan Steering CommitteeNeurology200054115616310636142
- MathewNTSchoenenJWinnerPMuirheadNSikesCRComparative efficacy of eletriptan 40 mg versus sumatriptan 100 mgHeadache200343321422212603639
- SandriniGFärkkiläMBurgessGForsterEHaughieSEletriptan Steering CommitteeEletriptan vs sumatriptan: a double-blind, placebo-controlled, multiple migraine attack studyNeurology20025981210121712391349
- Garcia-RamosGMacGregorEAHilliardBBordiniCALestonJHettiarachchiJComparative efficacy of eletriptan vs naratriptan in the acute treatment of migraineCephalalgia200323986987614616928
- SteinerTJDienerHCMacGregorEASchoenenJMuirheadsNSikesCRComparative efficacy of eletriptan and zolmitriptan in the acute treatment of migraineCephalalgia2003231094295214984226
- FärkkiläMOlesenJDahlöfCEletriptan for the treatment of migraine in patients with previous poor response or tolerance to oral sumatriptanCephalalgia200323646347112807526
- ChiaYCLimSHWangSJCheongYMDenaroJHettiarachchiJEfficacy of eletriptan in migraineurs with persistent poor response to nonsteroidal anti-inflammatory drugsHeadache200343998499014511275
- DiamondMLHettiarachchiJHilliardBSandsGNettREffectiveness of eletriptan in acute migraine: primary care for Excedrin nonrespondersHeadache200444320921615012657
- MartinVTLoderETaylorKAlmasMHilliardBEletriptan treatment of migraine in patients switching from barbiturate-containing analgesics: results from a multiple-attack studyCephalalgia200525972673416109055
- FerrariMDGoadsbyPJRoonKILiptonRBTriptans (serotonin, 5-HT1B/1D agonists) in migraine: detailed results and methods of a meta-analysis of 53 trialsCephalalgia200222863365812383060
- ThorlundKMillsEJWuPComparative efficacy of triptans for the abortive treatment of migraine: a multiple treatment comparison meta-analysisCephalalgia201434425826724108308
- Relpax (eletriptan hydrobromide) tablet, film coated [prescribing information]New York, NYPfizer Inc2013 Available from: http://labeling.pfizer.com/ShowLabeling.aspx?id=621Accessed July 31, 2014
- BelseyJDCost effectiveness of oral triptan therapy: a trans-national comparison based on a meta-analysis of randomised controlled trialsCurr Med Res Opin200420565966915140331
- KelmanLVon SeggernRLUsing patient-centered endpoints to determine the cost-effectiveness of triptans for acute migraine therapyAm J Ther200613541141716988536
- MullinsCDSubediPRHealeyPJSanchezRJEconomic analysis of triptan therapy for acute migraine: a Medicaid perspectivePharmacotherapy20072781092110117655509
- PerfettoEMWeisKAMullinsCDSubediPHealeyPJSrAn economic evaluation of triptan products for migraineValue Health20058664765516283865
- SlofJBadiaXLainez-AndresJMGalvanJHerasJManagement costs of chest and CNS-related adverse events associated with the treatment of acute migraine attacks with oral triptansNeurologia2005206290298 Spanish16007512
- WellsNHettiarachchiJDrummondMA cost-effectiveness analysis of eletriptan 40 and 80 mg versus sumatriptan 50 and 100 mg in the acute treatment of migraineValue Health20036443844712859585
- RamsbergJHenrikssonMThe cost-effectiveness of oral triptan therapy in SwedenCephalalgia2007271546217212684
- FerrariMDRoonKILiptonRBGoadsbyPJOral triptans (serotonin 5-HT(1B/1D) agonists) in acute migraine treatment: a meta-analysis of 53 trialsLancet200135892941668167511728541
- OldmanADSmithLAMcQuayHJMooreRAPharmacological treatments for acute migraine: quantitative systematic reviewPain200297324725712044621
- ThompsonMGawelMDesjardinsBFerkoNGrimaDAn economic evaluation of rizatriptan in the treatment of migrainePharmacoeconomics200523883785016097844
- RamosELiuLMardekianJCabreraJIdentification of subpopulations of migraine patients who have a favorable cost profile with eletriptan treatmentCephalalgia2013338148149
- MembeSMcGahanLCimonKGawelMGiammarcoRMierzwinski-UrbanMTechnology Report: Triptans for Acute Migraine: Comparative Clinical Effectiveness and Cost-EffectivenessOttawa, ONCanadian Agency for Drugs and Technologies in Health2007 Available from: http://www.cadth.ca/media/pdf/I4001_tr_Triptans_e.pdfAccessed July 29, 2014
- DodickDWLiptonRBGoadsbyPJPredictors of migraine headache recurrence: a pooled analysis from the eletriptan databaseHeadache200848218419318234045