
Abstract
Background
Despite titanium (Ti) implants have been commonly used in the medical device field due to their superior biocompatibility, implant-associated bacterial infection remains a major clinical complication. Nanosilver, an effective antibacterial agent against a wide spectrum of bacterial strains, with a low-resistance potential, has attracted much interest too. Incorporation of nanosilver on Ti implants may be a promising approach to prevent biofilm formation.
Purpose
The objective of the study was to investigate the antibacterial effects and osteoinductive properties of nanosilver/poly (dl-lactic-co-glycolic acid)-coated titanium (NSPTi).
Methods
Gram-positive methicillin-resistant Staphylococcus aureus (MRSA) and the Gram-negative opportunistic pathogen Pseudomonas aeruginosa (PAO-1) were used to evaluate the antibacterial activity of NSPTi implants through the analysis of bacterial colonization in vitro and in vivo. Furthermore, we examined the osteoinductive potential of NSPTi implants by investigating the proliferation and differentiation of MC3T3-E1 preosteoblast cells. In vivo, the osteoinductive properties of NSPTi implants were assessed by radiographic evaluation, H&E staining, and Masson’s trichrome staining.
Results
In vitro, bacterial adhesion to the 2% NSPTi was significantly inhibited and <1% of adhered bacteria survived after 24 hours. In vitro, the average colony-forming units (CFU)/g ratios in the 2% NSPTi with 103 CFU MRSA and PAO-1 were 1.50±0.68 and 1.75±0.6, respectively. In the uncoated Ti groups, the ratios were 1.03±0.82×103 and 0.94±0.49×103, respectively. These results demonstrated that NSPTi implants had prominent antibacterial properties. Proliferation of MC3T3-E1 cells on the 2% NSPTi sample was 1.51, 1.78, and 2.22 times that on the uncoated Ti control after 3, 5, and 7 days’ incubation, respectively. Furthermore, NSPTi implants promoted the maturation and differentiation of MC3T3-E1 cells. In vivo, NSPTi accelerated the formation of new bone while suppressing bacterial survival.
Conclusion
NSPTi implants have simultaneous antibacterial and osteoinductive activities and therefore have the potential in clinical applications.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
It is a challenging task to treat implant-associated bacterial infections that are severe complications in orthopedics. Implant-associated bacterial infections can lead to increased patient morbidity and may consequently lead to worse results.Citation1–Citation5 Management of an implant-associated infection often necessitates multiple debridement surgeries, implant replacement or removal, and long-term antibiotic treatment.Citation6–Citation9 These problems are aggravated in patients with bone healing disorders associated with rheumatoid arthritis, osteoporosis, diabetes, or aging due to the difficulty of clearing an infection from poorly vascularized bone tissues and other necrotic tissues.Citation3,Citation5,Citation10,Citation11 Implant-associated infections are caused by bacterial adhesion to an implant surface and subsequent formation of biofilms around implanted devices.Citation12 After implantation, a rapid conditioning layer covers the surface of the implant and facilitates bacterial adhesion, forming a slimy extracellular polymeric substance (EPS) bacterial biofilm.Citation5,Citation12,Citation13 The EPS blocks the penetration of antibiotics and host immune cells, because the altered chemical microenvironment in the biofilm associated with nutrient and oxygen consumption causes some bacteria more resistant to antimicrobial and immune cells killing.Citation5,Citation14–Citation16 Consequently, once a bacterial biofilm is produced, treating the infections is quite difficult, and bacteria in EPS biofilm form can be less susceptible to antibiotics or immune-reactive molecules than free-floating bacteria.Citation17 Multiple approaches have attempted to prevent infection and bacterial biofilm formation, in particular, surface coating strategies using antibacterial or antiadhesive materials that inhibit microbial infection while simultaneously promoting bone formation seems to be promising.
Although current antibiotics have been coated on orthopedic material surface to prevent infection, binding specificity of a designated bacteria to a specific conventional antimicrobial limits the clinical utility of local antibiotics.Citation18–Citation21 Because a wide variety of bacterial species are responsible for implant-associated infections: Gram-positive Staphylococcus bacteria species (Staphylococcus aureus, Staphylococcus epidermidis, Staphylococcus hominis, and Staphylococcus haemolyticus) and Gram-negative Pseudomonas aeruginosa and Escherichia coli, among which, S. aureus and P. aeruginosa are the two most common pathogens for implant infection.Citation22–Citation24 Narrow-spectrum antibiotic therapies may fail to prevent all implant-associated infecting bacteria, while broad-spectrum antibiotic therapies may induce antibiotic resistance. Treatment of infections becomes even more difficult due to the emergence of increasing number of antibacterial resistant bacteria, such as vancomycin-resistant S. aureus (VRSA) and methicillin-resistant S. aureus (MRSA).Citation24
Silver, an antimicrobial agent against a wide spectrum of Gram-positive and Gram-negative bacterial strains including MRSA, VRSA, and methicillin-resistant S. epidermidis, has been widely employed to treat infections.Citation18,Citation25,Citation26 It has been speculated that several mechanisms are associated with the antibacterial performance of silver such as structural damage to bacterial function, inhibition of bacterial function, and induction of bacterial apoptosis-like response;Citation28,Citation29 and the multilevel antimicrobial mode ensures that bacterial resistance cannot be easily acquired. Furthermore, previous studies have suggested that silver antimicrobial actions affect at least three bacterial cell systems, and silver resistance needs to have three high frequency distinct mutations, so silver-resistant bacteria are not common in clinical cases.Citation30–Citation32
Due to their extremely large surface area and surface reactivity, compared with traditional silver counterparts, nanosilver particles exhibit superior physicochemical and biomedical properties, including antimicrobial activity and catalysis.Citation33 The United States Food and Drug Administration (FDA)-approved, biocompatible and biodegradable polymer poly (dl-lactic-co-glycolic acid) (PLGA) was chosen in this research to stabilize nanosilver particles mainly because of its autocatalytic hydrolysis reaction through nucleophilic interactions with nanoparticles.Citation34 In the present work, the antibacterial effects and osteoinductive properties of nanosilver/PLGA-coated titanium (NSPTi) implants were investigated through in vitro and in vivo studies in rabbits.
Materials and methods
Pretreatment of Ti samples
Titanium, of 99.5% purity, was purchased from BaoTi Group Co., Ltd. (Xian, People’s Republic of China). Initial, Ti bars (Φ 1×10 mm) and discs (thickness: 1.0 mm, diameter: 6.5 mm) were mechanically wet abraded with abrasive SiC papers (1,200 grit). In order to improve surface roughness and remove native oxide, the Ti samples were etched using a mixed acid solution (H2SO4:HCl:H2O =2:2:1, volume ratio) at 50°C for 4 hours. Then, the samples were soaked in NaOH solution (100 mL of 5 M NaOH) at 60°C for 4 hours to increase surface hydrophilicity. After ultrasonic cleaning and air drying, the samples were sterilized by ultraviolet irradiation for 30 minutes.
Preparation of nanosilver/PLGA coatings
Nanosilver/PLGA coatings were obtained by solvent casting, mixing 20–30 nm diameter spherical nanosilver (Shanghai Naiou Nanotechnology Co., Ltd, Shanghai, People’s Republic of China) with 18% (w/v) PLGA (Daigang Biomaterial Co., Ltd, Jinan, People’s Republic of China, lactic:glycolic ratio =85:15, inherent viscosity: 0.64 dL/g in chloroform; Sigma-Aldrich Co., St Louis, MO, USA) solution at 300 rpm for 1 hour thoroughly. Coatings were produced by adding Ag nanoparticles at 1 and 2 wt% (designated as 1% NSPTi and 2% NSPTi, respectively) with respect to PLGA. Ti bars and discs were immersed in the nanosilver/PLGA solution in chloroform at room temperature for 45 seconds and thoroughly air-dried. The immersion and dry processes were repeated three times to ensure a homogenized coating for each NSPTi implant sample.
Characterization of coatings
The morphology and composition of the NSPTi implant surface were characterized using field-emission scanning electron microscopy (SEM) (HITACHI SU8010, Tokyo, Japan) equipped with an X-ray energy-dispersive spectrometer (EDS).
Culture of cells and cell viability assessment
MC3T3-E1 mouse preosteoblasts were obtained from Chinese Academy of Sciences Shanghai Cell Bank (Shanghai, People’s Republic of China). The cells were seeded on NSPTi discs and incubated at 37°C in a 5% CO2 environment with 500 mL osteogenic medium (α-Minimum Essential Medium supplied with 10% FBS, 100 nM dexamethasone, 1% penicillin–streptomycin, 50 µg/mL ascorbic acid, and 10 mM β-glycerophosphate). All media for cell culture were purchased from Invitrogen (Carlsbad, CA, USA). Cell counting kit-8 (Dojindo Molecular Technologies, Kumamoto, Japan) was used to identify potential cellular toxicity of the samples. The cell density was 2×104 cells/sample.
Ag release
The release of Ag from NSPTi samples (1% NSPTi and 2% NSPTi) in PBS was monitored by inductively coupled plasma–atomic emission spectrometry (Thermo Fisher ICP6300, Waltham, MA, USA) analyzing the resulting set of PBS solutions. The samples were incubated in PBS (6 mL, pH 7.4) at 37°C in dark conditions for 24 hours and rinsed with deionized water. The whole procedure was repeated for up to 14 days. The detection limit of Ag in this method was 0.001 ppm, and the emission line was 328.1 nm.
Antibacterial tests in vitro
The antibacterial properties of the coatings were evaluated against Gram-positive MRSA (ATCC43300; American Type Culture Collection [ATCC], Manassas, VA, USA) and Gram-negative PAO-1 (ATCC15442; ATCC).Citation22–Citation24 MRSA and PAO-1 were inoculated into Luria–Bertani (LB; Sigma-Aldrich Co.) broth medium. Initially, the uncoated Ti 1% NSPTi and 2% NSPTi were incubated in 103 or 105 colony-forming units (CFU) bacterial suspensions (in culture broth) with shaking at 200 rpm at 37°C for 1, 2, 6, and 24 hours. Next, adherent bacteria on each sample bar were suspended in sterilized PBS by sonication for 30 seconds at 40 kHz using a sonication device (BactoSonic; BANDELIN GmbH, Berlin, Germany)Citation35 and plated onto 10 cm LB culture medium plates.Citation36 After incubation, the colonies were quantitated by aerobic plate count method according to procedures described in the FDA Bacteriological Analytical Manual (BAM). Concisely, the whole bacteria collected in 1 mL sterilized PBS was inoculated into plates and diluted if number of CFU per plate exceeded 250. If number of CFU per plate was in the range of 25–250, total number of colonies counted was recorded. If number of CFU per plate was >250, the bacterial solution was diluted (1:10, 1:100, and 1:1,000) until the resulting number of CFU was within 25–250 per plate range, and number of colonies was then calculated.
Osteoinductivity in vitro
ALP activity (normalized to the total protein concentration) and degree of mineralization were employed to determine the osteoinductive potential of NSPTi implants on osteoblastic differentiation. ALP is an early phenotypic marker for osteogenic differentiation, and the formation of mineralized nodules caused by the calcium secretion of MC3T3-E1 cells is an important functional indicator of osteoblasts.Citation37,Citation38 The ALP activity was standardized to the total cellular protein concentration, which was determined with a BCA protein assay kit (Tiangen Biotech Company, Beijing, People’s Republic of China). ALP activity was detected by an ALP assay kit (Jiancheng Biotech, Nanjing, People’s Republic of China). The extent of matrix mineralization was determined by Alizarin red staining (Sigma-Aldrich Co.).
Animals and surgical procedures
Sixteen adult male New Zealand White rabbits, average weight 3 kg, were used in the full study. All surgical procedures were approved and performed according to the guidelines of the Institutional Animal Care and Use Committee of Shandong University. After shaving and disinfection operations, the rabbits were anesthetized by an intraperitoneal injection with 2% pentobarbital sodium (30 mg/kg; Sigma-Aldrich Co.). Local anesthesia was induced with 1 mL of 2% lidocaine (Sigma-Aldrich Co.) to control bleeding. Five intramedullary cavities were drilled on each tibia of rabbits, followed by implantation of sample bars (uncoated Ti and 2% NSPTi). Subsequently, MRSA or PAO-1 suspended in 100 µL sterile PBS (104 CFU/mL) was slowly injected into the tibia canal using a micropipette. The micropipette was left for 30 seconds in place to prevent the suspension of the bacteria from leaking out along the injection track. Then, the micropipette was removed. At the end of the procedure, the fascia and skin were closed with 4–0 Vicryl absorbable sutures (Vicryl Rapide, Ethicon, Johnson & Johnson, Livingston, UK). Operated rabbits were housed separately and fed a commercial pelleted diet. Operated rabbits were monitored daily. Analgesics were injected intramuscularly for 3 days to control pain, and no antibiotics were administered.
Clinical evaluation
A digital thermometer (OMRON, Dalian, People’s Republic of China) was used to measure body temperature. Fresh venous blood was obtained for the assessment of white blood cells (WBCs). Clinical signs and symptoms of infection (healing of incisions, appearance of the soft tissues, diarrhea, and lameness) following surgery were monitored. Clinical information was collected on days 0, 3, and 8 and weeks 2, 4, 6, and 8 postsurgery.
Radiographic evaluation
At 2, 4, 6, and 8 weeks after surgery, the operated rabbit tibias were scanned using cone beam computed tomography CBCT (NewTom 5 G, QR Verona, Verona, Italy) while the animals were under general anesthesia. Radiographs were taken at a peak tube voltage of 110 kV, a tube current of 4.2–4.6 mA, and an exposure time of 5.4 seconds. A reconstruction volume of 15×15 cm and a voxel size of 0.3 mm were used. Three-dimensional reconstruction was performed using the threshold and region growing technique with Mimics software, version 17.0 (Materialise, Leuven, Belgium). The animals were sacrificed 8 weeks postoperatively through air embolism. Operated tibias were dissected and harvested for microbiological and histological assessment.
Microbiological evaluation in vivo
Tibia bone tissue samples were split, cut into little pieces, frozen in liquid nitrogen, and crushed in an autopulverizer. The pulverized bone (500 mg) was suspended in 6 mL of PBS and centrifuged for 30 seconds at 10,000 rpm. Serial dilutions were made and plated onto the plates and incubated at 37°C for 24 hours. After incubation, the number of colonies per plate was counted for each tibia bone samples and the bacterial count was calculated per gram bone (CFU/g bone tissue).
Histological evaluation
Tibia bone tissue samples were fixed for 48 hours in 4% formaldehyde/PBS (pH 7.4), decalcified in 10% EDTA in PBS (0.5 M) for 3–4 weeks, dehydrated in ethanol, cleared with xylene, embedded in paraffin, and routinely processed for histological evaluation. Tissue sections of 5 µm were cut and stained with H&E and Masson’s trichrome collagen in order to evaluate morphology and inflammation.
Statistical analysis
Data are depicted as mean ± standard error of mean. Statistical analyses were performed using SPSS 16.0 software (SPSS Inc., Chicago, IL, USA). Independent sample t-test and one-way ANOVA were used to detect statistically significant differences. Statistical significance was set at P<0.05.
Results
Characterization of NSPTi implants
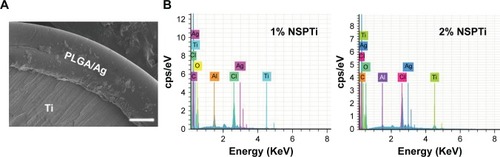
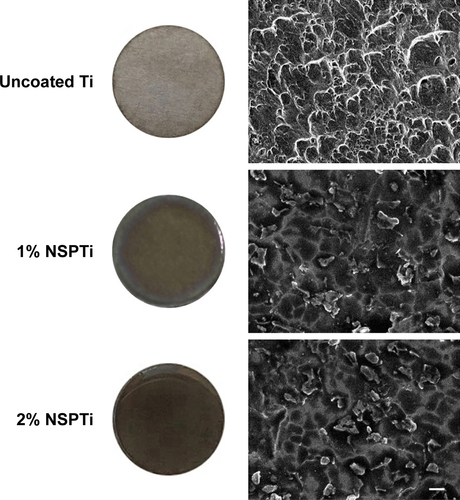
NSPTi implants were obtained by repeated incubations of titanium in nanosilver/PLGA-chloroform solution. A uniform layer (46.23±0.06 µm thickness as shown in , and ) of nanosilver/PLGA coating was formed on the surface of the titanium implant samples. SEM showed that deposition or clusters of silver nanoparticles were not observed in the coating to contain up to 2 wt% (2% NSPTi) (, and ). EDS line scan was performed across the nanosilver/PLGA coatings to determine the element distribution in the coatings (). The elemental analysis by EDS indicated the presence of Ag within the nanosilver/PLGA coatings (), and the content of Ag in the coating is 0.95 and 1.93 wt% for the 1% NSPTi and 2% NSPTi coatings, respectively ().
Table 1 Composition of nanosilver/PLGA coatings, as determined using EDS
Figure 1 (A) Light microscope images of NSPTi samples. (B) SEM images of NSPTi samples (preinsert and postinsert).
Notes: A uniform layer of silver nanoparticle/PLGA coating was observed on the surface of the titanium sample. The thickness of the nanosilver/PLGA coating was 46.23±0.06 µm. Placing NSPTi samples into the prereamed intramedullary canal did not considerably damage the coating. White scale bar =100 µm.
Abbreviations: NSPTi, nanosilver/poly (dl-lactic-co-glycolic acid)-coated titanium; PLGA, poly (dl-lactic-co-glycolic acid); SEM, scanning electron microscopy.
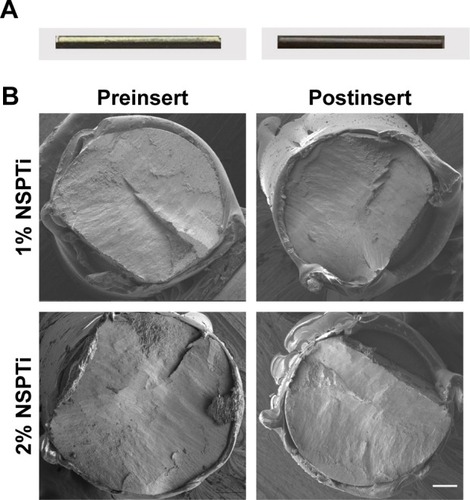
Figure 2 EDSscanning along the cross-section of nanosilver/PLGAcoating (A). Elements in nanosilver/PLGAcoatings detected by EDS(B). White scale bar =20 μm.
Abbreviations: EDS, energy-dispersive spectroscopy; NSPTi, nanosilver/poly (dl-lactic-co-glycolic acid)-coated titanium; PLGA, poly (dl-lactic-co-glycolic acid).
Ag release kinetics
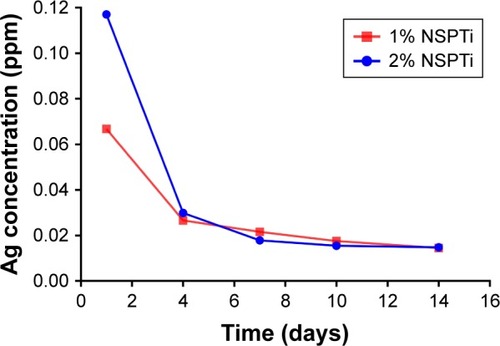
Ag release from the NSPTi samples (1% NSPTi and 2% NSPTi) was monitored once the samples were exposed to PBS (pH 7.4). shows the amount of detected Ag in the resulting PBS solutions, where the NSPTi samples were incubated in darkness. For two NSPTi sample groups, the concentration of released Ag followed the same pattern, although the absolute value is dependent on the Ag inside the nanosilver/PLGA coatings. Specifically, the release was significant at the initial 4 days of incubation. The rate of release started to decrease after day 4 and it became negligible after day 10 (). The maximum amount of released Ag was 0.067 and 0.117 ppm for the 1% NSPTi and 2% NSPTi samples, respectively, at day 1. At the plateau stage after 10 days, the amount of released Ag was 0.014 ppm per day. After 14 days’ incubation, ~82% (1.66 mg) and 73% (2.964 mg) silver released from the 1% NSPTi and 2% NSPTi samples, respectively.
Figure 3 Noncumulative silver release profiles from NSPTi samples (1% NSPTi and 2% NSPTi) into PBS.
Abbreviation: NSPTi, nanosilver/poly (dl-lactic-co-glycolic acid)-coated titanium.
Antibacterial tests in vitro
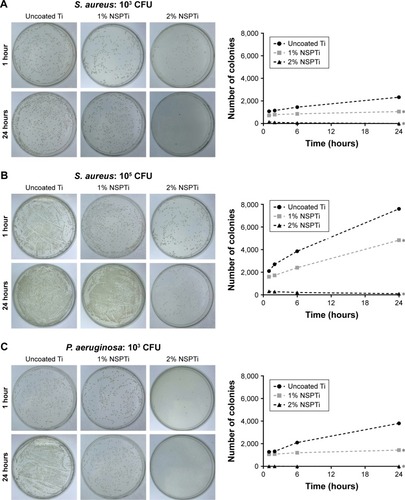
Antibacterial experiments in vitro indicated that the uncoated Ti control did not inhibit bacterial adhesion or proliferation, while nanosilver-concentration-dependent bactericidal behavior was observed in the NSPTi samples (1% NSPTi and 2% NSPTi). When uncoated titanium was incubated with 103 CFU of either MRSA or PAO-1, ~98% of the bacteria initially adhered to the sample in 1 hour, and bacteria proliferated significantly with time (). The initial adhesion of 103 CFU MRSA or PAO-1 to 2% NSPTi samples was <10% (); after 24 hours of incubation, only limited bacterial colonies were observed (). The 1% NSPTi implant group slightly reduced the initial adhesion of 103 CFU MRSA or PAO-1 and significantly inhibited their proliferation. When the initial inoculum of both species was 105 CFU, ~2×103 bacteria initially adhered to the uncoated Ti control samples and proliferated with incubation time (). In the 2% NSPTi group incubated with 105 CFU MRSA or PAO-1, the bacteria initially adhered to the samples was ~1.6×103, and their proliferation decreased markedly (). In contrast, initial bacterial adhesion to the 2% NSPTi samples was significantly inhibited and <1% of adhered bacteria survived after 24 hours, although the initial inoculum of MRSA or PAO-1 was increased to 105 CFU ().
Figure 4 In vitro bacterial colonization analysis of MRSA (A and B) and PAO-1 (C and D).
Notes: The antimicrobial activity of uncoated Ti and NSPTi samples against 103 and 105 CFU bacterial strains was evaluated. N=6, and * indicates a significant difference compared with uncoated Ti (P<0.05). Error bars were too small to show.
Abbreviations: CFU, colony-forming units; MRSA, methicillin-resistant Staphylococcus aureus; NSPTi, nanosilver/poly (dl-lactic-co-glycolic acid)-coated titanium; PAO, Pseudomonas aeruginosa; S. aureus, Staphylococcus aureus; Ti, titanium.

Osteogenic activity of NSPTi implants in vitro
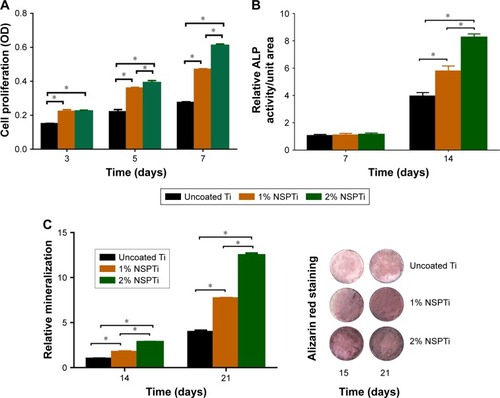
CCK-8 assay was carried out to compare MC3T3-E1 cell proliferation on the uncoated Ti and NSPTi samples quantitatively, which suggested that cellular toxicity was not a concern (). Briefly, MC3T3-E1 cell proliferation in NSPTi groups increased with increasing nanosilver concentrations (). Up to 2% silver particles in NSPTi samples (2% NSPTi) did not reduce MC3T3-E1 cell growth but improved cell proliferation. In addition, NSPTi samples with higher nanosilver concentrations promoted cell proliferation more effectively (). As shown in , proliferation of MC3T3-E1 cells on the 2% NSPTi sample was 1.51, 1.78, and 2.22 times that on the uncoated Ti control after 3, 5, and 7 days of incubation in osteogenic medium, respectively. To investigate the NSPTi effect on osteoblastic differentiation, the ALP activity of MC3T3-E1 cells was quantified after 7 and 14 days as shown in . The ALP activity of MC3T3-E1 cells in each group on day 14 increased dramatically compared with that on day 7. Compared with the uncoated Ti control, NSPTi samples with higher nanosilver concentrations promoted the ALP activity of cell more effectively. As shown in , after 15 and 21 days culture in osteogenic medium, there was obviously more matrix mineralization on the NSPTi samples than on the uncoated Ti control, suggesting that NSPTi samples also significantly increased the terminal differentiation of MC3T3-E1 cells. On day 21, the matrix mineralization of cells on the 2% NSPTi sample was 2.15 times greater than that on the uncoated Ti control ().
Figure 5 In vitro osteoinductive activity of NSPTi.
Notes: NSPTi significantly promoted MC3T3-E1 cell proliferation (A), ALP activity (B), and mineralization (C). Data were normalized to the uncoated Ti control on day 7 (B) and on day 14 (C). N=6, *P<0.05.
Abbreviations: N, number; NSPTi, nanosilver/poly (dl-lactic-co-glycolic acid)-coated titanium; OD, optical density; Ti, titanium.
Clinical evaluation
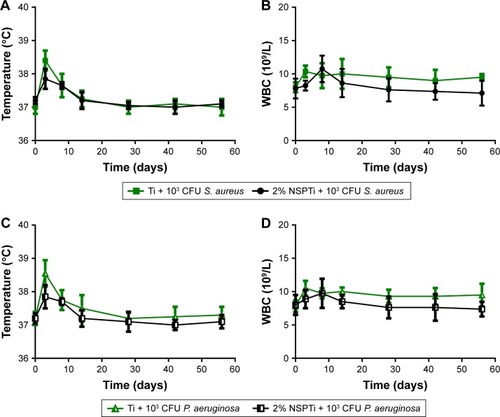
Three rabbits in uncoated Ti groups died on days 2 and 8 because of diarrhea and infection, respectively. Four rabbits in the uncoated Ti group showed infection at the surgical site, and there was no significant infection in animals in the 2% NSPTi group. The body temperature in all groups increased significantly during the initial 3 days, then started to decrease gradually from days 3 to 14, and remained relatively constant until day 56. On day 3, the body temperature in the 2% NSPTi group was lower than that in the uncoated Ti group, while there was no notable difference between the uncoated Ti and NSPTi groups from then until day 56 (). The WBC count of rabbits in the uncoated Ti group grew gradually during the initial 3 days, but the levels subsequently dropped from days 8 to 56. By contrast, in the 2% NSPTi group, the WBC count increased gradually in the first 8 days, followed by a sustainable decline from days 8 to 56 (). Generally, on days 3, 28, 42, and 56, the WBC count in the 2% NSPTi group was less than that in the uncoated Ti group (P<0.05).
Figure 6 Change patterns of the body temperature (A and C) and WBC (B and D) in rabbits from day 0 to day 56. MRSA or PAO-1 in 100 µL sterile PBS (105 CFU) was injected into the tibial canals of rabbits after implantation for bacterial invasion. N=8.
Abbreviations: CFU, colony-forming units; MRSA, methicillin-resistant Staphylococcus aureus; N, number; NSPTi, nanosilver/poly (dl-lactic-co-glycolic acid)-coated titanium; PAO, Pseudomonas aeruginosa; S. aureus, Staphylococcus aureus; Ti, titanium; WBC, white blood cell.
Radiographic and CT analysis
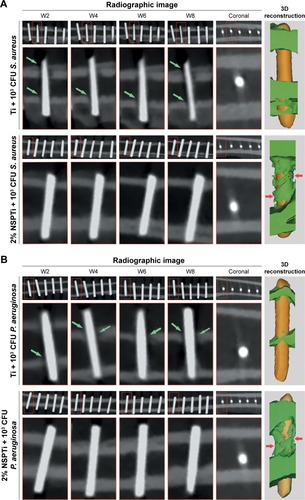
Eight weeks after implantation, radiographic analysis revealed little bone formation in the tibial canals injected with bacteria in the uncoated Ti group. In addition, there was a significant bone destruction in the tibial canals of rabbits in the infected uncoated Ti group (). In contrast, no signs of osteolysis were observed in the infected 2% NSPTi group. Three-dimensional CT reconstruction images showed newly formed bone in the tibial canals of rabbits surrounding the 2% NSPTi implants (). – confirmed these results.
Figure 7 Radiographic images and reconstruction images of infected Ti (A) and 2%-NSPTi implants (B) in the tibial canals of rabbits.
Notes: MRSA or PAO-1 in 100 µL sterile PBS (104 CFU/mL) was injected into the tibial canals after implantation. There was significant bone destruction (green arrows) in the tibial canals of rabbits in the infected uncoated Ti group. No obvious radiographic signs of bone formation were observed in the infected uncoated Ti group up to 8 weeks postsurgery, while in the infected 2% NSPTi group, significant bone formation surrounding 2% NSPTi implants was observed (red arrows). In addition, no bone destruction was observed in the infected 2% NSPTi group.
Abbreviations: CFU, colony-forming units; MRSA, methicillin-resistant Staphylococcus aureus; NSPTi, nanosilver/poly (dl-lactic-co-glycolic acid)-coated titanium; PAO, Pseudomonas aeruginosa; S. aureus, Staphylococcus aureus; Ti, titanium.
Microbiological evaluation in vivo
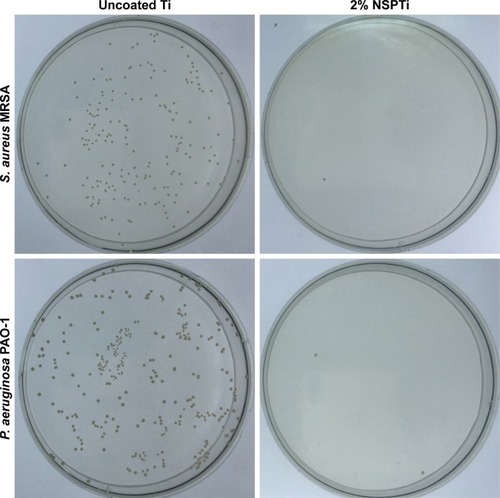
The average CFU/g ratios in the 2% NSPTi group injected with 103 CFU MRSA and PAO-1 were 1.50±0.68 and 1.75±0.6, respectively. In the uncoated Ti group, the ratios were 1.03±0.82×103 and 0.94±0.49×103, respectively. Bacterial colonization in the 2% NSPTi group was significantly less than that in the uncoated Ti group (P<0.05; ).
Figure 8 Bacterial colony formation of tibial bone tissues.
Note: Bacterial colonization in the 2% NSPTi group was significantly lower than those in uncoated Ti group.
Abbreviations: MRSA, methicillin-resistant Staphylococcus aureus; NSPTi, nanosilver/poly (dl-lactic-co-glycolic acid)-coated titanium; PAO, Pseudomonas aeruginosa; S. aureus, Staphylococcus aureus; Ti, titanium.
Histological results
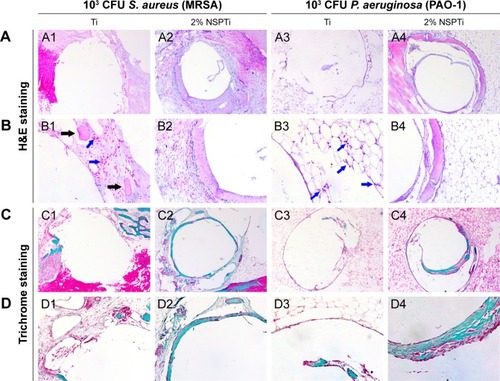
Histological sections of tibia bone samples were subjected to H&E and Masson’s trichrome staining to visualize and assess the new bone formation. Eight weeks after implantation, signs of inflammation () were evident around uncoated Ti implants in the tibial canals with 103 CFU MRSA or PAO-1. No apparent evidence of bone formation was present around the uncoated Ti implants in the infected tibial canals of rabbits (), and the result was in accordance with radiographic analysis. In contrast, significant newly formed bone appeared around 2% NSPTi implants under the same processing conditions 8 weeks after implantation (). Moreover, minimal inflammatory cell infiltration was detected around 2% NSPTi implants, which indicated that 2% NSPTi implants significantly prevented bacterial colonization and did not induce obvious inflammatory responses in vivo. No significant nanosilver toxicity was found in the 2% NSPTi group. Taken together, 2% NSPTi implants exhibited significant antibacterial properties and osteoinductivity in vivo due to the presence of nanosilver in a concentration-dependent manner.
Figure 9 Histological analysis of Ti and 2% NSPTi implants in tibial bone tissues at 8 weeks after implantation; 103 CFU MRSA or PAO-1 in 100 µL sterile PBS (104 CFU/mL) was injected into the canal before implantation.
Notes: H&E staining (A and B) suggested acute or chronic presence of inflammatory cells (blue arrows) with intramedullary abscesses and necrotic disintegrating bone fragments (black arrows) in the intramedullary tissue around uncoated Ti implants, while 2% NSPTi implants showed no apparent signs of bone infection. Consistent with the radiographic analysis, there was little bone formation around uncoated Ti implants, whereas significant bone formation (red arrows) was observed around 2% NSPTi implants, as shown by H&E staining (A and B) and Masson’s trichrome staining (C and D). A and B were to visualize and assess the new bone formation (A1–A4) and inflammation (B1–B4). C (C1–C4) and D (D1–D4) were used to evaluate new bone collagen. For A, magnification =50×. For B1 and B3, magnification =200×. For B2 and B4, magnification =100×. Column D is magnification of column C. For C, magnification =50×. For D, magnification =100×.
bbreviations: MRSA, methicillin-resistant Staphylococcus aureus; NSPTi, nanosilver/poly (dl-lactic-co-glycolic acid)-coated titanium; PAO, Pseudomonas aeruginosa; S. aureus, Staphylococcus aureus; Ti, titanium.
Discussion
Ag-based compounds and Ag ions are antimicrobial agents against a wide spectrum of bacterial strains, with a low-resistance potential, and hence have been widely employed to treat infections in medical field.Citation28 Nanosilver particles are small in size, have a huge surface-to-volume ratio, possess unique physicochemical properties, and have no charge compared with conventional non-nanoscale silver.Citation34 It has been speculated that several mechanisms are involved in the antibacterial performance of nanosilver. Nanosilver particles inhibit bacterial cell division, leading to cell death by destructing bacterial membrane structures.Citation29 They also cause a bacterial apoptosis-like response by inducing the generation of reactive oxygen species, which can lead to impaired physiological function through oxidative damage to cell macromolecules.Citation31 Most importantly, nanosilver particles are known to elicit antimicrobial properties due to their large surface-to-weight ratio, which in turn provides a larger area for microbial contact. Researches indicated that 5–50 nm silver nanosilver particles have antimicrobial properties against microorganismsCitation32 and that 10–30 nm nanosilver particles effectively suppress pathogens and show no statistically cytotoxicity.Citation39 In this study, 20–30 nm diameter spherical nanosilver particles were utilized.
Several polymers have been used to stabilize nanosilver particles because of their tendency to agglomerate and form large clusters, including polyallylamine,Citation40 polyethylenimine,Citation41 chitosan,Citation42 and poly (vinyl-pyrrolidone).Citation43 By donating electrons, the polymers can bind together with metal particles due to their superior nucleophilic properties.Citation44
The FDA-approved, biocompatible and biodegradable polymer PLGA was chosen for the present research as a delivery system due to its hydrolysable ester bonds, which were subjected to nucleophilic interactions with nanosilver particles.Citation35 PLGA degradation is involved in hydrolytic chain scission and transport of products, which are normal metabolic pathways in the body.
Due to the excellent biocompatibility, nanosilver/PLGA coating do not require surgical removal and could display antibacterial activity without evoking a host immune response. The uniform distribution of nanosilver particles in nanosilver/PLGA coating was facilitated by using the PLGA polymer matrix as a stabilizing system for nanosilver silver. The SEM images show no aggregates of silver nanoparticles in the coatings consisting of up to 2% silver nanoparticles (, and ). In our study, the 2% nanosilver/PLGA coating demonstrated no toxicity to cells (). PLGA, as polymer matrix, can slow down and sustain the release kinetics of bactericides (Ag) in nanosilver/PLGA coating, since high doses of Ag could be detrimental to biocompatibility. The nanosilver/PLGA coating could provide a satisfactory antibacterial protection on Ti implant surface against bacterial infections (). The release of silver was significant at the initial 4 days, followed by active release from days 4 to 10, and then the plateau was observed, which depicts a low but sustained release (). Experiments in in vitro indicated that 2% NSPTi implants significantly inhibited bacterial colonization and bacterial biofilm formation after invasive orthopedic and dental surgery (). For the in vivo studies in the tibial canals of rabbits, 2% NSPTi implants displayed significant antibacterial activity against 103 CFU MRSA or PAO-1 (, and ), which are typical bacteria responsible for invasive tissue infection.Citation22–Citation24 Osteogenic potency has long been highly desirable for the orthopedic and dental implants. Therefore, we tried to assess the osteoinductive properties of NSPTi implants. Interestingly, the results from the ALP and Alizarin red staining assays showed that 2% NSPTi coatings significantly improved cell proliferation and differentiation (). Significant newly formed bone appeared around 2% NSPTi implants in infected rabbit ( and ). The findings indicate that NSPTi implants significantly inhibit bacterial colonization and bacterial biofilm formation due to the presence of silver. Additionally, 2% NSPTi implants markedly improved bone formation although incubated with an initial bacterial inoculum. The osteoinductive properties of NSPTi implants can be explained by the fact that nanosilver inhibits cell division through disrupting multiple components of bacterial structure, function, and metabolism and induces specific effects of cell macromolecules (DNA, protein, lipid, and others) through oxidative damage.Citation27,Citation28
Conclusion
In this study, NSPTi implants exhibited superior antibacterial and osteoinductive activity compared with uncoated titanium implants, which make NSPTi implants promising candidates for applications in orthopedic surgery. The concentration of nanosilver in the coating can be higher in further research. Elucidating the mechanism of osteoinductive activity of NSPTi implants is essential in further research.
Supplementary materials
Videos S1–S4
The supplementary videos include four 3D reconstruction videos of infected titanium and nanosilver/poly (dl-lactic-co-glycolic acid)-coated titanium implants in the rabbits tibial canals. 103 colony-forming units methicillin-resistant Staphylococcus aureus or Pseudomonas aeruginosa in 100 µL sterile PBS (104 colony-forming units/mL) was injected into the canal before implantation.
Video S1 3D reconstruction video of Ti implants in the tibial canals with 103 CFU MRSA.
Notes: There was no bone formation in the tibial canals of rabbits in the infected uncoated Ti group up to 8 weeks postsurgery (video 1 and video 2), while in the infected 2%-NSPTi group, significant bone formation surrounding 2%-NSPTi implants was observed (Videos S3 and S4).
Abbreviations: CFU, colony-forming units; MRSA, methicillin-resistant Staphylococcus aureus; NSPTi, nanosilver/poly (dl-lactic-co-glycolic acid)-coated titanium; Ti, titanium.
Video S2 3D reconstruction video of Ti implants in the tibial canals with 103 CFU PAO-1.
Note: There was no bone formation in the tibial canals of rabbits in the infected uncoated Ti group up to 8 weeks postsurgery (Videos S1 and S2), while in the infected 2%-NSPTi group, significant bone formation surrounding 2%-NSPTi implants was observed (Videos S3 and S4).
Abbreviations: CFU, colony-forming units; NSPTi, nanosilver/poly (dl-lactic-co-glycolic acid)-coated titanium; PAO-1, Pseudomonas aeruginosa; Ti, titanium.
Video S3 3D reconstruction video of 2%-NSPTi implants in the tibial canals with 103 CFU MRSA.
Note: There was no bone formation in the tibial canals of rabbits in the infected uncoated Ti group up to 8 weeks postsurgery (Videos S1 and S2), while in the infected 2%-NSPTi group, significant bone formation surrounding 2%-NSPTi implants was observed (Videos S3 and S4).
Abbreviations: CFU, colony-forming units; MRSA, methicillin-resistant Staphylococcus aureus; NSPTi, nanosilver/poly (dl-lactic-co-glycolic acid)-coated titanium; Ti, titanium.
Video S4 3D reconstruction video of 2%-NSPTi implants in the tibial canals with 103 CFU PAO-1.
Note: There was no bone formation in the tibial canals of rabbits in the infected uncoated Ti group up to 8 weeks postsurgery (Videos S1 and S2), while in the infected 2%-NSPTi group, significant bone formation surrounding 2%-NSPTi implants was observed (Videos S3 and S4).
Abbreviations: CFU, colony-forming units; NSPTi, nanosilver/poly (dl-lactic-co-glycolic acid)-coated titanium; PAO-1, Pseudomonas aeruginosa; Ti, titanium.
Figure S1 SEM images of uncoated Ti and NSPTi samples.
Notes: There were no silver nanoparticle clusters in the nanosilver/PLGA coatings. White scale bars =5 µm.
Abbreviations: NSPTi, nanosilver/poly (dl-lactic-co-glycolic acid)-coated titanium; PLGA, poly (dl-lactic-co-glycolic acid); SEM, scanning electron microscopy; Ti, titanium.
Acknowledgments
This study was supported by the National Natural Science Fund of China (81701008), the Natural Science Foundation of Shandong Province (BS2015YY027, ZR2018LH012), the China Postdoctoral Science Foundation (2014M561941), Special Funds for Postdoctoral Innovation Projects of Shandong Province (201402030), and the Fundamental Research Funds of Shandong University (2016GN009). No benefits in any form have been received or will be received from any commercial party related directly or indirectly to the subject of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
- BakhshandehSGorgin KarajiZLietaertKSimultaneous delivery of multiple antibacterial agents from additively manufactured porous biomaterials to fully eradicate planktonic and adherent Staphylococcus aureusACS Appl Mater Interfaces2017931256912569928696671
- MullerAEPuntNMoutonJWOptimal exposures of ceftazidime predict the probability of microbiological and clinical outcome in the treatment of nosocomial pneumoniaJ Antimicrob Chemother201368490090623190766
- GiavaresiGBorsariVFiniMPreliminary investigations on a new gentamicin and vancomycin-coated PMMA nail for the treatment of bone and intramedullary infections: an experimental study in the rabbitJ Orthop Res200826678579218186130
- CroesMBakhshandehSvan HengelIAJAntibacterial and immunogenic behavior of silver coatings on additively manufactured porous titaniumActa Biomater20188131532730268917
- DarouicheROTreatment of infections associated with surgical implantsN Engl J Med2004350141422149915070792
- TanYLeonhardMMoserDMaSSchneider-SticklerBLong-term antibiofilm activity of carboxymethyl chitosan on mixed biofilm on siliconeLaryngoscope201612612E404E40827346839
- HegdeVDworskyEMStavrakisAISingle-dose, preoperative vitamin-D supplementation decreases infection in a mouse model of periprosthetic joint infectionJ Bone Joint Surg Am201799201737174429040128
- RioolMde BreijADrijfhoutJWNibberingPHZaatSAJAntimicrobial peptides in biomedical device manufacturingFront Chem201756328971093
- UppuluriPBusscherHJChakladarJvan der MeiHCChaffinWLTranscriptional profiling of C. albicans in a two species biofilm with Rothia dentocariosaFront Cell Infect Microbiol2017731128752078
- StewartPSWilliam CostertonJAntibiotic resistance of bacteria in biofilmsLancet2001358927613513811463434
- DonlanRMBiofilms: microbial life on surfacesEmerg Infect Dis20028988189012194761
- ZilbermanMElsnerJJAntibiotic-eluting medical devices for various applicationsJ Control Release2008130320221518687500
- TruongVKPhamVTMedvedevASelf-organised nanoarchitecture of titanium surfaces influences the attachment of Staphylococcus aureus and Pseudomonas aeruginosa bacteriaAppl Microbiol Biotechnol201599166831684025895086
- BatoniGMaisettaGEsinSAntimicrobial peptides and their interaction with biofilms of medically relevant bacteriaBiochim Biophys Acta2016185851044106026525663
- KarguptaRBokSDarrCMCoatings and surface modifications imparting antimicrobial activity to orthopedic implantsWiley Interdiscip Rev Nanomed Nanobiotechnol20146547549524867883
- EspositoSLeoneSProsthetic joint infections: microbiology, diagnosis, management and preventionInt J Antimicrob Agents200832428729318617373
- RabinNZhengYOpoku-TemengCduYBonsuESintimHOBiofilm formation mechanisms and targets for developing antibiofilm agentsFuture Med Chem20157449351225875875
- DarouicheROAntimicrobial approaches for preventing infections associated with surgical implantsClin Infect Dis200336101284128912746774
- LiHBidzilyaOVReview of the genus Gnorimoschema Busck, 1900 (Lepidoptera, Gelechiidae) in ChinaZootaxa20174365217319529686216
- NieBLongTAoHZhouJTangTYueBCovalent immobilization of enoxacin onto titanium implant surfaces for inhibiting multiple bacterial species infection and in vivo methicillin-resistant Staphylococcus aureus infection prophylaxisAntimicrob Agents Chemother2016611e017661627799220
- AntociVKingSBJoseBVancomycin covalently bonded to titanium alloy prevents bacterial colonizationJ Orthop Res200725785886617415753
- ChenRWillcoxMDHoKKSmythDKumarNAntimicrobial peptide melimine coating for titanium and its in vivo antibacterial activity in rodent subcutaneous infection modelsBiomaterials20168514215126871890
- AtefyektaSErcanBKarlssonJAntimicrobial performance of mesoporous titania thin films: role of pore size, hydrophobicity, and antibiotic releaseInt J Nanomedicine20161197799027022263
- CampocciaDMontanaroLArciolaCRThe significance of infection related to orthopedic devices and issues of antibiotic resistanceBiomaterials200627112331233916364434
- NandaASaravananMBiosynthesis of silver nanoparticles from Staphylococcus aureus and its antimicrobial activity against MRSA and MRSENanomedicine20095445245619523420
- MekkawyAIEl-MokhtarMANafadyNAIn vitro and in vivo evaluation of biologically synthesized silver nanoparticles for topical applications: effect of surface coating and loading into hydrogelsInt J Nanomedicine20171275977728176951
- EckhardtSBrunettoPSGagnonJPriebeMGieseBFrommKMNanobio silver: its interactions with peptides and bacteria, and its uses in medicineChem Rev201311374708475423488929
- TianXJiangXWelchCBactericidal effects of silver nanoparticles on lactobacilli and the underlying mechanismACS Appl Mater Interfaces201810108443845029481051
- BondarenkoOMSihtmäeMKuzmičiovaJRagelienėLKahruADaugelavičiusRPlasma membrane is the target of rapid antibacterial action of silver nanoparticles in Escherichia coli and Pseudomonas aeruginosaInt J Nanomedicine2018136779679030498344
- SilverSPhungLetSilverGSilver as biocides in burn and wound dressings and bacterial resistance to silver compoundsJ Ind Microbiol Biotechnol200633762763416761169
- LeaperDJSilver dressings: their role in wound managementInt Wound J20063428229417199764
- WoodmanseyEJRobertsCDAppropriate use of dressings containing nanocrystalline silver to support antimicrobial stewardship in woundsInt Wound J20181561025103230117675
- ShevlinDO’BrienNCumminsESilver engineered nanoparticles in freshwater systems – likely fate and behaviour through natural attenuation processesSci Total Environ20186211033104629079093
- HouchinMLToppEMChemical degradation of peptides and proteins in PLGA: a review of reactions and mechanismsJ Pharm Sci20089772395240417828756
- ThomaidisPCPantazatouAKamariotisSSonication assisted microbiological diagnosis of implant-related infection caused by Prevotella disiens and Staphylococcus epidermidis in a patient with cranioplastyBMC Res Notes20158130726183701
- LiuDHeCLiuZXuWGentamicin coating of nanotubular anodized titanium implant reduces implant-related osteomyelitis and enhances bone biocompatibility in rabbitsInt J Nanomedicine2017125461547128814863
- WangGZhengLZhaoHIn vitro assessment of the differentiation potential of bone marrow-derived mesenchymal stem cells on genipin-chitosan conjugation scaffold with surface hydroxyapatite nanostructure for bone tissue engineeringTissue Eng Part A2011179–101341134921247339
- SehgalRRCarvalhoEBanerjeeRStiffMMechanically stiff, zinc cross-linked nanocomposite scaffolds with improved osteostimulation and antibacterial propertiesACS Appl Mater Interfaces2016822137351374727176647
- VenugopalAMuthuchamyNTejaniHIncorporation of silver nanoparticles on the surface of orthodontic microimplants to achieve antimicrobial propertiesKorean J Orthod201747131028127534
- DotzauerDMDaiJSunLBrueningMLCatalytic membranes prepared using layer-by-layer adsorption of polyelectrolyte/metal nanoparticle films in porous supportsNano Lett20066102268227217034095
- KuoPLChenWFHuangHYChangICDaiSAStabilizing effect of pseudo-dendritic polyethylenimine on platinum nanoparticles supported on carbonJ Phys Chem B200611073071307716494311
- ErcanBKummerKMTarquinioKMWebsterTJDecreased Staphylococcus aureus biofilm growth on anodized nanotubular titanium and the effect of electrical stimulationActa Biomater2011773003301221515421
- TravanAPelilloCDonatiINon-cytotoxic silver nanoparticle-polysaccharide nanocomposites with antimicrobial activityBiomacromolecules20091061429143519405545
- ShibataTTostmannHBunkerBXAFS studies of gold and silver-gold nanoparticles in aqueous solutionsJ Synchrotron Radiat20018Pt 254554711512845