Abstract
Purpose
To determine the role of duplex Doppler ultrasonography (DDU) in patients with acute unilateral renal obstruction.
Subjects and methods
A total of 161 patients with suspected renal colic due to urolithiasis were evaluated by DDU followed by intravenous urography (IVU). The mean intra-arterial resistive index (RI) and the difference of mean resistive index between both kidneys (delta RI) were determined for each person. An RI value of ≥0.70 and a delta RI value of ≥0.06 were taken as the discriminatory threshold for obstruction. IVU results were considered the “ reference standard” against which renal DDU findings were compared.
Results
IVU showed both kidneys to be normal in 51 patients and with unilateral ureteric obstruction in 110 patients. The mean RI for obstructed kidneys was 0.67 (0.048), which was significantly higher (P-value <0.05) than a mean RI of contralateral normal kidneys 0.59 (0.04). The mean delta RI in patients with unilateral ureteric obstruction was significantly higher than that in patients with normal kidneys, at 0.076 (0.03) and 0.03 (0.05), respectively. In patients with complete obstruction, sensitivity of RI and delta RI were 77.5% and 92.5% with a specificity of 84.3% and 90.1%, respectively. In patients with partial obstruction, the sensitivity of these values was 22.8% and 62.8% with a specificity of 84.3% and 90.1%.
Conclusion
Delta RI is more sensitive and specific than RI in acute renal obstruction. However, due to relatively low sensitivity for detection of partial obstruction, DDU cannot replace IVU as the standard imaging technique.
Introduction
Renal colic is one of the most common problems in urologic practice.Citation1 Renal obstruction due to urolithiasis is the most frequent cause.Citation2,Citation3 It is more common in males at 6.1% than in females at 5.3%.Citation4 Early and accurate diagnosis is essential to minimize the devastating effects of obstruction on urinary tract structure and function.Citation5 Although intravenous urography (IVU) is still used as the standard investigation in Pakistan, it has its limitations. An abdominal x-ray (kidneys, ureters, and bladder) coupled with ultrasonography of the urinary tract is performed as an alternative method in many hospitals.Citation2,Citation6
Plain abdominal radiography has very low sensitivity for the detection of urolithiasis.Citation7 Grayscale ultrasonography may reveal a stone in the collecting system or it may suggest obstructive uropathy by demonstrating a dilatation of the urinary tract.Citation8 However, it often fails to differentiate between obstructive and nonobstructive dilatation.Citation3,Citation9 It may also be equivocal in early obstruction without significant dilatation.Citation5,Citation9 Furthermore, it does not provide functional data regarding the obstruction.Citation2 Intrarenal duplex Doppler ultrasonography (DDU) has been proposed as a possible noninvasive, adjunctive test in distinguishing between obstructive and nonobstructive pelvicaliceal dilatation,Citation2,Citation3 with the resistive index (RI) and delta resistive index (delta RI) being the variables most widely measured.Citation1,Citation10 The rationale for its use is a change in renal hemodynamic mediated by certain vasoactive mediators due to obstruction.Citation11,Citation12 As this occurs in the obstructed kidney, the RI of only the obstructed kidney is elevated. Thus, the difference of mean RI between the obstructed and normal contralateral kidney is also significantly elevated in the setting of acute urinary obstruction, which is measured as delta RI.Citation5,Citation13
This study was carried out to evaluate the efficacy of duplex Doppler ultrasound in the diagnosis of renal obstruction in patients with renal colic by taking IVU findings as the gold standard. The results were evaluated statistically, and comparison with several previous studies was made in terms of outcome and the factors contributing to it. On the basis of the results, conclusions were derived about the future utility of renal duplex Doppler sonography in the evaluation of renal colic due to renal obstruction.
Subjects and methods
Over a period of 1 year, 161 patients who presented with a complaint of acute unilateral flank pain radiating to the groin were evaluated. The DDU results were compared with IVU findings as a gold standard reference. There were 108 male and 53 female patients. The age range of the patients was from 18 years to 50 years (mean age 32.5 years). This was a cross-sectional, validational study. The sample technique used was nonprobability, purposive type.
Informed consent was taken from all the patients after explaining the study’s purpose, procedure, and risk-benefit ratio, and approval of the ethical committee was given. History was taken in each case, especially about the side of renal colic, duration of symptoms, pre-existing renal disease, and ingestion of nonsteroidal anti-inflammatory drugs (NSAIDs). Patients who had pre-existing renal disease, bilateral flank pain, and solitary kidneys were excluded from the study in order to control confounding variables.
All patients were examined in supine and lateral positions by a single machine (Aloka GmbH, Model No. SOP-4000-10B, Meerbusch, Germany) with a curvilinear transducer of 3.5–5 MHz. Doppler waveforms were recorded from interlobar and arcuate arteries at the upper, middle, and lower portions, first over the obstructed kidney and then over the contralateral kidney. The lowest possible pulse repetition frequency without aliasing and the highest possible gain were used. The Doppler sample width was set at 2–5 mm. The renal RI was calculated by subtracting the peak diastolic velocity from the peak systolic velocity and dividing the result by the peak systolic velocity. Mean RI and difference in mean RI of the obstructed and contralateral kidneys (delta RI) were also determined. A renal RI ≥0.7 and a delta RI ≥0.06 were considered as diagnostic of obstructive uropathy.
All patients then subsequently underwent an IVU examination, which was considered negative with a normal renoureteric unit and positive with pylocaliectasis proximal to a ureteric stone, or with delayed contrast excretion. The patients with persistent dense nephrogram or significantly delayed nephrogram were diagnosed as having complete urinary obstruction. The patients with nondelayed or slightly delayed nephrogram in the presence of obstructing calculus were diagnosed as having partial urinary obstruction. The IVU results were considered the “reference standard” against which DDU findings were compared.
Data were initially collected on Performa, which was then shifted to SPSS. Statistical analysis was performed with SPSS software (IBM SPSS statistics v 17; SPSS, Inc, Chicago, IL). Relationships between RI values, urinary calculi location, and the degree of obstruction were evaluated. All the graphs and charts were obtained on SPSS. Later, using the 2 × 2 table, sensitivity, specificity, positive predictive value, and negative predictive values of RI and delta RI were calculated, taking IVU findings as the gold standard.
Results
A total of 161 patients who fulfilled the inclusion criteria were included in the study. There were 108 (67.1%) males and 53 (32.9%) females of mean age 32.5 years (range 18–50 years). In 51 patients, IVU showed that both kidneys are normal with no signs of obstructive uropathy, and the cause of loin pain was considered nonurological. In 110 patients, IVU showed evidence of unilateral ureteric obstruction due to urolithiasis with normal contralateral kidney. Patients with acute unilateral ureteric obstruction were further classified into two groups, the first comprising 40 patients who showed evidence of complete ureteral obstruction, and the second comprising 70 patients who showed evidence of partial obstruction.
The mean RI for obstructed kidneys was 0.67 (0.048), which was significantly higher (P-value <0.05) than the mean RI of contralateral normal kidneys 0.59 (0.04).
The mean delta RI of patients with acute unilateral ureteric obstruction was significantly higher than the mean delta RI of patients in whom both kidneys were normal, at 0.07 (0.03) and 0.03 (0.05), respectively (P-value <0.05).
By taking an RI value of ≥0.70 as a discriminatory level for obstruction, the overall sensitivity of RI was 42.7% and specificity 84.3%. In patients with complete obstruction the sensitivity of RI was 77.5% and specificity 84.3%, whereas in patients with partial obstruction the sensitivity of RI was 22.8% and specificity 84.3% ().
Figure 1 Sensitivity and specificity of resistive index (RI) and delta RI in partial urinary obstruction.
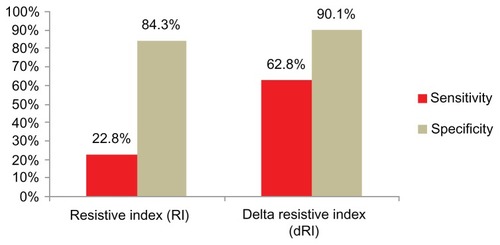
By taking a delta RI value of ≥0.06 as a discriminatory level for obstruction, the overall sensitivity of delta RI was 73.6% and specificity 90.1%. In patients with complete obstruction the sensitivity of delta RI was 92.5% and specificity 90.1%, whereas in patients with partial obstruction the sensitivity of delta RI was 62.8% and specificity 90.1%.
The positive and negative predictive values of RI in patients with complete urinary obstruction were 79.4% and 82.64%, and those of delta RI were 88.09% and 93.87%, respectively. The positive and negative predictive values of RI in patients with partial urinary obstruction were 66.67% and 42.14%, and those of delta RI were 89.79% and 63.89%, respectively.
In the 51 healthy individuals without renal obstruction (102 kidneys) the average RI and delta RI were 0.60 (0.05) and 0.03 (0.02), respectively. The RI was above 0.70 in eight healthy individuals, whereas delta RI was above 0.06 in five healthy individuals.
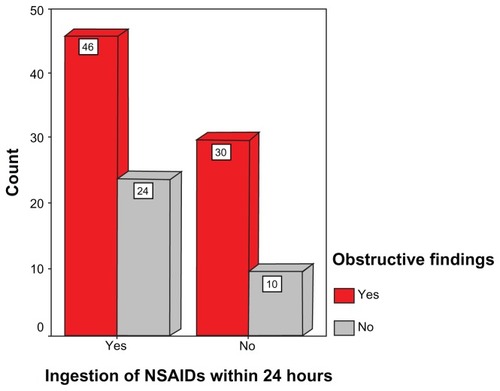
Of 110 patients, 70 (63.6%) had taken NSAIDs within the last 24 hours, whereas 40 (36.6%) had not. In 70 patients who had taken NSAIDs, RI showed obstruction in 20 (28.5%) patients. In another 40 who had not taken NSAIDs, RI showed obstruction in 27 (67.5%). Delta RI showed obstruction in 49 (68.5%) out of 70 patients with NSAID ingestion and 33 (82.5%) out of 40 patients without NSAID ingestion.
Seventy-one patients had a stone on the right side, whereas 39 had one on the left side. The distribution of urolithiasis according to location in the obstructive group was renal in eight patients (7.3%), ureteropelvic junction and proximal ureter in 30 patients (27.3%), midureteral in 24 patients (21.8%), and distal ureteral including uretrovesical junction in 48 patients (43.6%) of the cases, as shown in .
Table 1 Site of stone in the urinary tract of patients with unilateral ureteric obstruction
Dilatation of the pyelocaliceal system was mild in 74 patients (69.1%), moderate in 22 patients (20%), and severe in two patients (1.8%). Twelve patients (10.9%) had no pyelocaliceal dilatation, as shown in .
Table 2 Degree of pyelocaliceal dilatation on the side of urinary obstruction
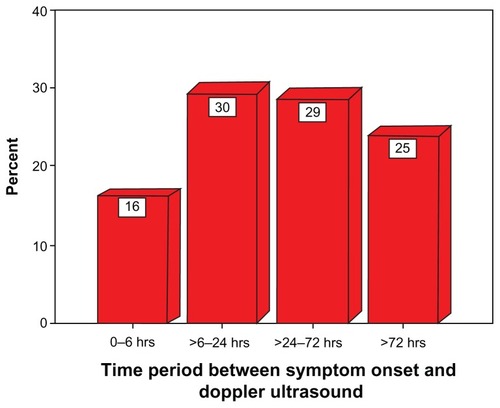
When the patients were classified according to pain duration, 18 patients (16.4%) presented within the first 6 hours, 35 patients (31.8%) between 6 hours and 24 hours, 32 patients (29.1%) between 25 hours and 72 hours, and 25 patients (22.7%) after 72 hours ().
Figure 2 Time period between symptom onset and Doppler ultrasound of the obstructed patients.
Discussion
IVU and grayscale sonography have been the two most common imaging modalities used in patients with acute renal colic to detect calculi and obstruction.Citation1,Citation5 More recently, helical computed tomography has also been used for the detection of calculi and obstruction.Citation6 IVU is not a very safe technique; it carries the risks of irradiation as well as complications in reaction to contrast material injection.Citation3,Citation5 Although grayscale renal ultrasonography can reliably detect collecting system dilatation, it is often not possible to differentiate obstructive and nonobstructive pyelocaliectasis on grayscale sonography alone.Citation8,Citation16 As prolonged renal obstruction induces hormonal alterations and thereby causes diffuse vasoconstriction of the vascular bed, the visualization of different patterns of blood flow is helpful in differentiating obstructive from nonobstructive pyelocaliectasis.Citation1,Citation2,Citation5 The availability of duplex Doppler sonography is apparently an attractive and well-reproducible adjunct to the partly invasive diagnostic procedures commonly used in the radiological assessment of renal obstruction.Citation5,Citation8,Citation14,Citation15
In the past two decades, previous investigators have reported somewhat conflicting results regarding the additional information from duplex Doppler sonography over grayscale sonography for the diagnosis of acute urinary tract obstruction.Citation3,Citation6,Citation16–Citation18 In the late 1980s, Plat et alCitation17 and Sauvain et alCitation19 reported an elevated RI in an obstructed kidney in unilateral ureteric obstruction when a discriminatory RI threshold of ≥0.70 was used. Since then, many researchers have reported an elevated RI in the setting of acute ureteric obstruction.Citation1,Citation5,Citation17,Citation20,Citation21 Shokeir et alCitation22 reported an elevated mean RI of 0.69 in pregnant patients with acute renal colic. More recently, Onur et alCitation1 reported an elevated mean RI of 0.69 in obstructed kidneys. Several researchers, however, have reported disappointing results in cases of acute obstruction.Citation23 In these studies, possible suggested mechanisms causing inaccuracy of Doppler sonography were partial ureteric obstruction, pyelosinus extravasations, and use of NSAIDs, which alter the vasomotor response and thus alter RI.
In our study we found mean RI values of 0.67 and 0.59 in acutely obstructed and nonobstructed kidneys, respectively. The mean delta RI was also significantly elevated with a value of 0.076. These results seem to be compatible with those of Onur et al,Citation1 Shokeir et al,Citation22 and Amin and GhaffarCitation8 but contradict the results of Tublin et alCitation23 and Gurel et al,Citation6 as shown in .
Table 3 Mean resistive index (RI) of obstructed and nonobstructed kidneys (comparison with several previous studies)
Our study showed that elevation of RI and delta RI was related to the degree of ureteric obstruction. In our study the RI was above the 0.70 threshold in 77.5% of cases of complete urinary obstruction and in 22.8% of cases of partial obstruction. Similarly, delta RI was elevated in 92.5% cases of complete obstruction and in 62.8% cases of partial obstruction ( and ). This can be explained by the fact that ureteral pressure in partial obstruction is not sufficiently elevated to induce an increase in renal vascular resistance.Citation5,Citation24 This is consistent with the results of Haroun.Citation5 He found that RI is sensitive in 64% of cases of complete obstruction and in 33% of cases of partial obstruction. DeToledo et alCitation24 found a sensitivity of RI of 91.8% for patients with complete obstruction and 48.1% in patients with partial obstruction with a specificity of 92.8% in respect of the group of normal patients.
Figure 4 (A) Patient presents with acute right sided renal colic. Spectral waveform from the arcuate arteries of the upper pole of right kidney shows elevated RI of 0.714. Spectral waveform from the arcuate arteries of the mid pole of left kidney shows normal RI of 0.55. In this case both RI and delta RI are elevated.
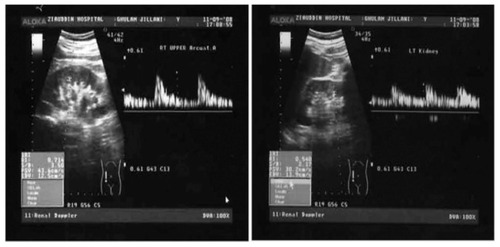
Figure 4 (B) Subsequent IVU of same patient shows complete obstruction on right side due to a distal ureteral calculus.

The present results confirmed that DDU is significantly more sensitive in diagnosing complete renal obstruction than partial obstruction. This also agrees with the results of several other authors.Citation5,Citation16,Citation22
Statistical analysis shows that the sensitivity of RI in the diagnosis of complete urinary obstruction is 77.5% in our study, which is relatively low. When we applied delta RI, sensitivity rose to 92.5% with a specificity of 90% ( and ). This is comparable with the study of Haroun.Citation5 He found the sensitivity of delta RI in complete obstruction to be 100% and specificity to be 89%. In a recent study, Granata et alCitation16 found the sensitivity and specificity of delta RI to be 95% and 98% in complete obstruction, respectively. These findings suggest that delta RI is the value to be measured in acute urinary obstruction.
Figure 5 (A) Patient presents with acute left sided renal colic. Spectral waveform from the arcuate arteries of the both kidneys shows normal RI of 0.60 and 0.68. However delta RI is elevated.
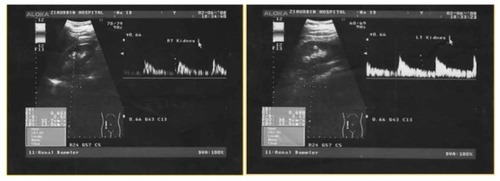
Figure 5 (B) IVU shows partial obstruction at left ureter due to a small calculus at left ureterovescial junction.

Some authors have found that there is a time dependency of increase in RI.Citation23–Citation25 Opdenakker et alCitation25 found that the sensitivity of RI dropped substantially 48 hours after onset of the symptoms. Platt et alCitation17 suggested that kidneys obstructed for >12 hours do not have a significantly higher RI than those with obstruction of shorter duration. On the other hand, deToledo et alCitation24 reported that RI was significantly higher in patients with renal colic duration of >24 hours. This time dependency was not found in our study, however, or in the studies of several other authors.Citation5,Citation26 These differences are possibly due to the duration of obstruction being based on the clinical history in all previous studies.
Cronan and TublinCitation18 first studied the effects of NSAIDs in the management of patients with acute renal colic. In animal models these medications have shown to reverse the vasoconstriction that occurs with acute renal obstruction. Shokeir et alCitation27 found that the sensitivity of RI decreases from 70% to 50% and that of delta RI from 98% to 68% 6 hours after the ingestion of 75 mg diclofenac. In our study, RI showed obstruction in 28.5% of patients who had taken NSAIDs and in 67.5% of patients who had not taken NSAIDs (). A majority of the patients in our study had taken NSAIDs before the Doppler examination. This also explains the overall low sensitivity of RI and delta RI in our study.
Figure 3 Effect of administration of nonsteroidal anti-inflammatory drugs (NSAIDs) on obstructive findings by resistive index.
The level of ureteric obstruction had no significant impact on RI in our study, which is in agreement with Shokeir and AbdulmaaboudCitation26 and Gurel et al.Citation6 However, deToledo et alCitation24 have shown that patients with proximal obstruction had RIs greater than those with distal obstruction.
Several authors have assessed the relationship between degree of pyelocaliceal dilatation and RI.Citation5,Citation6,Citation28 No significant correlation was detected between pyelocaliceal dilatation and RI in our study, which is in agreement with Gurel et al.Citation6 Several studies have demonstrated that RI is affected by factors other than renovascular resistance, such as vascular compliance, age of the patient, plasma rennin levels, diabetes, hypertension, abnormal heart rate, and several other renal diseases. These other factors can explain the elevation of RI and delta RI in patients without renal obstruction. A possible limitation of this study was the indetermination of the types of NSAIDs, because NSAIDs have a wide range of half-lives. Bertolotto et alCitation29 reported that values of renal RI depend on the type of NSAID that has been used to relieve the symptoms.
Conclusion
The study shows that DDU is not a very sensitive test for the diagnosis of partial ureteric obstruction; however, it is sensitive and specific in diagnosing complete ureteric obstruction, particularly if delta RI is applied.
We believe that measurement of delta RI can be used as an adjunctive test along with grayscale ultrasound in patients presenting with acute renal colic. It is particularly more helpful if performed before the administration of NSAIDs.
On the basis of the results, we recommend that DDU should be used in patients in whom IVU is undesirable, such as in pregnant patients and those with a risk of contrast media reaction. However, it cannot replace IVU as a standard diagnostic test.
Disclosure
The authors declare no conflicts of interest in relation to this work.
References
- OnurMRCubukMAndicCKartalMArslanGRole of resistive index in renal colicUrol Res200735630731217957364
- PepePMottaLPennisiMAragonaFFunctional evaluation of the urinary tract by color-Doppler ultrasonography (CDU) in 100 patients with renal colicEur J Radiol20055313113515607864
- GeavletePGeorgescuDCauniVNitaGValue of duplex Doppler ultrasonography in renal colicEur Urol200241717811999470
- SafarinejadMRAdult urolithiasis in a population based study in Iran: prevalence, incidence and associated risk factorsUrol Res2007352738217361397
- HarounADuplex Doppler sonography in patients with acute renal colic: prospective study and literature reviewInt Urol Nephrol20033513514015072483
- GurelSAkataDGurelKOzmenMNAkhanOCorrelation between the renal resistive index (RI) and nonenhanced computed tomography in acute renal colic: how reliable is the RI in distinguishing obstruction?J Ultrasound Med2006251113112016929011
- ChanVOBuckleyOPersaudTTorreggianiWCUrolithiasis: how accurate are plain radiographs?Can Assoc Radiol J200859313113418697719
- AminMUGhaffarAIntrarenal and intravesical color Doppler sonography in patients with acute renal colicJ Surg Pak200494042
- TublinMEBudeROPlattJFThe resistive index in renal Doppler sonography: where do we stand?AJR200318088589212646425
- BatemanGACuganesanRRenal vein Doppler sonography of obstructive uropathyAJR200217892192511906873
- KmetecAPeskar-BabnikDButurovic-PonikvarJTime-dependent changes of resistive index in acute renal obstruction during nonsteroidal drug administrationBJU Int20028984785012010226
- KilicSAltinokMTIpekDBeyturABaydincYCGunesGColor Doppler sonography examination of partially obstructed kidneys associated with ureteropelvic junction stone before and after percutaneous nephrolithotripsy: preliminary reportInt J Urol20051242943515948740
- BrkljacićBKuzmicACDmitrovicRRadosMVidjakVDoppler sonographic renal resistance index and resistance index ratio in children and adolescents with unilateral hydronephrosisEur Radiol2002122747275112386768
- PlattJRubinJEllisJDiPietroMADuplex Doppler US of the kidney; differentiation of obstructive from nonobstructive dilatationRadiology19891715155172649925
- KavakliHSKoktenerAYilmazADiagnostic value of renal resistive index for the assessment of renal colicSingapore Med J201152427127321552789
- GranataAAndrulliSBigiMQPozzoniPFioriniFLogiasFPredictive role of duplex Doppler ultrasonography in the diagnosis of acute renal obstruction in patients with unilateral renal colicClin Nephrol200971668068619473637
- PlattJRubinJEllisJAcute renal obstruction: evaluation with intrarenal duplex Doppler and conventional USRadiology19931866856888430174
- CronanJJTublinMERole of the resistive index in the evaluation of acute renal obstructionAJR Am J Roentgenol199516423773787839973
- SauvainJLPierratVChambersRBui XuanPPalascakPBoursheidDEchography and pulsed Doppler of the arteries of the renal parenchyma in obstructive syndromes and dilatation of the excretory cavities of the kidneyJ Radiol1989706–73893982681725
- BrkljacićBDrinkovićISabljar-MatovinovićMIntrarenal duplex Doppler sonographic evaluation of unilateral native kidney obstructionJ Ultrasound Med19941331972047932977
- SigirciAHallacTAkyncyATemelIGulcanHAslanMRenal interlobar artery parameters with duplex Doppler sonography and correlations with age, plasma renin, and aldosterone levels in healthy childrenAJR200618682883216498115
- ShokeirAAMahranMRAbdulmaaboudMRenal colic in pregnant women: role of renal resistive indexUrology20005534434710699607
- TublinMDoddGVerdileVAcute renal colic: diagnosis with duplex Doppler USRadiology19941936977017972809
- deToledoLSMartinez-BerganzaATCozcolluelaCRde Gregorio ArizaMACortinaPPSaldiasLDoppler-duplex ultrasound in renal colicEur J Radiol19962321431488886728
- OpdenakkerLOyenRVervloessemIAcute obstruction of the renal collecting system: the intrarenal resistive index is a useful yet time-dependent parameter for diagnosisEur Radiol199888142914329853230
- ShokeirAAAbdulmaaboudMResistive index in renal colic: a prospective studyBJU Int19998337838210210556
- ShokeirAAAbdulmaaboudMFarageYMutabaganiHResistive index in renal colic: the effect of nonsteroidal antiinflammatory drugsBJU Int19998424925110468715
- ShokeirAAProvoostAPNijmanRJResistive index in obstructive uropathyBr J Urol19978021952009284187
- BertolottoMQuaiaEGaspariniCCalderanLPozzi MucelliRResistive index in patients with renal colic: differences after medical treatment with indomethacin and ketorolacRadiol Med2003106437037514612828