
Abstract
Chronic kidney disease (CKD) and its associated morbidity pose a worldwide health problem. As well as risk of endstage renal disease requiring renal replacement therapy, cardiovascular disease is the leading cause of premature death among the CKD population. Proteinuria is a marker of renal injury that can often be detected earlier than any tangible decline in glomerular filtration rate. As well as being a risk marker for decline in renal function, proteinuria is now widely accepted as an independent risk factor for cardiovascular morbidity and mortality. This review will address the prognostic implications of proteinuria in the general population as well as other specific disease states including diabetes, hypertension and heart failure. A variety of pathophysiological mechanisms that may underlie the relationship between renal and cardiovascular disease have been proposed, including insulin resistance, inflammation, and endothelial dysfunction. As proteinuria has evolved into a therapeutic target for cardiovascular risk reduction in the clinical setting we will also review therapeutic strategies that should be considered for patients with persistent proteinuria.
Introduction
The association between chronic kidney disease (CKD) and cardiovascular disease has long been recognised and current guidelines recommend that patients with CKD be considered to be at particularly high cardiovascular risk.Citation1 Although often transient and benign, the persistent presence of protein or albumin in the urine has marked clinical significance as an early indicator of underlying renal pathology, preceding tangible decline in renal filtration function. In addition to its role as a marker for CKD risk, it is now widely accepted that proteinuria is an independent predictor of cardiovascular morbidity and mortality across divergent populations.Citation2 This review will address the role of proteinuria as a cardiovascular risk marker, the mechanisms and risk factors proposed to underlie this relationship and current pharmacological and non-pharmacological treatment strategies for individuals with proteinuria. Due to heterogeneity of detection methods used in published studies, this article will consider classifications including microalbuminuria, albuminuria, and proteinuria.
Background
National Health and Nutrition Examination Survey study (NHANES) data demonstrated that proteinuria is present in 4% of men and 2% of women between 45 and 74 years of age in the general populationCitation3 and up to 26% of patients with estimated glomerular filtration rate (eGFR) <30 mL/minute/1.73 m.Citation2,Citation4 Data from the Framingham Heart Study found a higher prevalence among older people, with dipstick proteinuria detected in 17.4% of men and 12.9% of women at baseline.Citation5 In treated hypertensive patients, the reported prevalence of proteinuria varies between 4 and 15%.Citation6,Citation7
Classifications of proteinuria according to the diagnostic test used are defined in . Although the accepted gold standard for measuring proteinuria is 24 hour urinary protein excretion, this method can be cumbersome for patients and frequent error is encountered due to improper collection. A spot urine dipstick sample is often considered to be a more practical alternative. This method has high specificity of 97% or greater but poor sensitivity as false negatives can be encountered when urine samples are particularly dilute.Citation8 The Kidney Disease Outcomes Quality Initiative (KDOQI) guidelines recommend initial screening of at risk individuals with a standard urine dipstick. Those with a positive test should then proceed to a confirmatory quantitative test such as spot urine protein:creatinine (PCR) or albumin:creatinine ratio (ACR), both of which have been shown to correlate well with 24 hour urine protein quantification.Citation9 Spot urine tests are subject to a significant degree of variability depending on multiple individual factors, and therefore repeating these tests is essential to obtain confirmation of initial abnormal results.Citation9
Table 1 Classification of proteinuria
CKD and cardiovascular risk
The presence of CKD is a powerful predictor of adverse clinical outcomes.Citation10,Citation11 Cardiovascular disease is by far the most common cause of death in dialysis-dependent and renal transplant patients. Only a small minority of the CKD population progress to endstage renal disease requiring renal replacement therapy (RRT), with death prior to RRT being far more common.Citation11 A 2010 meta-analysis with data for over 1 million subjects reported that stage 3 CKD (eGFR <60 mL/minute/1.73 m2) was associated with both cardiovascular and all-cause mortality.Citation12 In a systematic review of associations between non-dialysis-dependent CKD and mortality, Tonelli et al reported that the absolute risk of death increased exponentially with declining renal function.Citation13 Even the earliest, clinically silent stages of CKD have been associated with major cardiovascular disease.Citation14 In addition to reduced eGFR, ACR and dipstick positive proteinuria have also been associated with graded cardiovascular and all-cause mortality, acting as risk multipliers across all levels of renal function.Citation15,Citation16 In a large Canadian study, Hemmelgarn et al found that heavy proteinuria independently increased risk of death, myocardial infarction (MI) and progression of CKD in particular patient groups.Citation17
Proteinuria and clinical cardiovascular outcomes
General population
Evidence now suggests that proteinuria has implications for all-cause mortality and cardiovascular outcomes at a general population level, not only in individuals with CKD. Population based cohort studies have shown that multivariable relative risks of cardiovascular disease mortality for proteinuria range from 1.2–2.9.Citation3,Citation18,Citation19 The Prevention of Renal and Vascular Endstage Disease (PREVEND) study included over 40,000 individuals and found that a 2-fold increase in ACR equated to close to a 30% increase in risk for cardiovascular mortality.Citation20 Moreover, this relationship is constant across distinct ethnic groupsCitation1,Citation21–Citation23 and in elderly populations.Citation5,Citation24 In terms of cardiovascular morbidity, dipstick positive proteinuria and ACR have emerged as predictors of cardiovascular diseases including ischemic heart disease, stroke, and hypertension in the general population, with some sources suggesting that proteinuria is a stronger predictor of outcome than traditional risk factors such as blood pressure and cholesterol.Citation7,Citation22,Citation25,Citation26 Indeed, the Heart Outcomes Prevention Evaluation (HOPE) study found that proteinuria was associated with adverse outcome independently of traditional cardiovascular risk factors.Citation27 Furthermore, cardiovascular risk appears to be increased even at levels of urinary protein excretion that are not considered to be pathologicalCitation28 and in fact there is no distinct threshold level that confers increased cardiovascular risk; rather, increasing albuminuria is associated with a graded increase in risk.Citation29,Citation30 Proteinuria has also been associated with increased risk of atherosclerotic events affecting the peripheral vasculature. Patients with proteinuria have been shown to have increased risk of incident stroke. A 2010 meta-analysis of studies totaling 48,000 participants reported that the presence of microalbuminuria was associated with a future stroke risk 90% greater than that of normoalbuminuric individuals. The impact of microalbuminuria was greatest on ischemic stroke incidence in those with a prior history of cerebrovascular disease and found to be relatively modest within the diabetic population.Citation31 A further meta-analysis of the relationship between proteinuria and stroke has suggested that risk rises with degree of urinary protein excretion.Citation32
Hypertension and ischemic heart disease
In the hypertensive population, studies suggest that microalbuminuria confers a 4 times greater risk of subsequent ischemic heart disease than in normoalbuminuric individuals.Citation33 This effect appears to be independent of conventional atherosclerotic risk factors. In addition, albuminuria has been associated with the presence of left ventricular hypertrophy in patients with hypertension and diabetes.Citation29,Citation34–Citation36 It has also been demonstrated that in individuals with stable underlying coronary artery disease, proteinuria confers increased risks of all-cause and cardiovascular mortality, even at lower levels within the defined “normal range”.Citation37 This has also been shown in individuals who have recently suffered a coronary event.Citation38,Citation39 The Pravastatin or Atorvastatin Evaluation and Infection Therapy-Thrombolysis in Myocardial Infarction (PROVE IT-TIMI 22) study showed that macro- rather than microalbuminuria was a better predictor of mortality in this group.Citation39
Diabetes
Since the mid-1980s, accumulating evidence has linked microalbuminuria with mortality in patients with diabetes,Citation40–Citation42 both those with reduced and normal eGFR.Citation43,Citation44 Data from a pooled analysis of cohort studies including more than 2,000 patients suggest that the overall odds ratio for all-cause mortality in type 2 diabetic patients with microalbuminuria is 2.4 (confidence interval [CI] 1.8–3.1).Citation45 Similarly, data suggest that type 1 diabetic patients with albuminuria have nine times greater cardiovascular mortality than those who are normoalbuminuric.Citation46 The strong association between proteinuria and cardiovascular morbidity and mortality in type 2 diabetes has also been well-documented, both in patients with and without nephropathy.Citation47–Citation49 Data from the World Health Organization (WHO) Multinational Study of Vascular Disease in Diabetics confirm the association between clinical proteinuria and ischemic heart disease in type 2 diabetes.Citation50 However, the Bypass Angioplasty Revascularization Investigation 2 Diabetes study of type 2 diabetic patients with cardiovascular disease reported that only 33% of participants had clinically confirmed albuminuria, although this was found to be associated with left ventricular dysfunction and peripheral vascular disease.Citation51 The Strong Heart Study confirmed association between albuminuria and abnormal systolic and diastolic ventricular function in individuals with type 2 diabetes.Citation52 These findings have been replicated in the Non-Insulin-Dependent Diabetes, Hypertension, Microalbuminuria or Proteinuria, Cardiovascular Events, and Ramipril (DIABHYCAR), Reduction of Endpoints in NIDDM with the Angiotensin II Antagonist Losartan (RENAAL) and Losartan Intervention for Endpoint Reduction (LIFE) studies.Citation53–Citation55
Heart failure
Chronic heart failure lies at the end of the spectrum of cardiovascular disease, with 32% of individuals admitted to hospital with a diagnosis of heart failure dying within 1-year. It is thought to affect around 14 million people in Europe and 4.8 million Americans.Citation56 A 2005 study of 94 stable chronic heart failure patients with New York Heart Association (NYHA) functional class III to IV symptoms found that 32% had evidence of microalbuminuria.Citation57 Similar findings have been published from follow up of 2,310 patients in the Candesartan in Heart Failure-Assessment of Reduction in Mortality and Morbidity (CHARM) study, with 30% of patients having microalbuminuria and a further 11% with confirmed macroalbuminuriaCitation58 and these were echoed in the Aliskiren Observation of Heart Failure Treatment (ALOFT) study.Citation59 Proteinuria is a well documented risk factor for heart failureCitation57 but, in addition, appears to provide prognostic information. In the CHARM population, ACR was an independent predictor of mortality, conferring a 40%–80% increase in relative risk. It also predicted outcome when assessed as a continuous variable with each 100 mg/mmol increment conferring a 10% increase in mortality risk. The Prospective Randomized Enalapril Study Evaluating Regression of Ventricular Enlargement (PRESERVE) study found that dipstick positive proteinuria was an independent predictor of clinical outcome in heart failure patients irrespective of specific level of proteinuria.Citation60 Microalbuminuria also conferred a 30%–70% increased risk of hospitalization for heart failure.Citation58 Data from the ALOFT study suggested that albuminuria predicted greater left ventricular end diastolic dimension and a trend towards increased N-terminal prohormone of brain natriuretic peptide (NT-pro BNP) levels.Citation59
Surrogate cardiovascular risk markers
A number of studies have demonstrated an independent association between proteinuria and other surrogate markers of cardiovascular disease. For example, data from the PREVEND study found microalbuminuria to be independently associated with electrocardiographic (ECG) indicators of myocardial ischemia.Citation61 In addition, a number of cross sectional studies have linked microalbuminuria with carotid artery intima media thickness.Citation62,Citation63 The association between microalbuminuria and left ventricular hypertrophy (LVH) has been shown in a number of cohorts including the LIFE and Multi-Ethnic Study of Atherosclerosis (MESA) populations, where albuminuria was linked with both electrocardiogram (ECG) and magnetic resonance imaging (MRI) defined LVH.Citation30,Citation64 Microalbuminuria was also associated with increased coronary artery calcification scores in the MESA trial,Citation64 and with carotid-femoral pulse wave velocity in Framingham data.Citation65
Mechanisms underlying cardiovascular consequences of proteinuria
The Steno hypothesis suggested that urinary protein excretion not only reflects localized subclinical renal disease but also a more generalized vascular endothelial dysfunction.Citation66 High-sensitivity troponin T (hs-TnT) as a marker of vascular micronecrosis has been found to independently predict transitions in albuminuria grade.Citation67 Microalbuminuria is also accompanied by a fall in adiponectin levels and elevated C-reactive protein (CRP)Citation68 and there appears to be a significant correlation between degree of proteinuria and CRP level.Citation2 Evidence has also linked proteinuria with asymmetric dimethylarginine (ADMA), an inflammatory biomarker which causes endothelial dysfunction through inhibition of nitric oxide production.Citation69 Circulating von Willebrand Factor (vWF) antigen is released in greater concentrations in response to endothelial cell damage. Levels of vWF have been shown to be higher in patients with microalbuminuria compared to control subject.Citation70 Macrovascular endothelial dysfunction assessed by flow-mediated dilatation has beens hown to be impaired in individuals with proteinuria.Citation2 Vascular endothelial growth factor (VEGF) is another interesting potential mechanistic link between proteinuria and endothelial dysfunction. Use of VEGF-antagonists as angiogenesis inhibitors for the treatment of patients with cancers have been associated with increased incidence of proteinuria and hypertension, an effect which was reversed on withdrawal of therapy.Citation71
As well as inflammation and endothelial dysfunction, thrombogenic factors have been implicated as potential mechanisms underlying the relationship between proteinuria and cardiovascular disease. In addition to vWF, soluble vascular cell adhesion molecule, fibrinogen, and tissue plasminogen activator have been found to correlate with urinary albumin excretion.Citation72 A variety of hemostatic abnormalities have been described in patients with diabetesCitation73 and it has been suggested that high platelet adhesiveness and erythrocyte aggregation demonstrated in diabetic patients with proteinuria could indicate increased thrombosis risk.Citation74
Both insulin resistance and proteinuria have been associated with atherogenesis. The Insulin Resistance Atherosclerosis Study involving 982 nondiabetic participants found that microalbuminuric subjects had lower insulin sensitivity and higher plasma insulin levels compared to normal albuminuric participants, leading the authors to propose that insulin resistance has a role to play in the increased cardiovascular risk conferred by proteinuria.Citation75 Hyperinsulinemia has been shown to cause renal vasodilatation and increased glomerular filtration rate in rats, with some suggesting that this localized elevated pressure is involved in regulating urinary albumin excretion.Citation75 As well as demonstrating association between insulin resistance and microalbuminuria, Bianchi et al noted that in patients with essential hypertension, microalbuminuria was associated with altered lipid profile and an abnormal circadian blood pressure pattern, thus forming part of a cluster with potential to modify cardiovascular risk in these individuals.Citation76
Risk factors for proteinuria
Despite its evolving role as a major risk factor for cardiovascular disease, little is known about factors that determine the onset of proteinuria. The majority of studies demonstrating relationships between proteinuria and other major cardiovascular risk factors are cross-sectional and so inference regarding causality cannot be drawn. In one 10-year prospective cohort study of 157,377 healthy Korean adults who were free of proteinuria at baseline, fasting glucose and cholesterol levels, as well as body mass index and blood pressure were found to be independent predictors of incident proteinuria. Furthermore, cardiovascular risk increased in a progressive, dose-response manner, even at levels of protein excretion falling below currently accepted thresholds for cardiovascular disease prevention.Citation77 Data from the Baltimore Longitudinal Study of Ageing confirmed the association between albuminuria and blood pressure, but suggested that urine albumin excretion was more strongly associated with systolic blood pressure and pulse pressure, and this finding was statistically significant only in males.Citation78 Certainly, links between abnormal lipid profiles and CKD are well documented in both diabetic and non-diabetic populations.Citation79,Citation80 Obesity has been associated with glomerular hyperfiltration and microalbuminuria in subjects with and without diabetes.Citation77,Citation81 A number of studies have linked body mass index with incident proteinuria but it has been suggested that perhaps body fat distribution is more significant as central body fat appears to confer greater risk in lean, overweight and clinically obese patients.Citation82 Risk of incident proteinuria appears to increase in parallel with the number of features of the metabolic syndrome elicited in individuals, regardless of age or sex.Citation83
A cluster of cardiovascular risk factors has also been noted in hypertensive populations with microalbuminuria. In a study of normal albuminuric patients who were under 50 years old with essential hypertension followed up over 3 years, baseline microalbuminuria values and the slopes of systolic blood pressure and fasting glucose emerged as independent predictors of incident proteinuria.Citation84 Evidence also links hyperinsulinemia with microalbuminuria, and the increase in baseline albumin excretion may reflect a degree of subclinical end-organ damage in values below the defined threshold for microalbuminuria. The Hypertension and Ambulatory Recording Venetia Study (HARVEST) study followed normal albuminuric hypertensive patients for 7 years and confirmed that 24 hour systolic blood pressure was a predictor of microalbuminuria, but also named age and female sex amongst implicated risk factors.Citation85
The interrelationship between proteinuria and diabetes is well-documented. In a cross sectional study evaluating 24,000 type 2 diabetic patients, elevated albumin excretion was most prevalent in Asian and Hispanic patients. HbA1c, blood pressure, diabetes duration, smoking, and baseline renal function were all independent risk factors for miroalbuminuria.Citation86 Surprisingly, body mass index was not a risk factor for incident proteinuria, perhaps because microalbuminuria was most prevalent in the Asian population, who had lower values. In cross-sectional data from the Randomized Olmesartan and Diabetes Microalbuminuria Prevention (ROADMAP) study, the factors most strongly correlated with degree of albuminuria within the normal range were blood pressure, pulse pressure, HbA1c, eGFR, and uric acid levels. In terms of categorical variables, higher albumin excretion was found in those with greater waist circumference, smokers, females and those who were treated with insulin.Citation81 Although such observational correlations do not infer causality, many of the factors linked to albumin excretion are potential targets for intervention when aiming to minimize overall cardiovascular risk.
Pharmacological interventions
Given that the presence of proteinuria is independently associated with increased risk of cardiovascular morbidity and mortality it has evolved into a therapeutic target for cardiovascular risk reduction. In the LIFE study, greater reductions in urinary albumin excretion were seen in subjects with the lowest cardiovascular event rate.Citation87 Similar findings have been published from the RENAAL studyCitation49 but results of other projects such as the Prevention of Renal and Vascular Endstage Disease Intervention Trial (PREVEND- IT) have been less convincing.Citation88
Cardiovascular risk management in patients with proteinuria focuses on reduction or control of degree of proteinuria and modification of additional risk factors including blood pressure, diabetes, lipid profile, smoking, and obesity. Results of the Modification of Diet in Renal Disease study highlighted the importance of tight blood pressure control in patients with CKD and proteinuriaCitation89 as did the UK Prospective Diabetes Study (UKPDS) for those with diabetes.Citation90 Current evidence-based guidelines highlight the importance of renin-angiotensin-aldosterone system (RAAS) inhibition () as the first line therapeutic strategy in terms of slowing progression of nephropathy and reducing proteinuria in these populations.Citation91,Citation92 Many patients will require additional antihypertensive therapy which should be prescribed according to each individual’s characteristics. These additional agents may not have specific antiproteinuric properties but lowering of blood pressure itself can have beneficial effects on protein excretion.Citation89,Citation90
Figure 1 RAAS blocking agents and sites of action.
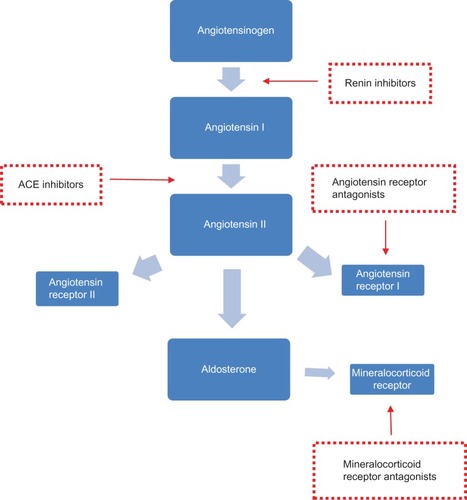
RAAS blocking agents
The renoprotective benefits of angiotensin-converting enzyme inhibitors (ACE-inhibitors) and angiotensin receptor blockers in both diabetic and non-diabetic chronic kidney disease are well documented and out of the scope of this review.Citation93–Citation97 In a sub-analysis of the HOPE study, ramipril treatment resulted in significantly reduced cardiovascular risk in participants with renal impairment. This cardioprotective effect was attributed to proteinuria reduction and limiting the deleterious effects of angiotensin II.Citation98 Similar reductions in cardiovascular endpoints were shown in the diabetic subset (micro-HOPE).Citation95 In another study, captopril reduced mortality in type 1 diabetic patients with nephropathy.Citation94 Angiotensin receptor blockers have also been shown to improve cardiovascular morbidity and mortality. For example, in the LIFE study, losartan therapy reduced occurrence of the primary composite endpoint including death, myocardial infarction, and stroke in both diabetic and non-diabetic participants concomitant with reduction in albuminuria.Citation99,Citation100 In addition, the Irbesartan Diabetic Nephropathy Trial demonstrated concomitant reductions in urinary protein excretion and cardiovascular endpoints in hypertensive type 2 diabetic participants;Citation101 however, in the RENAAL trial, losartan therapy reduced hospitalizations for heart failure but did not show any significant effect on mortality rate.Citation97
Early intervention/dual RAAS blockade
A number of studies have explored the risks and benefits of early initiation of RAAS blocking agents, or dual RAAS blockade. The ROADMAP study investigated early initiation of angiotensin receptor blockade in normoalbuminuric patients with type 2 diabetes and showed that this did indeed delay onset of microalbuminuria. This did not, however, translate into a beneficial impact on cardiovascular risk.Citation102 The Ongoing Telmisartan Alone and in combination with Ramipril Global Endpoint Trial (ONTARGET) randomized participants with vascular disease or diabetes to receive telmisartan, ramipril, or a combination of both. Combination therapy was shown to offer greater reduction in proteinuria but this apparent benefit was offset by the lack of overall benefit in terms of cardiovascular outcomes and indeed a significant increase in adverse events, such as hypotensive symptoms and renal dysfunction.Citation103,Citation104 In adults with proteinuric CKD, the addition of aldosterone antagonists such as spironolactone or eplerenone to angiotensin-converting-enzyme (ACE)-inhibitor or angiotensin receptor blocker therapy has been shown to reduce protein excretion but to increase risk of adverse events such as hyperkalemia.Citation105
Direct renin inhibitors
Direct renin inhibition offers potential to further optimize RAAS blockade by interfering with the first step in the pathway. Aliskiren is the first of this class to be licensed for treatment of hypertension. In comparative studies with other antihypertensives, aliskiren monotherapy appears to provide blood pressure reductions similar to those achieved with losartan or lisinoprilCitation106,Citation107 as well as significant additive blood pressure reduction in combination with other agents.Citation108,Citation109 Several trials have shown that treatment with direct renin inhibitors such as Aliskiren in combination with other RAAS blocking agents have beneficial effects on endpoints including proteinuria and left ventricular hypertrophy in patients with diabetic nephropathy and non-diabetic CKD including transplant recipients or heart failure.Citation110–Citation113 The recent Aliskiren Trial in Type 2 Diabetes Using Cardiorenal Endpoints (ALTITUDE), however, was terminated early because of increased adverse outcomes including non-fatal stroke, hypotension, and hyperkalemiaCitation114 and further prospective studies are needed to confirm the safety and tolerability of these agents in CKD populations.
Endothelin A blockade
Although effective and the current mainstay of treatment of proteinuria, RAAS blockade does not always completely retard progression of proteinuria.Citation115 Experimental data have demonstrated that endothelin A blockade can have favorable antiproteinuric and antifibrotic effects and these have been confirmed in studies in patients with diabetic nephropathy.Citation116 Encouraging results have been published from a short term pilot study of Atrasentan documenting significant reduction in proteinuria in participants with diabetic nephropathy although studies on long term safety and efficacy are lacking and some negative effects have been demonstrated in patients with underlying cardiac disease.Citation117
Statins
As well as being effective cholesterol-lowering agents with positive effects on cardiovascular outcomes, some have suggested that statins have an antiproteinuric effect. In a 2006 meta-analysis, statins were shown to reduce albuminuria in 13 out of 15 studies reviewed. The degree of reduction appeared to be greater in individuals who had higher baseline albumin excretion although there was marked variability in study quality.Citation118 A subsequent meta-analysis including randomized controlled trials of statins in patients with CKD again showed a significant reduction in protein excretion as well as a reduction in cardiovascular events.Citation119 It is unclear whether these perceived benefits are the result of lipid-lowering effects on endothelial function, reduction of inflammation and oxidative stress, or inhibitory effects on renal endothelin 1.Citation120
Non-pharmacological interventions
As well as known carcinogenic effects, smoking has been shown to induce intimal proliferation and vascular hyaline thickening.Citation121 As such, cigarette smoking is accepted as a major risk factor for cardiovascular disease. Similar histological changes have been described in the kidney.Citation122 Multiple studies have shown an association between smoking and renal damage, at general population level as well as in patients with diabetes or hypertension.Citation123 In epidemiological studies of otherwise healthy participants, the incidence of proteinuria has been positively associated with the number of cigarettes smoked per day, particularly in malesCitation124 and although no specific data exist to support cessation of smoking for reduction of proteinuria, smoking cessation is advised in KDOQI guidance on hypertension in CKD.
Obesity has been shown to be associated with proteinuria.Citation125,Citation126 Weight loss in combination with ACE-inhibitor therapy have been shown to decrease levels of protein excretion in obese patients as well as proteinuria of other etiologies including diabetes.Citation127 Moreover, a significant correlation between level of weight loss attained and reduction in proteinuria was demonstrated in the same study.Citation127
Dietary protein restriction in patients with CKD remains a controversial issue due to the delicate balance between slowing progression of proteinuria and the importance of good nutritional status in chronic disease. Although limiting dietary protein intake to between 0.75 and 1.0 g/kg/day is often recommended in the later stages of CKD, these diets can be unpalatable and compliance is variable. In addition, guidelines also recommend dietary sodium restriction to reduce cardiovascular risk in patients with CKD.Citation9 Although no specific guidance exists on sodium restriction in patients with proteinuria, evidence suggests that dietary sodium restriction can enhance the effects of RAAS blocking agents in reducing urinary protein excretion.Citation128,Citation129 Most clinical guidelines suggest that a dietetic review for discussion of such modifications be considered for patients with advanced CKD although no specific guidance is available for the earlier stages of disease when GFR remains >60 mL/minute/1.73 m2.
Renal sympathetic innervation is another key component of the pathogenesis of hypertension through its effects on renin secretion, renal sodium absorption and glomerular filtration rate.Citation130 In recent years, catheter-based renal sympathetic denervation has gained much attention as a potential tool in the management of resistant hypertension. Preliminary evidence suggests that this procedure can offer significant blood pressure reduction for resistant hypertensive patients with effects maintained at 24 months follow up,Citation131,Citation132 as well as beneficial effects on left ventricular mass and systolic function and arterial stiffness as measured by pulse wave velocity.Citation133 In terms of renal hemodynamics, recent evidence suggests that renal denervation improved ultrasound renal resistive indices. This study also demonstrated that renal function as measured by creatinine and cystatin C was unchanged at 6 months follow up, suggesting that the procedure itself has no adverse effects on the kidneys at least in the short term. Urinary albumin excretion remained unchanged after denervation but the number of patients with micro or macroalbuminuria did fall, although it should be kept in mind that this was a small study.Citation134 Whether this approach is equally safe and effective over longer term follow up in patients with eGFR less than 45 mL/minute remains to be seen.
Conclusion
The significant burden on health services posed by cardiovascular disease has prompted investigation of prognostic markers and therapeutic targets. There is a clear association between proteinuria and cardiovascular outcomes despite marked heterogeneity in the literature when considering the method of detection used and classification of degree of proteinuria. This association has been demonstrated both in disease population including hypertensives, diabetic patients, and those with CKD, as well as in otherwise healthy individuals. Proteinuria has evolved into a surrogate marker of cardiovascular risk and it seems intuitive that earlier detection and more aggressive intervention may serve to reduce risk in affected individuals. Several publications have considered the cost-effectiveness of population screening. In 2003 Boulware et al concluded that population screening for dipstick proteinuria was not cost-effective in terms of CKD morbidity and mortality unless specifically targeted towards higher risk groups such as hypertensive or elderly patients and done at less frequent intervals.Citation135 When considering prevention of cardiovascular events, an analysis of the PREVEND-IT study was more favourable.Citation136 RAAS inhibition, together with control of additional cardiovascular risk factors, remains the mainstay of treatment for individuals with proteinuria. Studies of earlier and more aggressive intervention with two or more RAAS blocking agents have demonstrated reduction in proteinuria but this has not yet translated into reduction in hard clinical cardiovascular endpoints and these studies have also reported a greater degree of side effects and adverse events.
Disclosure
Work in our group is supported by grants from the European Commission “PRIORITY” (grant agreement 279277), “EU-MASCARA” (grant agreement 278249) and “HOMAGE” (grant agreement 305507). The authors have no conflicts of interest to report.
References
- SarnakMJLeveyASSchoolwerthACAmerican Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and PreventionKidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and PreventionCirculation2003108172154216914581387
- AgrawalVMarinescuVAgarwalMMcCulloughPACardiovascular implications of proteinuria: an indicator of chronic kidney diseaseNat Rev Cardiol20096430131119352334
- WagnerDKHarrisTMadansJHProteinuria as a biomarker: risk of subsequent morbidity and mortalityEnviron Res19946621601728055838
- GargAXKiberdBAClarkWFHaynesRBClaseCMAlbuminuria and renal insufficiency prevalence guides population screening: results from the NHANES IIIKidney Int20026162165217512028457
- CulletonBFLarsonMGParfreyPSKannelWBLevyDProteinuria as a risk factor for cardiovascular disease and mortality in older people: a prospective studyAm J Med200010911810936471
- SeguraJCampoCRuilopeLMProteinuria: an underappreciated risk factor in cardiovascular diseaseCurr Cardiol Rep20024645846212379163
- LjungmanSWikstrandJHartfordMBerglundGUrinary albumin excretion – a predictor of risk of cardiovascular disease. A prospective 10-year follow-up of middle-aged nondiabetic normal and hypertensive menAm J Hypertens1996987707788862223
- KashifWSiddiqiNDincerAPDincerHEHirschSProteinuria: how to evaluate an important findingCleve Clin J Med200370653553754112828224
- National Kidney FoundationKDQOI clinical practice guidelines for chronic kidney disease: evaluation, classification and stratificationAm J Kidney Dis2002392 Suppl 1s1s26611904577
- GoASChertowGMFanDMcCullochCEHsuCYChronic kidney disease and the risks of death, cardiovascular events, and hospitalizationN Engl J Med2004351131296130515385656
- KeithDSNicholsGAGullionCMBrownJBSmithDHLongitudinal follow-up and outcomes among a population with chronic kidney disease in a large managed care organizationArch Intern Med2004164665966315037495
- MatsushitaKvan der VeldeMAstorBCChronic Kidney Disease Prognosis ConsortiumAssociation of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysisLancet201037597312073208120483451
- TonelliMWiebeNCulletonBChronic kidney disease and mortality risk: a systematic reviewJ Am Soc Nephrol20061772034204716738019
- Di AngelantonioEChowdhuryRSarwarNAspelundTDaneshJGudnasonVChronic kidney disease and risk of major cardiovascular disease and non-vascular mortality: prospective population based cohort studyBMJ2010341c498620884698
- HerzogCAKidney disease in cardiologyNephrol Dial Transplant2009241343719028753
- NagataMNinomiyaTKiyoharaYEPOCH-JAPAN Research GroupPrediction of cardiovascular disease mortality by proteinuria and reduced kidney function: pooled analysis of 39,000 individuals from 7 cohort studies in JapanAm J Epidemiol2013178111123752917
- HemmelgarnBRMannsBJLloydAAlberta Kidney Disease NetworkRelation between kidney function, proteinuria, and adverse outcomesJAMA2010303542342920124537
- KannelWBStampferMJCastelliWPVerterJThe prognostic significance of proteinuria: the Framingham studyAm Heart J19841085134713526496291
- MatsushitaKvan der VeldeMAstorBCChronic Kidney Disease Prognosis ConsortiumAssociation of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysisLancet201037597312073208120483451
- HillegeHLFidlerVDiercksGFPrevention of Renal and Vascular End Stage Disease (PREVEND) Study GroupUrinary albumin excretion predicts cardiovascular and noncardiovascular mortality in general populationCirculation2002106141777178212356629
- IrieFIsoHSairenchiTThe relationships of proteinuria, serum creatinine, glomerular filtration rate with cardiovascular disease mortality in Japanese general populationKidney Int20066971264127116501489
- InoueTIsekiKHigashiuesatoYProteinuria as a significant determinant of hypertension in a normotensive screened cohort in Okinawa, JapanHypertens Res200629968769317249524
- WangZHoyWEAlbuminuria and incident coronary heart disease in Australian Aboriginal peopleKidney Int20056831289129316105063
- DamsgaardEMFrølandAJørgensenODMogensenCEMicroalbuminuria as predictor of increased mortality in elderly peopleBMJ199030067202973002106959
- BelloAKHemmelgarnBLloydAAlberta Kidney Disease NetworkAssociations among estimated glomerular filtration rate, proteinuria, and adverse cardiovascular outcomesClin J Am Soc Nephrol2011661418142621527648
- PerkovicVVerdonCNinomiyaTThe relationship between proteinuria and coronary risk: a systematic review and meta-analysisPLoS Med2008510e20718942886
- GersteinHCMannJFYiQHOPE Study InvestigatorsAlbuminuria and risk of cardiovascular events, death, and heart failure in diabetic and nondiabetic individualsJAMA2001286442142611466120
- HillegeHLJanssenWMBakAAPrevend Study GroupMicroalbuminuria is common, also in a nondiabetic, nonhypertensive population, and an independent indicator of cardiovascular risk factors and cardiovascular morbidityJ Intern Med2001249651952611422658
- WachtellKIbsenHOlsenMHAlbuminuria and cardiovascular risk in hypertensive patients with left ventricular hypertrophy: the LIFE studyAnn Intern Med20031391190190614644892
- WachtellKOlsenMHDahlöfBMicroalbuminuria in hypertensive patients with electrocardiographic left ventricular hypertrophy: the LIFE studyJ Hypertens200220340541211875307
- LeeMSaverJLChangKHLiaoHWChangSCOvbiageleBImpact of microalbuminuria on incident stroke: a meta-analysisStroke201041112625263120930164
- NinomiyaTPerkovicVVerdonCProteinuria and stroke: a meta-analysis of cohort studiesAm J Kidney Dis200953341742519070947
- JensenJSFeldt-RasmussenBStrandgaardSSchrollMBorch-JohnsenKArterial hypertension, microalbuminuria, and risk of ischemic heart diseaseHypertension200035489890310775558
- NobakhthaghighiNKamgarMBekheirniaMRMcFannKEstacioRSchrierRWRelationship between urinary albumin excretion and left ventricular mass with mortality in patients with type 2 diabetesClin J Am Soc Nephrol2006161187119017699346
- PostWSBlumenthalRSWeissJLSpot urinary albumin-creatinine ratio predicts left ventricular hypertrophy in young hypertensive African-American menAm J Hypertens200013111168117211078176
- Dell’omoGGiorgiDDi BelloVMarianiMPedrinelliRBlood pressure independent association of microalbuminuria and left ventricular hypertrophy in hypertensive menJ Intern Med20032541768412823644
- SolomonSDLinJSolomonCGPrevention of Events With ACE Inhibition (PEACE) InvestigatorsInfluence of albuminuria on cardiovascular risk in patients with stable coronary artery diseaseCirculation2007116232687269318025537
- JosePSkaliHAnavekarNIncrease in creatinine and cardiovascular risk in patients with systolic dysfunction after myocardial infarctionJ Am Soc Nephrol200617102886289116928807
- NazerBRayKKMurphySAGibsonCMCannonCPUrinary albumin concentration and long-term cardiovascular risk in acute coronary syndrome patients: a PROVE IT-TIMI 22 substudyJ Thromb Thrombolysis201336323323923212806
- MogensenCEMicroalbuminuria predicts clinical proteinuria and early mortality in maturity-onset diabetesN Engl J Med198431063563606690964
- MessentJWElliottTGHillRDJarrettRJKeenHVibertiGCPrognostic significance of microalbuminuria in insulin-dependent diabetes mellitus: a twenty-three year follow-up studyKidney Int19924148368391513106
- Borch-JohnsenKAndersenPKDeckertTThe effect of proteinuria on relative mortality in type 1 (insulin-dependent) diabetes mellitusDiabetologia19852885905964054448
- LinCCChenCCKungPTJoint relationship between renal function and proteinuria on mortality of patients with type 2 diabetes: the Taichung Diabetes StudyCardiovasc Diabetol20121113123083001
- AnavekarNSGansDJBerlTPredictors of cardiovascular events in patients with type 2 diabetic nephropathy and hypertension: a case for albuminuriaKidney Int Suppl2004S50S5515485418
- DinneenSFGersteinHCThe association of microalbuminuria and mortality in non-insulin-dependent diabetes mellitus. A systematic overview of the literatureArch Intern Med199715713141314189224218
- StadlerMAuingerMAnderwaldCLong-term mortality and incidence of renal dialysis and transplantation in type 1 diabetes mellitusJ Clin Endocrinol Metab200691103814382016882744
- de JongPEGansevoortRTBakkerSJMacroalbuminuria and microalbuminuria: do both predict renal and cardiovascular events with similar strength?J Nephrol200720437538017879201
- RossingPHougaardPBorch-JohnsenKParvingHHPredictors of mortality in insulin dependent diabetes: 10 year observational follow up studyBMJ199631370607797848842069
- de ZeeuwDRemuzziGParvingHHAlbuminuria, a therapeutic target for cardiovascular protection in type 2 diabetic patients with nephropathyCirculation2004110892192715302780
- MorrishNJStevensLKFullerJHJarrettRJKeenHRisk factors for macrovascular disease in diabetes mellitus: the London follow-up to the WHO Multinational Study of Vascular Disease in DiabeticsDiabetologia19913485905941936663
- EscobedoJRanaJSLombarderoMSBARI 2D Study GroupAssociation between albuminuria and duration of diabetes and myocardial dysfunction and peripheral arterial disease among patients with stable coronary artery disease in the BARI 2D studyMayo Clin Proc2010851414620042560
- LiuJERobbinsDCPalmieriVAssociation of albuminuria with systolic and diastolic left ventricular dysfunction in type 2 diabetes: the Strong Heart StudyJ Am Coll Cardiol200341112022202812798576
- VaurLGueretPLievreMChabaudSPassaPDIABHYCAR Study Group (type 2 DIABetes, Hypertension, CARdiovascular Events and Ramipril) studyDevelopment of congestive heart failure in type 2 diabetic patients with microalbuminuria or proteinuria: observations from the DIABHYCAR (type 2 DIABetes, Hypertension, CArdiovascular Events and Ramipril) studyDiabetes Care200326385586012610049
- CarrAAKoweyPRDevereuxRBHospitalizations for new heart failure among subjects with diabetes mellitus in the RENAAL and LIFE studiesAm J Cardiol200596111530153616310435
- MacDonaldMRPetrieMCHawkinsNMDiabetes, left ventricular systolic dysfunction, and chronic heart failureEur Heart J200829101224124018424786
- On the horizon in heart failureLancet2011378979263721856462
- van de WalRMAsselbergsFWPlokkerHWHigh prevalence of microalbuminuria in chronic heart failure patientsJ Card Fail200511860260616230263
- JacksonCESolomonSDGersteinHCCHARM Investigators and CommitteesAlbuminuria in chronic heart failure: prevalence and prognostic importanceLancet2009374968954355019683640
- JacksonCEMacDonaldMRPetrieMCALiskiren Observation of heart Failure Treatment (ALOFT) investigatorsAssociations of albuminuria in patients with chronic heart failure: findings in the ALiskiren Observation of heart Failure Treatment studyEur J Heart Fail201113774675421459891
- SmithDHThorpMLGurwitzJHChronic kidney disease and outcomes in heart failure with preserved versus reduced ejection fraction: the Cardiovascular Research Network PRESERVE StudyCirc Cardiovasc Qual Outcomes20136333334223685625
- DiercksGFvan BovenAJHillegeHLMicroalbuminuria is independently associated with ischaemic electrocardiographic abnormalities in a large non-diabetic population. The PREVEND (Prevention of REnal and Vascular ENdstage Disease) studyEur Heart J200021231922192711071797
- BigazziRBianchiSNenciRBaldariDBaldariGCampeseVMIncreased thickness of the carotid artery in patients with essential hypertension and microalbuminuriaJ Hum Hypertens19959108278338576899
- MykkänenLZaccaroDJO’LearyDHHowardGRobbinsDCHaffnerSMMicroalbuminuria and carotid artery intima-media thickness in nondiabetic and NIDDM subjects. The Insulin Resistance Atherosclerosis Study (IRAS)Stroke1997289171017169303013
- KramerHJacobsDRBildDUrine albumin excretion and subclinical cardiovascular disease. The Multi-Ethnic Study of AtherosclerosisHypertension2005461384315956113
- UpadhyayAHwangSJMitchellGFArterial stiffness in mild-to-moderate CKDJ Am Soc Nephrol20092092044205319608701
- DeckertTFeldt-RasmussenBBorch-JohnsenKJensenTKofoed-EnevoldsenAAlbuminuria reflects widespread vascular damage. The Steno hypothesisDiabetologia19893242192262668076
- HellemonsMELambers HeerspinkHJGansevoortRTde ZeeuwDBakkerSJHigh-sensitivity troponin T predicts worsening of albuminuria in hypertension; results of a nested case-control study with confirmation in diabetesJ Hypertens201331480581223425705
- TsioufisCDimitriadisKChatzisDRelation of microalbuminuria to adiponectin and augmented C-reactive protein levels in men with essential hypertensionAm J Cardiol200596794695116188522
- YilmazMISonmezASaglamMADMA levels correlate with proteinuria, secondary amyloidosis, and endothelial dysfunctionJ Am Soc Nephrol200819238839518199801
- PedrinelliRGiampietroOCarmassiFMicroalbuminuria and endothelial dysfunction in essential hypertensionLancet1994344891414187912295
- ZhuXWuSDahutWLParikhCRRisks of proteinuria and hypertension with bevacizumab, an antibody against vascular endothelial growth factor: systematic review and meta-analysisAm J Kidney Dis200749218619317261421
- StehouwerCDGallMATwiskJWKnudsenEEmeisJJParvingHHIncreased urinary albumin excretion, endothelial dysfunction, and chronic low-grade inflammation in type 2 diabetes: progressive, interrelated, and independently associated with risk of deathDiabetes20025141157116511916939
- KnöblPSchernthanerGSchnackCThrombogenic factors are related to urinary albumin excretion rate in type 1 (insulin-dependent) and type 2 (non-insulin-dependent) diabetic patientsDiabetologia19933610104510508243853
- HiranoTKashiwazakiKMoritomoYNaganoSAdachiMAlbuminuria is directly associated with increased plasma PAI-1 and factor VII levels in NIDDM patientsDiabetes Res Clin Pract199736111189187410
- MykkänenLZaccaroDJWagenknechtLERobbinsDCGabrielMHaffnerSMMicroalbuminuria is associated with insulin resistance in nondiabetic subjects: the insulin resistance atherosclerosis studyDiabetes19984757938009588452
- BianchiSBigazziRValtrianiCElevated serum insulin levels in patients with essential hypertension and microalbuminuriaHypertension1994236 Pt 16816878206563
- JeeSHBoulwareLEGuallarESuhIAppelLJMillerERDirect, progressive association of cardiovascular risk factors with incident proteinuria: results from the Korea Medical Insurance Corporation (KMIC) studyArch Intern Med2005165192299230416246998
- FarasatSMValdesCShettyVIs longitudinal pulse pressure a better predictor of 24-hour urinary albumin excretion than other indices of blood pressure?Hypertension201055241542120008676
- BianchiSBigazziRCaiazzaACampeseVMA controlled, prospective study of the effects of atorvastatin on proteinuria and progression of kidney diseaseAm J Kidney Dis200341356557012612979
- RavidMBroshDRavid-SafranDLevyZRachmaniRMain risk factors for nephropathy in type 2 diabetes mellitus are plasma cholesterol levels, mean blood pressure, and hyperglycemiaArch Intern Med1998158999810049588433
- RitzEVibertiGCRuilopeLMDeterminants of urinary albumin excretion within the normal range in patients with type 2 diabetes: the Randomised Olmesartan and Diabetes Microalbuminuria Prevention (ROADMAP) studyDiabetologia2010531495719876613
- Pinto-SietsmaSJNavisGJanssenWMde ZeeuwDGansROde JongPEPREVEND Study GroupA central body fat distribution is related to renal function impairment, even in lean subjectsAm J Kidney Dis200341473374112666059
- FortJChronic renal failure: a cardiovascular risk factorKidney Int Suppl2005S25S2916336573
- RedonJRoviraEMirallesAJulveRPascualJMFactors related to the occurrence of microalbuminuria during antihypertensive treatment in essential hypertensionHypertension200239379479811897766
- PalatiniPMorminoPDorigattiFHARVEST Study GroupGlomerular hyperfiltration predicts the development of microalbuminuria in stage 1 hypertension: the HARVESTKidney Int200670357858416788693
- ParvingHHLewisJBRavidMRemuzziGHunsickerLGDEMAND investigatorsPrevalence and risk factors for microalbuminuria in a referred cohort of type II diabetic patients: a global perspectiveKidney Int200669112057206316612330
- IbsenHOlsenMHWachtellKDoes albuminuria predict cardiovascular outcomes on treatment with losartan versus atenolol in patients with diabetes, hypertension, and left ventricular hypertrophy? The LIFE studyDiabetes Care200629359560016505512
- AsselbergsFWDiercksGFHillegeHLPrevention of Renal and Vascular Endstage Disease Intervention Trial (PREVEND IT) InvestigatorsEffects of fosinopril and pravastatin on cardiovascular events in subjects with microalbuminuriaCirculation2004110182809281615492322
- PetersonJCAdlerSBurkartJMBlood pressure control, proteinuria, and the progression of renal disease. The Modification of Diet in Renal Disease StudyAnn Intern Med1995123107547627574193
- Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. UK Prospective Diabetes Study GroupBMJ199831771607037139732337
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work GroupKDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney DiseaseKidney Int Suppl2013311150
- National Institute for Health and Clinical ExcellenceNICE Clinical Guideline 66: The Management of Type 2 Diabetes Available from: http://www.nice.org.uk/nicemedia/pdf/cg66niceguideline.pdfAccessed November 27, 2013
- Randomised placebo-controlled trial of effect of ramipril on decline in glomerular filtration rate and risk of terminal renal failure in proteinuric, non-diabetic nephropathy. The GISEN Group (Gruppo Italiano di Studi Epidemiologici in Nefrologia)Lancet19973499069185718639217756
- LewisEJHunsickerLGBainRPRohdeRDThe effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. The Collaborative Study GroupN Engl J Med199332920145614628413456
- Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus: results of the HOPE study and MICRO-HOPE substudy. Heart Outcomes Prevention Evaluation Study InvestigatorsLancet2000355920025325910675071
- LewisEJHunsickerLGClarkeWRCollaborative Study GroupRenoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetesN Engl J Med20013451285186011565517
- BrennerBMCooperMEde ZeeuwDRENAAL Study InvestigatorsEffects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathyN Engl J Med20013451286186911565518
- MannJFGersteinHCPogueJBoschJYusufSRenal insufficiency as a predictor of cardiovascular outcomes and the impact of ramipril: the HOPE randomized trialAnn Intern Med2001134862963611304102
- DahlöfBDevereuxRBKjeldsenSELIFE Study GroupCardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenololLancet20023599311995100311937178
- LindholmLHIbsenHDahlöfBLIFE Study GroupCardiovascular morbidity and mortality in patients with diabetes in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenololLancet200235993111004101011937179
- ParvingHHLehnertHBröchner-MortensenJGomisRAndersenSArnerPIrbesartan in Patients with Type 2 Diabetes and Microalbuminuria Study GroupThe effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetesN Engl J Med20013451287087811565519
- HallerHItoSIzzoJLROADMAP Trial InvestigatorsOlmesartan for the delay or prevention of microalbuminuria in type 2 diabetesN Engl J Med20113641090791721388309
- ONTARGET InvestigatorsYusufSTeoKKPogueJDyalLCoplandISchumacherHDagenaisGSleightPAndersonCTelmisartan, ramipril, or both in patients at high risk for vascular eventsN Engl J Med2008358151547155918378520
- MannJSchmiederRMcQueenMONTARGET investigatorsRenal outcomes with telimsartan, ramipril or both in people at high vascular risk (the ONTARGET study): a multicentre, randomised, double blind, controlled trialLancet2008372963854755318707986
- NavaneethanSDNigwekarSUSehgalARStrippoliGFAldosterone antagonists for preventing the progression of chronic kidney disease: a systematic review and meta-analysisClin J Am Soc Nephrol20094354255119261819
- StantonAJensenCNussbergerJO’BrienEBlood pressure lowering in essential hypertension with an oral renin inhibitor, aliskirenHypertension20034261137114314597641
- StrasserRHPuigJGFarsangCCroketMLiJvan IngenHA comparison of the tolerability of the direct renin inhibitor aliskiren and lisinopril in patients with severe hypertensionJ Hum Hypertens2007211078078717541390
- VillamilAChrysantSGCalhounDRenin inhibition with aliskiren provides additive antihypertensive efficacy when used in combination with hydrochlorothiazideJ Hypertens200725121722617143194
- UresinYTaylorAAKiloCEfficacy and safety of the direct renin inhibitor aliskiren and ramipril alone or in combination in patients with diabetes and hypertensionJ Renin Angiotensin Aldosterone Syst20078419019818205098
- ParvingHHPerssonFLewisJBLewisEJHollenbergNKAVOID Study InvestigatorsAliskiren combined with losartan in type 2 diabetes and nephropathyN Engl J Med2008358232433244618525041
- OparilSYarowsSAPatelSFangHZhangJSatlinAEfficacy and safety of combined use of aliskiren and valsartan in patients with hypertension: a randomised, double-blind trialLancet2007370958322122917658393
- LiSChenYYangWEffects of add-on direct renin inhibitor aliskiren in patients with non-diabetes related chronic kidney diseaseBMC Nephrol2012138922917002
- LópezVMartinMCobeloCRenin-angiotensin system dual blockade using angiotensin receptor plus aliskiren decreases severe proteinuria in kidney transplant recipientsTransplant Proc20104282883288520970559
- ParvingHHBrennerBMMcMurrayJJALTITUDE InvestigatorsCardiorenal end points in a trial of aliskiren for type 2 diabetesN Engl J Med2012367232204221323121378
- ShiigaiTShichiriMLate escape from the antiproteinuric effect of ace inhibitors in nondiabetic renal diseaseAm J Kidney Dis200137347748311228170
- WenzelRRLittkeTKuranoffSSPP301 (Avosentan) Endothelin Antagonist Evaluation in Diabetic Nephropathy Study InvestigatorsAvosentan reduces albumin excretion in diabetics with macroalbuminuriaJ Am Soc Nephrol200920365566419144760
- KohanDEPritchettYMolitchMAddition of atrasentan to renin-angiotensin system blockade reduces albuminuria in diabetic nephropathyJ Am Soc Nephrol201122476377221372210
- DouglasKO’MalleyPGJacksonJLMeta-analysis: the effect of statins on albuminuriaAnn Intern Med2006145211712416847294
- StrippoliGFNavaneethanSDJohnsonDWEffects of statins in patients with chronic kidney disease: meta-analysis and meta-regression of randomised controlled trialsBMJ2008336764564565118299289
- LeeTMSuSFTsaiCHEffect of pravastatin on proteinuria in patients with well-controlled hypertensionHypertension2002401677312105140
- RemuzziGCigarette smoking and renal function impairmentAm J Kidney Dis199933480781310196031
- OberaiBAdamsCWHighOBMyocardial and renal arteriolar thickening in cigarette smokersAtherosclerosis19845221851906477670
- OrthSRHallanSISmoking: a risk factor for progression of chronic kidney disease and for cardiovascular morbidity and mortality in renal patients – absence of evidence or evidence of absence?Clin J Am Soc Nephrol20083122623618003763
- TozawaMIsekiKIsekiCOshiroSIkemiyaYTakishitaSInfluence of smoking and obesity on the development of proteinuriaKidney Int200262395696212164878
- MoralesEHuertaAGutiérrezEGutiérrez SolísESeguraJPragaMThe antiproteinuric effect of the blockage of the reninangiotensin-aldosterone system (RAAS) in obese patients. Which treatment option is the most effective?Nefrologia2009295421429 Spanish19820754
- PragaMTherapeutic measures in proteinuric nephropathyKidney Int Suppl2005S137S14116336567
- PragaMHernándezEAndrésALeónMRuilopeLMRodicioJLEffects of body-weight loss and captopril treatment on proteinuria associated with obesityNephron199570135417617115
- SlagmanMCWaandersFHemmelderMHHOlland NEphrology STudy GroupModerate dietary sodium restriction added to angiotensin converting enzyme inhibition compared with dual blockade in lowering proteinuria and blood pressure: randomised controlled trialBMJ2011343d436621791491
- VegterSPernaAPostmaMJNavisGRemuzziGRuggenentiPSodium intake, ACE inhibition, and progression to ESRDJ Am Soc Nephrol201223116517322135311
- GulatiVWhiteWBReview of the state of renal nerve ablation for patients with severe and resistant hypertensionJ Am Soc Hypertens2013
- EslerMDKrumHSobotkaPASchlaichMPSchmiederREBöhmMSymplicity HTN-2 InvestigatorsRenal sympathetic denervation in patients with treatment-resistant hypertension (The Symplicity HTN-2 Trial): a randomised controlled trialLancet201037697561903190921093036
- Symplicity HTN-1 InvestigatorsCatheter-based renal sympathetic denervation for resistant hypertension: durability of blood pressure reduction out to 24 monthsHypertension201157591191721403086
- BrandtMCMahfoudFRedaSRenal sympathetic denervation reduces left ventricular hypertrophy and improves cardiac function in patients with resistant hypertensionJ Am Coll Cardiol2012591090190922381425
- MahfoudFCremersBJankerJRenal hemodynamics and renal function after catheter-based renal sympathetic denervation in patients with resistant hypertensionHypertension201260241942422733462
- BoulwareLEJaarBGTarver-CarrMEBrancatiFLPoweNRScreening for proteinuria in US adults: a cost-effectiveness analysisJAMA2003290233101311414679273
- AtthobariJAsselbergsFWBoersmaCPREVEND IT Study GroupCost-effectiveness of screening for albuminuria with subsequent fosinopril treatment to prevent cardiovascular events: A pharmacoeconomic analysis linked to the prevention of renal and vascular endstage disease (PREVEND) study and the prevention of renal and vascular endstage disease intervention trial (PREVEND IT)Clin Ther200628343244416750458