
Abstract
Introduction
While Nigeria accounts for only 2% of the world population, it regrettably shares 14% of global maternal death burden. Whether its reported increase in antenatal care utilization is accompanied by increased use of skilled birth attendants (SBAs) is not known. This study assessed trends in utilization of SBAs in Nigeria between 1990 and 2013 and identified its determinants.
Methods
Data from four consecutive Nigerian Demographic and Health Survey reports between 1990 and 2013 were pooled. We used basic descriptive statistics, test of association, and logistic regression to assess the prevalence, relative change, and determinants of SBA use at 5% significance level. Sample weights were applied, and adjustment was made for survey design and sampling errors.
Results
Nearly half (46.7%) of the respondents were aged 25–34 years, while half (50.3%) of the respondents had no formal education. The prevalence of SBA use increased only marginally across the years and characteristics studied, from 32.4% in 1990 to 38.5% in 2013, an insignificant 6% increase. Educated women used SBA more than women with no education (92.4% vs 13.1%), and their odds ratio of using SBA were thrice that of uneducated women (odds ratio =3.09, 95% confidence interval =2.17–4.38). Women involved in decisions regarding their use of health facility were 12% more likely to use SBAs than others who do not. Educational attainment, religion, tribe, rural/urban residence, and zone of residence were significant to the use of SBA.
Conclusion
The use of SBA was very low throughout the study period, barely at one third usage with insignificant changes over the studied period. Women empowerment, including decision-making power and residence, were the strongest determinants of SBA use. To overturn poor child and maternal health outcomes in Nigeria through SBA use, efforts should be targeted at educating girls, sexual and reproductive health education, and accessible and improved health care facility services.
Introduction
Recent statistics show that while Nigeria accounts for only 2% of the world population, it carries 14% of global maternal death burden.Citation1 Maternal and newborn health, therefore, continues to be a major challenge in Nigeria despite approximately a half decrement in the maternal mortality rate (MMR) in the past 23 years (1,200 deaths per 100,000 live births in 1990 to 560 deaths per 100,000 live births in 2013).Citation1,Citation2 Little evidence abounds on the reasons for the decline so far. A regional study conducted in northern Nigeria showed an increase in skilled birth attendants (SBAs) use during delivery.Citation3 In addition, the Demographic and Health Survey (DHS) reports showed that antenatal care (ANC) visits in Nigeria increased from 45% in 2008 to 61% in 2013.Citation2 These buttresses the argument of Tey et al that reduction in maternal death and morbidities could be achieved through the effective use of ANC services, SBA, and postnatal care services.Citation4
However, ANC utilization does not seem to have translated to the use of SBA. The degree of progress recorded in the use of SBA over the years in most developing countries is not commensurate with an increase in ANC utilization.Citation5 In Nigeria, while 61% of pregnant women received ANC services, only 36% utilized SBA.Citation2,Citation6,Citation7 The situation is not different in other neighboring West Africa countries. For instance, recent Ghanaian studies showed that ANC utilization is increasing faster than SBA use.Citation8–Citation10 This is despite the fact that SBA use has been reported to contribute more to maternal death reduction than ANC visits.Citation11,Citation12
The advantages of SBA use during deliveries cannot be overemphasized. It increases the chances of safe delivery and also abates potential morbidity and mortality among mothers and newborns.Citation13,Citation14 The skills and performance of persons rendering assistance during delivery influence the chances of proper management of complications and hygienic practices.Citation2 First-birth delivery using SBA may influence future use of SBA for subsequent deliveries though preconditioned by the availability and quality of services.
A meta-analysis of available literatures on SBA in some databases grouped the identified 20 determinants into four: “1) sociocultural factors; 2) perceived benefit/need of SBA; 3) economic accessibility; and 4) physical accessibility.”Citation13 However, there are other determinants of SBA use beside the 3Ps – perceived needs/benefits, perceived accessibility of maternal health services, and perceived quality of care.Citation14,Citation15 Apart from sociocultural and economic characteristics, a recent study conducted in Nigeria highlighted attitudes of health workers, fear of stigma, and nonconfidentiality of the health workers as impediment to several pregnant women’s use of SBA.Citation16 Similar mistrusts of health care providers have been reported among persons living with HIV/AIDS.Citation17–Citation20 Acute shortages of SBA and long waiting time have also been reported as barriers to the use of SBA.Citation3
Other preconditions notable for the use of SBA in more recent literature include women’s decision-making power such as having a say on their earned money, their health care, and general household decision making. The overwhelming contribution of poverty level in mitigating the use of health care facility in Nigeria and elsewhere has been well documented.Citation6,Citation12,Citation16,Citation21–Citation23
While there are few regional studies on changes in SBA use over short periods such as 5 years in Nigeria, such studies for the entire country over a longer period are scarce. This study is therefore designed to assess the trends in utilization of SBA in Nigeria between 1990 and 2013 and to identify its determinants. With respect to SBA use in Nigeria, we provided answers to the following questions: What has changed? How significant is (are) the change (changes)? When was the change? What influenced the changes? The knowledge of trend of SBA use will aid adequate maternal health care use interventions so as to reduce the high poor maternal outcomes in Nigeria. Risk factors of SBA use were also identified so as to provide evidence-based information to policymakers and program implementers on maternal and child health care. The information will aid easier decisions on necessary interventions so as to improve usage and reduce associated risks.
Methods
Data obtained from four consecutive Nigerian Demographic and Health Survey NDHS reports in 1990, 2003, 2008, and 2013 were pooled. NDHS is a cross-sectional, in design, routinely conducted, and nationally representative survey. Geographically, Nigeria is divided into 6 zones (regions), and each zone has between 5 and 7 states depending on land mass and population density. Data were collected from each of the 36 states and the federal capital territory. The survey used a multistage approach in sampling the respondents and collected information about household and reproductive health of the participants. At the first stage, local government areas (LGAs) were selected from each state, then the enumeration areas (EAs) were selected from the selected LGAs at the second stage, while the primary sampling units commonly referred to as “clusters” and households within the selected EAs were selected at the third and fourth stages, respectively. Primary information about households, sexual and reproductive health, and history was collected from women aged 15–49 years within the selected households. The birth history of all women interviewed was among the key information collected. Details of the sampling methodology have been published.Citation2,Citation24 In all, 8,781, 7,620, 33,385, and 38,984 women participated in the 1990, 2003, 2008, and 2013 survey years, respectively.
The outcome variable in this study is the use of SBA. The SBAs include doctor, nurse, midwife, and auxiliary nurse/midwife.Citation2,Citation11,Citation25 Our outcome of interest is the skill of birth attendants at the most recent birth to any woman who had given birth at least once within the 5 years preceding the survey. A total of 46,487 women had at least one child within 5 years preceding each of the survey years. This was made up of 4,892 women in 1990, 3,775 women in 2003, 18,028 women in 2008, and 20,192 women in 2013. We therefore extracted the skills of person(s) who assisted the women during their latest childbirth and other characteristics as detailed below.
Based on significant variables associated with the use of SBA in literature,Citation13,Citation26 the independent variables included in this study were the following:
Sociocultural factors: maternal age (15–19, 20–24, 25–34, and 35+ years), mother’s education (primary, secondary, secondary+, and none), marital status (never married, currently married or living with sexual partner, and formerly married), ethnicity (Hausa/Fulani, Yoruba, Igbo, and others), religion (Islam, Christian/Catholic, and others), women autonomy: women involved in how her earnings are spent (yes and no), women involvement in decisions about her use of health care facility (yes and no).
Perceived benefit/need of skilled attendance: pregnancy wanted (wanted then and not wanted then), adequacy of ANC use, based on World Health Organization (WHO)-recommended four visits (none, inadequate [one to three visits], and adequate [four or more visits]; constructed from DHS data), SBA used during previous delivery (skilled [doctor, nurse, midwife, and auxiliary nurse/midwife; constructed from DHS data] and unskilled [others]), and birth order (1, 2–3, 4–6, and 7+).
Economic accessibility: mothers currently working (yes and no), household wealth (poorest [lowest and lower], middle, and richest [higher and highest]; constructed from DHS data).
Physical accessibility: region (north central, northeast, northwest, southeast, south–south, and southwest), residence (urban and rural), and distance to health facilities is a problem (problem and no problem).
We defined women autonomy as liberty to make or contribute to decisions regarding how a woman spends her earnings and whether to visit health care facilities or not.Citation6,Citation13,Citation27 The adequacy of number of ANC visits during the pregnancy and the use of SBA or otherwise during previous delivery and self-reported difficulty women had in accessing care were assessed at system level. We also included rural/urban differentials, location of residence as well as household wealth as household-level proximate determinants.
Data analyses
We used basic descriptive statistics to show the distribution of eligible participants vis-à-vis the characteristics studied (). We carried out a bivariate analysis of the characteristics and use of SBA and reported the prevalence as well as changes in the use of SBA among the survey years (). Using both bivariate and multiple logistic regression analyses, we determined and tested the association between each of the characteristics and SBA use and reported the unadjusted odds ratio (OR) and adjusted odds ratio (aOR), respectively. The OR is the influence of individual independent variable on the use of SBA. The aOR is the influence of an independent variable on the use of SBA while controlling for other independent variables. χ2 tests of association and tests of significance of OR were performed, and significance was determined at 5%. All analyses were conducted by using Stata Version 14, and sample weights duly applied so as to make provisions for unequal sample sizes across groups. We adjusted for survey design and sampling errors in all the analyses. There are some instances where some variables were not included in earlier DHS, and analyses were not performed on such variables for the particular DHS year.
Table 1 Weighted distribution of women who had given birth in the 5 years preceding the survey by analysis variables and survey year
Table 2 Trends in the percentage of married women who had given birth in the 5 years preceding survey who used SBA
Ethics approval
We relied on the series of ethical clearance(s) granted to the survey management by Nigeria National Health Research Ethics Committee in the respective survey years as documented earlier.Citation2,Citation24 Written informed consent for participation in the study was obtained from all the participants aged 18–49 years, and additional written consent was obtained from parents and guardians of participants who had not attained the age of 18 years.
Results
Among the 8,781, 7,620, 33,385, and 38,984 women interviewed in the 1990, 2003, 2008, and 2013 survey years, respectively, only 4,892 (55.7%), 3,775 (49.5%), 18,028 (54.0%), and 20,192 (48.2%) women had had at least a child within 5 years preceding the survey. Therefore, a further analysis included only 46,887 (52.8%) of all the 88,734 women interviewed in the four surveys (not shown in the tables). In all, nearly half (46.7%) of the respondents were aged 25–34 years with <10% aged 15–19 years. On average, most (94.5%) of the women were either currently married or living with a sexual partner, while about half (50.3%) of the women had no education, which fell from 63.9% in 1990 to 46.9% in 2013. Nine of every 10 women wanted the child when they got pregnant, while 63.3% encountered problem in getting access to health care facility (). Throughout the period of 2003–2013, 86.9% and 37.8% of the women claimed to have been involved in decisions on how their earnings are spent and on their use of health care facilities.
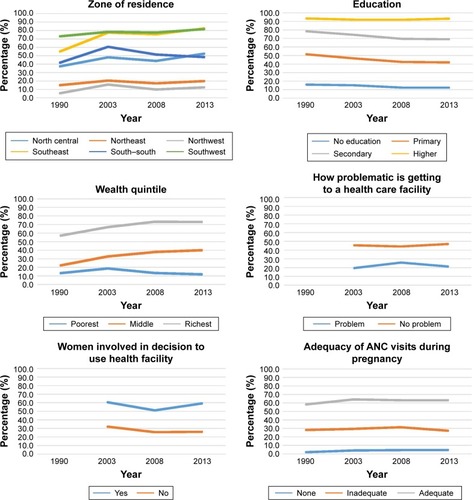
presents the prevalence of SBA use by the women by their characteristics. The estimates increased only marginally across the years studied, except by education and marital status which showed a downward trend. In all, SBA use rose from 32.4% in 1990 to 38.5% in 2013, a 5% increment. Nevertheless, more educated women had higher use of SBA compared with less educated women (92.4% vs 13.1%). The never married and formerly married women had higher SBA use compared with their currently married counterparts although SBA usage among the single women dwindled significantly. Involvement of women in how their earnings are spent did not influence SBA use significantly, but involvement in their use of health care facility was significant. Across the regions of residence, the prevalence was generally lower in the northern regions compared with the southern regions. Highest absolute change across regions was observed in southeast with 27.4% increase between 1990 and 2013. In addition, the higher the wealth quintile, adequate use of ANC, and use of SBA during previous delivery, the higher the SBA use as shown in and . Lower parity seemed to have encouraged SBA use across the years; however, the prevalence among women with >6 children fell from 30.5% in 1990 to 22.7% in 2013. Mothers who used SBA for previous pregnancy also have higher tendencies of repeating such SBA use. We found significant association among the categories of all variables considered, except women involvement in her income spending.
Figure 1 Trends in SBA utilization by selected women characteristics.
The bivariate logistic regression models showed that the use of SBA was more likely in 2013 and 2003 than it was in 1990. Women were 11% more likely to use SBA in 2013 than in 1990 (OR =1.11; 95% CI =1.04–1.19). Mothers with higher education were 80 times more likely to use SBA than those with no formal education (OR =80.2; 95% CI =68.6–93.7). Single mothers were almost double likely to use SBA than the currently married women (OR =1.75; 95% CI =1.55–1.96). Been older, Christian, from Yoruba or Igbo tribe, and living in urban area seemed to have increased likelihood of SBA use. Involvement of women in decisions regarding whether they use health care facilities or not increased SBA use by over three times (OR =3.39; 95% CI =3.25–3.54). The use of SBA at previous delivery and adequate ANC visits also increased the likelihood of SBA use by 37 (OR =36.9; 95% CI =34.1–39.9) and 98 (OR =97.9; 95% CI =89.3–107.3) times, respectively, as shown in (left panel).
Table 3 Unadjusted and adjusted determinants of SBA use among women in Nigeria
The multiple logistic regression for the use of SBA while controlling for other variables produced the adjusted ORs presented in (right panel). The only significant variables at this level are maternal age, educational attainment, religion, tribe, rural/urban residence, zone of residence, and involvement in health care facility use. Others are accessibility of facilities, wealth quintile, whether the child was wanted or not, adequate use of ANC, use of SBA at previous delivery, and parity. In the presence of other variables, there was no significant difference in SBA use by the years of survey. Mothers with higher education were thrice likely to use SBA than uneducated women (OR =3.09, 95% CI =2.17–4.38). Women involved in decisions regarding their use of health facility were 12% more likely to use SBA than others who do not. Usage of SBA was significantly higher in other regions compared with the northwest, and the highest and lowest likelihoods were found in the southwest (OR =1.98, 95% CI =1.34–2.50) and northeast (OR =1.26, 95% CI =1.04–1.53), respectively. Women who had adequately accessed ANC were five times more likely to use SBA, relative to those who did not attend ANC (OR =5.45, 95% CI =4.63–6.41), and repeated use of SBA was 31 times more likely among women who used SBA during previous delivery than those who did not (OR =31.1, 95% CI =27.7–34.4). Women who stated that distance to health care facility was not a problem were significantly more likely to use SBA (OR =1.31, 95% CI =1.15–1.48), as were those who did not want the child (OR =1.22, 95% CI =1.03–1.44). Furthermore, the odds of SBA use was 45% times higher in urban areas than in rural areas (OR =1.45, 95% CI =1.27–1.66).
Discussion
In this study, we reviewed the trends in the use of SBA in Nigeria and also identified pertinent risk factors influencing the use of SBA. We analyzed four consecutive NDHS reports in 1990, 2003, 2008, and 2013. The distributional characteristics of the women and the observed pattern in use of SBA over these two decades are of importance. While our findings showed that a half of the women had at least a birth with almost all the reference child wanted, the rate of woman participation in the decisions on how their earnings were spent and their use of health care within the last 10 years (2003–2013) was alarming and constituted a major concern. Surprisingly, only a minimal upward trend of 6% was observed in the use of SBA within the 23-year period, which was characterized with fluctuations in 2003 and 2008.
Going by the reported increase in the use of ANC in the national surveys and empirical studies,Citation2,Citation6,Citation7 a corresponding increase in the use of SBA would have been expected, but our results showed that only marginal changes occurred. This is further consummated by past studies conducted in northern NigeriaCitation3 and another west African country, Ghana,Citation8–Citation10 that SBA use has remained low. However, the 11% success rate in SBA between 2003 and 2013 might be due to various investments and intervention programs conducted over these years: for instance, increased government participation in health sector at all levels, enhanced capacity and increased staff strength, expanded coverage and equipping of the primary health care facilities and better operation platforms obtained through the Millennium Development Goals debt relief gains, Midwives Service Scheme, the Subsidy Reinvestment and Empowerment Program, Maternal and Child Health, and perhaps the sustained gained attention in complete childhood immunization and HIV/AIDS prevention.Citation28
Despite these efforts and initiatives, the nonuse of SBA during delivery had brought about morbidities as a result of complications and eventual maternal and newborn deaths. Reports have shown that MMR in Nigeria is as high as 560 per 100,000 with neonatal mortality rate of 37 per 1,000 live births providing Nigeria a rate more than the sum of all neonatal mortalities across the entire Africa.Citation2,Citation6,Citation7,Citation29 These negative health burdens though directly affect the mothers and newborns, the burden on families, communities, and the country is overwhelming. While a recent WHO report suggested that MMR in Nigeria had crashed by 53% between 1990 and 2013,Citation5 the estimate of 576 per 100,000 for 2013 was not significantly different from the estimate of 545 per 100,000 in 2008.Citation2 In addition, our findings suggested only a marginal increase of 6% in SBA use within the same period, averaging 35% utilization within the 1990–2013 window,Citation5 it is not certain whether the MMR target of 70 per 100,00 will be met in Nigeria.Citation30
In addition, a preponderance of factors also interplayed in explaining the changes in SBA use observed in the study. These factors remained consistent at both bivariate and multivariate levels of analysis. Education and residence were found to have mostly influenced SBA use. Similar findings have been reported earlier.Citation26 Outstandingly, low educational attainment and rural residence have been widely reported as a disadvantage to the use of SBA.Citation6,Citation11,Citation31,Citation32 Researchers have attributed the wide gap difference in the use of SBAs occasioned by educational attainment to wide gap in perceived need, but attributed household wealth inequalities to residential settings.Citation10,Citation33,Citation34
In general, SBA use is lower in the northern region particularly in the northeast compared with the southern women, especially women in the southwestern regions. Besides the recent terrorist attacks in the former, the regions have long been reported to lag behind in the uptake of maternal and child health services.Citation3,Citation35 Nevertheless, better individual social status such as higher levels of education, wealth status, and working status among women in the southwest regions could have influenced the differences. Literature is replete on the fact that demands for SBA use are affected by social pedigree of women such as education, ownership of property, and employment status.Citation15,Citation26 Our finding suggests that achieving steady progress in the use of SBA depends so much on women empowerment, since better empowerment has been linked to higher propensity of using SBA both in the past and in the recent times.Citation6,Citation11,Citation31,Citation32 In the same vein, studies conducted in neighboring West African countries have associated inequalities in the use of SBAs to socioeconomics factors. The studies showed disparities in socioeconomic status and also identified the ordinal contributions of education and wealth through the intermediate factors to utilization of SBAs.Citation10,Citation33,Citation34 Physical accessibility of SBA, measured by distance to health care facility, and economic accessibility expressed by women autonomy were not significant to SBA use. Financial autonomy, which we defined as participation in decisions about how women’s income are spent (a well-known indicator for empowerment), is not associated with SBA use at deliveries. This is an indication that the level of women earnings may influence financial autonomy more than her participation in decisions on how her earnings are spent since earnings are most likely to be correlated to the level of educational attainment, at least in contemporary African setting. This suggests that empowerment should go beyond participation in decision makings and focus more on other empowerment indicators such as education and employability. However, woman participation in decisions to use health care facilities seemed to have increased odds of SBA use thrice compared with those without such opportunity. This finding is corroborated by earlier studies.Citation6,Citation13,Citation27 As women get more involved in taking proactive decisions regarding their health and as they move up to better wealth status, they get more empowered to use SBA since differences in wealth quintiles have been found to be rooted in the spatial gaps that exist in the residential settings. Similar assertions have been made earlier.Citation14,Citation15
The parity and wantedness of the index child preempt the women’s perceived benefit/need of SBA. Women who are pregnant for the first time exhibit more cautions than others and thus may attract more positive attitude. Pregnant women must therefore be encouraged to use SBA right from the first pregnancy as a strategy to ensuring usage during succeeding deliveries. This may be connected with more emotional and psychological preparedness enjoyed during the first pregnancy compared with higher-order parities.Citation2,Citation13,Citation14 On the contrary, we found women who did not want the pregnancy to have higher use of SBA. This finding might have been influenced by other characteristics of the involved pregnant women.
Experience of women during ANC visits and most importantly during their previous child delivery is highly consequential for their subsequent use as found in the current study. Women who perceived the quality of services in delivery as optimally acceptable would have higher likelihood of using SBA again. Similar assertion has been made earlier with respect to the use of ANC.Citation12 In addition, previous experience with birth attendant may affect reuse of SBA. This is in consonance with earlier findings that ascribed negative attitude of health workers and poor confidentiality as hindrances to the use of SBA.Citation16 The nonuse of SBA may be worst among women who felt that their health reports, particularly those living with HIV/AIDS, are not treated confidentially. This might stir up a fearful and negative disposition among the women.Citation17–Citation20
Study limitations and strengths
There were no means of verifying the information supplied on the use of SBA by the women. It is not impossible that the data might have suffered recall bias. However, the national representativeness of huge data collected from four waves of survey in studying the trends in the use of SBA and its determinants has made our findings much more reliable, unlike the commonly utilized hospital records in most studies. The uniqueness of our study in data type, sample size, and methodology among others could serve as a benchmark, underpinning subsequent national studies in related topics.
Conclusion
The use of SBA has remained very low throughout the periods covered at barely one third usage. The 6% difference recorded between 1990 and 2013 was not significant. Sociocultural factors, maternal education, and urban residence are strong determinants of SBA use. Women autonomy, in particular with reference to their involvement in decisions on their use of health care facility and economic and physical accessibilities, influenced the use of SBA. Women who adequately use ANC and whose previous birth and experience were encouraging had a repeated use. Efforts geared at increasing the use of SBA should take a holistic approach as this will fast-track the ongoing slow progress. Such efforts should be targeted at girl child education, better family planning methods, sexual and reproductive health education, and accessible and improved health care facility services so as to overturn poor children and maternal health outcomes in Nigeria. However, an effective and efficient collaboration is necessary between the education sector and the government health apparatus so as to achieve optimal education needed to empower and enlighten women on the use of SBA.
Availability of data and materials
All materials, data, and methods used for this study are readily available at the website of Measure DHS and ICF Macro, USA.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
We acknowledge ICF Macro and the National Population Commission on behalf of the Federal Government of Nigeria for granting us access to the data used for this study. The authors received no funding for this study. AFF and OBY are researchers of Medical Statistics in the University of Ibadan, Nigeria. AFF and ESI are researchers in the School of Research and Postgraduate Studies, Faculty of Human and Social Sciences, North West University, Mafikeng, South Africa. EOH is a researcher of Demography and Social Statistics at Obafemi Awolowo University, Nigeria.
Disclosure
The authors report no conflicts of interest in this work.
References
- WHO, UNICEF, UNFPA, World Bank, UN Population DivisionTrends in Maternal Mortality: 1990 to 2013 EstimatesGeneva, SwitzerlandWorld Health Organization2014
- National Population Commission (Nigeria) and ICF InternationalNigeria Demographic and Health Survey 2013Abuja, NigeriaNational population Commission2014
- GaladanciHIdrisSSadaukiHYakasaiIPrograms and policies for reducing maternal mortality in Kano State, Nigeria: a reviewAfr J Reprod Health201014303136
- TeyNLaiSCorrelates of and barriers to the utilization of health services for delivery in South Asia and sub-Saharan AfricaSci World J20132013111
- WHOWorld Health Statistics, 2015Washington DCWorld Health Organization2015 Available from: http://apps.who.int/iris/bitstream/10665/170250/1/9789240694439_eng.pdfAccessed September 2, 2016
- FagbamigbeAFIdemudiaESBarriers to antenatal care use in Nigeria: evidences from non-users and implications for maternal health programmingBMC Pregnancy Childbirth2015159511025591791
- Federal Ministry of Health NigeriaNational HIV/AIDS and Reproductive Health and Serological Survey, 2012 (NARHS Plus)Abuja, NigeriaFederal Ministry of Health2013
- D’AmbruosoLAbbeyMHusseinJPlease understand when I cry out in pain: women’s accounts of maternity services during labour and delivery in GhanaBMC Public Health2005514016372911
- TunçalpOHindinMJAdu-BonsaffohKAdanuRListening to women’s voices: the quality of care of women experiencing severe maternal morbidity, in Accra, GhanaPLoS One20127e4453622952992
- MoyerCAAdongoPBAborigoRAHodgsonAEngmannCM‘They treat you like you are not a human being’: maltreatment during labour and delivery in rural northern GhanaMidwifery20143026226823790959
- LincettoOMothebesoane-anohSGomezPMunjanjaSAntenatal Care: Opportunities for Africa’s NewbornsNew YorkWorld Health Organization2010 Available from: http://www.who.int/pmnch/media/publications/aonsectionIII_2.pdfAccessed September 2, 2016
- FagbamigbeAFIdemudiaESWealth and antenatal care utilization in Nigeria: policy implicationsHealth Care Women Int2016381173727537979
- GabryschSCampbellOMStill too far to walk: literature review of the determinants of delivery service useBMC Pregnancy Childbirth200991–93419671156
- KyeiNNCampbellOMGabryschSThe influence of distance and level of service provision on antenatal care use in rural ZambiaPLoS One201271016
- FapohundaBMOrobatonNGWhen women deliver with no one present in Nigeria: who, what, where and so what?PLoS One201387e6956923936047
- EnvuladuEAAgboHALassaSKigbiJHZoakahAIFactors determining the choice of a place of delivery among pregnant women in Russia Village of Jos North, Nigeria: achieving the MDGs 4 and 5Int J Med Biomed Res201322329
- BasseyEBElemuwaCOAnukamKCKnowledge of, and attitudes to, acquired immune deficiency syndrome (AIDS) among traditional birth attendants (TBAs) in rural communities in Cross River State, NigeriaInt Nurs Rev20075435435817958664
- IyaniwuraCAYussufQUtilization of antenatal care and delivery services in Sagamu, south western NigeriaAfr J Reprod Health20091311112220690266
- EnwerejiEEEnwerejiKOAssessing factors that affect childbirth choices of people living positively with HIV/AIDS in Abia State of NigeriaOman Med J201025919922125708
- EzeanochieMCOlagbujiBNAgholorKNOkonofuaFEAttaining MDG 5 in northern Nigeria: need to focus on skilled birth attendanceAfr J Rep Health201014915
- TitaleyCRDibleyMJRobertsCLFactors associated with underutilization of antenatal care services in Indonesia: results of Indonesia Demographic and Health Survey 2002/2003 and 2007BMC Public Health20101048520712866
- FagbamigbeAFBamgboyeEAYusufBOThe Nigeria wealth distribution and health seeking behaviour: evidence from the 2012 national HIV/AIDS and reproductive health surveyHealth Econ Rev20155525853003
- OnonokponoDNOdimegwuCOImasikuEAdediniSContextual determinants of maternal health care service utilization in NigeriaWomen Health20135364766824093448
- National Population Commission (Nigeria) and ICF InternationalNigeria Demographic and Health Survey, 2008New YorkDHS Measure MacroAbuja, NigeriaNigeria Population Commission2009
- WHOWHO Antenatal Care Randomized Trial: Manual for the Implementation of the New Model-WHO Program to Map Best Reproductive Health PracticesGenevaWorld Health Organization2002
- AustinAFapohundaBLangerAOrobatonNTrends in delivery with no one present in Nigeria between 2003 and 2013Int J Womens Health2015734535625897265
- FagbamigbeAFIdemudiaESAssessment of quality of antenatal care services in Nigeria: evidence from a population-based surveyReprod Health20151281925561377
- National Primary Health Care Development AgencyNational Guidelines for Development of a Primary Healthcare System in Nigeria (4th Revised Edition)Abuja, NigeriaFederal Ministry of Health2012
- OestergaardMZInoueMYoshidaSNeonatal mortality levels for 193 countries in 2009 with trends since 1990: a systematic analysis of progress, projections, and prioritiesPLoS Med201188e100108021918640
- United NationsSustainable Development Goals (SDG)Washington, DCUnited Nations2015 Available from: http://www.un.org/sustainabledevelopment/sustainable-development-goals/Accessed July 5, 2016
- BabalolaSFatusiAODeterminants of use of maternal health services in Nigeria: looking beyond individual and household factorsBMC Pregnancy Childbirth200994319754941
- ArthurEWealth and antenatal care use: implications for maternal health care utilisation in GhanaHealth Econ Rev201221422866869
- AndersenHM“Villagers”: differential treatment in a Ghanaian hospitalSoc Sci Med2004592003201215351468
- AfulaniPAMoyerCExplaining disparities in use of skilled birth attendants in developing countries: a conceptual frameworkPLoS One201611e015411027105309
- DoctorHBairagiRFindleySEHelleringerSNorthern Nigeria Maternal, Newborn and Child Health Programme: selected analyses from population-based baseline surveyOpen Demogr J201141121