
Abstract
Purpose
Lifestyle intervention studies performed during pregnancy have shown inconsistent results in relation to prevention of gestational diabetes mellitus (GDM). Therefore, the aim of this study was to assess the effect of an intervention initiated already before pregnancy in prevention of GDM in high-risk women.
Patients and methods
A randomized controlled trial was conducted in four Finnish maternity hospitals between the years 2008 and 2014. Altogether 228 high-risk women planning pregnancy were randomized to an intervention (n=116) or a control group (n=112). The risk factors were body mass index ≥30 kg/m2 (n=46), prior GDM (n=120), or both (n=62), without manifest diabetes at study inclusion. Trained study nurses provided individualized lifestyle counseling every 3 months in addition to a group session with a dietician. The control group received standard antenatal care. GDM was defined as one or more pathological glucose values in a 75 g 2-hour oral glucose tolerance test, performed between 12 and 16 weeks of gestation and if normal repeated between 24 and 28 weeks of gestation.
Results
Within 12 months, 67% of the women (n=72) in the intervention group and 63% of the women (n=71) in the control group (p=0.84) became pregnant. The cumulative incidence of GDM among the women available for the final analyses was 60% (n=39/65) in the intervention group and 54% (n=34/63) in the control group (p=0.49). GDM was diagnosed already before 20 weeks of gestation in 60% (n=44/73) of the cases.
Conclusion
The preconceptional lifestyle intervention applied in the present study did not reduce the incidence of GDM.
Introduction
During the last decades, both prevalence of overweight and obesityCitation1 and consequently the incidence of gestational diabetes mellitus (GDM) have increased.Citation2 GDM refers to glucose intolerance that is first recognized during pregnancy.Citation3 Both genetic predisposition and environmental risk factors play a role in its pathogenesis.Citation4 High body mass index (BMI)Citation5 and prior GDMCitation6 are associated with an increased GDM risk. Obesity and gestational diabetes are independent risk factors for several short-termCitation7–Citation9 and long-term adverse maternal and neonatal outcomes, including type 2 diabetes (T2D).Citation10–Citation12
Lifestyle interventions are known to be effective in the prevention of T2D,Citation13 but studies assessing the effect of such interventions during pregnancy on perinatal and neonatal outcomes have produced inconsistent results.Citation14–Citation18 In 2015, a Cochrane review assessing combined diet and exercise interventions during pregnancy aiming at prevention of GDM and associated adverse outcomes concluded that no effect had been seen on the development of GDM, the rate of caesarean sections, or large-for-gestational-age newborns.Citation19 A more recent meta-analysis with data including 11,487 pregnant women concluded, however, that lifestyle interventions initiated before 15 weeks of gestation reduced the risk of GDM by 20%.Citation20 Furthermore, adherence to a healthy lifestyle both before and during pregnancy is associated with a lower GDM risk.Citation21,Citation22 As reviewed by Catalano and deMouzon,Citation23 maternal prepregnancy and early pregnancy metabolic conditions program early placental function and increase the expression of maternal lipogenic and inflammatory genes related to complications of fetal overgrowth and GDM. Thus, an intervention initiated before pregnancy could theoretically have a significant impact on the incidence of GDM and related complications.
This study is part of the Finnish Gestational Diabetes Prevention Study (RADIEL) that aimed to prevent GDM and its complications in high-risk women through a combined physical activity and dietary intervention initiated either before pregnancy or during early pregnancy. The intervention that was initiated during early pregnancy succeeded in reducing GDM incidence by 36% among women with normal oral glucose tolerance test (OGTT) in the first half of pregnancy.Citation24 In this manuscript, we present the results of the high-risk study population in which the intervention was initiated already in the prepregnancy period with the aim to reduce the prevalence of GDM. To our knowledge, no previous randomized study with the aim to prevent GDM with a lifestyle intervention initiated in the prepregnancy period has been published.
Patients and methods
The Finnish RADIEL study is a multicenter randomized controlled trial conducted between February 2008 and January 2014 targeting women at high risk for GDM. The study took place in the three maternity hospitals of the Helsinki metropolitan area (Department of Obstetrics and Gynecology, Helsinki University Hospital (HUH); Kätilöopisto Maternity Hospital; and Jorvi Hospital) and in the South Karelia Central Hospital (SKCH), Lappeenranta, Finland. The study was designed to evaluate the efficacy of a combined diet and physical activity intervention in GDM prevention. The intervention design and methods have been published in detail elsewhere.Citation25 This study focuses on the part of the RADIEL study in which the intervention was initiated before pregnancy.
Participants
Eligible participants were women aged 18 years or older, planning pregnancy within 1 year, with BMI ≥30 kg/m2 or a previous history of GDM, and with no overt diabetes at inclusion. T2D at inclusion was defined as fasting plasma glucose ≥7.0 mmol/L, 2-hour plasma glucose level ≥11.1 mmol/L in a 75 g OGTT, or glycated hemoglobin (HbA1c) ≥48 mmol/mol.Citation3 Other exclusion criteria were use of medication that influences glucose metabolism (such as continuous oral corticosteroids or metformin), multiple pregnancy, physical disability, current substance abuse, severe psychiatric disorder, and significant difficulty to cooperate (such as insufficient Finnish language skill). The women who did not become pregnant within 1 year from their first visit were excluded from further analyses. Personal invitation letters were sent out based on hospital registry data, and notices in antenatal clinics, newspapers, and social media served as additional means for recruitment.
In the randomization procedure, we used computer-generated randomly permuted blocks, stratified by risk factors used as inclusion criteria (BMI ≥30 kg/m2, prior diet-treated GDM, and prior drug-treated GDM) and the four study sites (ie, 12 strata in total). An independent statistician outside the study group created the randomization sequence and prepared the opaque randomization envelopes. Study nurses then allocated each participant to the next sequentially numbered subject code and the corresponding envelope in the appropriate stratum containing information on the intervention arm.
Intervention
Participants visited the study nurse once every 3 months before pregnancy. During pregnancy, they had structured educational visits with the study nurse once in each trimester in addition to visits to local antenatal clinics according to standard practice. During the study visits, those in the intervention arm received individually modifiable dietary and physical activity counseling from trained study nurses. For example, if during pregnancy there were problems such as antenatal contractions and the participant was unable to exercise, the counseling focused more on dietary aspects. At each study visit, participants also filled in questionnaires and underwent a physical examination that included anthropometric and blood pressure measurements and collection of blood samples as described in detail elsewhere.Citation25 In addition, participants in the intervention arm attended a group visit with a dietician at the time of study enrollment.
Dietary counseling in the intervention group focused on encouraging the use of vegetables, fruits, and berries; high-fiber whole grain products; low-fat dairy products; vegetable fats high in unsaturated fatty acids; fish and low-fat meat products; and lower intake of sugar-rich foods.Citation26 The recommendation for physical activity in the intervention group aimed at achieving a minimum of 150 minutes of moderate intensity physical activity in a weekCitation27 and adopting an overall active lifestyle, for example, by increasing household and commuting physical activity. With the assistance of a study nurse, each participant planned an individualized physical activity program that was updated during the follow-up.
In the intervention group, a 5%–10% weight loss before pregnancy was recommended for women with BMI ≥25 kg/m2 at inclusion. Avoidance of weight gain during the first two trimesters was recommended for women with a prepregnancy BMI ≥30 kg/m2.
Usual care
In the control group, participants had the same number of visits to the study nurse as the participants in the intervention arm. They also completed the same questionnaires, and the same measurements were taken. At inclusion, they received information leaflets on healthy diet and exercise similar to those routinely provided by local antenatal clinics. In addition, the participants in both groups received usual antenatal care provided to all Finnish pregnant women by public primary healthcare centers. The usual care in the primary health care at the time of the trial included 10–15 visits to a nurse and two to three visits to a physician during pregnancy.
Outcomes
The primary end point was incidence of GDM. During pregnancy, participants underwent a 75 g 2-hour OGTT at ~12–16 weeks of gestation, and if normal, it was repeated at ~24–28 weeks of gestation unless insulin or metformin treatment was initiated earlier. GDM was diagnosed based on one or more pathological glucose values in the OGTT. The diagnostic thresholds were the same as recommended by the American Diabetes Association at the time of the study: fasting plasma glucose ≥5.3 mmol/L, 1-hour value ≥10.0 mmol/L, and 2-hour value ≥8.6 mmol/L.Citation28 Preeclampsia was defined as SBP of ≥140 mmHg or DBP of ≥90 mmHg occurring after 20 weeks of gestation combined with diurnal proteinuria of ≥0.3 g.Citation29 Pregnancy-induced hypertension was defined similarly but without the presence of proteinuria. Essential hypertension was defined with similar blood pressure levels occurring before 20 weeks of gestation. Study physicians reviewed the obstetric records of all participants and confirmed maternal and perinatal diagnoses prior to end point analysis.
The overall quality of diet was assessed with a dietary index (the maximum points being 17) based on a food frequency questionnaire designed for this study that measured the general adherence to the recommended diet.Citation30 Evaluation of leisure time physical activity (LTPA) was based on the self-reported weekly duration of LTPA that made the participant at least slightly out of breath and sweating.Citation31
Statistics
The data are presented as mean (SD) or frequencies (%). An unpaired t-test for continuous variables and chi-squared test for categorical variables were used in comparisons between groups. We applied a logistic regression and an analysis for covariance model for adjustments of age, BMI, prior GDM status, the length of intervention before pregnancy (ie, time between the baseline visit and conception), and in addition for baseline values. In the case of violation of the assumptions (such as nonnormality), a bootstrap-type t-test was used. The Shapiro–Wilk W-test was used to test the normality of the data. All analyses were performed using STATA software, version 14.0 (StataCorp LP, College Station, TX, USA). To detect a 15% difference in the incidence of GDM between the intervention (20%) and control groups (35%; α=0.05, power=80%), a sample of 280 women (140 in each intervention arm) would be needed. With an assumed dropout rate of 40%, the total number needed is ~460.
Ethics approval and informed consent
Ethics committees of HUH (September 14, 2006, Dnro 300/E9/06) and SKCH (September 11, 2008, Dnro M06/08) approved the study. The study complied with the Declaration of Helsinki. Participants entered into the study voluntarily and signed an informed consent form.
Results
We recruited 247 women at high risk for GDM and planning pregnancy to the study. The number of women randomized was 228 (). Of whom, 116 were allocated to the intervention group and 112 to the control group. The inclusion criteria were BMI ≥30 kg/m2 in 46 (20%) women, prior GDM in 120 (53%) women, and both in 62 (27%) women. The number of women who became pregnant within 12 months from inclusion was 72 (62%) in the intervention group and 71 (63%) in the control group (p=0.84). Two (3%) of the pregnancies in the intervention group and three (5%) of the pregnancies in the control group began with embryo transfer or insemination (p=0.68). No outcome data were available for 15 (10%) of the 143 women who conceived, resulting in 128 women for the final analyses ().
Figure 1 Study flow of the participants.
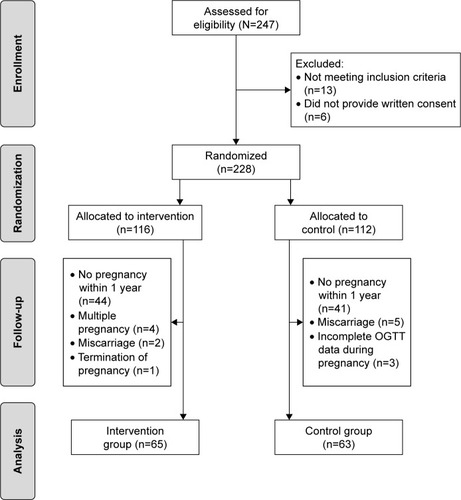
Baseline characteristics of all participants are presented in . No differences were observed in the baseline characteristics between randomized women who became pregnant compared with those who did not (data not shown), but we detected differences within intervention arms. Within the control group, women who became pregnant demonstrated a 33% obesity rate compared with a 61% obesity rate in women who failed to become pregnant (p=0.003) and 87% rate of prior GDM compared with 67% rate of prior GDM, respectively (p=0.011). Among the participants included in the final analyses, the women in the intervention group were more often obese, had a higher waist-to-hip ratio, had a higher systolic blood pressure, and had a higher low-density lipoprotein cholesterol concentration ().
Table 1 Baseline characteristics of study participants randomized and included in the final analysis
The cumulative incidence of GDM in the intervention group was 60% (n=39) and that in the control group was 54% (n=34; p=0.49 and p=0.61, respectively, after adjustments of age, BMI, previous GDM status, and the length of preconception intervention). The proportion of early GDM (diagnosis set in the OGTT performed before 20 weeks of gestation; mean 13.3 weeks [SD 2.5 weeks] of gestation) was 64% (n=25/39) in the intervention group and 56% (n=19/34) in the control group (p=0.47). In the intervention group, 33% (13/39) of the women with GDM and in the control group, 26% (9/34) of the women with GDM needed insulin or met-formin treatment (p=0.52). Of the participants with GDM in the index pregnancy, the proportion of women with prior GDM was 90% (n=35/39) in the intervention group and 91% (n=31/34) in the control group.
Women belonging to the intervention group had a crude reduction in fasting plasma glucose concentration of −0.46 mmol/L (95% CI: −0.65 to −0.27 mmol/L) from inclusion to the third trimester compared with −0.61 mmol/L (95% CI: −0.73 to −0.49 mmol/L) in those belonging to the control group (p=0.16 and p=0.77, respectively, after adjustments of age, BMI, previous GDM status, the length of preconception intervention, and baseline glucose concentration).
Gestational weight gain, calculated as weight at the third-trimester visit minus weight at the last prepregnancy visit, was 9.6 kg (95% CI: 7.8 to 11.5) in the intervention group and 9.2 kg (95% CI: 7.6 to 10.8) in the control group (p=0.71 and p=0.93, respectively, after adjustment of age, previous GDM status, the length of preconception intervention, and baseline weight).
Between the baseline and the first trimester visits, the participants in the intervention group increased their self-reported weekly mean LTPA by 24 minutes (95% CI: −15 to 63 minutes), whereas the change in the control group was negative, −12 minutes (95% CI: −50 to 25 minutes; p=0.18). In the intervention group, the participants improved their diet, ie, their dietary index increased by 1.2 points (95% CI: 0.4 to 2.1 points), whereas the change was 0.6 points (95% CI: −0.1 to 1.4 points) in the control group (p=0.28). Further adjustments did not influence these findings.
In the intervention group, 25 (38%) of the participants and in the control group, 33 (52%) of the participants attended only one study visit before pregnancy. The mean duration between the baseline visit and conception was 4.6 months (SD 3.6 months) in the intervention group and 3.8 months (SD 3.7 months) in the control group (p=0.26). In the intervention group, participants had on average 2.9 visits (range 1–6 visits) and in the control group, 2.8 visits (range 1–5 visits) with the study nurse before the first OGTT in pregnancy (p=0.12).
No differences were seen between the groups for obstetric or neonatal outcomes (). Further adjustments did not change these results.
Table 2 Maternal and neonatal outcomes in the intervention and control groups
Discussion
The need for pre- and interconception care programs, including prevention of recurrence of GDM, has been acknowledged.Citation23,Citation32 The preconceptional lifestyle intervention applied in the RADIEL study did not modify the risk for GDM among high-risk women. The incidence of GDM was high in both the intervention and the control groups, and a majority of the women were diagnosed already in the first half of pregnancy.
A preconception intervention study, aiming at improvement in health-related behavior and weight management before and during pregnancy, reduced gestational weight gain in the intervention group, but the difference between the study groups was nonsignificant when adjusted for baseline adiposity.Citation33 Another trial with tailored preconception dietary and lifestyle counseling reported an improvement in the quality of diet and a decrease in harmful behaviors, including consumption of alcohol, in subfertile couples, but no pregnancy outcomes were reported.Citation34 In a recent trial assessing the effect of a 6-month lifestyle intervention before pregnancy on the rate of live births within 24 months in obese infertile women, a greater weight loss was achieved in the intervention group.Citation35 The rate of GDM was a secondary outcome, and no difference was observed between the groups.Citation35 To the best of our knowledge, no previous intervention study initiated in prepregnancy and aiming specifically at prevention of GDM has been published.
One strength of this study is that the intervention protocol is applicable to a primary healthcare setting. We also managed to recruit high-risk women. In previous T2D prevention studies, as well as in our GDM prevention study RADIEL initiated in early pregnancy, lifestyle interventions had the largest impact on participants with the highest diabetes risk.Citation13,Citation24 In this study, 80% of all participants had a history of GDM, emphasizing their high risk for GDM, given that the reported global recurrence rate of GDM ranges between 30% and 84%.Citation6
In the present study, the implementation of a prepregnancy intervention turned out to be challenging. During the study period, recruiting high-risk women planning pregnancy was difficult. This was the case particularly in relation to nulliparous women. The most effective method of recruiting participants was by personal invitation letters based on information obtained from hospital registries on prior GDM, which may have caused a selection bias. In addition, the pregnancy rate within 1 year among the participants turned out to be low, which complicated the study setting further by increasing the dropout rate as compared with assumptions made prior to the study. It is further possible that some women participating in the trial had changed their intention to get pregnant, but we lack data on this possibility. Wishes regarding pregnancy can change quickly.Citation36 Information on the duration of possible pregnancy attempts before study inclusion was also not collected. It is possible that our high-risk population presents a group of subfertile women, which might have confounded the outcomes. Among women with successful pregnancies, however, no difference was seen between the intervention and control groups in use of infertility treatments. No data were collected regarding the possible infertility treatments among women who failed to conceive.
The recruitment goal was not reached during the 4-year recruitment period. Therefore, the final number of women available for the primary outcome analyses, and consequently the statistical power, remained too small to reliably establish the association between the intervention and GDM incidence. Neither the Finnish national guidelines for diagnosis and treatment of GDM nor the practice of antenatal care changed during the recruitment and follow-up period of the present study, reducing the possible effect of the long recruitment period on the study.
The women who became pregnant and had been allocated to the intervention group were more often obese and presented a more unfavorable lipid profile compared with those in the control group, indicating a greater metabolic burden in the intervention group, which may have confounded the effects of the intervention.
The women with a high risk of GDM form a highly heterogeneous group. Although obesity is a well-established risk factor for GDM, not all obese women develop GDM. In our early pregnancy intervention study, the highest prevalence of GDM, 36%, was seen among nonobese participants with prior GDM compared with the prevalence among obese women of 10% for nulliparous and 12% for multiparous without prior GDM.Citation37 The proportion of these nonobese women with prior GDM in the present study was 53%, which is greater than the 34% in our early pregnancy intervention.Citation37 The limited size of the study population, however, prevents further analyses of the subgroups of participants: obese women without history of GDM, nonobese women with prior GDM, and obese women with prior GDM.
A total of 60% of the women with GDM were diagnosed already at ~12–16 weeks of gestation. It could be argued that a pathologic OGTT during the first half of pregnancy suggests preexisting T2D. However, women meeting T2D criteria at inclusion were excluded. Furthermore, the most recent recommendation of World Health Organization proposes differentiating T2D and lesser degrees of hyperglycemia (ie, GDM) at any time during pregnancy.Citation38
Compared with women with late-onset GDM, women diagnosed with early GDM are known to be more insulin resistant already before pregnancy.Citation39 Women with early onset of GDM were excluded from our prior study concerning the intervention initiated in pregnancy.Citation24 The two different study populations, women planning pregnancy and women already pregnant, are hence inherently different, which could be one explanation for the different outcome between the two interventions and lack of an effect of the prepregnancy intervention. The proportion of women with prior GDM for example was lower in our previous study (33%) compared with current study (80%).
A longer and more intense intervention, including more frequent contact with study nurses, might have been needed to influence the possible preexisting insulin resistance in these women before conception. Women in the present study needed insulin or metformin treatment more often (30%) compared with the 20% of the GDM women (unpublished data) included in our prior study,Citation24 further supporting the concept of a more severe form of GDM in the current study population.
Periconceptional nutrition influences both reproductive health and pregnancy outcomes as reviewed by Cetin et al.Citation40 In our study, 45% of participants included in the final analyses had already conceived after the first study visit. Therefore, the intervention period might have been too brief to improve maternal metabolism during early pregnancy.Citation23 For the same reason, it was impossible to assess the weight loss before pregnancy between the groups. It is also likely that the frequency of lifestyle counseling was insufficient to have a significant impact on health behavior before and during pregnancy, even though the motivation level of women planning to conceive, and pregnant women, to make and maintain positive lifestyle changes may be enhanced by hopes of having a good pregnancy outcome. In addition, the intervention was not based on any behavior theory, which can be a limitation.
It is worth keeping in mind that all the participants in the study were at high risk for GDM and during pregnancy, the women in the control group received general health advice and visited antenatal clinics outside the study protocol. Furthermore, in the control group, 19 (30%) women with early GDM received additional lifestyle counseling in their antenatal clinics starting, commencing in the first half of pregnancy. In addition, the study follow-up, including repeated measurements, may have acted as a mini-intervention in the control group. This may have influenced secondary outcomes such as glucose metabolism, quality of diet, and physical activity levels in these participants of the control group during the follow-up. The weight gain during pregnancy was similar and moderate in both groups.
Conclusion
To our knowledge, this is the first study to report a prepregnancy lifestyle intervention trial aiming at GDM prevention. Even though a lifestyle intervention initiated in the first half of pregnancy showed a 36% reduction in the incidence of GDM,Citation24 the same type of intervention initiated before conception failed to show any effect on GDM incidence. Many elements complicated the implementation of the study, and the incidence of early GDM was considerably high in our cohort of high-risk women.
More studies assessing preconceptional lifestyle interventions are needed. It is possible that a longer, more intensive, and more frequent lifestyle intervention in the preconception period in a larger study population would have an impact on the incidence of GDM and on perinatal and neonatal outcomes.Citation23 Future prevention trials need to take the problems of recruitment and low pregnancy rates observed in the current trial into account and consider the possibility of applying more intense interventions.
Data sharing statement
The data sets generated and analyzed during the current study are not publicly available due to data that could compromise research participant privacy/consent but are available from the corresponding author on reasonable request.
Author contributions
KR wrote the first draft of the manuscript, participated in the implementation of the study, prepared the database, and participated in the statistical analyses. SBK initiated the study and participated in the design and planning of the study in collaboration with MMK, MP-A, BS-L, SA, HL, and AT. JGE participated in the implementation of the study in collaboration with SBK, KR, BS-L, MMK, RPR, and EH. SBK coordinated the study in Helsinki and B-SL in Lappeenranta. AV and JM participated in the implementation and statistical analyses of the nutrition aspects of the study. HK supervised the statistical analyses. All authors contributed to the revision of the manuscript and accepted the final version. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
The authors acknowledge the contribution of the study nurses Hanna Oksa, Kirsi Arponen, Päivi Saksa, Maaret Ahola, Pirkko Haapanen, Karoliina Himanen, and Eija Kortelainen, dietitians Riitta Kivelä, and Johanna Metsälä, as well as all the women participating in the study. The RADIEL study was funded by the Jalmari and Rauha Ahokas Foundation, the Finnish Foundation for Cardiovascular Research, state funding for university-level health research of HUH and SKCH, Samfundet Folkhälsan, the Finnish Diabetes Research Foundation, the State Provincial Office of Southern Finland, the Vyborg Tuberculosis Foundation, and the Social Insurance Institution of Finland. The Finnish Medical Foundation, the Finnish Diabetes Research Foundation, the Finnish Cultural Foundation, and the Helsinki University Doctoral School in Health Sciences supported the PhD study of the first author. The Academy of Finland supported JGE (grant nos 129369, 129907, 135072, 129255, and 126775). The research leading to these results has received funding from the European Commission within the Seventh Framework Programme and EU H2020-PHC-2014-DynaHealth grant no 633595. None of the funding bodies had any role in the design of the study; collection, analysis, and interpretation of data; or writing the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
- FinucaneMMStevensGACowanMJNational, regional, and global trends in body-mass index since 1980: systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9.1 million participantsLancet2011377976555756721295846
- CoustanDRGestational diabetes mellitusClin Chem20135991310132123536513
- American Diabetes AssociationStandards of medical care in diabetes – 2014Diabetes Care201437Suppl_1S14S8024357209
- ChenLMaglianoDJZimmetPZThe worldwide epidemiology of type 2 diabetes mellitus – present and future perspectivesNat Rev Endocrinol20118422823622064493
- ChuSYCallaghanWMKimSYMaternal obesity and risk of gestational diabetes mellitusDiabetes Care20073082070207617416786
- KimCBergerDKChamanySRecurrence of gestational diabetes mellitus: a systematic reviewDiabetes Care20073051314131917290037
- OwensLAO’SullivanEPKirwanBATLANTIC DIP: the impact of obesity on pregnancy outcome in glucose-tolerant womenDiabetes Care201033357757920067952
- LandonMBMeleLSpongCYThe relationship between maternal glycemia and perinatal outcomeObstet Gynecol20111172 pt 121822421309194
- PerssonMJohanssonSVillamorECnattingiusSMaternal overweight and obesity and risks of severe birth-asphyxia-related complications in term infants: a population-based cohort study in SwedenPLoS Med2014115e100164824845218
- BellamyLCasasJ-PHingoraniADWilliamsDType 2 diabetes mellitus after gestational diabetes: a systematic review and meta-analysisLancet200937396771773177919465232
- MooreTRFetal exposure to gestational diabetes contributes to subsequent adult metabolic syndromeAm J Obstet Gynecol2010202664364920430355
- MaRCWChanJCNTamWHHansonMAGluckmanPDGestational diabetes, maternal obesity, and the NCD burdenClin Obstet Gynecol201356363364123820121
- TuomilehtoJLindströmJErikssonJGPrevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose toleranceN Engl J Med2001344181343135011333990
- Oteng-NtimEVarmaRCrokerHPostonLDoylePLifestyle interventions for overweight and obese pregnant women to improve pregnancy outcome: systematic review and meta-analysisBMC Med20121014722574949
- DoddJMTurnbullDMcPheeAJAntenatal lifestyle advice for women who are overweight or obese: LIMIT randomised trialBMJ2014348g128524513442
- PostonLBellRCrokerHEffect of a behavioural intervention in obese pregnant women (the UPBEAT study): a multicentre, randomised controlled trialLancet Diabetes Endocrinol201531076777726165396
- SimmonsDJelsmaJGMGaljaardSResults from a European Multicenter Randomized Trial of Physical Activity and/or healthy eating to reduce the risk of gestational diabetes mellitus: the DALI lifestyle pilotDiabetes Care20153891650165626112044
- Assaf-BalutCGarcía de la TorreNDuranAA Mediterranean diet with additional extra virgin olive oil and pistachios reduces the incidence of gestational diabetes mellitus (GDM): a randomized controlled trial: the St. Carlos GDM prevention studyPLoS One20171210e018587329049303
- BainECraneMTieuJHanSCrowtherCAMiddletonPDiet and exercise interventions for preventing gestational diabetes mellitusCochrane Database Syst Rev20154CD010443
- SongCLiJLengJMaRCYangXLifestyle intervention can reduce the risk of gestational diabetes: a meta-analysis of randomized controlled trialsObes Rev2016171096096927417680
- ZhangCTobiasDKChavarroJEAdherence to healthy lifestyle and risk of gestational diabetes mellitus: prospective cohort studyBMJ2014349g545025269649
- BadonSEEnquobahrieDAWartkoPDHealthy lifestyle during early pregnancy and risk of gestational diabetes mellitusAm J Epidemiol2017186332633328481961
- CatalanoPdeMouzonSHMaternal obesity and metabolic risk to the offspring: why lifestyle interventions may have not achieved the desired outcomesInt J Obes (Lond)201539464264925777180
- KoivusaloSBRönöKKlemettiMMGestational diabetes mellitus can be prevented by lifestyle intervention: the Finnish Gestational Diabetes Prevention Study (RADIEL) a randomized controlled trialDiabetes Care2016391243026223239
- RönöKStach-LempinenBKlemettiMMPrevention of gestational diabetes through lifestyle intervention: study design and methods of a Finnish randomized controlled multicenter trial (RADIEL)BMC Pregnancy Childbirth20141417024524674
- BeckerWLyhneNPedersenANordic Nutrition Recommendations 2004 – integrating nutrition and physical activityScand J Nutr2004484178187
- ACOG Committee on Obstetric PracticeACOG committee opinion. Exercise during pregnancy and the postpartum period. Number 267, January 2002. American College of Obstetricians and GynecologistsInt J Gynaecol Obstet2002771798112053898
- American Diabetes AssociationStandards of medical care in diabetes – 2008Diabetes Care200831Suppl 1S12S5418165335
- ACOG Committee on Obstetric PracticePractice bulletin# 33: diagnosis and management of preeclampsia and eclampsiaObstet Gynecol200299115916716175681
- MeiniläJValkamaAKoivusaloSBHealthy Food Intake Index (HFII) – validity and reproducibility in a gestational-diabetes-risk populationBMC Public Health201616168027475905
- BorodulinKMakinenTFogelholmMLahti-KoskiMPrattalaRTrends and socioeconomic differences in overweight among physically active and inactive Finns in 1978–2002Prev Med2007452–315716217376523
- TieuJShepherdEMiddletonPCrowtherCAInterconception care for women with a history of gestational diabetes for improving maternal and infant outcomesCochrane Database Syst Rev20175981655
- WeismanCSHillemeierMMDownsDSImproving women’s preconceptional health: long-term effects of the strong healthy women behavior change intervention in the Central Pennsylvania Women’s Health StudyWomens Health Issues201121426527121536455
- HammicheFLavenJSEvan MilNTailored preconceptional dietary and lifestyle counselling in a tertiary outpatient clinic in the NetherlandsHum Reprod20112692432244121752799
- MutsaertsMAQvan OersAMGroenHRandomized trial of a lifestyle program in obese infertile womenN Engl J Med2016374201942195327192672
- ElsingaJVan der Pal-de BruinKMle CessieSde Jong-PotjerLCVerloove-VanhorickSPAssendelftWPreconception counselling initiated by general practitioners in the Netherlands: reaching couples contemplating pregnancy [ISRCTN53942912]BMC Fam Pract2006714116824233
- HuvinenEGrotenfeltNEErikssonJGHeterogeneity of maternal characteristics and impact on gestational diabetes (GDM) risk-Implications for universal GDM screening?Ann Med2016481–2525826745028
- World Health OrganizationDiagnostic criteria and classification of hyperglycaemia first detected in pregnancy: a World Health Organization GuidelineDiabetes Res Clin Pract2014103334136324847517
- BozkurtLGöblCSPfliglLPathophysiological characteristics and effects of obesity in women with early and late manifestation of gestational diabetes diagnosed by the International Association of Diabetes and Pregnancy Study Groups CriteriaJ Clin Endocrinol Metab201510031113112025574889
- CetinIBertiCCalabreseSRole of micronutrients in the periconceptional periodHum Reprod Update2010161809519567449