
Abstract
Background
One-in-three women has experienced domestic violence, which is a serious public health problem and a human right violation. Domestic violence is a common life experience among women in Ethiopia. The tool used to assess violence against women (VAW) has not been validated to assess its consistency. Cronbach’s alpha (α, or coefficient alpha) is a measure of internal consistency, or reliability, that is, how closely a set of items are related as a group. Reliability is how well a test measures what it should. Therefore, the aim of this study was to estimate the inter-item correlation (reliability) of the tool adapted from literature.
Methods
A community-based study was conducted in Northwestern Ethiopia between November 15, 2017 and December 31, 2017. A total of 1,269 women at their permanent place of residence (specifically at their households) were recruited using the multistage stratified systematic sampling method. A structured questionnaire was adapted from literature. Also, 12 trained female data collectors collected the data using the face-to-face interview method. Data were entered into EpiData 3.1.0 and exported to SPSS 23.0 for analysis. Descriptive statistical analysis was carried out to estimate the reliability of the response(s).
Results
Overall, Cronbach’s alpha was higher than the minimum recommended value of 0.70. Cronbach’s alpha for specific sections were 0.764 for women’s decision-making autonomy (13 items); women’s accepting attitude toward justified wife-beating (five items, 0.894); physical violence (seven items, 0.876); psychological violence (15 items, 0.925); sexual violence (five items, 0.812); and inequitable gender-norms (seven items, 0.867).
Conclusion
The tool used to assess domestic VAW in Northwestern Ethiopia had a high reliability. Therefore, researchers can adapt the tool and further assess its reliability in other settings to have a common and validated tool to study VAW in a low-income countries.
Introduction
Violence against women (VAW) is a global public health pandemic and a serious human rights violation. Worldwide, one-in-three women has experienced VAW.Citation1–Citation8 Domestic VAW is a common experience in the lives of women in Ethiopia. A World Health Organization’s (WHO’s) multi-country study indicated that domestic VAW in Ethiopia was 71%, which is the highest in the world.Citation9 A systematic review conducted in Ethiopia (2000–2014) indicated that domestic VAW is a common phenomenon ranging from 20% to 78%.Citation10 Women’s favorable attitude toward justifiable wife-beating, exacerbated by traditional gender-norms is a key underlying factor explaining domestic VAW. Currently, women’s receptive attitude toward justified wife-beating has declined from 81%Citation11 to 69%;Citation12 however, this is still unacceptably high.
In response to the high prevalence of domestic VAW, the government of Ethiopia has incorporated women’s right and gender equality in the constitution [Art-35 and 89(7)Citation13 and other proclamations: Criminal code under proclamation No 414/2004 (Art 564)Citation14 and Family Code Proclamation No 213/2000].Citation15 Violence against a marriage partner or a person cohabiting, even in an irregular union, is prohibited. Moreover to help implement this, the Ethiopian Ministry of Health has developed a standard operating procedure for the response and prevention of VAW in 2016.Citation16 Most of the studies on domestic VAW that have been conducted in Ethiopia, like ours, have adapted tools from existing literature, including the WHO’s domestic VAW assessment tool.Citation13,Citation16–Citation34
Cronbach’s alpha (α, or coefficient alpha) is a measure of internal consistency, or reliability, that is, how closely a set of items are related as a group. Cronbach’s alpha is developed by Lee Cronbach in 1951, which measures reliability of the tool. Reliability is how well a test measures what it should.Citation17,Citation18 A review of all the studies showed that the level of Cronbach’s alpha of the domestic VAW assessment tools is not reported in most of the studies, which have been conducted in low-income countries (particularly Ethiopia). The consistency of the items of domestic VAW assessment tool is a core component of the studies, and Cronbach’s alpha is not estimated and reported. We could not find a literature that reported the reliability (Cronbach’s alpha) estimates of the domestic VAW assessment tool. Hence, the main objective of this study was to estimate the inter-item-correlation (reliability) of the tool adapted from any literature on domestic VAW in low-income country settings. This study tool was adapted from literature to assess the level of domestic VAW in the Northwestern Ethiopia. Therefore, this study may contribute to filling the literature gap of reliability estimates of tools that often used to assess domestic VAW.
Methods
Study design and setting
A community-based cross-sectional study was conducted in the Awi zone of Northwestern Ethiopia from November 15, 2017 to December 31, 2017. This was to serve as a baseline survey for a three-arm quasi-experimental study. Awi zone has nine districts, of which three districts were included in the study. It is located 447 km from Addis Ababa. According to the Awi zonal health department report published in June 2018, this zone has a total population of 1,285,242, of whom 631,054 (49.1%) are men and 654,188 (50.9%) are women. About 12.5% of the population in Awi zone live in urban areas. Almost 93.5% of the population are Ethiopian Orthodox Christian while 5.4% of the population are Muslim.Citation11 Very little is known about domestic VAW in Awi zone, but one study shows the level of VAW to be as high as 78.0%.Citation13
Sample size determination and sampling procedures
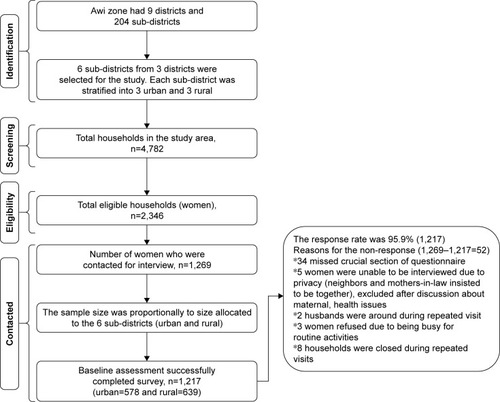
Sample size was calculated using a statistical formulaCitation19 with 5% margin of error, 95% significance level, 80% power, desired intervention effect of 13%, and design effect of 1.11.Citation12 Eventually, the final sample size was 1,269 married or cohabitating women (15–49 years). Married or cohabitating women (15–49 years) who had lived at least 12 months with their current husband and lived at least 6 months in the selected sub-districts were eligible. Three out of nine districts were selected randomly in the Awi zone by a lottery method. Then two (urban and rural) sub-districts were selected purposefully considering their appropriateness, resource, time, and geographical non-proximity to reduce threats to validity arising from possible information contamination. Sampling frame was constructed from the health extension workers’ household registry (family-folder) to recruit eligible women from each selected sub-district. Multistage, stratified, and systematic sampling methods were used to recruit women at their permanent places of residence. The first household (random start) was recruited by lottery method using the first eligible household numbers (1 to kth value =2). In the case of two eligible women being present in a single household, one woman was selected for the interview using the lottery method (). For further details, the protocol has been registered (ClinicalTrials.gov ID: NCT03265626) and published elsewhere.Citation20
Figure 1 Illustration of participant recruitment process.
The protocol was reviewed and approved by the Institutional Health Research Ethical Review Committee, College of Health and Medical Sciences, Haramaya University (Ref. No IHRERC/146/2017). This study was conducted in accordance with the Declaration of Helsinki,Citation21 and written informed consent was obtained from each study participant (woman), and the information was kept confidential and anonymous. Confidentiality of the information was maintained, among others by avoiding personal identifiers, locking the metallic cabinet for hardcopy questionnaire and investigators placing password on computers with stored data. Participant’s deidentified data that support the analysis finding of this study as well as further analysis works will be shared as per official and valid request to the corresponding author (AS). Participant deidentified data will also be available online in the protocol registration database (ClinicalTrials.gov ID: NCT03265626), and also this journal web-pages as necessary as soon as further analysis for additional manuscripts is completed on SPSS (23.0) software after May 2019. In addition, ethical approval letter is available at any time.
Tool development and data collection methods
The data collection tool was adapted from several source in the literatureCitation13,Citation16–Citation34 (). Face-to-face interviewer-administered method was carried out using the structured questionnaire administered by the 12 trained female data collectors. Data collectors’ training, pretest, and supportive supervision were provided by the principal investigator to assure the quality of data collected. Qualified female professionals (midwives, nurses, or public health workers) who have experience in field surveys and were neither resident nor deployed at nearby health facilities were hired as data collectors in order to increase the trustworthiness of the information. The training of data collectors was focused on the questionnaires, interview techniques, sampling methods, protection of confidentiality, ethical issues of domestic VAW research, and data quality assurance. Necessary amendments were made based on feedback from study participants and comments from data collectors.
Table 1 Adapted tool to measure domestic violence against women in a low-income country setting
Data processing and analysis
Overall, the domestic VAW assessment tool comprised nine sections. Three of the sections were sociodemographic and economic characteristics of women; access to sources of information about VAW and gender equality; and their husbands’ sociodemographic characteristics. The latter was not included in the reliability analysis. Six of the sections that covered the women’s decision-making potential and women’s access to household resources and control over autonomy (13 items);Citation35 women’s accepting attitude toward justified wife-beating (five items),Citation28,Citation36 physical violence (seven items), psychological violence (15 items), sexual violence (five items),Citation37,Citation38 and gender inequitable norm (seven items).Citation23 The reliability analysis was carried out for the six sections of the tool. The gathered data were entered into EpiData 3.1.0 and exported to SPSS 23.0 for further analysis. The frequency, percentage, mean, and standard deviations were computed for the participants’ sociodemographic characteristics. To examine the reliability of the tool to assess domestic VAW, the following analyses were performed: mean, standard deviation, scale mean if item deleted, scale variance if item deleted, corrected item total correlation, and Cronbach’s alpha if item deleted.
Results
The overall response rate of the survey was 95.9% (1,217/1,269). The reasons for non-response were described in detail in . The mean age of the women was 30.0 (±7.1) years. The majority of women (98.8%, n=1,202) were formally married. Slightly more than half (52.5%, n=639) of the women were rural residents. The mean of women’s marital duration was 11.5 (±7.9) years. Furthermore, the mean age of their husbands was 37.3 (±9.3) years. About one-quarter (24.9%, n=303) were unable to read and write. About half (50.7%, n=617) engaged in trade or income-generating activities. Three-fourth (75.0%, n=913) of the women’s husbands had a history of addictive substance misuse. Of these, 99.9% (n=912) of husbands had a history of alcohol consumption. Almost one-quarter (26.4%, n=321) of the women knew their husbands’ earning ().
Table 2 Sociodemographic characteristics of women, Northwestern Ethiopia, December, 2017 (n=1,217)
Cronbach’s alpha estimate of the domestic VAW questions
Cronbach’s alpha is a measure of internal consistency (reliability) of the items in the tool, usually a scale. It shows how closely a set of items are rated as a group. It is expressed as a number between 0 and 1, the closer it is 1, the higher the reliability. Internal consistency describes the extent to which all the items in a tool measure the same concept, and hence, it is connected to the inter-relatedness of the items within the tool.Citation44 The overall Cronbach’s alpha of the tool was higher than the minimum recommended value of 0.70. The women’s decision-making and household resource control autonomy were assessed using 13 items and its mean was 30.2 (±5.4). The women’s accepting attitude of justified wife-beating was assessed using five items with a mean of 10.6 (±2.6). The women’s attitude toward inequitable gender-norms was assessed using seven items with a mean of 11.1 (±2.5). Cronbach’s alpha for the women’s decision-making autonomy, women’s accepting attitude toward justified wife-beating, and inequitable gender-norm were 0.764, 0.894, and 0.867, respectively. In addition, physical domestic VAW was assessed using seven items, and the mean was 12.9 (±1.8). Psychological domestic VAW was assessed using a tool with 15 items with the mean of the scale analysis of items being 27.1 (±4.0). Sexual domestic VAW was assessed using a five-item questionnaire with the mean of the scale analysis of items being 9.2 (±1.3). The Cronbach’s alphas for physical, psychological, and sexual domestic VAW assessment questions were 0.876, 0.925, and 0.812, respectively. The overall Cronbach’s alpha of the domestic VAW assessment tool was 0.785 ().
Table 3 Item characteristics, item-total correlation, and alpha if item-deleted of the different types of domestic violence against women (VAW) assessment items (n=1,217)
Discussion
This reliability analysis estimated the consistency of response from the adapted structured questionnaire(s) that were used to assess domestic VAW. Generally, the adapted survey tool had Cronbach’s alpha score of 0.785, higher than the recommended minimum of 0.70. Specifically, Cronbach’s alphas were women’s decision-making autonomy (13 items, 0.764); women’s accepting attitude of justified wife-beating (five items with 0.894); physical violence (seven items, 0.876); psychological violence (15 items, 0.925); sexual violence (five items, 0.812); and gender inequitable norm (seven items, 0.867). This tool had a Cronbach’s alpha consistent with other studies with a range of 0.68–0.80,Citation39 higher than 0.80,Citation40 and greater than 0.90.Citation41 Furthermore, this finding is similar to that of a study conducted in Sweden which showed that the Cronbach’s alpha of the VAW assessment tool was higher than the minimum recommended value (>0.70).Citation42
In addition, the Cronbach’s alpha of the tool is also consistent with the tools used to assess the risk of domestic VAW in China which indicated a Cronbach’s alpha of 0.76.Citation43,Citation44 However, this study finding is a bit lower than a study conducted in the USA to assess VAW which showed that Cronbach’s alpha of 0.96.Citation45 Nevertheless, this finding shows a relatively higher reliability than a study conducted on measurement tool used for physician assessment which has a Cronbach’s alpha of >0.65.Citation46 There are some arguments behind the value of Cronbach’s alpha. It is argued that it is a coefficient of the reliability or internal consistency of the items, but not a statistical test.Citation44 In addition, a high value for alpha does not imply that the measure is unidimensional.
The study’s finding can motivate researchers to adopt this consistent tool, which would have a great implication on the analysis of data to inform evidence-based decision-making. This is important since concrete evidence on the level of domestic VAW to understand the problem is needed to help make appropriate decisions. Therefore, this tool can be used by researchers, policy makers, clinicians, and other key stakeholders in sub-Saharan Africa and other low-income settings to enhance studies on domestic VAW. It can also be used for need assessments, program implementation monitoring, and impact evaluations.
Strengths and limitations
This study has notable strengths including it being community-based, urban–rural mix of sample, well-defined study participants, and representative sample size that can allow for generalization of findings to the general community. However, this study also has some limitations. The disclosure of domestic VAW issues can be a sensitive private issue kept as family secret in most instances. This may be affected by social desirability bias. In addition, some women may suffer from recall bias, unable to remember some of the domestic VAW experiences that they may have accepted as a part of marital life. So social desirability and recall biases may result in underreporting of domestic VAW by the study participants.
Conclusion
The adapted tool used to assess domestic VAW in Ethiopia had high reliability. Therefore, the researcher can adapt the tool for future studies. Furthermore, assessment of the reliability of the tool in other settings is recommended to confirm its applicability as a tool for low-income countries to determine the level of domestic VAW.
Author contributions
AS, KT, AM, and AA conceived and designed the study. AS carried out activities from inception to the draft of the manuscript. AS, KT, AM, NA, and AA extensively reviewed the manuscript. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Acknowledgments
We thank Tropical Disease Research/WHO, University of Ghana, and study participants.
Availability of data and materials
The data that support the findings are available upon submitting a reasonable request to the corresponding author.
Disclosure
The authors report no conflicts of interest in this work.
References
- WHO [webpage on the Internet]Addressing violence against women and achieving the Millennium Development GoalsGeneva, Switzerland2005 Available from: https://www.who.int/gender-equity-rights/knowledge/who_fch_gwh_05_1/en/Accessed March 1, 2016
- PRBIGWG Gender-Based Violence and Reproductive Health & HIV/AIDSSummary of technical updateWashington, DC 20009–57282002 Available from: www.prb.orgAccessed March 1, 2016
- USAID, PRB IGWGGender-Based Violence: Impediment to Reproductive Health2010 Available from: https://www.popline.org/node/211911Accessed June 1, 2017
- OxfamEnding Violence Against WomenAn Oxfam Guide2012 Available from: https://www.oxfam.org/sites/www.oxfam.org/files/ending-violence-against-women-oxfam-guide-nov2012.pdfAccessed November 1, 2015
- Violence AgainstWHOWomen and HIV/AIDS: Critical Intersections Intimate Partner Violence and HIV/AIDSWHO Bulletin Series2004119
- The World Student Christian Federation and the world YWCADomestic Violence Fact SheetA 2010 Lenten Study Compiled by the World Council of Churches2010 Available from: http://women.overcomingviolence.orgAccessed May 1, 2017
- WHOGlobal regional estimates of violence against women: prevalence and health effects of intimate partner violence and non-partner sexual violenceGeneva, Switzerland2013 Available from: www.who.int/reproductivehealthAccessed December 1, 2015
- Boldosser-BoeschAByrnesDCarrCSexual and Reproductive Health and Rights (SRHR) and the Post- Development AgendaBrief Cards2015 Available from: https://www.scribd.com/document/235297283/UAP-SRHR-Post-2015-Briefing-CardsAccessed June 1, 2016
- EllsbergMJansenHAFMHeiseLWattsCHGarcía-MorenoCStudyWIntimate partner violence and women’s physical and mental health in the WHO multi-country study on women’s health and domestic violence: an observational studyLancet200837196191165117218395577
- SemahegnAMengistieBDomestic violence against women and associated factors in Ethiopia; systematic reviewReprod Health20151217826319026
- CSA, Central Statistics AgencyEthiopia Demographic and Health Survey (2011): Central Statistical Agency Addis Ababa, EthiopiaICF International CalvertonMaryland, USA2012 Available from: https://dhsprogram.com/pubs/pdf/SR191/SR191.pdfAccessed October 1, 2015
- CSA, Central Statistical agencyEthiopia Demographic and Health Survey 2016Addis Ababa, Ethiopia, and Rockville, Maryland, USACSA and ICF2016 Availbale from: www.ethiodemographyandhealth.org/Measure_DHS_Ethiopia2016.pdfAccessed June 1, 2017
- FDRE, Constitution of the Federal Democratic Republic of Ethiopia Constitution of The Federal Democratic Republic of EthiopiaAddis Ababa, Ethiopia1994 Available from: www.wipo.int/edocs/lexdocs/laws/en/et/et007en.pdfAccessed June 1, 2017
- FDRE, The Criminal Code of the Federal Democratic Republic of Ethiopia 2004Proclamation No 414/2004Addis Ababa, EthiopiaFederal Democratic Republic of Ethiopia2005 Available from: www.wipo.int/edocs/lexdocs/laws/en/et/et011en.pdfAccessed February 1, 2018
- FDREThe Revised Family Code Proclamation No 213/2000Addis Ababa, Ethiopia200096 Available from: hrlibrary.umn.edu/research/family code (English).pdfAccessed September 1, 2017
- FMOHStandard Operation procedure for the response and prevention of sexual violence in Ethiopia: Federal Democratic Republic of Ethiopia Ministry of HealthAddis Ababa, Ethiopia2016
- TavakolMDennickRMaking sense of Cronbach’s alphaInt J Med Educ20112535528029643
- Idre [webpage on the Internet]What does Cronbach’s alpha mean?Institute for Digital Research and Education, UCLA2018 Available from: https://stats.idre.ucla.edu/spss/faq/what-does-cronbachs-alpha-mean/Accessed June 1, 2018
- BiresawAAwi zone health department annual report of the population with in the zonal administration catchments on June 30th, 2018Zonal reproductive health team leader (received via phone call)Injibara, Ethiopia2018
- SemahegnABelachewTAbdulahiMDomestic violence and its predictors among married women in reproductive age in Fagitalekoma Woreda, Awi zone, Amhara regional state, North Western EthiopiaReprod Health20131016324308763
- ZhongBHow to Calculate Sample Size in Randomized Controlled Trial?J Thorac Dis 20092009115154
- SemahegnATorpeyKManuAAssefaNAnkomahACommunity based intervention to prevent domestic violence against women in the reproductive age in northwestern Ethiopia: a protocol for quasi-experimental studyReprod Health201714115529162117
- World Medical Association (WMA)World Medical association Declaration of Helsinki ethical principles for medical research involving human subjects, 5th (Edinburgh) Amendment and note of clarificationJAMA2013310202191219424141714
- NguyenPHNguyenSVNguyenMQThe association and a potential pathway between gender-based violence and induced abortion in Thai Nguyen Province, VietnamGlob Health Action201251900611
- Abebe AbateBAdmassu WossenBTilahun DegfieTAbateBAWossenBADegfieTTDeterminants of intimate partner violence during pregnancy among married women in Abay Chomen district, Western Ethiopia: a community based cross sectional studyBMC Womens Health20161611626960962
- RahmanMNakamuraKSeinoKKizukiMDoes gender inequity increase the risk of intimate partner violence among women? Evidence from a national Bangladeshi samplePLoS One2013812e8242324376536
- SapkotaDBhattaraiSBaralDPokharelPKDomestic violence and its associated factors among married women of a village Development Committee of rural NepalBMC Res Notes20169117826994899
- LamichhanePPuriMTamangJDulalBWomen’s status and violence against young married women in rural NepalBMC Womens Health20111111921612603
- DalalKWangSSvanströmLIntimate partner violence against women in Nepal: an analysis through individual, Empowerment, family and societal level factorsJ Res Heal Sci J2014144251257
- UthmanOAMoradiTLawokoSAre individual and community acceptance and witnessing of intimate partner violence related to its occurrence? Multilevel structural equation modelPLoS One2011612e2773822194791
- ShannonKLeiterKPhaladzeNGender inequity norms are associated with increased male-perpetrated rape and sexual risks for HIV infection in Botswana and SwazilandPLoS One201271e2873922247761
- AbramskyTWattsCHGarcia-MorenoCWhat factors are associated with recent intimate partner violence? Findings from the WHO multi-country study on women’s health and domestic violenceBMC Public Health201111110921324186
- IsmayilovaLSpousal violence in 5 transitional countries: a population-based multilevel analysis of individual and contextual factorsAm J Public Health201510511e12e22
- HayatiENHögbergUHakimiMEllsbergMCEmmelinMBehind the silence of harmony: risk factors for physical and sexual violence among women in rural IndonesiaBMC Womens Health20111115222112243
- AntaiDTraumatic physical health consequences of intimate partner violence against women: what is the role of community-level factors?BMC Womens Health20111115622185323
- UthmanOALawokoSMoradiTFactors associated with attitudes towards intimate partner violence against women: a comparative analysis of 17 sub-Saharan countriesBMC Int Health Hum Rights2009911419619299
- ConroyAAGender, power, and intimate partner violence: a study on couples from rural MalawiJ Interpers Violence201429586688824227592
- HeiseLLViolence against women: an integrated, ecological frameworkViolence Against Women19984326229012296014
- EllsbergMHeiseLResearching Violence against Women; A Practical Guide for Researchers and ActivistsWashington DC, United StatesWorld Health Organizationand PATH2005259
- EmamiASafipourJConstructing a questionnaire for assessment of awareness and acceptance of diversity in healthcare institutionsBMC Health Serv Res201313114523607334
- JenkinsonCCoulterAWrightLShort form 36 (SF36) health survey questionnaire: normative data for adults of working ageBMJ19933066890143714408518639
- ShakilADonaldSSinacoreJMKrepchoMValidation of the hits domestic violence screening tool with malesFam Med200537319319815739135
- SvalinKMellgrenCLevanderMTLevanderSThe inter-rater reliability of violence risk assessment tools used by police employees in Swedish police settingsNord Polit201741928
- ChanKLPredicting the risk of intimate partner violence: the Chinese risk assessment tool for victimsJ Fam Violence201227215716422448088
- ChanKLAssessing the risk of intimate partner violence in the Chinese Population: The Chinese Risk Assessment Tool for Perpetrator Assessing the Risk of Intimate Partner Violence in the Chinese Population: The Chinese Risk Assessment Tool for Perpetrator (CRAT)Violence Against Women201420550051624842058
- DienemannJGlassNHansonGLunsfordKThe domestic violence survivor assessment (DVSA): a tool for individual counseling with women experiencing intimate partner violenceIssues Ment Health Nurs200728891392517729174