Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Preterm birth is a major health problem for the neonate, family, country, and society in general. Despite many risk factors being identified for women destined to deliver preterm, short cervical length detected on transvaginal ultrasound is the most plausible, practical and sensitive risk factor for prediction of spontaneous preterm birth. The definition of short cervix has varied in various studies, but most commonly accepted is ≤2.5 cm in the midtrimester of pregnancy, though risk of spontaneous preterm birth (sPTB) increases as the cervical length decreases. Vaginal progesterone, a naturally occurring steroid hormone, is the most bioavailable form of progesterone for uterine and cervical effects with the fewest side effects. Multiple prospective studies have consistently shown its benefits in decreasing sPTB rate in women with asymptomatic midtrimester short cervix. The safety for mother and fetus, and tolerability of vaginal progesterone, particularly the gel form, is also well established. Vaginal progesterone is a minimally invasive intervention that is not painful and is very safe, with reasonable cost where the benefits (even if argued to be small) clearly outweigh the risks. Thus there should be little hesitation for implementation of universal transvaginal cervical length screening and preventive vaginal progesterone treatment for women with short cervix.
Keywords:
Overview
The incidence of preterm birth in United States in 2010 was 11.99% with 3.5% born < 34 weeks’ gestation.Citation1 This seemingly small group of neonates account for more than 75% of all neonatal deaths and 35.4% of all infant deaths.Citation2 Of the premature survivors, a quarter have substantial neurological morbidity persisting into adulthood with associated increased emotional, physical, and monetary costs to families and society.Citation3 The advancements in technology and health care have resulted in improved survival of preterm infants with resultant increase in absolute numbers of cerebral palsy cases and adolescents with cognitive deficits, academic underachieving, grade failures, and increased need for remedial assistance, as well as increase in mental disorders with associated societal consequences.Citation4 Two-thirds of preterm births in the United States are spontaneous (sPTB) and account for half of infant hospitalization costs and a quarter of pediatric costs.Citation5 In 2005, over $26.2 billion was spent in the United States on prematurity-related medical problems.Citation6 It would make sense that decrease in incidence of prematurity would benefit the mother, the child, the family, and society in general with decreased morbidity, mortality, and societal long-term burden as well as cost savings. As an example, CIGNA HealthCare reported a $6000 per pregnancy cost savings with good maternity care resulting in slight decrease in prematurity.Citation7
Short cervical length
The first step in prevention of preterm births is adequate identification of at-risk cases (). For tertiary prevention, onset of uterine contractions with cervical change or rupture of membranes makes it easy to identify patients in preterm labor. Tertiary prevention has proven to be more useful in improving neonatal morbidity with administration of corticosteroids and antibiotics, without much success in actually decreasing the number of preterm births. Therefore focus has shifted towards primary and secondary prevention and led us to identify multiple risk factors for preterm births (). However, the sensitivity as well as the positive predictive value of any one of these factors or even a combination is poor. Two of the most important predictors of preterm delivery are prior obstetrical history and cervical effacement measured as shortened cervical length (sCL) by ultrasound. Logistic regression analysis has revealed cervical length (CL) to be the single independent contributor to early sPTB (≤32 weeks) when neonatal morbidity and mortality is highest. Citation8 This also is the most plausible tool for risk assessment since cervical ripening is also the final detectable pathway prior to onset of term labor. Short cervix has been shown in many prospective trials across different populations (US,Citation9,Citation10 British,Citation8 FinnishCitation11) to predict sPTB.
Table 1 Levels of prevention
Table 2 Clinically identifiable risk factors for spontaneous preterm birth
Short cervix can be diagnosed by manual digital exam, by Cervilenz (CerviLenz, Chagrin Falls, OH), transabdominal (TAS) or transvaginal ultrasound (TVS). Manual digital exam is subjective, with high failure rate (inability to assess CL) particularly in asymptomatic women with closed cervix, and differences amongst examiners making standardization of findings difficult.Citation9 Cervilenz measures the cervico-portio length and in a single prospective trial of 189 patients, correlated with TVS for diagnosing CL < 3 cm with a sensitivity of 88% and specificity of 92%.Citation12 Its role so far appears to be in weeding out women with normal CL, requires TVS for confirming a sCL, and requires further investigation to establish role in clinical practice. Ultrasound allows objective evaluation of CL, but TVS is favored over TAS. TAS findings result in greater scatter, higher failure rates (6.7% compared to <1% with TVS),Citation13 and longer cervix estimation from full maternal bladder and resultant higher false-negative rates.Citation14 TVS is an easy skill to learn for sonographers with reported inter- and intraobserver variability of <5% (or 2–4 mm).Citation11,Citation15 TVS is highly reproducible, safe, and minimally invasive with good acceptability by women.Citation15,Citation16 CL screening by TVS meets the six criteria of a ‘good screening tool’: validity, reliability, yield, cost, acceptance, and follow-up services.Citation17 Despite the low sensitivity, the high negative predictive value (>97%) across all trials,Citation18 makes CL by TVS a useful screening tool for low-risk pregnant women. A sCL is a good screening predictor as it heralds onset of preterm delivery weeks prior, to allow for intervention to prevent it.Citation14 In addition, sCL can be diagnosed reliably and easily by ultrasound which can be performed at the time of an already scheduled visit for fetal anatomic survey. The infrastructure and equipment for TVS already exist in most centers performing fetal ultrasounds though may not be in certain geographic areas.
Many have advocated universal TVS CL screening in all singleton pregnancies.Citation19–Citation21 However, the USA Society of Maternal–Fetal Medicine (SMFM) clinical guideline states, “CL screening in singleton gestations without prior sPTB cannot yet be mandated universally,” despite acknowledging it fulfills criteria for an effective screening test.Citation22 Yet, the guideline recommends TVS CL measurements every 2 weeks in singletons with prior sPTB and provides management decisions for those who choose universal screening in all singleton gestations. This suggests SMFM is encouraging universal screening without mandating it. Resources for TVS when needed for a certain population (women with prior sPTB), as recommended by SMFM, then could also be utilized for other populations. Uncertainty of outcome of screening in actual practice compared to in controlled trials due to population differences, logistical differences in screening protocols, use of therapy beyond the scope of clinical trials or unintended adverse consequences of screening like more TVS or overuse of invasive procedures like cervical cerclage are cited as reasons against universal screening. However, these consequences are inherent in introduction of any proven test or therapy and should be a reason for formulation of strict guidelines and an effective quality assurance program, but not for not requiring the performance of a cost-effective beneficial screening test.Citation23,Citation24
The definition of ‘sCL’ is open for debate. There is no cut-off CL when the risk for sPTB is increased; instead it is a continuous variable. The risk of sPTB ≤ 32 weeks is 0.2% at CL of 60 mm at 20–24 weeks gestation, 0.8% at 30 mm, 1.1% at 25 mm, 1.5% at 20 mm, 4% at 15 mm, 15% at 10 mm, and 78% at 5 mm.Citation8 Not only does the risk of sPTB increase as the CL decreases,Citation10 there is a linear relationship between length of cervix and gestational age of prior sPTB.Citation25 In addition, the risk of sPTB for a particular CL varies depending on the gestational age it was measured. For example, a CL of <25 mm at 20 weeks has a 40% chance of sPTB < 35 weeks compared to 70% if detected at 16 weeks.Citation26 Other important factors affecting the predictability of CL include number of fetuses, patient symptoms, and prior history of sPTB. Therefore, for clinical practice, the ‘cut-off ’ CL at which to institute therapy will depend on the balance of detection rate and false positivity considered acceptable and most cost-effective. Current studies showing efficacy of therapies (vaginal progesterone or cervical cerclage) in women with ‘short cervix’ have all been in singleton gestations, asymptomatic women, and CL measured in midtrimester () in women with and without prior sPTB.Citation27–Citation31 CL ‘cut-off ’ used in different studies has varied between ≤15–25 mm. Based on current data, measurement of TVS CL is most appropriate between 19–<24 weeks and women with cervical length of 5–25 mm, with or without prior sPTB, would most benefit from vaginal progesterone;Citation20,Citation30 while women with prior sPTB and CL ≤ 15 mm would most benefit from cervical cerclage.Citation31
Table 3 Frequency of women with short cervix
Vaginal progesterone
Pharmacology, mode of action, pharmacokinetics
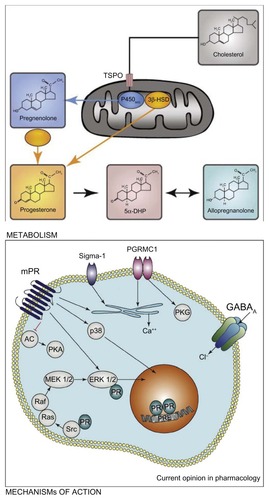
Progesterone is a naturally occurring steroid hormone produced by the adrenals, gonads, nervous system, and placenta in pregnancy. It is a derivative of cholesterol. Cholesterol is converted into pregnenolone by enzyme cytochrome P450, and pregnenolone is converted to progesterone by 3β-hydroxy-steroid dehydrogenase/Δ5, Δ4 isomerase in the smooth endoplasmic reticulum ().Citation32 Progesterone exerts its modulatory effects on target organs via intracellular receptor isoforms A (94 kDa) and B (116 kDa).Citation33 The receptors are expressed by a single gene on chromosome 11q22–q23 but have separate translational start sites and promoters. Progesterone actions via membrane-based nongenomic receptors have also been illustrated.Citation34 In therapeutics, progesterone is available in its natural form or synthetic form. Even though both forms are used for similar purposes, they are not chemically identical and their effect on target organs may not be similar.Citation32,Citation33
Figure 1 Cholesterol is converted to pregnenolone by cytochrome P450scc inside steroidogenic mitochondria. The transport of cholesterol across the mitochondrial membranes is a limiting step, and it involves the transport protein (TSPO). Ligands of TSPO can stimulate the passage of cholesterol into the mitochondria and, as a consequence, the synthesis of pregnenolone. The conversion of pregnenolone to progesterone by different isoforms of the 3β-hydroxysteroid dehydrogenase (3β-HSD) also takes place inside the mitochondria or within the cytoplasm.
Abbreviation: 5αDHP, 5α dihydroprogesterone.
The natural progesterone is chemically identical to the ovarian progesterone and synthesized from Mexican yams or soybean extracts or animal sources. Its micronization decreases particle size, increases surface area, and thus improves absorption. This results in exponential rise in bioavailability with decreased metabolic and vascular side effects.Citation35 The vaginal route further adds advantages to this form by rapid absorption and avoiding the first-pass hepatic metabolism, resulting in sustained plasma concentrations, and high bioavailability especially locally in the most desired target organ, the uterus. This has been termed as the ‘first uterine pass effect’ as progestational effects on the endometrium are seen despite low plasma levels suggesting direct transit of vaginal progesterone into the uterus.Citation36,Citation37 In addition to the above advantages, vaginal route possibly is the preferred mode of administration as the pain associated with oil-based intramuscular (IM) injections, bad taste associated with intranasal route, poor absorption and higher doses with oral route, conflicting evidence and variable effects with transdermal route, and inconvenience with the intravenous or rectal routes is avoided.
Vaginal progesterone is available in the form of gel, suppository, or pessary. Natural and micronized progesterone constitutes all the vaginal forms. Vaginal gel (Crinone/Prochieve; Watson Pharmaceuticals, Morristown, NJ) is the sustained release form with 90 mg progesterone in 1.125 g of gel with a 2% polycarbophil base. The capsule approved for oral use is used as vaginal suppository: 100 mg capsule in peanut oil (Utrogestan; Ferring Pharmaceuticals, West Drayton, UK and Prometrium; Abbott Laboratories, Abbott Park, IL). Compounded 100 or 200 mg suppositories in petroleum jelly base have also been used in USA. Recently a nonoil-based 100 mg progesterone tablet became available (Endometrin; Ferring Pharmaceuticals) for vaginal use. No pessary is available in the USA, but 200 mg and 400 mg progesterone pessary wrapped in wax is available in Europe (Cyclogest; Actavis UK, Devon, UK). All the above products are currently available and approved for other indications, but not for prevention of preterm labor.
Progesterone derives its name from ‘progestational steroid hormone’ due to its primary function of preparing and maintaining the uterine bed for conception.Citation38 Its benefits in decreasing early pregnancy loss via providing luteal support, both in women with threatened abortion and those undergoing artificial reproduction cycles, has led to its widespread use in the first trimester.Citation39,Citation40 Its role in the 2nd and 3rd trimesters of pregnancy is less clear, but its effects on the uterus (myometrium and cervix) form a biological plausible reason for its role in prevention of sPTB. Progesterone inhibits production of stimulatory prostaglandins (PG) and expression of contraction-associated protein genes in the myometrium.Citation38 Clinically, this correlates with its mild tocolytic effects and significantly decreased spontaneous uterine contractions in women receiving progesterone compared to control groups.Citation41 However, this has not translated into a clinical success as a stand-alone tocolytic, but progesterone possibly could have adjunctive role in decreasing sPTB in women with threatened or established preterm labor.Citation42
In contrast to traditional concepts, progesterone’s most significant actions appear to be on the cervix and thus in prevention rather than treatment of sPTB.Citation43,Citation44 As the ‘gatekeeper for pregnancy’,Citation45 the cervix remains firm, long and closed to contain and protect the conceptus from outside influences for the duration of the pregnancy. It remodels (softens, ripens, and dilates) to herald the onset of parturition which begins several days or weeks prior to onset of regular uterine contractions, a late step in the parturition process.Citation44 Cervical remodeling occurs with loss of tissue effects of progesterone. This is supported by the fact that administration of antiprogestins like RU-486 (mifepristone) in mid-trimester or term, results in cervical ripening not labor.Citation44,Citation46 The prolonged interval between cervical ripening and labor, allows for the opportunity to institute measures to arrest further progression of the process and prolong gestation.
Multiple mechanisms have been proposed to explain the role of progesterone in uterine quiescence and its deficiency (relative or absolute) resulting in parturition.Citation38 In many animal species, systemic drop in progesterone levels heralds the onset of parturition. However, in humans, systemic progesterone levels remain high until after delivery of the placenta. Current evidence suggests that decrease in local progesterone responsiveness, termed ‘functional withdrawal’ heralds cervical remodeling. Progesterone effects gene transcription via activation of the progesterone receptor (PR) isoforms A and B. Progesterone-responsive genes are suppressed by PR-A, but activated by PR-B (). The ratio of PR-A/PR-B determines progesterone action with an increase in PR-A expression initiating cervical ripening. Another mechanism proposed for the ‘functional’ progesterone withdrawal is a decrease in PR coactivators, resulting in impaired progesterone–PR interaction, and thus reduced expression of progesterone-responsive genes. The differential expression of the PR is hypothesized to be mediated by PGs, inflammatory cytokines, and/or estrogen activation. Progesterone also exerts anti-inflammatory actions by inhibiting the transcription factor, nuclear factor-κB, which results in decreased cyclooxygenase-2 and PG synthase actions, and low PG levels. A second pathway to suppress PG production within the endometrium/decidua is to upregulate production of the unbound secretory component of immunoglobulin A (IgA) which directly inhibits phospholipase A2 and thus suppresses endometrial PG synthesis and release. In addition to the gene effects, progesterone can act via membrane-bound receptors and nongenomic pathways to suppress cytokine mediated inflammatory response. Progesterone decreases myometrial responsiveness by inhibiting estrogen receptor-α expression, and its byproducts competitively bind to oxytocin receptors and decrease oxytocin-induced contractility. Another hypothesis proposed for timing of labor is the maturation of the fetal hypothalamic–pituitary–adrenal axis resulting in cortisol secretion which regulates placental corticotrophin-releasing hormone (pCRH).Citation47 CRH stimulates decidual PG secretion and increases myometrial responsiveness. Progesterone and cortisol have opposing actions in the fetoplacental unit and compete for regulation of pCRH gene expression. Exogenous progesterone supplementation may effectively restore some, but not all, of its actions to maintain uterine quiescence. This may explain why sPTB is prevented in some women using progesterone, but not universally. In others, the process of parturition may have progressed beyond the point of no return.
Efficacy studies
After the initial success of synthetic progesterone in prevention of recurrent sPTB in women with prior sPTB,Citation48 investigation into the use of more convenient vaginal progesterone in this high risk population was met with controversial findings.Citation41,Citation49 Looking at benefits of vaginal progesterone in other risk factors for sPTB only further heightened this controversy. The Turkish study in 150 high-risk women (with twins, uterine malformation or prior sPTB) showed lower sPTB and neonatal intensive care unit (NICU) admissions with use of 100 mg vaginal progesterone suppository,Citation50 but the Danish study in 675 twin pregnancies showed no benefit from 200 mg vaginal suppository.Citation51 However, controversial findings of these different studies suggested and helped identify a subgroup of particularly at-risk women for sPTB in which vaginal progesterone could be beneficial. The secondary analysis of the vaginal gel study in women with prior sPTB showed that using objective criteria such as ultrasonographically detected sCL, a stronger predictor of sPTB,Citation10,Citation52 was better able to identify women who could benefit from prophylactic treatment with vaginal progesterone.Citation27 The investigators showed that daily use of 90 mg vaginal progesterone gel not only decreased risk of early sPTB ≤ 32 weeks in women with CL < 28 mm identified between 18.0 and 22.9 weeks of gestation, but also improved neonatal outcomes, the ultimate goal of therapy. The sPTB rate with vaginal gel progesterone compared to placebo (Replens®; Columbia Laboratories, Inc, Livingston, NJ) was 0 vs 29.6%; P = 0.01; lower NICU admissions (15.8 vs 51.9%, P = 0.01); shorter NICU stay (1.1 vs 16.5 days; P = 0.01), and a trend towards lower occurrence of respiratory distress syndrome (RDS) (5.3% vs 29.6%; P = 0.06).Citation27 At the same time, the Fetal Medicine Foundation second trimester screening group from London, UK had reported 44% lower sPTB < 34 weeks with once-daily 200 mg progesterone suppositories (19.2% vs 34.4%; P = 0.007) in women with 20–25 week CL ≤ 15 mm.Citation28 However, they noted a nonsignificant reduction in composite adverse neonatal outcomes (8.1% vs 13.8%; P = 0.17). Subsequently the largest-to-date prospective, randomized, placebo-controlled, double-blind, parallel-group study was conducted at 44 centers in 10 countries using progesterone vaginal gel in women with 19–<24 week CL of 10–20 mm.Citation29 In the 458 women enrolled, the gel decreased sPTB < 33 weeks by 45% in comparison to placebo users (8.9% vs 16.1%; P = 0.02). There was also a 38% reduction in sPTB < 35 (14.5% vs 23.3%; P = 0.02) and a 50% reduction <28 weeks (5.1% vs 10.3%; P = 0.04). Improvement in neonatal outcome was also demonstrated with lower incidence of RDS (3% vs 7.6%; P = 0.03); lower rate of any morbidity or mortality (7.7% vs 13.5%, P = 0.04); and reduction in neonates with birth weight < 1500 g (6.4% vs 13.6%; P = 0.01). Romero and colleagues then conducted an individual patient data meta-analysis of randomized controlled trials in asymptomatic women with midtrimester CL ≤ 25 mm, as the resultant larger sample size would provide greater statistical power for subgroup analyses, improve standardization and consistency across data sets, and allow time-to-event analyses.Citation30 Analysis of 775 women (723 singleton and 52 twin pregnancies) confirmed reduction in risk of sPTB < 33 weeks in both women with singleton gestation without prior sPTB (relative risk [RR] = 0.60; 95% confidence interval [CI]: 0.39–0.92) as well as women with ≥1 prior sPTB (RR = 0.54; 95% CI: 0.30–0.98) with improved composite neonatal outcomes in both groups. In singletons, neonatal outcomes significantly improved were RDS (RR = 0.47; 95% CI: 0.27–0.81); composite neonatal morbidity and mortality (RR = 0.59; 95% CI: 0.38–0.91); apgar score < 7 at 5 minutes (RR = 0.48; 95% CI: 0.24–0.95); NICU admissions (RR = 0.67; 95% CI: 0.50–0.91); and birth weight < 1500 g (RR = 0.52; 95% CI: 0.34–0.81). The meta-analysis recommended a future, properly designed study in twin pregnancies with short cervix as the analysis showed nonsignificant reductions in early sPTB < 33 weeks (RR = 0.70; 95% CI: 0.34–1.44); and <28 weeks (RR = 0.44, 95% CI: 0.11–1.85) but significant reduction in composite neonatal morbidity and mortality (RR = 0.52; 95% CI: 0.29–0.93).
Comparative studies
Currently, there are no studies comparing any of the formulations of progesterone to each other for prevention of sPTB. However, for luteal phase support in women undergoing assisted reproductive technologies, vaginal progesterone (oil-in-capsule or the gel) was comparable to the IM form on the clinical end-points (clinical pregnancy and ongoing pregnancies).Citation53,Citation54 Pharmacokinetic comparisons have shown higher endometrial tissue levels despite lower serum levels with vaginal (1.05 ± 0.67 ng/mg protein and 4.82 ± 2.25 ng/mL, respectively) compared to IM (0.43 ± 0.19 ng/mg protein and 29.42 ± 14.14 ng/mL, respectively) preparations.Citation36,Citation55
Vaginal gel progesterone
Safety and tolerability
The synthetic progesterones administered parenterally result in undesirable side effects like alteration in lipid levels, glucose metabolism, a hypercoagulant state, vasomotility, edema, central nervous system effects like sedation, fatigue, dizziness and dysphoria, gastrointestinal effects like abdominal cramps, back pain, nausea, and constipation; reproductive system effects like vaginal bleeding and breast tenderness.Citation33 These side effects are decreased with the micronized form and systemic effects almost eliminated with the vaginal form. The most common side effects reported with the vaginal form include vaginal discharge, vaginal pruritus, drowsiness, nausea, and ‘feeling of coolness’ in the vagina.Citation29,Citation54,Citation57
The gel formulation contains 90 mg micronized progesterone mixed in a small volume of nonimmunogenic polycarbophil gel, which is an oil-in-water emulsion. The polycarbophil base attaches to the vaginal epithelial cells until they turn over every 3–5 days. The progesterone is partially soluble in both oil and water phases, with the aqueous form being absorbed by facilitated diffusion across the vaginal wall. The progesterone stored in the oil reservoir replaces the depleted aqueous form, resulting in controlled release of the drug. So the gel form does not result in leakage, unlike the suppositories which can be messy as the oil base liquefies at body temperature. The resulting leakage causes vaginal irritation and yeast infections at ten times greater frequency with suppositories compared to the gel formulation. Citation54,Citation56 However, the gel can result in vaginal build-up, cloddy discharge, and vaginal irritation in up to 2%–4% of patients in the 2nd and 3rd trimestersCitation29,Citation49 and 7% in the 1st trimester.Citation57 The increased incidence in the 1st trimester is most likely due to more frequent administration. These side effects are due to the vehicle rather than the drug itself.
Safety of progesterone is well established in the 1st trimester and exemplified by its popular use for luteal phase support in both natural and assisted pregnancies.Citation54,Citation58,Citation59 Safety in the 2nd and 3rd trimesters has only recently been established in prospectively randomized, double-blind, placebo-controlled trials.Citation28,Citation29,Citation41,Citation49–Citation51 In a meta-analysis, no difference was noted between progesterone and placebo groups with respect to congenital anomalies (1.5 vs 1.7%; 95% CI: 0.55–1.44); any maternal adverse event (13.8 vs 13.4%; 95% CI: 0.79–1.38); vaginal discharge (22.9 vs 23.5%; 95% CI: 0.87–1.15); and vaginal pruritus (5.1 vs 4.7%; 95% CI: 0.74–1.57).Citation30 Rate of therapy discontinuation due to gel side effects was 1.6% in one study (one patient stopped due to vaginal discharge and other two due to nausea)Citation49 and overall with all vaginal formulations was 2.6% in both drug and placebo groups.Citation30 Follow-up of neonates was reported in two trials, one using the suppository and the other using the gel.Citation51,Citation60 Rode and colleagues reported neurodevelopmental disability using the Ages and Stages Questionnaire (ASQ) scores in neonates exposed to progesterone suppositories in the PREDICT trial at 6 (79.2%) and 18 months (74.8%). The mean ASQ scores (193 ± 42.6 vs 194 ± 40.6; P = 0.89) or the proportions below 115 at 18 months were similar (3.8% vs 3.7%) in the progesterone and placebo groups, respectively.Citation51 Infants exposed to the vaginal gel trial were evaluated at 6 (69.9%), 12 (61.1%), and 24 months (46%) for biometric growth, developmental debilities by Denver II screening test (10.3% vs 10.4%; 95% CI: 0.62–1.55), chronic morbid conditions (5.6% vs 5.4%; 95% CI: 0.55–1.99) and congenital abnormalities (3.4% vs 3.8%; 95% CI: 0.4–2.01). Again, no differences were noted between progesterone and placebo groups in neonatal parameters up to 24 months.Citation60
Patient-focused perspectives patient satisfaction/acceptability, adherence
Overall vaginal progesterone is safe for the mother and fetus with minimal side-effects when compared to placebo. The adverse effects are similar with all vaginal forms of progesterone.Citation54 Comparing vaginal gel to oil-in-capsules, patients find the gel more convenient and easy to use as there is less vaginal discharge and fewer application difficulties.Citation61,Citation62 Despite equivalent efficacy of different forms of natural progesterone, the gel provides superior acceptability and tolerability due to less leakage and once daily application with a tampon-like familiar insertion.Citation61 In the reported trials, over 98% patients accepted a complete course of vaginal gel therapy with high compliance rates of 93%–96%.Citation29,Citation49 Women express greater satisfaction with the convenience of administration of vaginal gel progesterone compared to the discomfort with IM progesterone.Citation63
Conclusion: place in therapy
In summary, there is ample Level 1 evidence supporting use of vaginal progesterone in women with midtrimester short cervix to decrease sPTB. Adding to this benefit is the fact that it has no significant adverse effects for mother or the neonate. Critics argue that with low frequency of sCL (), low sensitivity of sCL to predict preterm delivery, and only ~40% reduction of sPTB will result in many women undergoing the treatment unnecessarily. However, proponents would argue that the data suggests that only 11 need to be treated to prevent one sPTB.Citation41 This one prevented sPTB will result in insurmountable benefits not only to that neonate, but also to that family, and the society not only monetarily but also emotionally and intellectually and lighten the burden of chronic diseases. Even if critics argue regarding the degree of benefit, the risk–benefit ratio balance tips towards vaginal progesterone use in women with sCL especially as there are no significant side effects. Therefore I recommend universal CL screening of all women with singleton gestation at midtrimester, and offering prophylactic treatment with vaginal progesterone in those with sCL. I believe this will become the standard of care.
Disclosure
The author was an investigator in the ‘PREGNANT’ trial, and was also a paid consultant as part of the Watson Pharmaceutical Team presenting to FDA in 2011 for vaginal progesterone gel.
References
- HamiltonBEMartinJAVenturaSJBirths: preliminary data for 2010Natl Vital Stat Rep20116012622670489
- MathewsTJMacDormanMFInfant mortality statistics from the 2008 period linked birth/infant death data setNatl Vital Stat Rep20126014922670489
- SaigalSDoyleLWAn overview of mortality and sequelae of preterm birth from infancy to adulthoodLancet200837126126918207020
- McCormickMCLittJSSmithVCZupancicJAFPrematurity: an overview and public health implicationsAnn Rev Public Health20113236737921219170
- RussellRBGreenNSSteinerCACost of hospitalization for preterm and low birth weight infants in the United StatesPediatrics2007120e1e917606536
- National Research CouncilPreterm birth: causes, consequences, and preventionBehrmanREButlerASCommittee on Understanding Premature Birth Assuring Healthy OutcomesWashington, DCThe National Academies Press2007
- March of Dimes FoundationMedical costs for one premature baby could cover a dozen healthy births3172009 Available from: http://www.eurekalert.org/pub_releases/2009-03/modf-mcf031309.phpAccessed on August 1, 2012
- HeathVCSouthallTRSoukaAPElisseouANicolaidesKHCervical length at 23 weeks of gestation: prediction of spontaneous preterm deliveryUltrasound Obstet Gynecol1998123123179819868
- AndersenHFNugentCEWantySDHayashiRHPrediction of risk for preterm delivery by ultrasonographic measurement of cervical lengthAm J Obstet Gynecol19901638598672206073
- IamsJDGoldenbergRLMeisPJThe length of the cervix and the risk of spontaneous premature delivery. National Institute of Child Health and Human Development Maternal Fetal Medicine Unit NetworkN Engl J Med19963345675728569824
- TaipalePHiilesmaaVSonographic measurement of uterine cervix at 18–22 weeks’ gestation and the risk of preterm deliveryObstet Gynecol1998929029079840546
- RossMGCousinsLBaxter-JonesRBemis-HeysRCatanzariteVDowlingDObjective cervical portio length measurements: consistency and efficacy of screening for a short cervixJ Reprod Med20075238538917583236
- AndersenHFTransvaginal and transabdominal ultrasonography of the uterine cervix during pregnancyJ Clin Ultrasound19911977831847952
- OkitsuOMimuraTNakayamaTAonoTEarly prediction of preterm delivery by transvaginal ultrasonographyUltrasound Obstet Gynecol1992240240912796914
- HeathVCSouthallTRSoukaAPNovakovANicolaidesKHCervical length at 23 weeks of gestation: relation to demographic characteristics and previous obstetric historyUltrasound Obstet Gynecol1998123043119819867
- ClementSCandyBHeathVToMNicolaidesKHTransvaginal ultrasound in pregnancy: its acceptability to women and maternal psychological morbidityUltrasound Obstet Gynecol20032250851414618665
- OlatunbosunOAal-NuaimLTurnellRWEmergency cerclage compared with bed rest for advanced cervical dilatation in pregnancyInt Surg1995801701748530237
- ArisoyRYaylaMTransvaginal sonographic evaluation of the cervix in asymptomatic singleton pregnancy and management options in short cervixJ Pregnancy201220162822
- LockwoodCThe real progesterone story: Exploring the Makena drug controversyContemp Ob/Gyn2011561014
- CampbellSUniversal cervical-length screening and vaginal progesterone prevents early preterm births, reduces neonatal morbidity and is cost saving: doing nothing is no longer an optionUltrasound Obstet Gynecol2011381921713990
- CombsCAVaginal progesterone for asymptomatic cervical shortening and the case for universal screening of cervical lengthAm J Obstet Gynecol201220610110322284154
- Society for Maternal-Fetal Medicine Publications CommitteeProgesterone and preterm birth prevention: translating clinical trials data into clinical practiceAm J Obstet Gynecol201220637638622542113
- CahillAGOdiboAOCaugheyABUniversal cervical length screening and treatment with vaginal progesterone to prevent preterm birth: a decision and economic analysisAm J Obstet Gynecol2010202548. e1e820079888
- WernerEFHanCSPettkerCMUniversal cervical-length screening to prevent preterm birth: a cost-effectiveness analysisUltrasound Obstet Gynecol201138323721157771
- IamsJDJohnsonFFSonekJSachsLGebauerCSamuelsPCervical competence as a continuum: a study of ultrasonographic cervical length and obstetric performanceAm J Obstet Gynecol199517210971103 discussion, 104–1067726247
- BerghellaVRomanADaskalakisCNessABaxterJKGestational age at cervical length measurement and incidence of preterm birthObstet Gynecol200711031131717666605
- DeFrancoEAO’BrienJMAdairCDVaginal progesterone is associated with a decrease in risk for early preterm birth and improved neonatal outcome in women with a short cervix: a secondary analysis from a randomized, double-blind, placebo-controlled trialUltrasound Obstet Gynecol20073069770517899571
- da FonsecaEBCelikEParraMSinghMNicolaidesKHProgesterone and the risk of preterm birth among women with a short cervixN Engl J Med200735746246917671254
- HassanSSRomeroRVidyadhariDVaginal progesterone reduces the rate of preterm birth in women with a sonographic short cervix: a multicenter, randomized, double-blind, placebo-controlled trialUltrasound Obstet Gynecol201138183121472815
- RomeroRNicolaidesKConde-AgudeloAVaginal progesterone in women with an asymptomatic sonographic short cervix in the midtrimester decreases preterm delivery and neonatal morbidity: a systematic review and metaanalysis of individual patient dataAm J Obstet Gynecol2012206124. e1e1922284156
- OwenJHankinsGIamsJDMulticenter randomized trial of cerclage for preterm birth prevention in high-risk women with shortened midtrimester cervical lengthAm J Obstet Gynecol2009201375. e1e819788970
- SchumacherMSitruk-WareRDe NicolaAFProgesterone and progestins: neuroprotection and myelin repairCurr Opin Pharmacol2008874074618929681
- GoletianiNVKeithDRGorskySJProgesterone: Review of safety for clinical studiesExper Clin Psychopharmacol20071542744417924777
- XuHGonzalezJMOforiEElovitzMAPreventing cervical ripening: the primary mechanism by which progestational agents prevent preterm birth?Am J Obstet Gynecol2008198314. e1314e818313454
- de LignieresBOral micronized progesteroneClin Ther1999214160 discussion 1–210090424
- CicinelliEde ZieglerDBullettiCMatteoMGSchonauerLMGalantinoPDirect transport of progesterone from vagina to uterusObstet Gynecol20009540340610711552
- FanchinRMDe ZieglerDMBergeronCPRighiniCMTorrisiCMFrydmanRMTransvaginal administration of progesteroneObstet Gynecol1997903964019277651
- SfakianakiAKNorwitzERMechanisms of progesterone action in inhibiting prematurityJ Matern Fetal Neonatal Med20061976377217190686
- DayaSLuteal support: progestogens for pregnancy protectionMaturitas200965Suppl 1S29S3419913373
- WahabiHAAbed AlthagafiNFElawadMAl ZeidanRAProgestogen for treating threatened miscarriageCochrane Database Syst Rev201112CD00594322161393
- da FonsecaEBBittarRECarvalhoMHProphylactic administration of progesterone by vaginal suppository to reduce the incidence of spontaneous preterm birth in women at increased risk: a randomized placebo-controlled double-blind study. [see comment.]Am J Obstet Gynecol200318841942412592250
- SuL-LSamuelMChongYSProgestational agents for treating threatened or established preterm labourCochrane Database Syst Rev20101CD00677020091604
- RomeroRPrevention of spontaneous preterm birth: the role of sonographic cervical length in identifying patients who may benefit from progesterone treatmentUltrasound Obstet Gynecol20073067568617899585
- WordRALiX-HHnatMCarrickKDynamics of cervical remodeling during pregnancy and parturition: mechanisms and current conceptsSemin Reprod Med200725697917205425
- YellonSMBurnsAESeeJLLechugaTJKirbyMAProgesterone withdrawal promotes remodeling processes in the nonpregnant mouse cervixBiol Reprod2009811619228593
- ChwaliszKThe use of progesterone antagonists for cervical ripening and as an adjunct to labour and deliveryHum Reprod19949Suppl 11311617962460
- JeschkeUMylonasIRichterD-URegulation of progesterone production in human term trophoblasts in vitro by CRH, ACTH and cortisol (prednisolone)Arch Gynecol Obstet200527271215834733
- MeisPJKlebanoffMThomEPrevention of recurrent preterm delivery by 17 alpha-hydroxyprogesterone caproateN Engl J Med20033482379238512802023
- O’BrienJMAdairCDLewisDFProgesterone vaginal gel for the reduction of recurrent preterm birth: primary results from a randomized, double-blind, placebo-controlled trialUltrasound Obstet Gynecol20073068769617899572
- CetingozECamCSakalliMKaratekeACelikCSancakAProgesterone effects on preterm birth in high-risk pregnancies: a randomized placebo-controlled trialArch Gynecol Obstet201128342342920091317
- RodeLKleinKNicolaidesKHKrampl-BettelheimETaborAfor the PREDICT GroupPrevention of preterm delivery in twin gestations (PREDICT): a multicenter, randomized, placebo-controlled trial on the effect of vaginal micronized progesteroneUltrasound Obstet Gynecol20113827228021739497
- ToMSSkentouCARoystonPYuCKHNicolaidesKHPrediction of patient-specific risk of early preterm delivery using maternal history and sonographic measurement of cervical length: a population-based prospective studyUltrasound Obstet Gynecol20062736236716565989
- ZarutskiePWPhillipsJAA meta-analysis of the route of administration of luteal phase support in assisted reproductive technology: vaginal versus intramuscular progesteroneFertil Steril20099216316919362303
- PolyzosNPMessiniCIPapanikolaouEGVaginal progesterone gel for luteal phase support in IVF/ICSI cycles: a meta-analysisFertil Steril2010942083208720171629
- MilesRAPaulsonRJLoboRAPressMFDahmoushLSauerMVPharmacokinetics and endometrial tissue levels of progesterone after administration by intramuscular and vaginal routes: a comparative studyFertil Steril1994624854908062942
- GermondMCapelliPBrunoGComparison of the efficacy and safety of two formulations of micronized progesterone (Ellios and Utrogestan) used as luteal phase support after in vitro fertilizationFertil Steril20027731331711821089
- KleinsteinJLuteal Phase Study GEfficacy and tolerability of vaginal progesterone capsules (Utrogest 200) compared with progesterone gel (Crinone 8%) for luteal phase support during assisted reproductionFertil Steril2005831641164915950631
- HaasDMRamseyPSProgestogen for preventing miscarriageCochrane Database Sys Rev2008CD003511
- KatzZLancetMSkornikJChemkeJMogilnerBMKlinbergMTeratogenicity of progestogens given during the first trimester of pregnancyObstet Gynecol1985657757803158848
- O’BrienJMSteichenJJPhillipsJACreasyGW490: Two year infant outcomes for children exposed to supplemental intravaginal progesterone gel in utero: secondary analysis of a multicenter, randomized, double-blind, placebo-controlled trialAm J Obstet Gynecol2012206S223
- SimunicVTomicVTomicJNizicDComparative study of the efficacy and tolerability of two vaginal progesterone formulations, Crinone 8% gel and Utrogestan capsules, used for luteal supportFertil Steril200787838717081536
- LudwigMSchwartzPBabahanBLuteal phase support using either Crinone 8% or Utrogest: results of a prospective, randomized studyEur J Obstet Gynecol Reprod Biol2002103485212039463
- YanushpolskyEHurwitzSGreenbergLRacowskyCHornsteinMCrinone vaginal gel is equally effective and better tolerated than intramuscular progesterone for luteal phase support in in vitro fertilizationembryo transfer cycles: a prospective randomized studyFertil Steril2010942596259920347079
- ShamanskySLClausenCLLevels of prevention: examination of the conceptNurs Outlook1980281041086898305
- RamaekerDMSimhanHNSonographic cervical length, vaginal bleeding, and the risk of preterm birthAm J Obstet Gynecol2012206224. e1e422133802
- MercerBMGoldenbergRLDasAThe preterm prediction study: a clinical risk assessment systemAm J Obstet Gynecol199617418851893 discussion, 93–958678155
- HonestHBachmannLMSundaramRGuptaJKKleijnenJKhanKSThe accuracy of risk scores in predicting preterm birth – a systematic reviewJ Obstet Gynaecol20042434335915203570
- LeitichHEgarterCKaiderAHohlagschwandtnerMBerghammerPHussleinPCervicovaginal fetal f ibronectin as a marker for preterm delivery: a meta-analysisAm J Obstet Gynecol19991801169117610329873
- YangJHartmannKESavitzDAVaginal bleeding during pregnancy and preterm birthAm J Epidemiol200416011812515234932
- GoldenbergRLCulhaneJFIamsJDRomeroREpidemiology and causes of preterm birthLancet2008371758418177778
- MandalDMandaSRakshiADeyRPBiswasSCBanerjeeAMaternal obesity and pregnancy outcome: a prospective analysisJ Assoc Physicians India20115948648921887903
- SmithGCSPellJPDobbieRInterpregnancy interval and risk of preterm birth and neonatal death: retrospective cohort study. [Erratum appears in BMJ. 2003;327(7419):851.]BMJ200332731312907483
- OforiBDLe TiecMBerardARisk factors associated with preterm birth according to gestational age at birthPharmacoepidemiol Drug Saf20081755656418327870
- HuaMOdiboAOLongmanREMaconesGARoehlKACahillAGCongenital uterine anomalies and adverse pregnancy outcomesAm J Obstet Gynecol201120522
- VergnesJ-NSixouMPreterm low birth weight and maternal periodontal status: a meta-analysisAm J Obstet Gynecol2007196135.e1135e717306654
- HassanSSRomeroRBerrySMPatients with an ultrasonographic cervical length <or=15 mm have nearly a 50% risk of early spontaneous preterm deliveryAm J Obstet Gynecol20001821458146710871466
- MorozLASimhanHNRate of sonographic cervical shortening and the risk of spontaneous preterm birthAm J Obstet Gynecol2012206234. e1e522189048
- GrobmanWAfor the Eunice Kennedy Shriver National Institute of Health and Human DevelopmentRandomized controlled trial of progesterone treatment for preterm birth prevention in nulliparous women with cervical length less than 30 mmAm J Obstet Gynecol2012206S367
- MercerBMGoldenbergRLMoawadAHThe preterm prediction study: effect of gestational age and cause of preterm birth on subsequent obstetric outcome. NICHHD MFMU NetworkAm J Obstet Gynecol19991811216122110561648