Abstract
Malignant ascites affects approximately 10% of patients with recurrent epithelial ovarian cancer and is associated with troublesome symptoms, including abdominal pressure and distension, dyspnea, bloating, pelvic pain, and bowel/bladder dysfunction. To date, no effective therapy has been identified for the treatment of malignant ascites in patients with recurrent, advanced ovarian cancer. In this article, we discuss currently existing options for the treatment of ascites associated with ovarian cancer, and review the literature as it pertains to novel, targeted therapies. Specifically, preclinical and clinical trials exploring the use of the antiangiogenic agents, bevacizumab and vascular endothelial growth factor-trap, as well as the nonangiogenic agent, catumaxomab, will be reviewed. Despite current limitations in treatment, knowledge regarding management options in the palliation of ascites is critical to practicing physicians. Ultimately, as with all novel therapies, symptom relief and treatment goals must be weighed against patient discomfort and potentially significant adverse events.
Introduction
Epithelial ovarian cancer accounts for 25% of all malignancies affecting the female genital tract, and is the most lethal gynecologic malignancy. In 2012, there will be an estimated 22,280 new ovarian cancer cases in the US, with 15,500 deaths.Citation1 Advanced epithelial ovarian cancer is traditionally managed with cytoreductive surgery, followed by combination platinum and taxane chemotherapy.Citation2 Patients with advanced disease who undergo successful cytoreductive surgery with no gross residual disease have a median survival of just over 5 years after completion of adjuvant chemotherapy.Citation3 However, despite aggressive treatment, the majority of these patients develop recurrent cancer, with selection of chemotherapy-resistant clones.Citation4 The subset of patients that develops recurrent disease comprises a population that traditionally faces extended exposure to multiple cytotoxic chemotherapy regimens, dictated by their disease-free interval.Citation5–Citation8 Throughout this period, management of disease-associated morbidities becomes a priority in an effort to improve quality of life.
Malignant ascites, which affects approximately two-thirds of patients with epithelial ovarian, primary peritoneal, and fallopian tube cancer is common, and to date few effective therapies have been identified.Citation9 Importantly, ascites is associated with troublesome symptoms, including abdominal pressure and distension, dyspnea, bloating, pelvic pain, and bowel/bladder dysfunction.Citation10 Malignant ascites is defined by the National Cancer Institute as an accumulation of fluid containing cancer cells in the abdomen.Citation11 Unlike other solid malignancies, where ascites portends a universally poor prognosis, patients with epithelial ovarian cancer and ascites at the time of diagnosis can expect 5-year survival rates approaching 40%.Citation11,Citation12 This discrepancy is largely attributable to the biology of ovarian cancer, and subsequent etiology of abdominal fluid accumulation. Specifically, malignant ascites in patients with epithelial ovarian cancer is thought to be attributable to lymphatic obstruction, increased vascular permeability release of inflammatory cytokines, and a direct increase of fluid production by the cancer cells lining the peritoneal cavity.Citation13,Citation14
Upfront treatment of patients with advanced epithelial ovarian cancer, irrespective of the presence or absence of ascites, relies on a combination of aggressive cytoreductive surgery and adjuvant chemotherapy. The goal of surgical cytoreduction is to reduce disease burden to ≤1 cm (defined as optimal cytoreduction by the Gynecologic Oncology Group). As a result of optimal cytoreduction, these patients experience effective control of their ascites. Unfortunately, despite improvement in surgical management, only a small fraction of patients are cured following primary surgery and chemotherapy, with greater than 75% experiencing disease recurrence. Repeat attempts at surgical excision are only performed in selected patients with prolonged disease-free intervals, localized disease recurrence, and good performance status. The remaining patients are managed with systemic therapies. Accumulation of ascites affects patients with progressive disease or treatment failure, and must be managed in order to maintain overall quality of life.Citation15
Historically, malignant ascites in patients with epithelial ovarian cancer was treated utilizing diuretics, salt restriction, and intraperitoneal administration of sclerosing agents and radioactive isotopes.Citation16,Citation17 Patients with malignant ascites secondary to epithelial ovarian cancer rarely suffer from fluid accumulation due to intraparenchymal liver metastasis, and portal hypertension is rarely identified. Rather, these patients traditionally exhibit reduced intravascular volume, making use of diuretics an unattractive option.Citation18 With respect to the use of radioactive isotopes, poor tumor penetration and intestinal toxicity (necrosis and perforation) due to loculations and prolonged exposure have caused them to fall out of favor. Limited success rates, in combination with significant side effects, have resulted in infrequent use of these modalities.
Mechanical drainage of accumulated ascetic fluid via therapeutic paracentesis results in relief in up to 90% of patients.Citation19 However, recurrence/reaccumulation of ascites is common, and multiple paracenteses are required, with their associated risks of pain, visceral perforation, infection, and formation of hematoma.Citation11,Citation20 Furthermore, these patients are likely to have intra-abdominal adhesions as a result of extensive surgical cytoreduction, and the resultant fluid loculations limit the therapeutic benefit derived.Citation21 Alternatively, placement of permanent intra-abdominal drains and peritoneovenous shunts has been explored. Experience with these modalities has been poor, with blockage of the shunt, infectious morbidity, as well as embolization and implantation of tumor cells in distant organs reported to be relatively common complications.Citation17,Citation22–Citation25
Given the above, exploration of innovative approaches for the treatment of malignant ascites in patients with advanced epithelial ovarian cancer has been a clinical priority. With advances in our understanding of cancer biology, novel therapeutic targets have been identified. Specifically, the relationship between angiogenesis and epithelial ovarian cancer has been elucidated over the last decade, and strategies developed to interfere with this process have shown promise in the control of ascites associated with epithelial ovarian cancer. This mini review article discusses the role of emerging therapies targeting angiogenesis in the management of ascites, and summarizes the currently available data in the literature.
Angiogenesis and ascites
Under normal homeostatic conditions, excluding wound healing and embryonic development, a balance exists between proangiogenic and antiangiogenic signals, resulting in a quiescent vascular environment. However, within the tumor microenvironment, aberrant signaling has been shown to favor the proangiogenic cascade, resulting in formation of new vessels.Citation26,Citation27 The formation of new blood vessels, a process termed angiogenesis, is essential for tumor growth beyond 1–2 mm3. This process is mediated via the vascular endothelial growth factor (VEGF) family of growth factors and receptors, and is believed to be essential for tumor growth and ascites formation. Furthermore, these tumor vessels, formed under the influence of VEGF, are disorganized, tortuous, and leaky.Citation28 Inhibition of VEGF-mediated signaling leads to “normalization” of this tumor vasculature, as well as improved oxygen, nutrient and chemotherapy delivery, and is believed to result in increased tumor toxicity and decreased formation of ascites fluid.Citation8
VEGF expression has been repeatedly demonstrated in epithelial ovarian cancer tissue specimens, and the degree of expression of VEGF and its receptors has been shown to correlate with a poor prognosis.Citation29,Citation30 VEGF-A (commonly known and referred to as VEGF) was first identified and cloned in 1989.Citation31 In a series of molecular biology and animal model studies, VEGF was noted to be a potent mitogen for endothelial cells in vitro and acted as an angiogenic molecule in vivo. In addition to VEGF, the VEGF family is composed of VEGF-B, VEGF-C, VEGF-D, VEGF-E, and the placental growth factors, PlGF-1 and PlGF-2.Citation32–Citation34 The most important member of this group is VEGF itself, which appears to play a principal role in angiogenesis.
VEGF binds to and interacts with a series of receptor tyrosine kinases known as VEGFR-1, VEGFR-2, and VEGFR- 3, as well as accessory receptors known as neuropilins.Citation35 It appears that signal transduction through VEGFR-2 mediates the permeability actions of VEGF, as evidenced by the fact that VEGFR-2 gene knockout mice fail to develop vasculature and have sparse endothelial cells.Citation36 It is hypothesized that as cancerous cells multiply and the tumor mass grows, there is secretion of VEGF, promoting neovascularization, allowing for nutrient delivery, and facilitating metastasis. In cases of disseminated intra-abdominal metastatic disease, both increased production of peritoneal fluid by the cancer cells, and increased microvascular permeability result in significant ascites. In addition, investigators have shown increased VEGF protein levels in malignant ascites compared with levels in nonmalignant cirrhotic controls.Citation37
VEGF inhibition for treatment of malignant ascites
VEGF-specific monoclonal antibody
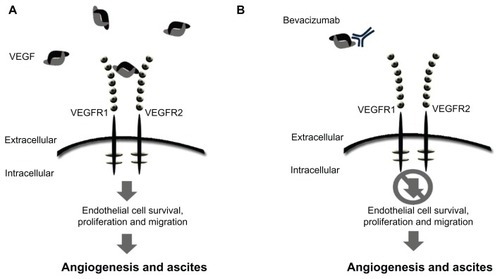
Given the apparent dependence of ascites formation on abnormal tumor vascularity and permeability, it was hypothesized that VEGF inhibitors would show efficacy in the treatment of ascites associated with ovarian cancer (). In preclinical nude mouse models of advanced ovarian cancer, inhibition of VEGF signaling was associated with a marked decrease in ascites formation and tumor burden.Citation38–Citation40 Furthermore, it has been shown that malignant effusions derived from tumorbearing mice and guinea pigs contain high concentrations of VEGF.Citation41 VEGF production by cancer cells has been shown to correlate directly with tumor-cell induced production of ascites in animal models.Citation41 Strikingly, direct transfection of mouse peritoneum with VEGF alone is sufficient to cause accumulation of peritoneal effusions.
Figure 1 Schematic of mode of action for VEGF signaling and bevacizumab. (A) Free unbound VEGF interacting with the receptor. (B) The monoclonal antibody, bevacizumab, binds to VEGF-A, preventing ligand-receptor interaction and downstream signaling.
This strong preclinical evidence catalyzed the investigation of bevacizumab for the palliation of symptomatic ascites in patients with heavily pretreated recurrent ovarian carcinoma ().Citation42 Numnum et al described four patients with recurrent ovarian cancer and ascites requiring frequent paracentesis who were treated with intravenous bevacizumab at a dose of 15 mg/kg every 3 weeks. All four patients demonstrated symptomatic relief of ascites, with manageable toxicity. No therapeutic paracenteses were required after initiation of treatment with bevacizumab (follow-up of up to 6 months).Citation42
Table 1 Studies reporting use of bevacizumab for treatment of ascites associated with ovarian cancer
In an analogous manner, Hamilton et al described a case report detailing the impact of intraperitoneal bevacizumab (5 mg/kg) on severe symptomatic ascites in an elderly patient with advanced, recurrent ovarian cancer and very poor functional status.Citation43 The authors reported a dramatic improvement in ascites and quality of life parameters following two doses. Two additional case reports described the off-label use of bevacizumab in 10 patients with refractory ascites and significant disease burden.Citation44 Relief of ascites was seen in all subjects, lasting 2–6 months.Citation41 The largest of these reports, described by El Shami et alCitation61 investigated the efficacy and safety of bevacizumab (5 mg/kg administered intraperitoneally every 4 weeks) in nine patients with refractory ascites secondary to colorectal, breast, uterine, and ovarian cancer.Citation41 Remarkably, the malignant ascites resolved in all treated patients after a single dose, without reaccumulation over a median observation period of more than 2 months.
VEGF-trap
VEGF-trap, a fusion protein that prevents VEGF receptor binding, has also been studied in the treatment of refractory ascites. In contrast with the antibody-based VEGF binding strategy used by bevacizumab, VEGF-trap, or aflibercept, incorporates the second binding domain of the VEGFR-1 receptor and the third domain of the VEGFR-2 receptor ().Citation45 By fusing these extracellular protein sequences to the Fc segment of a human IgG backbone, developers created a chimeric protein with a very high VEGF binding affinity, binding all isomers of the VEGF-A family.Citation45,Citation46 Of note, it has also been shown to bind VEGF-B and placental growth factor, with uncertain clinical implications.
Figure 2 Schematic of VEGF-trap mode of action. VEGF-trap is a fusion protein that prevents VEGF-receptor binding. (A) VEGF-trap, or aflibercept, incorporates the second binding domain of the VEGFR-1 receptor and the third domain of the VEGFR-2 receptor. (B) This chimeric protein has a high VEGF binding affinity, preventing VEGF-receptor interaction and downstream signaling.
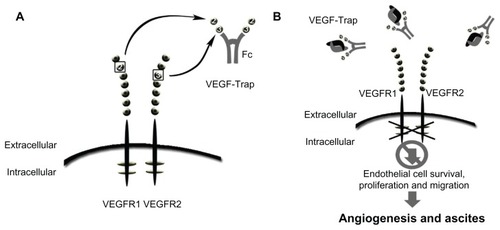
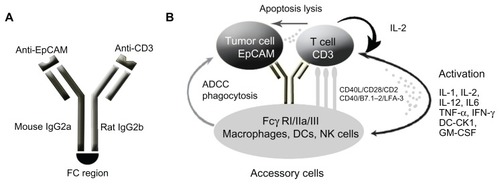
Figure 3 Schematic of mode of action of catumaxomab. (A) Catumaxomab is a trifunctional monoclonal antibody with two different antigen-binding sites and a functional Fc domain. (B) The two specific antigen-binding sites bind to epithelial tumor cells via the epithelial cell-adhesion molecule (EpCAM) and to T cells via CD3, while activating Fcγ receptor I-positive, IIa-positive, and III-positive accessory cells (dendritic cells, macrophages and natural killer cells) via its functional Fc domain.
Preclinical xenograft animal models have shown that VEGF-trap is effective in inhibiting tumor growth and angiogenesis, reducing blood vessel density, inhibiting metastasis, and improving survival.Citation38,Citation47,Citation48 Hu et al investigated the impact of VEGF-trap on ascites formation in a mouse model of ovarian cancer.Citation49 Following intraperitoneal administration of VEGF-trap and paclitaxel, complete resolution of ascites was noted, with a 98% reduction in tumor burden. Furthermore, no measurable ascites developed in the population treated with VEGF-trap. Tumor vessel imaging showed sparse, short vessels in treated mice as compared with controls, in which vessels were numerous, irregular, tortuous, and leaky.Citation49 In 2003, Byrne et al reported that single-agent aflibercept significantly reduced both ascites and tumor burden in experimental models of ovarian cancer.Citation38
The safety and tolerability of VEGF-trap were evaluated in a Phase I clinical trial conducted by Lockhart et al.Citation50 A total of 47 patients (14 of whom had ovarian, peritoneal, or fallopian tube cancer) were enrolled from two institutions. The dose ranged from 0.3 mg/kg to 7.0 mg/kg given intravenously every 2 weeks. The most common adverse events were fatigue, nausea, and vomiting. Within this cohort, three partial responses were observed according to RECIST (Response Evaluation Criteria in Solid Tumors) criteria, one at the 3.0 mg/kg and two at the 7.0 mg/kg dose level. The authors concluded that VEGF-trap, when administered intravenously, was well tolerated at the dose levels tested.Citation50
Several single-agent and combination Phase II clinical trials have explored the safety and efficacy of VEFG-trap in the treatment of ascites associated with advanced solid tumors, including ovarian cancer.Citation51,Citation52 Two recently published trials investigated the use of VEGF-trap in the treatment of advanced epithelial ovarian cancer and symptomatic malignant ascites.
Colombo et al enrolled 16 patients with advanced chemoresistant epithelial ovarian cancer and symptomatic malignant ascites into an open-label Phase II trial assessing the efficacy and safety of aflibercept.Citation53 Patients who required ≥ 3 previous paracenteses at 1–4 paracenteses per month received intravenous aflibercept at a dose of 4 mg/kg every 2 weeks. The primary endpoint was repeat paracentesis response rate, with response defined as at least a two-fold increase in time to repeat paracentesis compared with the baseline interval. Ten of the 16 enrolled patients achieved a response; the repeat paracentesis response rate was 62.5% (95% confidence interval 35.4–84.8, ) in these patients. Aflibercept was considered effective based on a hypothesis that the repeat paracentesis response rate was ≥60%. Median time to repeat paracentesis was 76.0 days (95% confidence interval 64.0–178.0), which was 4.5 times longer than the baseline interval (16.8 days, ). Adverse events reported as part of the study included hypertension (seven patients), headache, anorexia, and dysphonia (three patients each).Citation53 Only two subjects experienced grade 3/4 treatment-related adverse events, ie hypertension and weight loss, and one patient developed intestinal perforation.
Figure 4 Kaplan–Meier plot of time to repeat paracentesis in patients treated with VEGF-trap (aflibercept) for the management of malignant ascites. Median time to repeat paracentesis was 76.0 days (95% confidence interval 64.0–178.0), which was 4.5 times longer than the baseline interval (16.8 days) in the aflibercept group.
Copyright © 2012. Elsevier. Adapted with permission from Colombo N, Mangili G, Mammoliti S, et al. A Phase II study of aflibercept in patients with advanced epithelial ovarian cancer and symptomatic malignant ascites. Gynecol Oncol. 2012;125(1):42–47.Citation53
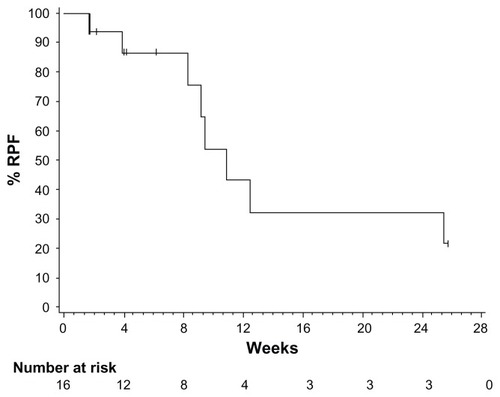
Table 2 Summary of efficacy endpoints
A similar study conducted by Gotlieb et al specifically explored treatment of malignant ascites in patients with advanced epithelial ovarian cancer using aflibercept.Citation54 In this double-blind, placebo-controlled, parallel-group, Phase II study, patients with advanced chemoresistant ovarian cancer and recurrent symptomatic malignant ascites were randomly assigned to receive either intravenous aflibercept (4 mg/kg every 2 weeks) or placebo, stratified according to time interval (≤2 weeks versus >2 weeks) between the two most recent paracenteses before randomization.Citation54 The primary efficacy endpoint was time to repeat paracentesis. A total of 55 patients with a median of four (range 2–11) previous lines of chemotherapy were randomly assigned to receive placebo (n = 26) or aflibercept (n = 29). Mean time to repeat paracentesis was significantly longer with aflibercept than with placebo (55.1 versus 23.3 days; difference 31.8 days, 95% confidence interval 10.6–53.1; P = 0.0019). Notably, in the aflibercept group, two patients did not need a repeat paracentesis during six months of double-blind treatment. In this subset of heavily pretreated patients with advanced ovarian cancer, three gastrointestinal perforations were noted in the aflibercept group, and one intestinal fistula was identified in the placebo group.
Nonangiogenic targeted therapies used for malignant ascites
Trifunctional antibody catumaxomab
In addition to the VEGF-directed antibodies, bevacizumab and VEGF-trap, alternate targeted agents have been investigated in the treatment of ascites. Catumaxomab is a trifunctional monoclonal antibody with two different antigen-binding sites and a functional Fc domain.Citation55,Citation56 The two specific antigen-binding sites bind to epithelial tumor cells via the epithelial cell-adhesion molecule (EpCAM) and to T cells via CD3. In addition, catumaxomab activates Fcγ receptor I-positive, IIa-positive, and III-positive accessory cells (dendritic cells, macrophages, and natural cells) via its functional Fc domain ().Citation55,Citation56
The functionality and selectivity of this novel antibody rely on the fact that tumor cells in effusions associated with malignant ovarian cancer have been shown to express EpCAM in 70%–100% of cases, while the mesothelial cells lining the peritoneal cavity lack expression.Citation57 Following binding with EpCAM, catumaxomab recruits and activates of immune effector cells, resulting in its antineoplastic activity.
Intraperitoneal administration of catumaxomab was first studied in the treatment of eight patients (two of whom had ovarian cancer) with malignant ascites in 2005.Citation58 All patients had >2% EpCAM expression via flow cytometry on nuclear ascites cells. Trifunctional antibodies were administered intraperitoneally over 6–8 hours for at least four cycles. Seven of eight patients required no further paracentesis during follow-up or until death, with a mean paracentesis-free interval of 38 weeks (median 21.5, range 4–136). A clinical response with disappearance of ascites was seen in all patients, and correlated with elimination of tumor cells (P = 0.0014).Citation58
Following this study, a multicenter Phase I/II clinical trial was conducted evaluating the tolerability and efficacy of intraperitoneal catumaxomab in ovarian cancer patients with malignant ascites containing EpCAM-positive tumor cells.Citation59 Twenty-three women with recurrent ascites due to pretreated refractory ovarian cancer were treated with 4–5 intraperitoneal infusions of catumaxomab at doses of 5–200 μg over 9–13 days. Treatment with catumaxomab resulted in significant and sustained reduction of ascites. Twenty-two of 23 patients did not require paracentesis between the last infusion and the end of the study at day 37.Citation59 The most commonly reported grade 2/3 adverse events in the study were fever, nausea, and vomiting.
Recently, a prospective, randomized Phase II/III study was conducted comparing the efficacy of catumaxomab plus paracentesis with paracentesis alone in the treatment of malignant ascites.Citation57 Following paracentesis, catumaxomab was administered at doses of 10, 20, 50, and 150 μg on days 0, 3, 7, and 10, respectively, via an intraperitoneal catheter. The primary efficacy endpoint was puncture-free survival. Secondary efficacy parameters included time to next paracentesis, signs and symptoms of ascites, and overall survival. Puncture-free survival was significantly longer in the catumaxomab group (median 46 days) than in the control group (median 11 days, hazards ratio 0.254; P < 0.0001), as was the median time to next paracentesis (77 versus 13 days; P < 0.0001, ). Within the ovarian cancer cohort, median puncture-free survival was 52 days in the catumaxomab arm versus 11 days in the placebo arm (hazards ratio 0.205; P < 0.0001). In addition, catumaxomab patients had fewer signs and symptoms of ascites than control patients. The most common adverse events included fever, abdominal pain, nausea, and vomiting (). One patient had a grade 3 gastric hemorrhage. Findings from the above trials ultimately resulted in approval by the European Medicines Agency for catumaxomab for the treatment of malignant ascites in patients with EPCAM-positive tumors for whom no standard therapy is available.Citation13
Figure 5 Kaplan–Meier estimates of puncture-free survival and time to next paracentesis in both the catumaxomab and control populations. (A) Puncture-free survival in the pooled population. (B) Time to next paracentesis in the pooled population.
Copyright © 2010. John Wiley and Sons. Adapted with permission from Heiss MM, Murawa P, Koralewski P, et al. The trifunctional antibody catumaxomab for the treatment of malignant ascites due to epithelial cancer: Results of a prospective randomized Phase II/III trial. Int J Cancer. 2010;127(9):2209–2221.Citation57
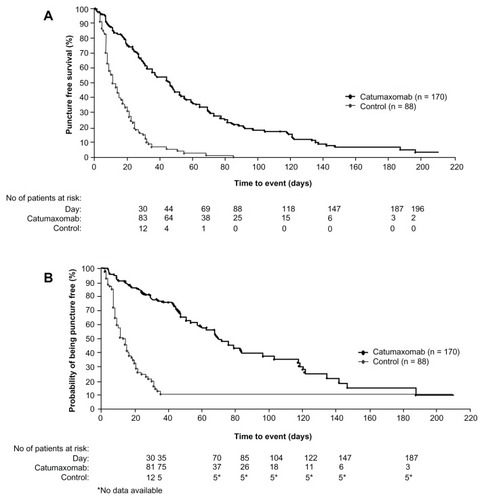
Table 3 Summary of adverse events related to catumaxomab occurring in ≥5% of subjects
Given the mouse-rat origin of catumaxomab, limitations in retreatment were anticipated due to formation of human antidrug antibodies. However, in 2011, Pietzner et al described a case of successful retreatment with catumaxomab for the management of malignant ascites.Citation60 A 74-year-old female patient with breast cancer and ascites associated with peritoneal carcinomatosis was treated with catumaxomab, with resolution of her symptoms. The patient remained puncture-free for 45 days, and evaluation of human antidrug antibody levels demonstrated increased levels after cycle 1, followed by a considerable decline and a delayed increase in ascites for each subsequent cycle. This experience suggested that a repeat cycle of catumaxomab might be feasible and effective in patients suffering from recurrent malignant effusions.
Conclusion
Malignant abdominal effusions affect a significant proportion of patients suffering from advanced ovarian cancer, and are associated with troubling symptoms including abdominal pain, dyspnea, bloating, weight loss, and bowel and bladder dysfunction. The biology of the disease and its propensity for peritoneal spread are unique, predisposing patients to formation of ascites. To date, no consensus has been reached regarding the treatment of ascites in patients with ovarian cancer. Traditional treatment methods, including salt restriction, diuretics, sclerosing agents, radioactive isotopes, paracentesis, and shunt placement, have shown limited and variable efficacy with significant toxicities.
More recently, targeted therapies have emerged as promising alternatives for the management of malignant effusions. Our understanding of the contribution of angiogenesis to ascites formation has resulted in the study of the antiangiogenic antibodies, bevacizumab and VEGF-trap, which have shown clinical efficacy in cohorts of heavily pretreated patients. In addition, the trifunctional antibody, catumaxomab, has shown positive signals in the treatment of malignant ascites. Ultimately, as with all novel therapies, symptom relief and treatment goals must be weighed against patient discomfort and potentially lethal adverse events. Careful patient selection and identification of risk factors to help reduce significant side effects associated with treatment are required. Further comparative studies and quality of life assessments are warranted before incorporation of these agents into daily practice.
Acknowledgment
We would like to thank Toa Ji for his artistic and digital imaging expertise, which were essential for the creation of the figures in this manuscript.
Disclosure
The authors have no conflicts of interest to disclose in this work.
References
- SiegelRNaishadhamDJemalACancer statistics, 2012CA Cancer J Clin2012621102922237781
- BookmanMTrials with impact on clinical management: first lineInt J Gynecol Cancer200919Suppl 2S55S6219955916
- OzolsRBundyBGreerBPhase III trial of carboplatin and paclitaxel compared with cisplatin and paclitaxel in patients with optimally resected stage III ovarian cancer: a Gynecologic Oncology Group studyJ Clin Oncol200321173194320012860964
- MonkBChoiDPugmireGBurgerRActivity of bevacizumab (rhuMAB VEGF) in advanced refractory epithelial ovarian cancerGynecol Oncol200596390290515721449
- CannistraSEvaluating new regimens in recurrent ovarian cancer: how much evidence is good enough?J Clin Oncol201028193101310320516442
- Pujade-LauraineEWagnerUAavall-LundqvistEPegylated liposomal doxorubicin and carboplatin compared with paclitaxel and carboplatin for patients with platinum-sensitive ovarian cancer in late relapseJ Clin Oncol201028203323332920498395
- CannistraSIs there a “best” choice of second-line agent in the treatment of recurrent, potentially platinum-sensitive ovarian cancer?J Clin Oncol20022051158116011870154
- EskanderRNRandallLMBevacizumab in the treatment of ovarian cancerBiologics201151521383911
- MalayevYLeveneRGonzalezFPalliative chemotherapy for malignant ascites secondary to ovarian cancerAm J Hosp Palliat Care2232012 [Epub ahead of print.]
- LoggieBWPeriniMFlemingRARussellGBGeisingerKTreatment and prevention of malignant ascites associated with disseminated intraperitoneal malignancies by aggressive combined-modality therapyAm Surg19976321371439012427
- BarniSCabidduMGhilardiMPetrelliFA novel perspective for an orphan problem: old and new drugs for the medical management of malignant ascitesCrit Rev Oncol Hematol201179214415320708947
- JemalASiegelRXuJWardECancer Statistics, 2010CA Cancer J Clin201060527730020610543
- BeckerGBlumHEVEGF trap for the treatment of malignant ascitesLancet Oncol201213211511622192728
- GarrisonRNGallowayRHHeuserLSMechanisms of malignant ascites productionJ Surg Res19874221261322434730
- AdamRAAdamYGMalignant ascites: past, present, and futureJ Am Coll Surg20041986999101115194082
- QaziRSavlovEDPeritoneovenous shunt for palliation of malignant ascitesCancer19824936006026174196
- ArielIMOropezaRPackGTIntracavitary administration of radioactive isotopes in the control of effusions due to cancer. Results in 267 patientsCancer1966198109611025912325
- RunyonBACare of patients with ascitesN Engl J Med199433053373428277955
- GotliebWHFeldmanBFeldman-MoranOIntraperitoneal pressures and clinical parameters of total paracentesis for palliation of symptomatic ascites in ovarian cancerGynecol Oncol19987133813859887235
- BeckerGGalandiDBlumHEMalignant ascites: systematic review and guideline for treatmentEur J Cancer200642558959716434188
- KeenAFitzgeraldDBryantADickinsonHOManagement of drainage for malignant ascites in gynaecological cancerCochrane Database Syst Rev20101CD00779420091648
- StarkRHSauterKESurgical treatment of adenocarcinoma of the stomach in a community hospitalSurg Gynecol Obstet198516021531563969612
- OstrowskiMJHalsallGMIntracavitary bleomycin in the management of malignant effusions: a multicenter studyCancer Treat Rep19826611190319076182995
- MaatBOosterleeJSpaasJAWhiteHLammesFBDissemination of tumour cells via LeVeen shuntLancet19791812398887670
- PaladineWCunninghamTJSponzoRDonavanMOlsonKHortonJIntracavitary bleomycin in the management of malignant effusionsCancer19763851903190862609
- BurgerRAAntiangiogenic agents should be integrated into the standard treatment for patients with ovarian cancerAnn Oncol201122Suppl 8viii65viii6822180405
- BurgerRAOverview of anti-angiogenic agents in development for ovarian cancerGynecol Oncol2011121123023821215996
- FerraraNVEGF as a therapeutic target in cancerOncology200569Suppl 3111616301831
- MonkBJHanEJosephs-CowanCAPugmireGBurgerRASalvage bevacizumab (rhuMAB VEGF)-based therapy after multiple prior cytotoxic regimens in advanced refractory epithelial ovarian cancerGynecol Oncol2006102214014416790264
- PaleyPJStaskusKAGebhardKVascular endothelial growth factor expression in early stage ovarian carcinomaCancer1997801981069210714
- SengerDRVan de WaterLBrownLFVascular permeability factor (VPF, VEGF) in tumor biologyCancer Metastasis Rev1993123–43033248281615
- FerraraNMolecular and biological properties of vascular endothelial growth factorJ Mol Med (Berl)199977752754310494799
- FerraraNRole of vascular endothelial growth factor in the regulation of angiogenesisKidney Int199956379481410469350
- FerraraNVascular endothelial growth factor: molecular and biological aspectsCurr Top Microbiol Immunol19992371309893343
- FerraraNKerbelRSAngiogenesis as a therapeutic targetNature2005438707096797416355214
- ShalabyFRossantJYamaguchiTPFailure of blood-island formation and vasculogenesis in Flk-1-deficient miceNature1995376653562667596435
- ZebrowskiBKLiuWRamirezKAkagiYMillsGBEllisLMMarkedly elevated levels of vascular endothelial growth factor in malignant ascitesAnn Surg Oncol19996437337810379858
- ByrneATRossLHolashJVascular endothelial growth factortrap decreases tumor burden, inhibits ascites, and causes dramatic vascular remodeling in an ovarian cancer modelClin Cancer Res20039155721572814654557
- XuLYonedaJHerreraCWoodJKillionJJFidlerIJInhibition of malignant ascites and growth of human ovarian carcinoma by oral administration of a potent inhibitor of the vascular endothelial growth factor receptor tyrosine kinasesInt J Oncol200016344545410675474
- StoelckerBEchtenacherBWeichHASztajerHHicklinDJMannelDNVEGF/Flk-1 interaction, a requirement for malignant ascites recurrenceJ Interferon Cytokine Res200020551151710841080
- KoboldSHegewisch-BeckerSOechsleKJordanKBokemeyerCAtanackovicDIntraperitoneal VEGF inhibition using bevacizumab: a potential approach for the symptomatic treatment of malignant ascites?Oncologist200914121242125120008305
- NumnumTMRocconiRPWhitworthJBarnesMNThe use of bevacizumab to palliate symptomatic ascites in patients with refractory ovarian carcinomaGynecol Oncol2006102342542816797681
- HamiltonCAMaxwellGLChernofskyMRBernsteinSAFarleyJHRoseGSIntraperitoneal bevacizumab for the palliation of malignant ascites in refractory ovarian cancerGynecol Oncol2008111353053218561992
- KestersonJPMhawech-FaucegliaPLeleSThe use of bevacizumab in refractory ovarian granulosa-cell carcinoma with symptomatic relief of ascites: a case reportGynecol Oncol2008111352752918710781
- StewartMWGripponSKirkpatrickPAfliberceptNat Rev Drug Discov201211426927022460118
- StewartMWAflibercept (VEGF trap-eye): the newest anti-VEGF drugBr J Ophthalmol3232012 [Epub ahead of print.]
- KimESSerurAHuangJPotent VEGF blockade causes regression of coopted vessels in a model of neuroblastomaProc Natl Acad Sci U S A20029917113991140412177446
- HuangJFrischerJSSerurARegression of established tumors and metastases by potent vascular endothelial growth factor blockadeProc Natl Acad Sci U S A2003100137785779012805568
- HuLHofmannJHolashJYancopoulosGDSoodAKJaffeRBVascular endothelial growth factor trap combined with paclitaxel strikingly inhibits tumor and ascites, prolonging survival in a human ovarian cancer modelClin Cancer Res20051119 Pt 16966697116203789
- LockhartACRothenbergMLDupontJPhase I study of intravenous vascular endothelial growth factor trap, aflibercept, in patients with advanced solid tumorsJ Clin Oncol201028220721419949018
- GayaATseVA preclinical and clinical review of aflibercept for the management of cancerCancer Treat Rev1192012 [Epub ahead of print.]
- TengLSJinKTHeKFZhangJWangHHCaoJClinical applications of VEGF-trap (aflibercept) in cancer treatmentJ Chin Med Assoc201073944945620875616
- ColomboNMangiliGMammolitiSA Phase II study of aflibercept in patients with advanced epithelial ovarian cancer and symptomatic malignant ascitesGynecol Oncol20121251424722112608
- GotliebWHAmantFAdvaniSIntravenous aflibercept for treatment of recurrent symptomatic malignant ascites in patients with advanced ovarian cancer: a Phase 2, randomised, double-blind, placebo-controlled studyLancet Oncol201213215416222192729
- RufPLindhoferHInduction of a long-lasting antitumor immunity by a trifunctional bispecific antibodyBlood20019882526253411588051
- ZeidlerRMysliwietzJCsanadyMThe Fc-region of a new class of intact bispecific antibody mediates activation of accessory cells and NK cells and induces direct phagocytosis of tumour cellsBr J Cancer200083226126610901380
- HeissMMMurawaPKoralewskiPThe trifunctional antibody catumaxomab for the treatment of malignant ascites due to epithelial cancer: Results of a prospective randomized Phase II/III trialInt J Cancer201012792209222120473913
- HeissMMStrohleinMAJagerMImmunotherapy of malignant ascites with trifunctional antibodiesInt J Cancer2005117343544315906359
- BurgesAWimbergerPKumperCEffective relief of malignant ascites in patients with advanced ovarian cancer by a trifunctional anti-EpCAM x anti-CD3 antibody: a phase I/II studyClin Cancer Res200713133899390517606723
- PietznerKJagerMSchoberthAFirst patient treated with a re-challenge of catumaxomab in recurrent malignant ascites: a case reportMed Oncol20122921391139621544631
- El-ShamiKAEEl-KermYOpen-label safety and efficacy pilot trial of intraperitoneal bevacizumab as palliative treatment in refractory malignant ascitesJ Clin Oncol20072518S620 Supplement9043