Abstract
Background
The female is programmed to nurture one fetus and to take care of one neonate at a time; hence, twin pregnancy is associated with an increased risk of preterm deliveries, perinatal morbidity, and mortality and maternal complications. This study aimed to determine the twinning rate, and maternal and fetal outcomes of all twin pregnancies managed at the Niger Delta University Teaching Hospital Okolobiri.
Methods
The study is a 4-year descriptive retrospective evaluation of twin pregnancies managed at the Niger Delta University Teaching Hospital Okolobiri. Records of all pregnancies, booked and unbooked, managed from January 1, 2007 to December 31, 2010 were reviewed. Details of delivery and maternal and fetal outcomes were obtained using a pro forma designed for the study. Epi Info version 3.5.3 was used for statistical analysis. The Chi-square test was used to test for associations between variables. The level of significance was set at P ≤ 0.05.
Results
A total of 1341 deliveries including 41 cases of twin deliveries were recorded during the study period, giving an incidence of 30.6/1000. Twenty-nine (70.7%) of the patients were unbooked. The mean gestational age was 33.3 ± 2.6 weeks, and the mean fetal weight was 2.34 ± 0.54 kg. There were 13 perinatal deaths, with a perinatal mortality rate of 158.5/1000. There was no association between booking status and perinatal mortality rate (χ2 = 0.017, P = 1.000). Prematurity was the chief cause of perinatal death (65.4%). Maternal morbidities included anemia, wound infection, and genital sepsis. There were no maternal deaths.
Conclusion
The twinning rate was high. There was a high perinatal mortality rate, with prematurity accounting for most of the mortality. There is a need for improved incubation/neonatal care for better outcomes with twin pregnancies in the hospital.
Introduction
Twin pregnancy refers to the presence of two fetuses in the uterus.Citation1 It results commonly from the fertilization of two separate ova (dizygotic) and about one third of cases arises from division of one fertilized ovum into two separate embryo (monozygotic).Citation1 There are considerable ethnic, racial, and geographical variations in the frequency of twin pregnancy.
The reported spontaneous twinning rate in the Yoruba-speaking western part of Nigeria is the highest in the world, with values as high as 45 per 1000 deliveries (1 in 22 deliveries) being reported.Citation2–Citation4 A rate of 1 in 36.2 has been reported among the Igbos in Nigeria.Citation5
The incidence of spontaneous twinning is higher in black women than in Caucasians and Asians.Citation2 It is about 1 in 83 deliveries in Caucasian women, being lowest in Asians. The difference in twinning rates seems to be due to differences in the incidence of dizygotic births, while the monozygotic rate varies very little between races and occurs with a constant incidence of 3.9 per 1000 births.Citation6 The incidence of twinning in developed countries has been rising over the last 20 years. The increase is entirely due to assisted reproductive technologies and ovulation induction agents.Citation7 Twins now comprise 25%–30% of all deliveries resulting from assisted reproductive techniques.Citation8 Other factors associated with twinning include heredity (family history of twinning, especially in a first-degree relative on the maternal side), increasing maternal age and parity, maternal height, weight for height, previous twin deliveries, use of ovulation induction agents, easy conception (usually within 3 months of marriage), and pregnancy soon after cessation of long-term oral contraceptive use.Citation8
Well known complications of twin pregnancy include abortion, hyperemesis gravidarum, congenital malformations, anemia, pregnancy-induced hypertension, intrauterine growth restriction, preterm labor, prelabor spontaneous rupture of membranes, and antepartum hemorrhage. Others are malpresentation, abnormal lie, polyhydramnios, cord prolapse, cord entanglement, urinary tract infection, postpartum hemorrhage, retained second twin, and increased operative vaginal delivery.Citation7–Citation11
Prematurity poses the greatest threat to twins, with an associated perinatal mortality rate of 3–8 times that of a singleton pregnancy.Citation1 Elective hospitalization for bed rest, prophylactic use of tocolytics, and use of cervical cerclage are measures proposed to reduce the high fetal wastage associated with premature labor in multiple pregnancies, but these have not been shown conclusively to be beneficial. Citation7,Citation8 However, during the past decade, maternal nutritional intervention has emerged as the only means that consistently improves outcome in twin pregnancy.Citation12 From the available guidelines, it appears that most clinicians would consider nonvertex first sets as an indication for cesarean sectionCitation13 and vertex first twins as candidates for vaginal delivery. Controversy exists for vertex–nonvertex pairs.Citation14
This study aimed to determine the twinning rate and describe maternal and fetal outcomes of all twin pregnancies managed at the Niger Delta University Teaching Hospital Okolobiri over a 4-year period.
Materials and methods
This study is a 4-year retrospective review of all twin pregnancies managed from January 1, 2007 to December 31, 2010 at the Niger Delta University Teaching Hospital Okolobiri, a tertiary hospital in Bayelsa State. The sources of information were patient case notes, and antenatal, labor, neonatal ward, and theater records. The total number of deliveries, fetal outcome, and numbers of labor and postnatal ward admissions were obtained for the period under review. The information obtained was coded and transferred onto a pro forma designed for the study. Data collected were analyzed using Epi Info version 3.5.3. Frequencies were generated for variables including maternal age, parity, booking status, birth weight, baby’s gender, and maternal and perinatal outcomes. The Chi-square test was used to test for any association between variables of interest. The level of significance was set at P ≤ 0.05. The following operational definitions were used during the conduct of this study: prematurity, ie, a baby born before 37 weeks of gestation, counting from the first day of the last menstrual period, and perinatal death, ie, all still births, plus death in first week after birth.
Results
During the 4-year period of the study, there were 41 twin deliveries out of a total of 1341 deliveries, giving an overall incidence of twin delivery of 30.6/1000 or 1 in 33 deliveries. shows the sociodemographic characteristics of the patients. Their age ranged from 17 to 41 years, with a mean of 28.1 ± 5.7 years. The majority (19, 46.3%) of the patients were aged 30–39 years, and four (9.8%) of the patients were teenagers. Their parity was 0–6, with a mean of 2.4 ± 1.9. About a third (14, 34.1%) were grand multiparous, 24 (58.5%) had at least secondary education, and the majority (29, 70.7%) were unbooked. The mean gestational age was 33.3 ± 2.6 weeks, and mean fetal weight was 2.34 ± 0.54 kg. There was no statistically significant difference in mean weight between first and second twins (P = 0.550). There were more males (42, 51.2%) than females, and more low birth weight babies (44, 53.7%). The most common mode of presentation was cephalic/cephalic (25, 61.0%), followed by cephalic/breech (seven, 17.1%), breech/cephalic (five, 12.2%), and breech/ breech (four, 9.7%).
Table 1 Sociodemographic characteristics of patients
Twenty sets (48.8%) of twins were delivered by cesarean section, the majority (16, 80%) of which were emergencies. Eighteen sets (43.9%) had spontaneous vaginal delivery, while three (7.3%) had a combination of assisted vaginal breech delivery and instrumental vaginal delivery. shows the indications for emergency cesarean section. The two commonest indications were breech presentation (second twin cephalic) 3/18.8%, and severe pre-eclampsia/ eclampsia 3/18.8%. The indications for all cesarean sections performed are shown in . The three commonest indications were breech presentation (second twin cephalic) 6/30%, breech presentation (second twin breech) 3/15%, and eclampsia/severe pre-eclampsia 3/15%. shows the maternal morbidities in the patients who had cesarean section.
Figure 1 Indication for emergency cesarean section.
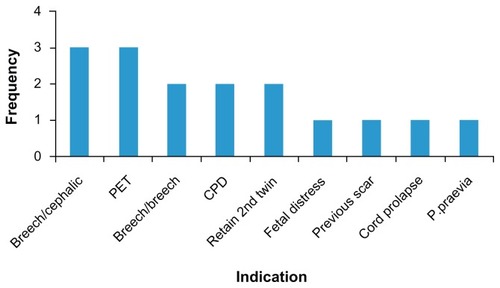
Table 2 Indication for cesarean section
Table 3 Morbidity among patients who had emergency cesarean section
The causes of perinatal mortality are presented in . There were 13 perinatal deaths, comprising nine in the unbooked patients, with a perinatal mortality rate of 155.2/1000, compared with four in the booked patients, with a perinatal mortality rate of 166.7/1000 (χ2 = 0.017, P = 1.0). The overall perinatal mortality rate was 158.5/1000. Prematurity accounted for 61.5% of these deaths.
Table 4 Causes of perinatal death
Discussion
The twining rate of 30.6 per 1000 (one in 33) in this study was lower than the 53 per 1000 deliveries (one in 19)Citation3,Citation4,Citation6 reported among the Yorubas in the Western part of Nigeria and one in 24 reported among the Igbos,Citation14 but higher than the one in 76 reported from a similar institution in Maiduguri, Nigeria.Citation15 The species of yam (Dioscorea rotundata) found in the Yoruba land is said to contain an ovulation induction agent and this may explain the high incidence of multiple pregnancy among the Yorubas in Nigeria.Citation16 However, a decline in this rate has been observed.Citation17 Thus, the twinning rate in Nigeria is probably influenced by factors other than ethnicity.
In this study, 46.3% of the patients were aged 30–39 years, which is lower than the 77% reported from a study in another developing country.Citation18 Over 30% of the patients in this study were grand multiparous. Older age and high parity are two strong independent factors associated with an increased incidence of twinning.Citation11
Regarding the mode of delivery, the guidelines are mainly based on presentation, fetal weight, and well being. These guidelines have not changed over past decades, and national data from the US and the UK suggest that about 60% of multiples are delivered by cesarean section.Citation13 Cesarean section has been advised where the first twin is breech, based on extrapolation from the Term Breech Trial, and the desire to avoid the rare interlocking with head entrapment of a presenting breech above a second cephalic twin. The presentation of the second twin is of little relevance until after the birth of the first.
In this study, 48.8% of women underwent cesarean section (80.0% of which were emergency cesarean sections). This is higher than the 10.6%Citation15 but lower than the 60%Citation19 reported from previous studies. The reason is that most of these patients were referred from private and public primary and secondary health facilities within and sometimes outside Bayelsa. Often, the women had been in labor for more than 24 hours at these centers and were often referred late in the night for various reasons, hence the high rate of emergency procedures. The high cesarean section rate is a major public health problem because cesarean section increases the health risk for both mothers and their babies, as well as the cost of health care compared with normal deliveries.Citation20 Furthermore, doubt has been raised about whether the observed increase in cesarean section can be justified in terms of perinatal statistics. In developed countries, there has been no significant diminution in the perinatal mortality rate despite the increase in the cesarean section rates.Citation21
Essentially the risks of vaginal delivery are increased in twins compared with singletons, as are the risks of cesarean section.Citation22 Therefore, it is not surprising that maternal morbidity was high in this study. Evidence from other studies suggest that maternal morbidity from cesarean section is comparable with that of vaginal delivery where the emergency rate exceeds one in three,Citation23 as was found in this study where most of the cesarean sections were performed as emergencies, with some patients admitted with dehydration, intrapartum genital sepsis, or anemia, all of which further enhance the risk of post partum infection. Anemia was the commonest complication in this group of women with cesarean section (nine, 45.0%). Others were wound infection (seven, 35.0%), genital sepsis (five, 25.0%), and thrombophlebitis (three, 15.0%).
There were 13 perinatal deaths, which gives a perinatal mortality rate of 158.5 per 1000. Over 70% of the babies were delivered prematurely and more than half were of low birth weight. Prematurity and low birth weight are two major causes of perinatal death, especially in the developing world where facilities and supportive care are inadequate, the Niger Delta University Teaching Hospital being no exception. Other identified causes that may explain the poor birth outcome include failure to diagnose twinning before the onset of labor, birth asphyxia, a retained second twin, and malpresentation. The referral system in this state is inadequate because most primary and secondary health facilities are remotely located with poor access to places like the Niger Delta University Teaching Hospital, where further help could be sought. Most state hospitals are also limited in facilities and expertise. Private hospitals also contribute to the poor outcomes experienced in the hospital. A great number of them persevere with labor cases beyond what they can handle for career and economic reasons, and refer only when complications have set in. Although the perinatal mortality rate of 158.5/1000 births in this study is similar to that reported by other studies,Citation15,Citation19 it is higher than the perinatal mortality rate of 79.6/1000 for singleton births during the study period. Not all the women delivered at the hospital were from Bayelsa State, and some were referred from neighboring states. Therefore, the twinning rate in this study may be an overestimate of the true rate in the area that the hospital primarily serves.
In conclusion, twinning has always been an important topic not only medically but also socially and economically in obstetric practice in Nigeria because of the high twinning rate in the country. The perinatal mortality was higher than for singletons in this study, and prematurity was largely responsible. We recommend that the hospital should apply interventions that will minimize premature delivery in twin pregnancies and improve on its incubation/ neonatal care.
Acknowledgment
We acknowledge all the hospital staff members who assisted in collection of the study data.
Disclosure
The authors report no conflicts of interest in this work.
References
- NkyekyerKMultiple pregnancyKwawukwumeEYEmuveyanEEComprehensive Obstetrics in the TropicsAccra GhanaAsante and Hittscher Printing Press Ltd2002
- AbuduOOAnorluRIMultiple pregnancyAgboolaATextbook of Obstetrics and Gynaecology for Medical Students2nd edIbadan, NigeriaHeinemann Educational Books2006
- FiskNMMultiple pregnancyEdmondsKDewhurst’s Textbook of Obstetrics and Gynaecology for Postgraduates7th edOxford, UKBlackwell Scientific Publication2007
- AkinkugbeAMultiple pregnancyA Textbook of Obstetrics and GynaecologyIbadan, NigeriaEvans Brothers Nigeria Publishers Ltd1996
- AdinmaJIBAgbaiAOPattern of twin birth in Nigerian Igbo womenWest Afr J Med1994132342367756191
- OlayemiOOAdenijiARAimakhuCODeterminant of perinatal mortality in twins at IbadanTrop J Obstet Gynaecol2002193638
- MartinJAHamiltonBESuttonPDVenturaSJMenackerFMunsonMLBirths: final data for 2002Natl Vital Stat Report2003521113
- FakeyeOPerinatal factors in twin mortality in NigeriaInt J Gynaecol Obstet1986243093142878841
- ObisesanKAArowojoluAOIlesanmiAORobertsOAFawoleORelative risk associated with the second-born twin at birthNig J Clin Pract199921314
- PernollMLMelissaMMultiple pregnancyDecherneyDHPernollMLCurrent Obstetric and Gynaecologic Diagnosis and Treatment9th edNew York, NYMcGraw-Hill and Lange Medical Books2003
- LukeBImproving multiple pregnancy outcomes with nutritional interventionsClin Obstet Gynecol20044714616215024282
- BlicksteinIGoldmanRDKupfermincMDelivery of breech first twins: a multicenter retrospective studyObstet Gynecol200095374210636499
- HogleKIHuttonEKMcbrienKABarretJFHannahMECesarean delivery for twins: a systematic review and meta-analysisAm J Obstet Gynecol20038822022712548221
- Sunday-AdeoyeITwomeyEDEgwuatuVEBirths at Mater Misericordiae Hospital, Afikpo, South Eastern NigeriaNiger J Clin Pract20081123123419140360
- NwobodoEIBobzomDNObedJTwin births at University of Maiduguri Teaching Hospital: incidence, pregnancy complications and outcomeNiger J Med200211676912221962
- OdunsiKObinmwanneFCJekelJOtoideVOWyshakGOkonofuaFEWhite Yam (Dioscorea rotundata) and socioeconomic status as risk factors for twin births in Southwest NigeriaPresented at the the Fifth International Congress of the Society of Gynecology and Obstetrics of NigeriaBenin City, Edo State, NigeriaNovember 23–28, 1998
- MarinhoAOIlesanmiAOLadeleOAA fall in the rate of multiple births in Ibadan and Igbo-Ora, NigeriaActa Genet Med Gemellol (Roma)1986352012043591227
- KouamLKamdom-MoyoJDohASNgassaPOutcome of twin deliveries at the University Teaching Hospital, Yaounde, Cameroon – a 15 year experienceJ Obstet Gyneacol199818340344
- IgberaseGOEbeigbePNBock-OrumaATwinning rate in a rural mission tertiary hospital in the Niger Delta, NigeriaJ Obstet Gynaecol20082858658919003650
- NaymiRSRehanNPrevalence and determinants of caesarean section in a teaching hospital of PakistanJ Obstet Gynaecol20002047948315512631
- BeazleyJMCaesarean sectionChamberlainGTurnbullSAObstetrics1st edChurchill Livingstone1993
- WardRHWhittleMMultiple PregnancyLondon, UKRoyal College of Obstetricians and Gynaecologists Press1995
- BarrettJFRitchieWKTwin deliveryBest Pract Res Clin Obstet Gynaecol20026435611866496